A Pilot Study on AI-Powered Gamified Chatbot with OMO Strategy for Enhancing Parental Nutrition Knowledge †



Abstract
1. Introduction
2. Theoretical Background
2.1. Gamification in Education
2.2. The Role of AI in Gamification
2.3. Online Merge Offline Model
3. Materials and Methods
3.1. Design of Gamified Chatbots
- (1)
- User Interface: The system leverages the LINE messaging platform as the primary interface. Parents can access the chatbot by scanning a QR code, facilitating easy onboarding. The chatbot provides an interactive conversational interface for user engagement.
- (2)
- Backend Infrastructure: The backend is composed of two primary databases and a management system: (a) Knowledge Database: stores nutritional information and content. (b) Results Database: captures user interactions and progress data. (c) Backend Management of Gamified Chatbots: oversees the chatbot’s functionality and gamification elements.
- (3)
- Artificial Intelligence Integration: An AI component is central to the system. The knowledge imparted by professional dietitians in each lecture was incorporated into the learning process, becoming a source of knowledge that can provide user feedback. It is responsible for: (a) Processing nutritional knowledge. (b) Implementing the nutritional response mechanism. (c) Generating quiz questions. (d) Creating educational nutrition videos.
- (4)
- Gamification Elements: The system incorporates levels and rankings, displayed on a mobile interface, to enhance user engagement and motivation.
- (5)
- Stakeholder Interactions: (a) Parents interact directly with the chatbot through LINE. (b) Caregivers receive push notifications, allowing for timely interventions or support.
- (6)
- Data Flow: (a) User interactions are saved to the Results Database. (b) The system can push notifications to both parents and caregivers.
3.2. Research Subject
- (1)
- Mobile phone use: It was specified in the recruitment announcement that participants of the health seminar should be capable of using a mobile phone, allowing parents to register themselves.
- (2)
- Pre-test and post-test surveys: Participants completed a pre-test questionnaire before each health seminar to gauge their initial overall knowledge of nutrition. A pre-test was administered before each health seminar and a post-test afterward. At the final health seminar, a comprehensive post-test was conducted, ensuring a thorough assessment of the overall improvement in nutritional knowledge among the children’s parents.
3.3. Data Collection and Analysis
- (1)
- Pre-test and Post-test Assessments: Participants completed knowledge assessments before and after each seminar to measure changes in nutritional knowledge. These assessments were administered through the chatbot interface.
- (2)
- Engagement Metrics: The system automatically tracked various engagement metrics, including frequency of chatbot interactions, completion rates for quizzes and activities, and time spent on different features.
- (3)
- Demographic Information: Basic demographic data were collected from participants, including gender, age range, and educational level, to explore potential relationships between these factors and intervention outcomes.
4. Results
4.1. Gamified Chatbot System
4.2. The OMO Strategy of the Gamified Chatbot
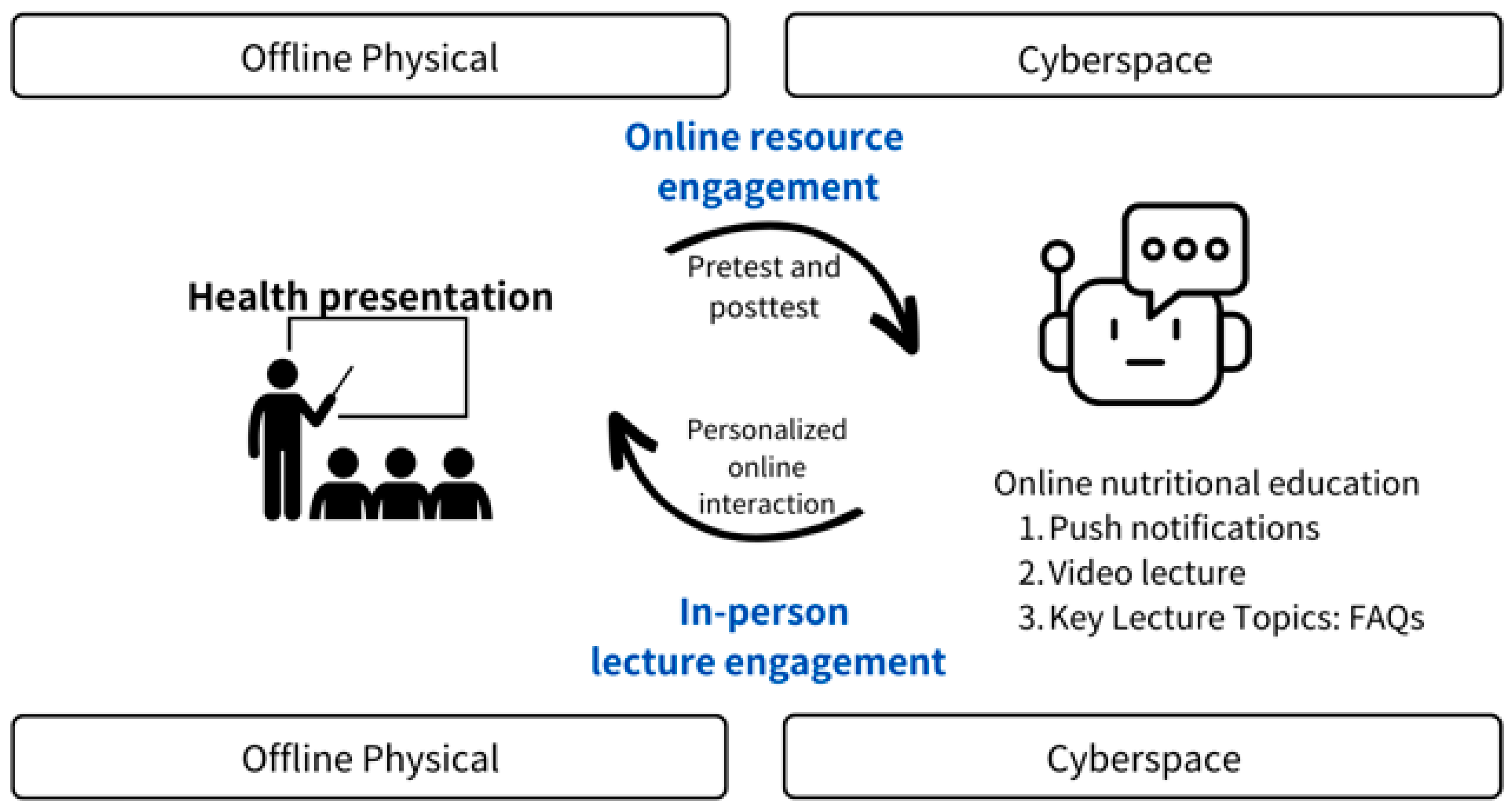
- Offline Physical
- (1)
- Conducting eight health presentations: These lectures focused primarily on parents of children and introduced eight sessions related to nutrition from the perspective of essential nutritional health.
- (2)
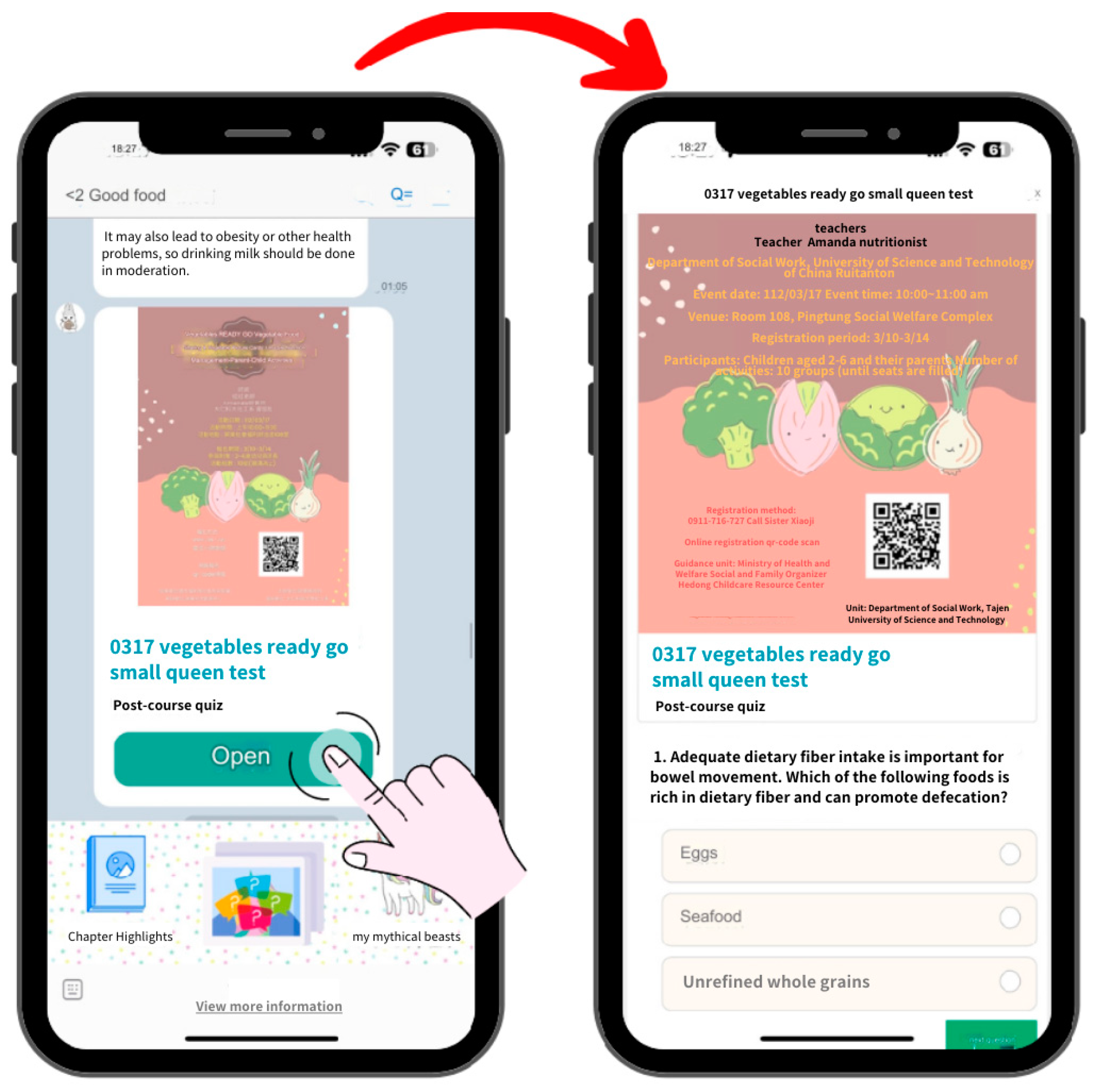
- Implementing pre-tests and post-tests: To evaluate the effectiveness of the nutritional knowledge intervention, each health lecture involved guiding parents to scan a QR code to access the chatbot and complete a pre-test. After the health lecture, post-test information was pushed to participants via the chatbot to conduct the post-test.
- Online resource engagement and in-person lecture engagement
- (1)
- Conduct “pre-tests” before starting physical seminars: The content of each pre-test is based on nutritional knowledge literature summaries related to the particular seminar. This approach allows parents not only to take a pre-test but also to better understand the key points of each health seminar. The pre-test is built on a chatbot platform, which plays a crucial role in the pre-testing process, providing parents with an interactive and engaging online space.
- (2)
- Pre-testing and post-testing: The pre-tests and post-tests for each health seminar are channels integrating OMO (Online Merges Offline), guiding parents into chatbots, and enabling them to access personalized interactive channels.
- Cyberspace
- (1)
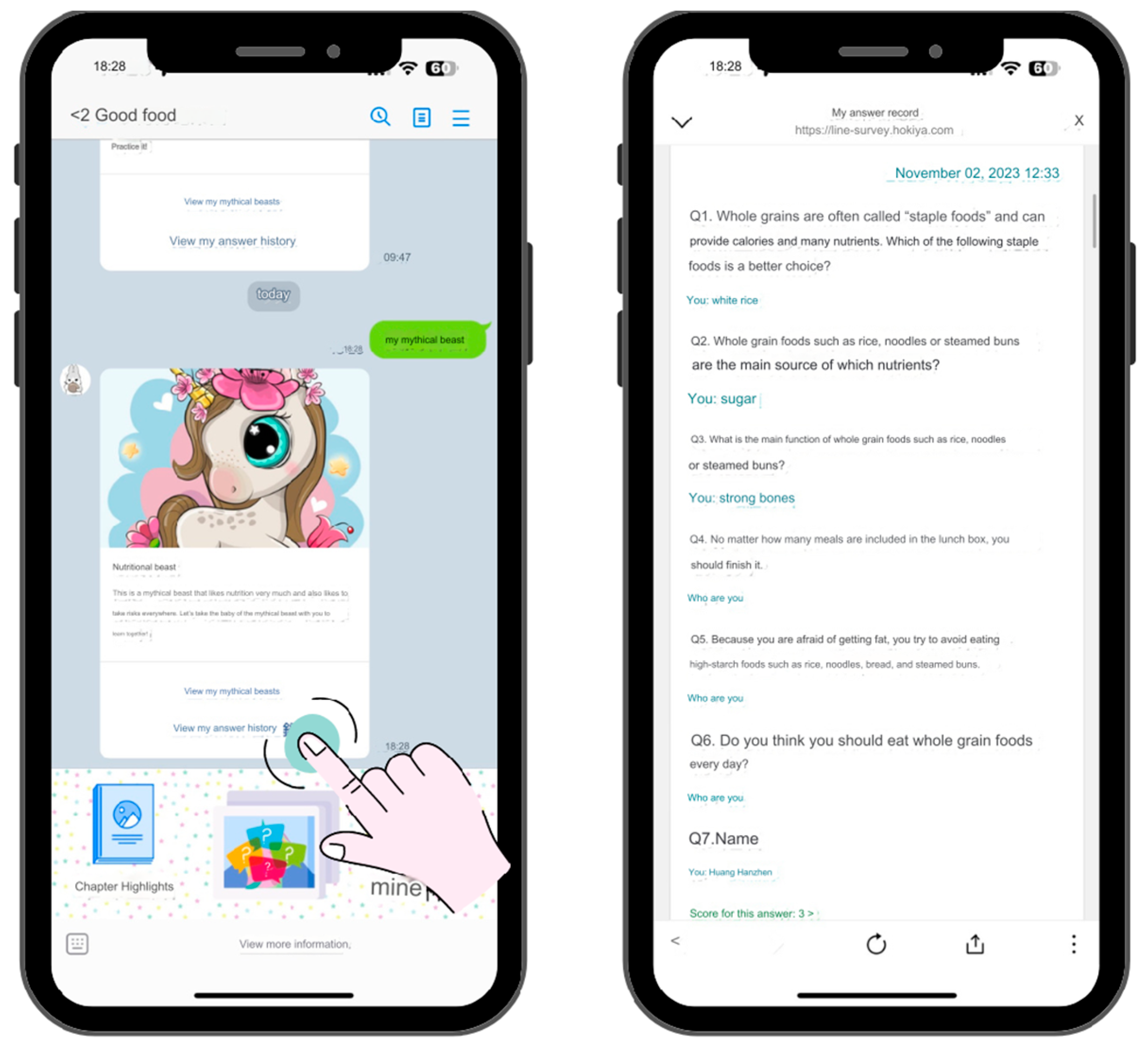
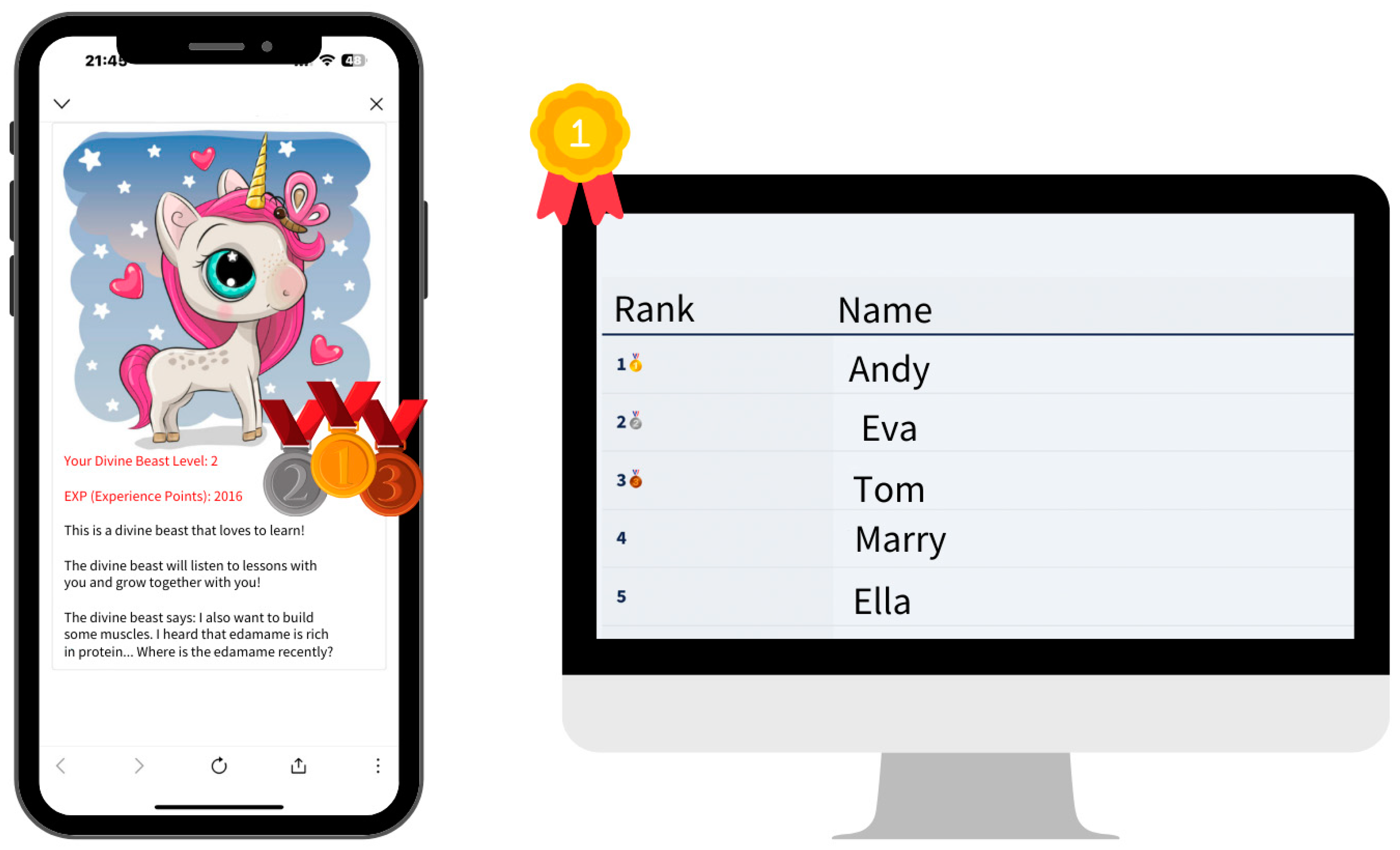
- Pre-test content serves as personal online resources: Individuals can continuously view their answers from each health seminar’s pre-test responses. By reviewing these answers, they become more familiar with the nutritional knowledge conveyed by nutritionists in each session. The system interface is shown in Figure 4.
- (2)
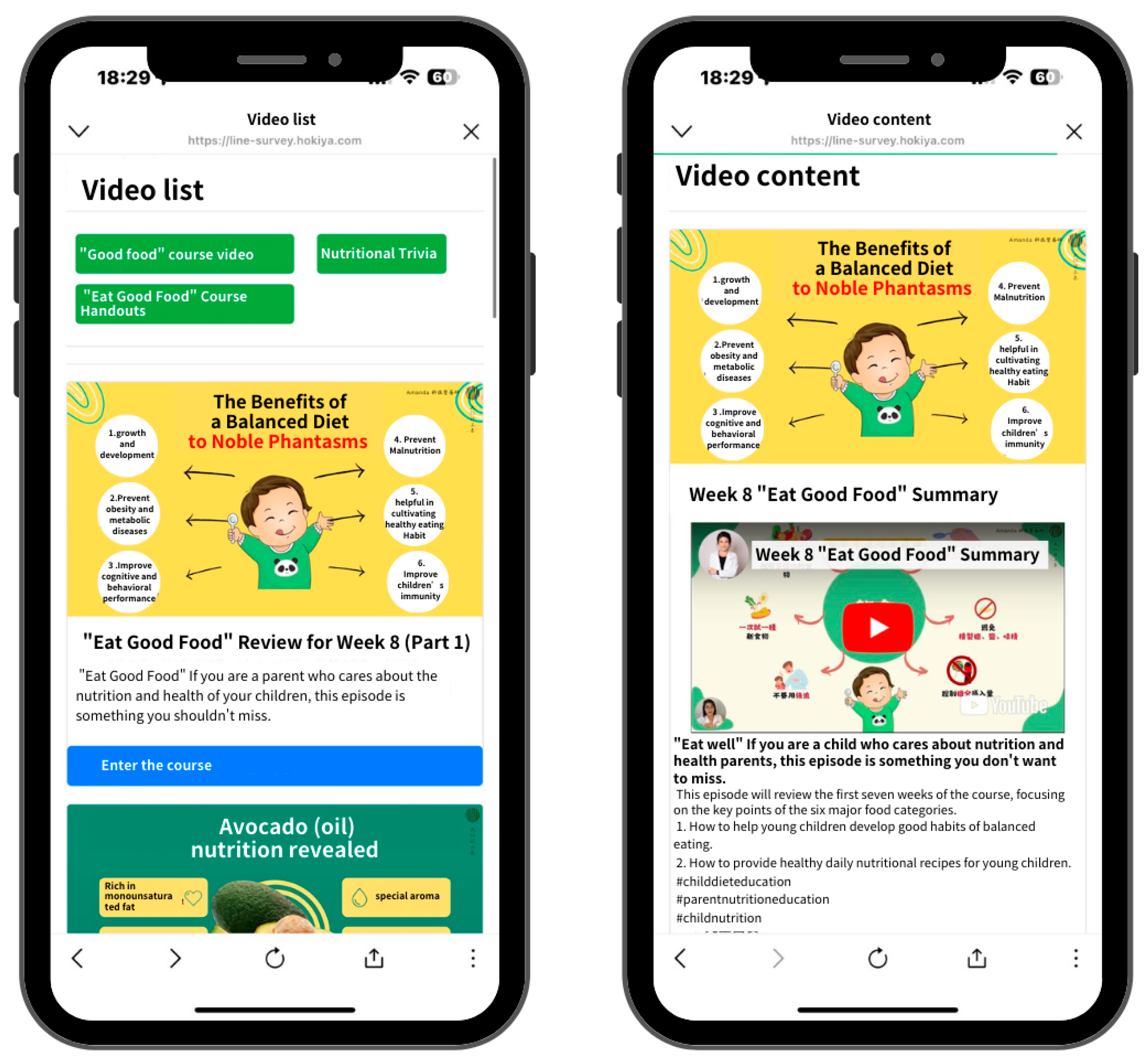
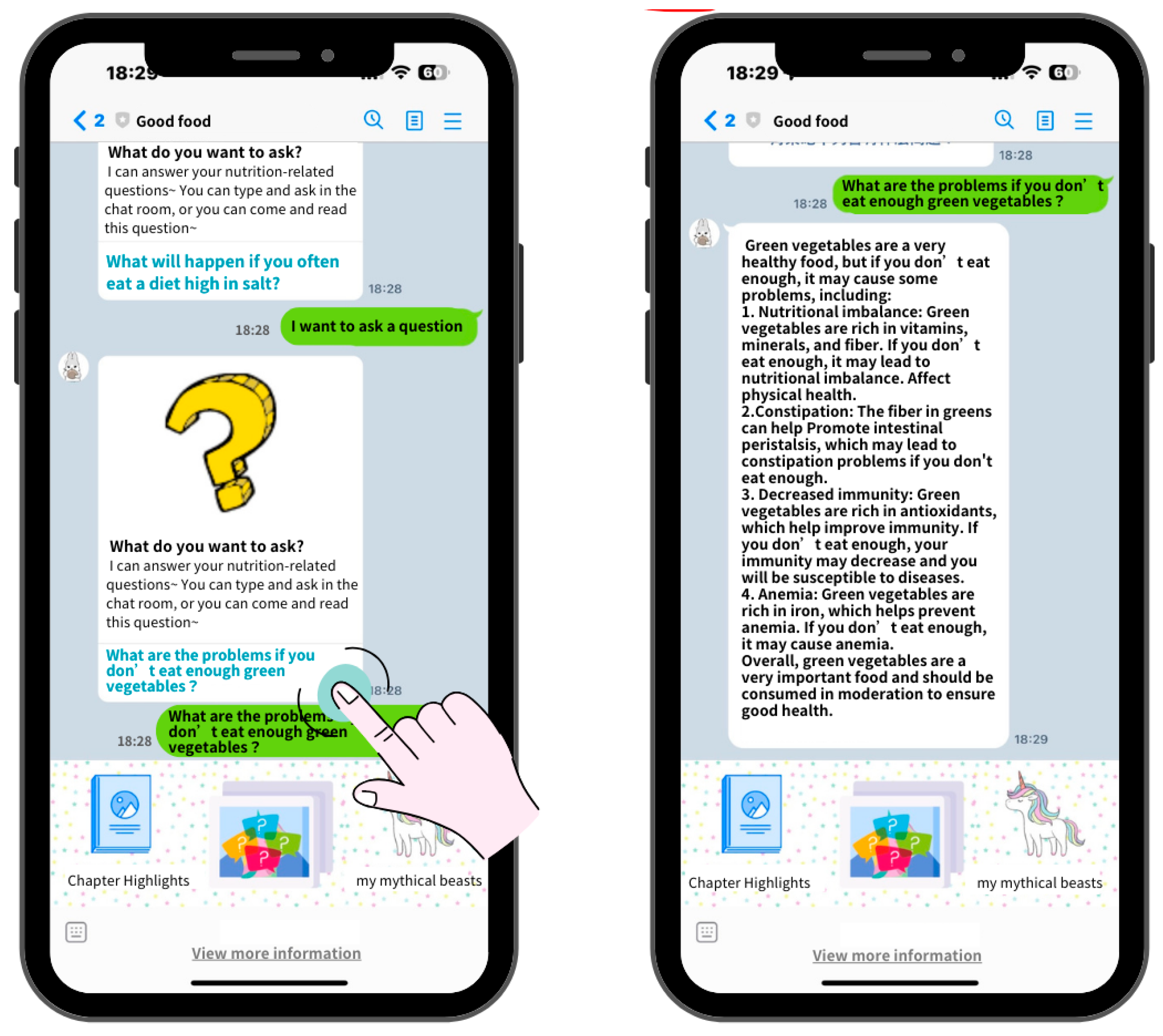
- Individualized online interaction after health seminars: Users can watch videos on nutrition topics they are interested in. When encountering relevant issues or questions, they can inquire within the chatbot, which has been trained by AI technology to respond with answers related to questions raised during the health seminars. The system interface is shown in Figure 5 and Figure 6.
- Gamification
- (1)
- Level Completion Mechanism: Both the pre-test and post-test consist of nutritional knowledge questions with correct answers. Each completion of the pre-test or post-test will have a score. Reaching a certain threshold allows the participant to pass the level. This gamified chatbot system is equipped with a level completion mechanism.
- (2)
- Community Ranking: As the chatbot is built on a social platform, the level completion scores of participants on this platform are ranked. The community ranking creates a sense of fun and competition among users, enhancing the enjoyment of using this chatbot and promoting the improvement of nutritional knowledge. It is shown in Figure 7.
4.3. Basic Information Description
4.4. Pre-Test and Post-Test Data Analysis
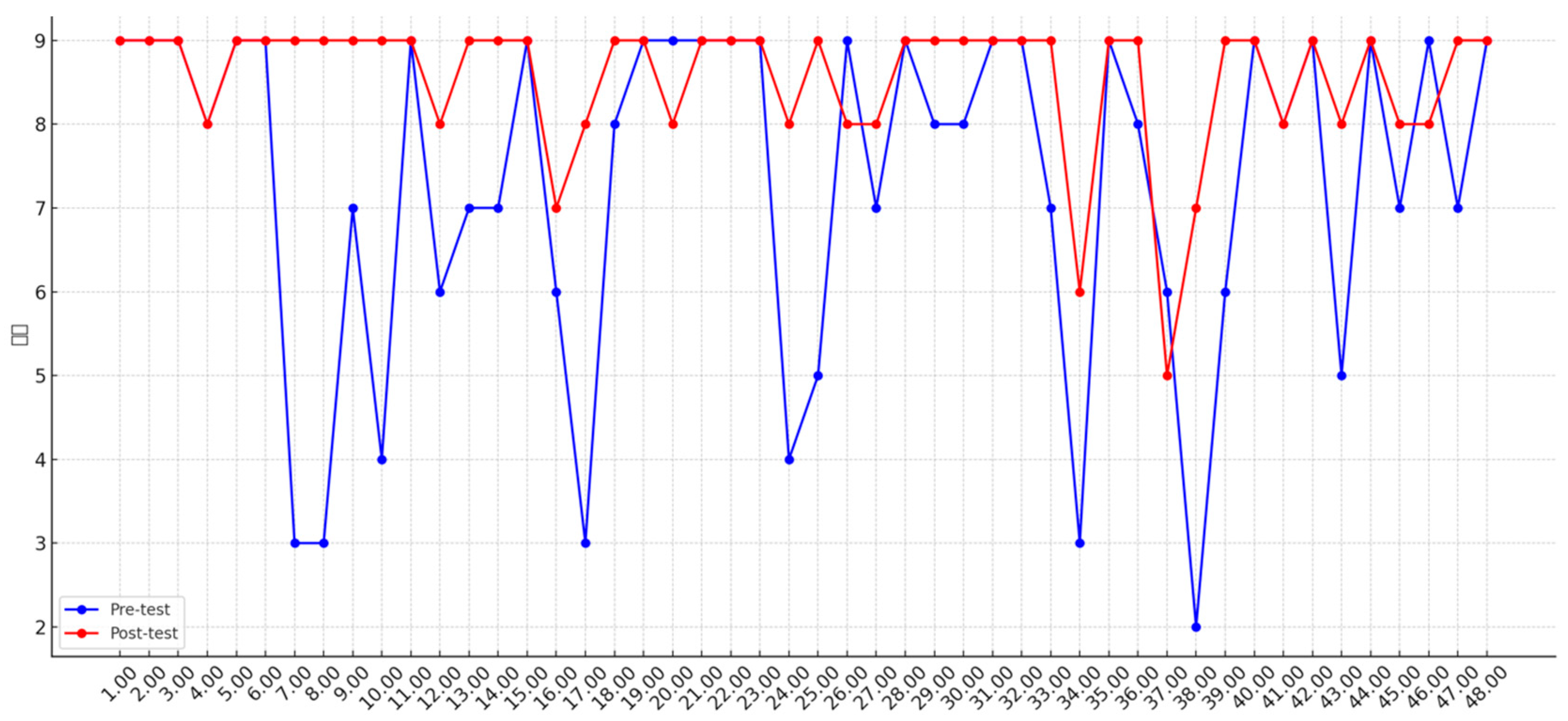
4.5. Pre-Test and Post-Test Evaluation of Effectiveness
5. Discussion
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Kemp, S. DIGITAL 2023: TAIWAN. 2023. Available online: https://datareportal.com/reports/digital-2023-taiwan (accessed on 9 February 2025).
- El Hefny, W.; El Bolock, A.; Herbert, C.; Abdennadher, S. Chase away the virus: A character-based chatbot for COVID-19. In Proceedings of the 2021 IEEE 9th International Conference on Serious Games and Applications for Health (SeGAH), Dubai, United Arab Emirates, 4–6 August 2021; pp. 1–8. [Google Scholar]
- Jakob, R.; Harperink, S.; Rudolf, A.M.; Fleisch, E.; Haug, S.; Mair, J.L.; Salamanca-Sanabria, A.; Kowatsch, T. Factors influencing adherence to mHealth apps for prevention or management of noncommunicable diseases: Systematic review. J. Med. Internet Res. 2022, 24, e35371. [Google Scholar] [CrossRef] [PubMed]
- Deterding, S.; Dixon, D.; Khaled, R.; Nacke, L. From game design elements to gamefulness: Defining “gamification”. In Proceedings of the 15th International Academic MindTrek Conference: Envisioning Future Media Environments, Tampere, Finland, 28–30 September 2011; pp. 9–15. [Google Scholar]
- Bas-Sarmiento, P.; Julián-López, C.; Fernández-Gutiérrez, M.; Poza-Méndez, M.; Marín-Paz, A.-J. Gamified eHealth interventions for health promotion and disease prevention in children and adolescents: A scoping review. Humanit. Soc. Sci. Commun. 2025, 12, 1–14. [Google Scholar] [CrossRef]
- Edwards, E.A.; Lumsden, J.; Rivas, C.; Steed, L.; Edwards, L.; Thiyagarajan, A.; Sohanpal, R.; Caton, H.; Griffiths, C.; Munafò, M. Gamification for health promotion: Systematic review of behaviour change techniques in smartphone apps. BMJ Open 2016, 6, e012447. [Google Scholar] [CrossRef]
- Li Lan, P.W.; Wenting, Y. Results of a Survey on Nutritional Dietary Knowledge and Eating Behavior of Taiwanese People in 1993–1996; Executive Yuan Department of Health: Taipei, Taiwan, 1999. [Google Scholar]
- Wenhan, P. Report on the Results of the Survey on Changes in National Nutrition and Health Status 2017–2020; Research Project Commissioned by the National Health Administration of the Ministry of Health and Welfare: Taiwan, 2022. [Google Scholar]
- Wenhan, P. Report on the Survey Results of National Nutrition and Health Changes, 2013–2016; Research Project Commissioned by the National Health Administration of the Ministry of Health and Welfare: Taiwan, 2019. [Google Scholar]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef]
- Yee, A.Z.; Lwin, M.O.; Ho, S.S. The influence of parental practices on child promotive and preventive food consumption behaviors: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–14. [Google Scholar] [CrossRef]
- Hurmuz, M.Z.; Jansen-Kosterink, S.M.; Hermens, H.J.; van Velsen, L. Game not over: Explaining older adults’ use and intention to continue using a gamified eHealth service. Health Inform. J. 2022, 28, 14604582221106008. [Google Scholar] [CrossRef] [PubMed]
- Laymouna, M.; Ma, Y.; Lessard, D.; Schuster, T.; Engler, K.; Lebouché, B. Roles, users, benefits, and limitations of chatbots in health care: Rapid review. J. Med. Internet Res. 2024, 26, e56930. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Mustafa, M.Y.; Tlili, A.; Zhuang, R.; Chang, T.-W.; Burgos, D. Design of Online-Merge-Offline (OMO) learning environments in the post-COVID-19 era: Case study analysis. In International Encyclopedia of Education, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2023; pp. 296–304. [Google Scholar]
- Hamari, J.; Koivisto, J. “Working out for likes”: An empirical study on social influence in exercise gamification. Comput. Hum. Behav. 2015, 50, 333–347. [Google Scholar] [CrossRef]
- Alzghoul, B. The Effectiveness of Gamification in Changing Health-related Behaviors: A Systematic Review and Meta-analysis. Open Public Health J. 2024, 17, 1. [Google Scholar] [CrossRef]
- Floryan, M.R.; Ritterband, L.M.; Chow, P.I. Principles of gamification for Internet interventions. Transl. Behav. Med. 2019, 9, 1131–1138. [Google Scholar] [CrossRef]
- Hamari, J.; Koivisto, J. Social Motivations To Use Gamification: An Empirical Study Of Gamifying Exercise. In Proceedings of the ECIS, Utrecht, The Netherlands, 5–8 June 2013; pp. 18–19. [Google Scholar]
- Winkler, R.; Söllner, M. Unleashing the potential of chatbots in education: A state-of-the-art analysis. In Academy of Management Proceedings; Academy of Management: Briarcliff Manor, NY, USA, 2018; p. 15903. [Google Scholar]
- Adamopoulou, E.; Moussiades, L. Chatbots: History, technology, and applications. Mach. Learn. Appl. 2020, 2, 100006. [Google Scholar] [CrossRef]
- Laranjo, L.; Dunn, A.G.; Tong, H.L.; Kocaballi, A.B.; Chen, J.; Bashir, R.; Surian, D.; Gallego, B.; Magrabi, F.; Lau, A.Y. Conversational agents in healthcare: A systematic review. J. Am. Med. Inform. Assoc. 2018, 25, 1248–1258. [Google Scholar] [CrossRef] [PubMed]
- Tudor Car, L.; Dhinagaran, D.A.; Kyaw, B.M.; Kowatsch, T.; Joty, S.; Theng, Y.-L.; Atun, R. Conversational agents in health care: Scoping review and conceptual analysis. J. Med. Internet Res. 2020, 22, e17158. [Google Scholar] [CrossRef] [PubMed]
- Følstad, A.; Brandtzaeg, P.B. Users’ experiences with chatbots: Findings from a questionnaire study. Qual. User Exp. 2020, 5, 3. [Google Scholar] [CrossRef]
- Fadhil, A. Can a chatbot determine my diet?: Addressing challenges of chatbot application for meal recommendation. arXiv 2018, arXiv:1802.09100. [Google Scholar]
- Cheng, C.; Ebrahimi, O.V. Gamification: A novel approach to mental health promotion. Curr. Psychiatry Rep. 2023, 25, 577–586. [Google Scholar] [CrossRef]
- Tolks, D.; Schmidt, J.J.; Kuhn, S. The role of AI in serious games and gamification for health: Scoping review. JMIR Serious Games 2024, 12, e48258. [Google Scholar] [CrossRef]
- Damaševičius, R.; Maskeliūnas, R.; Blažauskas, T. Serious games and gamification in healthcare: A meta-review. Information 2023, 14, 105. [Google Scholar] [CrossRef]
- Patel, A.V.; Jasani, S.; AlAshqar, A.; Doshi, R.H.; Amin, K.; Panakam, A.; Patil, A.; Sheth, S.S. Comparative Evaluation of Artificial Intelligence Models for Contraceptive Counseling. Digital 2025, 5, 10. [Google Scholar] [CrossRef]
- Rahman, A.; Uddin, J. Revealing Factors Influencing mHealth Adoption Intention Among Generation Y: An Empirical Study Using SEM-ANN-IPMA Analysis. Digital 2025, 5, 9. [Google Scholar] [CrossRef]
- Verhoef, P.C.; Kannan, P.K.; Inman, J.J. From multi-channel retailing to omni-channel retailing: Introduction to the special issue on multi-channel retailing. J. Retail. 2015, 91, 174–181. [Google Scholar] [CrossRef]
- Economy, M.O. Survey Report on Digital Transformation in Retail; Taiwan, 2021. [Google Scholar]
- Zhang, D.; Ma, J.; Lin, Q.; Yang, C.; Bo, W.; Xia, Y.; Wang, G.; Yang, Y.; Zhang, J. Online-merge-offline (OMO)-based music therapy for asthmatic children during the COVID-19 pandemic in China. Eur. J. Pediatr. 2024, 183, 1277–1286. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Mustafa, M.Y.; Tlili, A.; Chang, T.-W.; Xu, L. Ready or not? Investigating teachers’ readiness for adopting online merge offline (OMO) learning in digital transformation. In Proceedings of the International Conference on Blended Learning, Hong Kong, China, 17–20 July 2023; pp. 3–13. [Google Scholar]
- Xiao, J.; Sun-Lin, H.-Z.; Cheng, H.-C. A framework of online-merge-offline (OMO) classroom for open education: A preliminary study. Asian Assoc. Open Univ. J. 2019, 14, 134–146. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nutritional Lecture Units | Pre-Test and Post-Test Question Count | Children’s Parent Participants | |
|---|---|---|---|
| 1. | Nutritional Supplements & My Healthy Meal Plate | 6 Questions | 11 |
| 2. | Sweet and Sour Yogurt | 6 Questions | 9 |
| 3. | Whole Grains and Cereals | 6 Questions | 7 |
| 4. | Vegetable READY GO | 6 Questions | 13 |
| 5. | Fruit Party | 6 Questions | 11 |
| 6. | Bean, Fish, Egg, Meat Salad | 6 Questions | 9 |
| 7. | Little Chefs | 6 Questions | 7 |
| 8. | My Healthy Meal Plate | 6 Questions | 10 |
| Basic Attributes | Category | Frequency | Proportion |
|---|---|---|---|
| Gender | |||
| female | 18 | 90% | |
| male | 2 | 10% | |
| Age range | |||
| 31–40 | 6 | 30% | |
| 41–50 | 5 | 25% | |
| 21–30 | 4 | 20% | |
| 61–70 | 4 | 20% | |
| Education | |||
| University/Junior College | 16 | 80% | |
| High School/Higher Vocational | 4 | 20% | |
| Occupation | |||
| Stay-at-home mom | 12 | 60% | |
| public servant | 5 | 25% | |
| retire | 3 | 15% | |
| How happy you are to participate in the event | 90% | ||
| 💙💚💗💛💜 | 18 | ||
| 💚💛💝💜 | 2 | 10% | |
| Are you looking forward to the next event? | 95% | ||
| 😄 😄 😄 | 19 | ||
| 😉 😉 | 1 | 5% |
| No. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 |
| Pre-test | ||||||||||||||||||||
| score | 9 | 9 | 9 | 8 | 9 | 9 | 3 | 3 | 7 | 4 | 9 | 6 | 7 | 7 | 9 | 6 | 3 | 8 | 9 | 9 |
| Post-test | ||||||||||||||||||||
| score | 9 | 9 | 9 | 8 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 8 | 9 | 9 | 9 | 7 | 8 | 9 | 9 | 8 |
| No. | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 | 29 | 30 | 31 | 32 | 33 | 34 | 35 | 36 | 37 | 38 | 39 | 21 |
| Pre-test | ||||||||||||||||||||
| score | 9 | 9 | 9 | 8 | 9 | 8 | 8 | 9 | 9 | 9 | 9 | 9 | 9 | 6 | 9 | 9 | 5 | 7 | 9 | 9 |
| Post-test | ||||||||||||||||||||
| score | 9 | 9 | 9 | 4 | 5 | 9 | 7 | 9 | 8 | 8 | 9 | 9 | 7 | 3 | 9 | 8 | 6 | 2 | 6 | 9 |
| No. | 40 | 41 | 42 | 43 | 44 | 45 | 46 | 47 | 48 | |||||||||||
| Pre-test | ||||||||||||||||||||
| score | 9 | 8 | 9 | 8 | 9 | 8 | 8 | 9 | 9 | |||||||||||
| Post-test | ||||||||||||||||||||
| score | 9 | 8 | 9 | 5 | 9 | 7 | 9 | 7 | 9 |
| Test | Variable | Statistic Value | Degrees of Freedom | p-Value |
|---|---|---|---|---|
| Kolmogorov–Smirnov | pre-test total scores | 0.222 | 9 | 0.2 |
| post-test total scores | 0.25 | 9 | 0.11 | |
| Shapiro–Wilk | pre-test total scores | 0.903 | 9 | 0.268 |
| post-test total scores | 0.795 | 9 | 0.018 |
| 95% CI | ||||||||
|---|---|---|---|---|---|---|---|---|
| Measure | Mean | Standard Deviation | Standard Error | Lower Bound | Upper Bound | t-Statistic | Degrees of Freedom | p-Value |
| Pre-test Score | 38.67 | 3.08 | 1.03 | 36.03 | 41.30 | — | — | — |
| Post-test Score | 44.67 | 1.58 | 0.53 | 43.35 | 45.98 | — | — | — |
| Difference (Post-Pre) | 6.00 | 2.40 | 0.80 | 4.17 | 7.83 | 7.50 | 8 | <0.0001 |
| post-test total scores—pre-test total scores | |
| Z | −2.670 b |
| Asymptotic Significance (2-tailed) | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, H.C.; Chuang, H.W. A Pilot Study on AI-Powered Gamified Chatbot with OMO Strategy for Enhancing Parental Nutrition Knowledge. Digital 2025, 5, 13. https://doi.org/10.3390/digital5020013
Huang HC, Chuang HW. A Pilot Study on AI-Powered Gamified Chatbot with OMO Strategy for Enhancing Parental Nutrition Knowledge. Digital. 2025; 5(2):13. https://doi.org/10.3390/digital5020013
Chicago/Turabian StyleHuang, Han Chun, and Hsiao Wen Chuang. 2025. "A Pilot Study on AI-Powered Gamified Chatbot with OMO Strategy for Enhancing Parental Nutrition Knowledge" Digital 5, no. 2: 13. https://doi.org/10.3390/digital5020013
APA StyleHuang, H. C., & Chuang, H. W. (2025). A Pilot Study on AI-Powered Gamified Chatbot with OMO Strategy for Enhancing Parental Nutrition Knowledge. Digital, 5(2), 13. https://doi.org/10.3390/digital5020013