

Effects of Infection Control Barriers on Light Output from a Dental Light-Curing Unit Used in Various Positions



Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
- When ICBs are used or when an increase in distance/angle is unavoidable, clinicians should consider compensating for the loss in radiant exposure by increasing curing times.
- The increased opacity and thickness of ICBs reduces radiant exposure to a greater extent. When opting to use ICBs for infection control, a thinner, clear barrier has less effect on light output.
- Manufacturers’ guidelines should be followed in regard to the radiant exposure needed to cure particular resin-based dental materials. LCUs should also be tested regularly with a laboratory-grade spectrometer to ensure adequate radiant exposures are being produced.
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Calheiros, F.C.; Daronch, M.; Rueggeberg, F.A.; Braga, R.R. Degree of conversion and mechanical properties of a BisGMA:TEGDMA composite as a function of the applied radiant exposure. J. Biomed. Mater. Res. Part B Appl. Biomater. 2008, 84, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Bhamra, G.S.; Fleming, G.J. Influence of halogen irradiance on short- and long-term wear resistance of resin-based composite materials. Dent. Mater. 2009, 25, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Rueggeberg, F.A.; Cole, M.A.; Looney, S.W.; Vickers, A.; Swift, E.J. Comparison of manufacturer-recommended exposure durations with those determined using biaxial flexure strength and scraped composite thickness among a variety of light-curing units. J. Esthet. Restor. Dent. 2009, 21, 43–61. [Google Scholar] [CrossRef] [PubMed]
- Hammouda, I.M. Effect of light-curing method on wear and hardness of composite resin. J. Mech. Behav. Biomed. Mater. 2010, 3, 216–222. [Google Scholar] [CrossRef]
- Jadhav, S.; Hegde, V.; Aher, G.; Fajandar, N. Influence of light curing units on failure of directcomposite restorations. J. Conserv. Dent. 2011, 14, 225–227. [Google Scholar] [CrossRef]
- Souza-Junior, E.; Souza-Régis, M.; Alonso, R.; Freitas, A.; Sinhoreti, M.; Cunha, L. Effect of the curing method and composite volume on marginal and internal adaptation of composite restoratives. Oper. Dent. 2011, 36, 231–238. [Google Scholar] [CrossRef]
- Rueggeberg, F. Precision of hand-held dental radiometers. Quintessence Int. 1993, 24, 391–396. [Google Scholar]
- Price, R.B.; Labrie, D.; Kazmi, S.; Fahey, J.; Felix, C.M. Intra- and inter-brand accuracy of four dental radiometers. Clin. Oral Investig. 2012, 16, 707–717. [Google Scholar] [CrossRef] [PubMed]
- Shimokawa, C.A.K.; Harlow, J.E.; Turbino, M.L.; Price, R.B. Ability of four dental radiometers to measure the light output from nine curing lights. J. Dent. 2016, 54, 48–55. [Google Scholar] [CrossRef]
- Giannini, M.; André, C.B.; Gobbo, V.C.; Rueggeberg, F.A. Accuracy of irradiance and power of light-curing units measured with handheld or laboratory grade radiometers. Braz. Dent. J. 2019, 30, 397–403. [Google Scholar] [CrossRef]
- Price, R.; Ferracane, J.; Shortall, A. Light-curing units: A review of what we need to know. J. Dent. Res. 2015, 94, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Shortall, A.C.; Felix, C.J.; Watts, D.C. Robust spectrometer-based methods for characterizing radiant exitance of dental LED light curing units. Dent. Mater. 2015, 31, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Harlow, J.; Sullivan, B.; Shortall, A.; Labrie, D.; Price, R. Characterizing the output settings of dental curing lights. J. Dent. 2016, 44, 20–26. [Google Scholar] [CrossRef]
- Roulet, J.-F.; Rocha, M.G.; Shen, C.; Khudhair, M.M.; De Oliveira, D.C.R.S. Beam profile characterization of a dental light curing unit using a spectrometer-based method. Stomatol. EDU J. 2018, 5, 84–91. [Google Scholar] [CrossRef]
- Peutzfeldt, A.; Asmussen, E. Resin composite properties and energy density of light cure. J. Dent. Res. 2005, 84, 659–662. [Google Scholar] [CrossRef]
- Gritsch, K.; Souvannasot, S.; Schembri, C.; Farge, P.; Grosgogeat, B. Influence of light energy and power density on the microhardness of two nanohybrid composites. Eur. J. Oral Sci. 2008, 116, 77–82. [Google Scholar] [CrossRef]
- Jain, L.; Mehta, D.; Meena, N.; Gupta, R. Influence of light energy density, composite type, composite thickness, and postcuring phase on degree of conversion of bulk-fill composites. Contemp. Clin. Dent. 2018, 9, 147–152. [Google Scholar] [CrossRef]
- Bizzoca, M.E.; Campisi, G.; Lo Muzio, L. COVID-19 pandemic: What changes for dentists and oral medicine experts? A narrative review and novel approaches to infection containment. Int. J. Environ. Res. Public Health 2020, 17, 3793. [Google Scholar] [CrossRef]
- Brokos, I.; Turner, S.; Santini, A. The effect of disposable infection control sleeves on the total energy delivered by dental LCUs. Prim. Dent. J. 2012, 1, 11–16. [Google Scholar] [CrossRef]
- AlShaafi, M.M. Effects of different infection control methods on the intensity output of LED light-curing units. King Saud Univ. J. Dent. Sci. 2013, 4, 27–31. [Google Scholar] [CrossRef]
- Konerding, K.L.; Heyder, M.; Kranz, S.; Guellmar, A.; Voelpel, A.; Watts, D.C.; Jandt, K.D.; Sigusch, B.W. Study of energy transfer by different light curing units into a class III restoration as a function of tilt angle and distance, using a MARC Patient Simulator (PS). Dent. Mater. 2016, 32, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Sword, R.J.; Do, U.N.; Chang, J.H.; Rueggeberg, F. Effect of curing light barriers and light types on radiant exposure and composite conversion. J. Esthet. Restor. Dent. 2016, 28, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Suliman, A.; Abdo, A.; Elmasmari, H.A. Effect of contamination, damage and barriers on the light output of light-curing units. Open Dent. J. 2019, 13, 196–202. [Google Scholar] [CrossRef]
- Soares, C.J.; Braga, S.S.L.; Ribeiro, M.T.H.; Price, R.B. Effect of infection control barriers on the light output from a multi-peak light curing unit. J. Dent. 2020, 103, 103503. [Google Scholar] [CrossRef] [PubMed]
- Price, R.B.; Labrie, D.; Whalen, J.M.; Felix, C.M. Effect of distance on irradiance and beam homogeneity from 4 light-emitting diode curing units. J. Can. Dent. Assoc. 2011, 77, b9. [Google Scholar]
- Beolchi, R.S.; Moura-Netto, C.; Palo, R.M.; Torres, C.R.G.; Pelissier, B. Changes in irradiance and energy density in relation to different curing distances. Braz. Oral Res. 2015, 29, 1–7. [Google Scholar] [CrossRef]
- Al-Zain, A.; Eckert, G.; Platt, J. The influence of distance on radiant exposure and degree of conversion using different light-emitting-diode curing units. Oper. Dent. 2019, 44, E133–E144. [Google Scholar] [CrossRef]
- Price, R.B.T.; McLeod, M.E.; Felix, C.M. Quantifying light energy delivered to a Class I restoration. J. Can. Dent. Assoc. 2010, 76, a23. [Google Scholar]
- Mutluay, M.M.; Rueggeberg, F.A.; Price, R.B. Effect of using proper light-curing techniques on energy delivered to a Class 1 restoration. Quintessence Int. 2014, 45, 549–556. [Google Scholar] [CrossRef]
- Soares, C.; De Bragança, G.F.; Pereira, R.A.D.S.; Rodrigues, M.D.P.; Braga, S.S.L.; Oliveira, L.R.S.; Giannini, M.; Price, R. Irradiance and radiant exposures delivered by LED light-curing units used by a left and right-handed operator. Braz. Dent. J. 2018, 29, 282–289. [Google Scholar] [CrossRef]
- Coutinho, M.; Takayassu, R.N.; Leme, A.A.; Soares, G.P.; Trevizam, N.C. Distance and protective barrier effects on the composite resin degree of conversion. Contemp. Clin. Dent. 2013, 4, 152. [Google Scholar] [CrossRef]
- Chang, H.-S.; Lee, S.-R.; Hong, S.-O.; Ryu, H.-W.; Song, C.-K.; Min, K.-S. Effect of infection control barrier thickness on light curing units. J. Korean Acad. Conserv. Dent. 2010, 35, 368–373. [Google Scholar] [CrossRef]
- Al-Marzok, M.I. The effect of wrapping of light-cure tips on the cure of composite resin. Eur. J. Gen. Dent. 2012, 1, 183–186. [Google Scholar] [CrossRef]
- Price, R.B.T.; Fahey, J.; Felix, C.M. Knoop microhardness mapping used to compare the efficacy of LED, QTH and PAC curing lights. Oper. Dent. 2010, 35, 58–68. [Google Scholar] [CrossRef]
- Price, R.B. Light curing in dentistry. Dent. Clin. N. Am. 2017, 61, 751–778. [Google Scholar] [CrossRef]
- Khaksaran, N.K.; Kashi, T.J.; Rakhshan, V.; Zeynolabedin, Z.S.; Bagheri, H. Kinetics of pulpal temperature rise during light curing of 6 bonding agents from different generations, using light emitting diode and quartz-tungsten-halogen units: An in-vitro simulation. Dent. Res. J. 2015, 12, 173–180. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| ICB | Correct | Incorrect | Difference | % Difference |
|---|---|---|---|---|
| Control—No ICB | 13.12 | n/a | n/a | n/a |
| Pinnacle | 11.59 | 11.83 | 0.24 | 2.1% |
| CMS | 11.76 | 12.34 | 0.58 | 4.9% |
| SmartLite | 12.31 | 11.85 | −0.46 | −3.7% |
| Cling Wrap | 12.48 | 12.13 | −0.35 | −2.8% |
| Aluro | 12.29 | 12.44 | 0.15 | 1.2% |
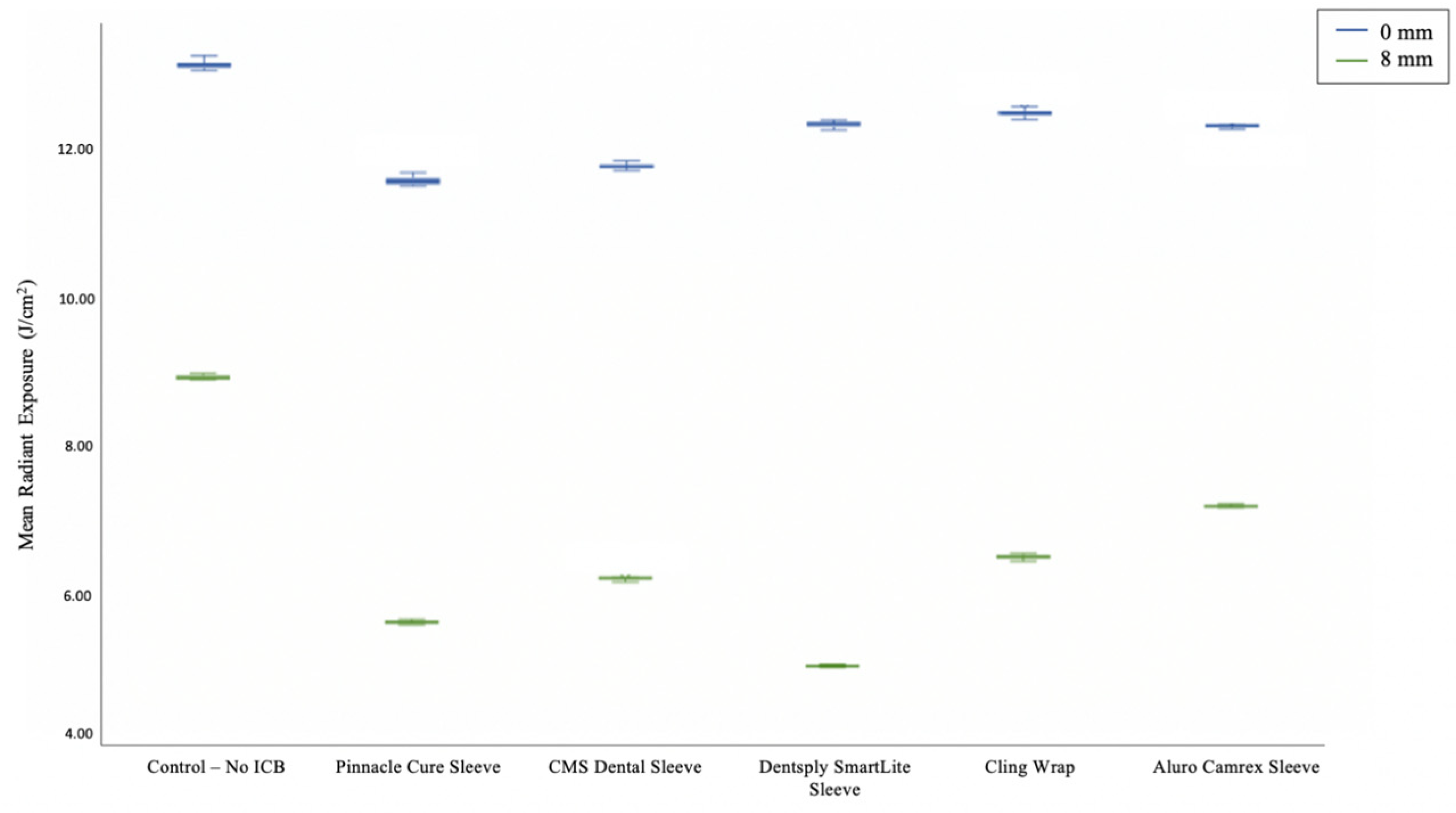
| Distance (mm) | Radiant Exposure at Control | Control—No ICB | Pinnacle | CMS | SmartLite | Cling Wrap | Aluro | Mean % Reduction All Groups |
|---|---|---|---|---|---|---|---|---|
| 0 | 13.12 | n/a | n/a | n/a | n/a | n/a | n/a | n/a |
| 2 | 11.50 | −12.4% | −17.0% | −10.4% | −12.5% | −10.1% | −19.3% | −16.5% |
| 4 | 10.88 | −17.1% | −22.3% | −15.4% | −23.0% | −19.4% | −25.7% | −26.4% |
| 6 | 9.80 | −25.3% | −38.1% | −29.6% | −42.5% | −35.7% | −32.0% | −37.5% |
| 8 | 8.93 | −31.9% | −51.2% | −47.8% | −58.9% | −47.7% | −41.3% | −47.5% |
| Angle (°) | Radiant Exposure at Control | Control—No ICB | Pinnacle | CMS | SmartLite | Cling Wrap | Aluro | Mean % Reduction All Groups |
|---|---|---|---|---|---|---|---|---|
| 0 | 13.12 | n/a | n/a | n/a | n/a | n/a | n/a | n/a |
| 10 | 11.57 | −11.8% | −7.8% | −1.0% | −3.4% | −2.0% | −1.5% | −4.7% |
| 20 | 10.29 | −21.6% | −19.2% | −10.2% | −12.0% | −6.2% | −7.6% | −13.8% |
| 30 | 10.23 | −22.0% | −15.8% | −12.2% | −19.6% | −8.8% | −10.2% | −19.2% |
| 40 | 7.98 | −39.1% | −37.0% | −35.6% | −32.0% | −24.3% | −29.7% | −36.7% |
| ICB/ Angle/ Distance | ICB Effect | Angle Effect | Distance Effect | Combined Effect of Individual Variables | Cumulative Effect | Difference |
|---|---|---|---|---|---|---|
| Pinnacle/10°/2 mm | 0.38 | 0.50 | 1.56 | 2.44 | 4.00 | 1.56 |
| Pinnacle/20°/4 mm | 0.84 | 1.21 | 1.57 | 3.62 | 5.33 | 1.70 |
| Pinnacle/30°/6 mm | 1.76 | 1.44 | 4.04 | 7.24 | 7.40 | 0.16 |
| Pinnacle/40°/8 mm | 1.40 | 1.88 | 3.53 | 6.81 | 9.35 | 2.54 |
| CMS/10°/2 mm | −0.80 | 0.25 | 1.35 | 0.80 | 2.83 | 2.03 |
| CMS/20°/4 mm | 0.95 | 2.27 | 2.88 | 6.10 | 5.44 | −0.66 |
| CMS/30°/6 mm | 1.23 | 2.03 | 4.07 | 7.33 | 6.87 | −0.46 |
| CMS/40°/8 mm | 1.67 | 2.77 | 4.08 | 8.52 | 9.62 | 1.10 |
| Aluro/10°/2 mm | −1.00 | −0.57 | 1.62 | 0.05 | 2.63 | 2.58 |
| Aluro/20°/4 mm | 0.25 | 0.88 | 2.98 | 4.11 | 4.74 | 0.63 |
| Aluro/30°/6 mm | 1.29 | 2.17 | 4.85 | 8.31 | 6.93 | −1.38 |
| Aluro/40°/8 mm | 0.81 | 2.86 | 4.29 | 7.96 | 8.77 | 0.81 |
| SmartLite/10°/2 mm | −0.46 | 0.83 | 1.95 | 2.32 | 3.17 | 0.85 |
| SmartLite/20°/4 mm | 0.95 | 1.80 | 3.14 | 5.89 | 5.43 | −0.46 |
| SmartLite/30°/6 mm | 1.72 | 1.32 | 4.13 | 7.17 | 7.35 | 0.18 |
| SmartLite/40°/8 mm | 0.78 | 0.68 | 3.99 | 5.45 | 8.74 | 3.29 |
| Cling Wrap/10°/2 mm | −1.40 | 0.32 | 1.33 | 0.25 | 2.22 | 1.97 |
| Cling Wrap/20°/4 mm | −0.12 | 1.32 | 2.96 | 4.16 | 4.37 | 0.21 |
| Cling Wrap/30°/6 mm | 0.19 | 0.73 | 4.08 | 5.00 | 5.83 | 0.83 |
| Cling Wrap/40°/8 mm | 0.42 | 1.78 | 4.70 | 6.90 | 8.37 | 1.47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Zee, J.; Tawse-Smith, A.; Ma, S. Effects of Infection Control Barriers on Light Output from a Dental Light-Curing Unit Used in Various Positions. Oral 2023, 3, 166-175. https://doi.org/10.3390/oral3020015
van der Zee J, Tawse-Smith A, Ma S. Effects of Infection Control Barriers on Light Output from a Dental Light-Curing Unit Used in Various Positions. Oral. 2023; 3(2):166-175. https://doi.org/10.3390/oral3020015
Chicago/Turabian Stylevan der Zee, Jitte, Andrew Tawse-Smith, and Sunyoung Ma. 2023. "Effects of Infection Control Barriers on Light Output from a Dental Light-Curing Unit Used in Various Positions" Oral 3, no. 2: 166-175. https://doi.org/10.3390/oral3020015
APA Stylevan der Zee, J., Tawse-Smith, A., & Ma, S. (2023). Effects of Infection Control Barriers on Light Output from a Dental Light-Curing Unit Used in Various Positions. Oral, 3(2), 166-175. https://doi.org/10.3390/oral3020015