
The Experiences of Patients Treated with Complete Removable Dentures: A Systematic Literature Review of Qualitative Research





Abstract
:1. Introduction
2. Methods
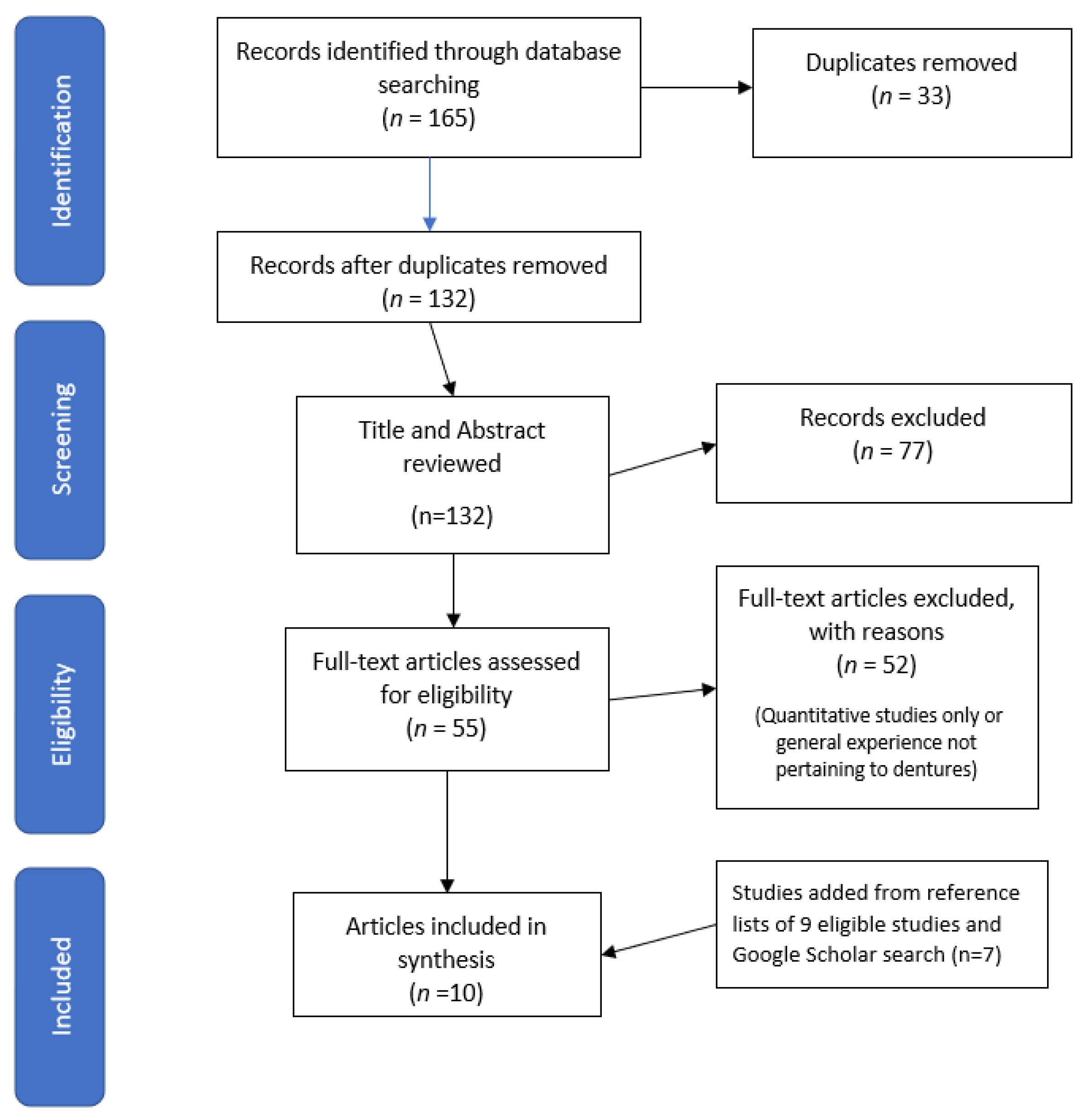
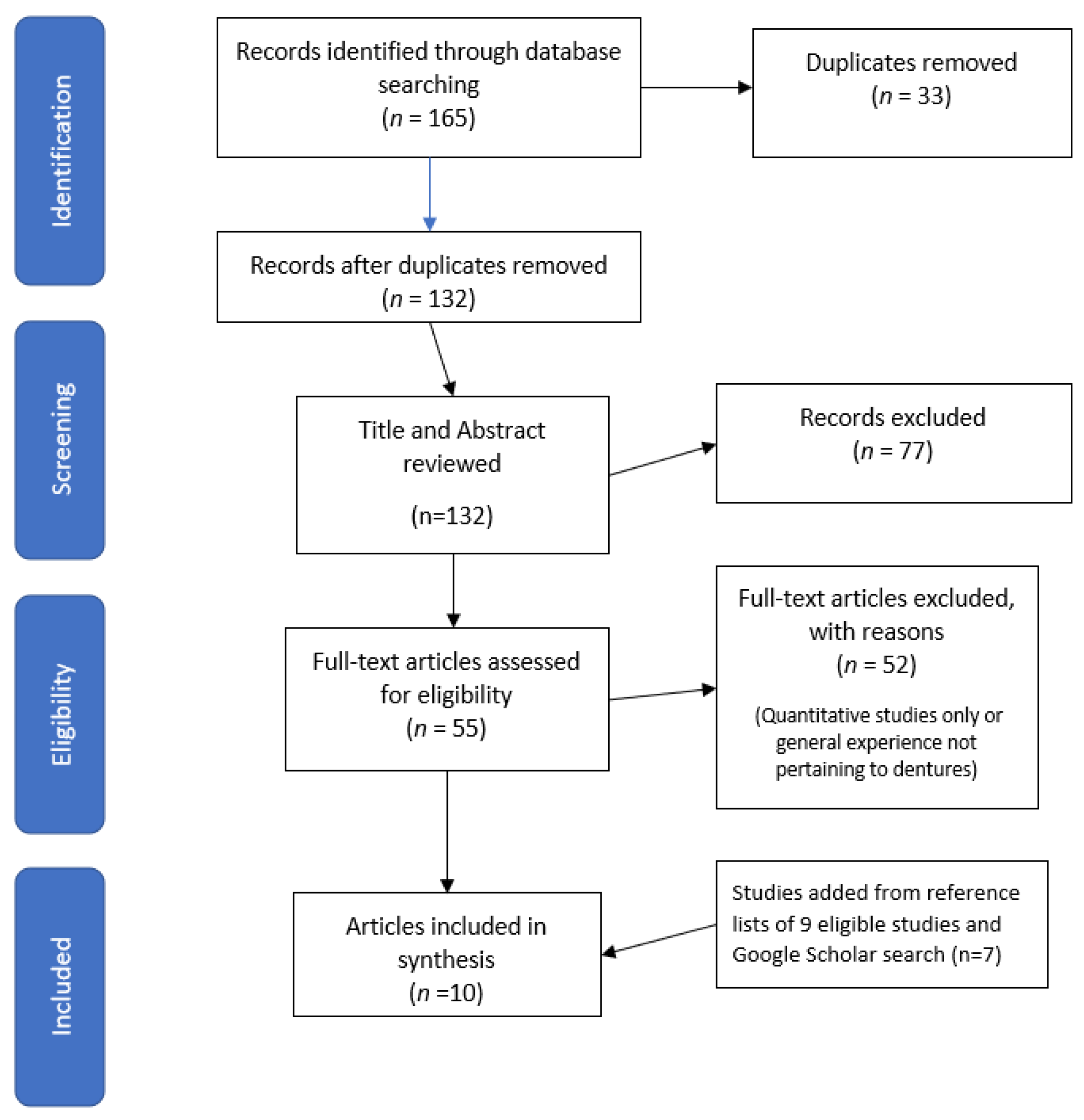
2.1. Search Strategy
2.2. Study Selection
2.3. Quality Assessment
3. Results
3.1. Themes
3.2. Emotional Factors
3.3. Physical Factors
3.4. Psychological Processes and Affective Responses
3.5. Social Interaction
3.6. Denture Hygiene and Maintenance Factors
3.7. Access and Cost Related Factors
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Article | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Item | Ellis et al., 2011 [19] | Osman et al., 2014 [25] | Narby et al., 2012 [23] | Thomason et al., 2012 [27] | Nodenram et al., 2013 [5] | Grey, et al., 2013 [20] | Rousseau, et al., 2014 [26] | Kashbour et al., 2015 [21] | Nogueira, et al., 2019 [24] | Lima de Paula et al., 2019 [22] |
| Was there a clear statement of the aims of the research? | + | + | + | + | + | + | + | + | + | + |
| Is the qualitative methodology appropriate? | + | + | + | + | + | + | + | + | ||
| Was the research design appropriate to address the aims of the research? | + | + | + | + | + | + | + | + | + | + |
| Was the recruitment strategy appropriate to the aims of the research? | + | + | + | + | + | - | + | + | + | + |
| Were the data collected in a way that addressed the research issues? | - | + | + | + | + | + | + | + | + | + |
| Has the relationship between researcher and participants been adequately considered? | + | + | ct | - | ct | ct | ct | + | ||
| Have ethical issues been taken into consideration? | + | + | + | - | - | + | + | + | ||
| Was the data analysis sufficiently rigorous? | + | + | + | + | + | + | + | + | + | + |
| Is there a clear statement of finding | + | + | + | + | + | + | + | + | + | + |
| How valuable is the research? | + | + | + | + | + | + | + | + | + | + |
| TOTAL | 9 | 10 | 9 | 7 | 7 | 7 | 8 | 9 | 9 | 10 |
Appendix B
| No | Author and Year | Study Type | Country | Sample | Data Collection | Theme Outcomes | Comments | Quality Appraisal Score |
|---|---|---|---|---|---|---|---|---|
| 1 | Ellis et al., 2011 [19] | Qualitative | UK and Canada | 30 participants | Semi structured interviews, focus groups | Theme Post-surgical denture-wearing; gums cut, leaving dentures in despite. cleaning of dentures | Embarrassed to go without dentures. | 9 |
| 2 | Osman et al., 2012 [25] |
| New Zealand | 16 ISODs participants | In-depth semi-structured interviews |
|
| 10 |
| 3 | Narby et al., 2012 [23] | Qualitative Grounded theory | Sweden | 10 participants Some having worn removable dentures | Constant comparative | Journey from social stigma to exhilaration: becoming the insecure person. becoming determined person; becoming the person I once was acquiring more realistic perspective. |
| 9 |
| 4 | Thomason et al., 2012 [27] | Systematic review of mixed articles | UK | 10 articles |
|
| 7 | |
| 5 | Nordenram et al., 2013 [5] | Systematic review literature review | Sweden | 9 articles |
|
| 7 | |
| 6 | Grey et al., 2013 [20] | Qualitative Semi-structure telephone interviews | UK | 9 participants |
|
| 7 | |
| 7 | Rousseau et al., 2014 [26] | Qualitative | UK | 29 participants including denture wearers | Semi structure |
| CCDs problematic experiences prompted Pts to seek dental implants
| 8 |
| 8 | Kashbour et al., 2015 [21] | Systematic review on qualitative research -textual narrative synthesis | UK | 10 articles | To identify and summarise qualitative studies relating to patients’ experience of dental implant treatment (DIT) at various treatment stages | ISODs patients placed functional and social improvement as main motivation to treatment. |
| 9 |
| 9 | Nogueira et al., 2019 [24] | Qualitative | Brazil | 13 participants | Thematic analysis Focus group | Four main themes emerged:
|
| 9 |
| 10 | Lima de Paula et al., 2019 [22] | Qualitative | Brazil | 11 participants | Semi-structured interviews | Living with complete dentures: problems in adaptation period; interpersonal relationship; functional gains | Very difficult; access; cost; avoidance of food; chewing difficulty; living lower denture out; work on your psychology; you have to be calm; getting used to it. Effect on self-esteem; recover yourself; complete with dentures; pray; attend parties; meet with relatives; chewing recovery; eating everything | 10 |
References
- Todd, A.L.; Nutbeam, D. Involving consumers in health research: What do consumers say? Public Health Res. Pract. 2018, 28, e2821813. [Google Scholar] [CrossRef] [PubMed]
- Australian Commission on Safety and Quality in Healthcare (ACSQHC). Safety and Quality Improvement Guide. Standard 2 Partnering with Consumers. 2012. Available online: https://www.safetyandquality.gov.au/sites/default/files/migrated/Standard2_Oct_2012_WEB.pdf (accessed on 20 July 2020).
- Nilsen, E.S.; Myrhaug, H.T.; Johansen, M.; Oliver, S.; Oxman, A.D. Methods of consumer involvement in developing healthcare policy and research, clinical practice guidelines and patient information material. Cochrane Database Syst. Rev. 2006, 2006, CD004563. [Google Scholar] [CrossRef] [PubMed]
- Bower, E.; Scambler, S. The contributions of qualitative research towards dental public health practice. Community Dent. Oral Epidemiol. 2007, 35, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Nordenram, G.; Davidson, T.; Gynther, G.; Helgesson, G.; Hultin, M.; Jemt, T.; Lekholm, U.; Nilner, K.; Norlund, A.; Rohlin, M.; et al. Qualitative studies of patients’ perceptions of loss of teeth, the edentulous state and prosthetic rehabilitation: A systematic review with meta-synthesis. Acta Odontol. Scand. 2012, 71, 937–951. [Google Scholar] [CrossRef] [PubMed]
- Lambert, H.; McKevitt, C. Education and debate Anthropology in health research. From qualitative methods to multidisci-plinarity. BMJ 2002, 325, 210–213. [Google Scholar] [CrossRef]
- Tran, J.; Wright, F.; Takara, S.; Shu, C.C.; Chu, S.Y.; Naganathan, V.; Hirani, V.; Blyth, F.M.; Le Couteur, D.G.; Waite, L.M.; et al. Oral health behaviours of older Australian men: The Con-cord Health and Ageing in Men Project. Aust. Dent. J. 2019, 64, 246–255. [Google Scholar] [CrossRef]
- Van Der Wijk, P.; Bouma, J.; A Van Waas, M.; Van Oort, R.P.; Rutten, F.F. The cost of dental implants as compared to that of conventional strategies. Int. J. Oral Maxillofac. Implant. 1998, 13, 546–553. [Google Scholar]
- Chrisopoulos, S.; Hardford, J. Oral Health and Dental Care in Australia: Key Facts and Figures; Australian Insitute of Health and Welfare: Canberra, Australia, 2012.
- Heydecke, G.; Tedesco, L.A.; Kowalski, C.; Inglehart, M.R. Complete dentures and oral health-related quality of life—Do coping styles matter? Community Dent. Oral Epidemiol. 2004, 32, 297–306. [Google Scholar] [CrossRef]
- Al Quran, F.; Clifford, T.; Cooper, C.; Lamey, P.J. Influence of Psychological Factors on the Acceptance of Complete Dentures. Gerodontology 2001, 18, 35–40. [Google Scholar] [CrossRef]
- Rathi, A.; Banerjee, R.; Radke, U.; Lahoti, S.; Sahni, S. Knowledge and Attitude about Relining of Complete Dentures in Clinical Practice: A Cross-Sectional Study. J. Indian Prosthodont. Soc. 2018, 18, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Kranjcic, J.; Kostelic-Stunic, M.; Vojvodic, D.; Komar, D.; Mehulic, K. Patient’s satisfaction with removable dentures after relining. Med. Glas. 2012, 9, 376–382. [Google Scholar]
- Schierano, G.; Arduino, E.; Bosio, E.; Preti, G. The Influence of Selective Grinding on the Thickness Discrimination Threshold of Patients Wearing Complete Dentures. J. Oral Rehabil. 2002, 29, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Knott, N. A tale of two dentures. Fac. Dent. J. 2016, 7, 68–73. [Google Scholar] [CrossRef]
- Celebic, A.; Knezovic-Zlataric, D.; Papic, M.; Carek, V.; Baucic, I.; Stipetic, J. Factors Related to Patient Satisfaction With Complete Denture Therapy. J. Gerontol. Med. Sci. 2003, 58, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Mendes, F.A.; Borges, T.D.F.; Gonçalves, L.C.; de Oliveira, T.R.; do Prado, C.J.; das Neves, F.D. Effects of new implant-retained overdentures on masticatory function, satisfaction and quality of LIFE. Acta Odontol. Latinoam. 2016, 29, 123–129. [Google Scholar] [PubMed]
- Marchini, L. Patients’ satisfaction with complete dentures: An update. Braz. Dent. Sci. 2014, 17, 5–16. [Google Scholar] [CrossRef]
- Ellis, J.S.; Levine, A.; Bedos, C.; Mojon, P.; Rosberger, Z.; Feine, J.; Thomason, J.M. Refusal of Implant Supported Mandibular Overdentures by Elderly Patients. Gerodontology 2011, 28, 62–68. [Google Scholar] [CrossRef]
- Grey, E.B.; Harcourt, D.; O’Sullivan, D.; Buchanan, H.; Kilpatrick, N.M. A qualitative study of patients’ motivations and expectations for dental implants. Br. Dent. J. 2013, 214, E1. [Google Scholar] [CrossRef]
- Kashbour, W.A.; Rousseau, N.S.; Ellis, J.S.; Thomason, J.M. Patients’ experiences of dental implant treatment: A literature review of key qualitative studies. J. Dent. 2015, 43, 789–797. [Google Scholar] [CrossRef]
- Lima de Paula, L.M.L.; Sampaio, A.A.; Costa, J.G.; Gomes, V.E.; Ferreira, E.F.E.; Ferreira, R.C. The course from tooth loss to successful rehabilitation with denture: Feelings influenced by socioeconomic status. SAGE Open Med. 2019, 7, 2050312119874232. [Google Scholar] [CrossRef]
- Narby, B.; Hallberg, U.; Bagewitz, I.C.; Söderfeldt, B. Grounded theory on factors involved in the decision-making processes of patients treated with implant therapy. Int. J. Prosthodont. 2012, 25, 270–278. [Google Scholar]
- Nogueira, T.E.; Dias, D.R.; Rios, L.F.; Silva, A.L.M.; Jordao, L.M.R.; Leles, C.R. Perceptions and experiences of patients following treatment with single-implant mandibular overdentures: A qualitative study. Clin. Oral Implants Res. 2019, 30, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Osman, R.B.; Morgaine, K.C.; Duncan, W.; Swain, M.V.; Ma, S. Patients’ perspectives on zirconia and titanium implants with a novel distribution supporting maxillary and mandibular overdentures: A qualitative study. Clin. Oral Implants Res. 2014, 25, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, N.; Steele, J.; May, C.; Exley, C. ‘Your whole life is lived through your teeth’: Biographical disruption and experiences of tooth loss and replacement. Sociol. Health Illn. 2014, 36, 462–476. [Google Scholar] [CrossRef] [PubMed]
- Thomason, J.M.; Kelly, S.A.; Bendkowski, A.; Ellis, J.S. Two implant retained overdentures--a review of the literature supporting the McGill and York consensus statements. J. Dent. 2012, 40, 22–34. [Google Scholar] [CrossRef]
- Zhang, Y.A. Study on the Effects of Emotional Factors on Middle School Students in English Learning. Adv. Soc. Sci. Educ. Humanit. Res. 2018, 89, 679–684. [Google Scholar]
- Carr, A.B.; McGivney, G.; Brown, D. McCracken’s Removable Partial Prosthodontics, 11th ed.; Elsevier/Mosby: St. Louis, MI, USA, 2005. [Google Scholar]
- Stansfeld, S.; Rasul, F. Psychosocial Factors, Depression and Illness. In Depression and Physical Illness; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Long, J.; Cumming, J. Psychosocial Variables. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 1585–1587. [Google Scholar]
- Vandegrift, R.; Bateman, A.C.; Siemens, K.N.; Nguyen, M.; Wilson, H.E.; Green, J.L.; Van Den Wymelenberg, K.G.; Hickey, R.J. Cleanliness in context: Reconciling hygiene with a modern microbial perspective. Microbiome 2017, 5, 76. [Google Scholar] [CrossRef]
- Cakan, U.; Yuzbasioglu, E.; Kurt, H.; Kara, H.; Turunç, R.; Akbulut, A.; Aydın, K. Assessment of hygiene habits and attitudes among removable partial denture wearers in a university hospital. Niger. J. Clin. Pract. 2015, 18, 511–515. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Monitoring Access to Personal Health Care Services. Access to Health Care in America; Millman, M., Ed.; National Academies Press: Washington, DC, USA, 1993. [CrossRef]
- Isman, R.; Isman, B. Oral Health America White Paper: Access to Oral Health Services in the U.S. 1997 and Beyond; Oral Health America: Chicago, IL, USA, 1997. [Google Scholar]
- Dolan, T.A.; Atchison, K.; Huynh, T.N. Access to Dental Care Among Older Adults in the United States. J. Dent. Educ. 2005, 69, 961–974. [Google Scholar] [CrossRef]
- Oben, P. Understanding the Patient Experience: A Conceptual Framework. J. Patient Exp. 2020, 7, 906–910. [Google Scholar] [CrossRef]
- Shetty, M.S.; Panchaml, G.S.; Shenoy, K.K. Denture Acceptance among Newly Rehabilitated Elderly Population in Old Age Homes in South India. Contemp. Clin. Dent. 2015, 6, S90–S93. [Google Scholar] [CrossRef] [PubMed]
- Thompson, B.; Cooney, P.; Lawrence, H.; Ravaghi, V.; Quiñone, C. The potential oral health impact of cost barriers to dental care: Findings from a Canadian population-based study. BMC Oral Health 2014, 14, 78. [Google Scholar] [CrossRef] [PubMed]
- Vieira, C.L.; Caramelli, B. The history of dentistry and medicine relationship: Could the mouth finally return to the body? Oral Dis. 2009, 15, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Simon, L. Overcoming Historical Separation between Oral and General Health Care: Interprofessional Collaboration for Promoting Health Equity. AMA J. Ethics 2016, 18, 941–949. [Google Scholar]
- Srinivasan, K. Holistic Dentistry: Natural Approaches to Oral Health. Saudi Sch. Bull. 2015, 1, 267–270. [Google Scholar]
- Pietrabissa, G.; Simpson, S.G. Psychological Consequences of Social Isolation During COVID-19 Outbreak. Front. Psychol. 2020, 11, 2201. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of Exercise Is a Major Cause of Chronic Diseases. Compr. Physiol. 2012, 2, 1143. [Google Scholar]
- Braveman, P.; Gottlieb, L. The Social Determinants of Health: It’s Time to Consider the Causes of the Causes. Public Health Rep. 2014, 129 (Suppl. 2), 19–31. [Google Scholar] [CrossRef]
- Fiske, J.; Davis, D.; Horrocks, P. A Self Help Group for Complete Denture Wearers. Br. Dent. J. 1995, 178, 18–22. [Google Scholar] [CrossRef]
| Concept 1 | Concept 2 | Concept 3 | Database | |
|---|---|---|---|---|
| Key concepts | Denture patients | Experiences | Study Design | |
| Free text terms | Denture patient * Denture client * Denture wearer * Denture recipient * Overdenture patient * Overdenture client * Overdenture wearer * Overdenture recipient * | Experience * Feeling * Opinion * knowledge Perspective * Expectation * Attitude | Qualitative Mixed research | PubMed CINHAL Scopus |
| MeSH terms | Dentures | Patient Satisfaction Perception * Attitude * Pain | PubMed CINHAL Scopus |
| Item | Questions |
|---|---|
| 1 | Was there a clear statement of the aims of the research? |
| 2 | Is the qualitative methodology appropriate? |
| 3 | Was the research design appropriate to address the aims of the research? |
| 4 | Was the recruitment strategy appropriate to the aims of the research? |
| 5 | Were the data collected in a way that addressed the research issues? |
| 6 | Has the relationship between researcher and participants been adequately considered? |
| 7 | Have ethical issues been taken into consideration? |
| 8 | Was the data analysis sufficiently rigorous? |
| 9 | Is there a clear statement of finding |
| 10 | How valuable is the research? |
 | Free Codes | Peace with dentures Unhappy to remove Normalcy Restoration Insecurity Denture wearing Endurance Disliking of denture wearing | Functionality Intrusiveness of dentures Loose dentures Dentures and foreign objects Denture insertion Discomfort | Quality of life Successful adaptation Patient satisfaction Old age disliked Self-esteem Denture wearing mystified Persistence pays Psychological | Socialisation impacted Socialisation enhanced Socialisation limited | Cleaning of dentures Contaminated dentures | Dentures unaffordable Teeth left to rot as too costly to go to dentist ISODs too costly Too far to get to dentist |
| Descriptive Themes | Discomfort Anxiety Helplessness Satisfaction Shameful | Physical pain Resisting Stable and retentive Comfortable Endurance Denture removal Self-management dentures | Confidence Denture dependency Negative perception Denture adaptation | Self-consciousness Privacy | Cleanliness | Access Affordability Cost | |
| Final (Analytical Themes | Emotional Factors | Physical Factors | Psychological and Affective Response | Social interaction | Hygiene and Maintenance | Access and Cost |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chakaipa, S.; Prior, S.J.; Pearson, S.; Van Dam, P.J. The Experiences of Patients Treated with Complete Removable Dentures: A Systematic Literature Review of Qualitative Research. Oral 2022, 2, 205-220. https://doi.org/10.3390/oral2030020
Chakaipa S, Prior SJ, Pearson S, Van Dam PJ. The Experiences of Patients Treated with Complete Removable Dentures: A Systematic Literature Review of Qualitative Research. Oral. 2022; 2(3):205-220. https://doi.org/10.3390/oral2030020
Chicago/Turabian StyleChakaipa, Shamiso, Sarah J. Prior, Sue Pearson, and Pieter J. Van Dam. 2022. "The Experiences of Patients Treated with Complete Removable Dentures: A Systematic Literature Review of Qualitative Research" Oral 2, no. 3: 205-220. https://doi.org/10.3390/oral2030020
APA StyleChakaipa, S., Prior, S. J., Pearson, S., & Van Dam, P. J. (2022). The Experiences of Patients Treated with Complete Removable Dentures: A Systematic Literature Review of Qualitative Research. Oral, 2(3), 205-220. https://doi.org/10.3390/oral2030020