
Maxillary Distomolar Associated with Dentigerous Cyst: An Unusual Entity



Abstract
:1. Introduction
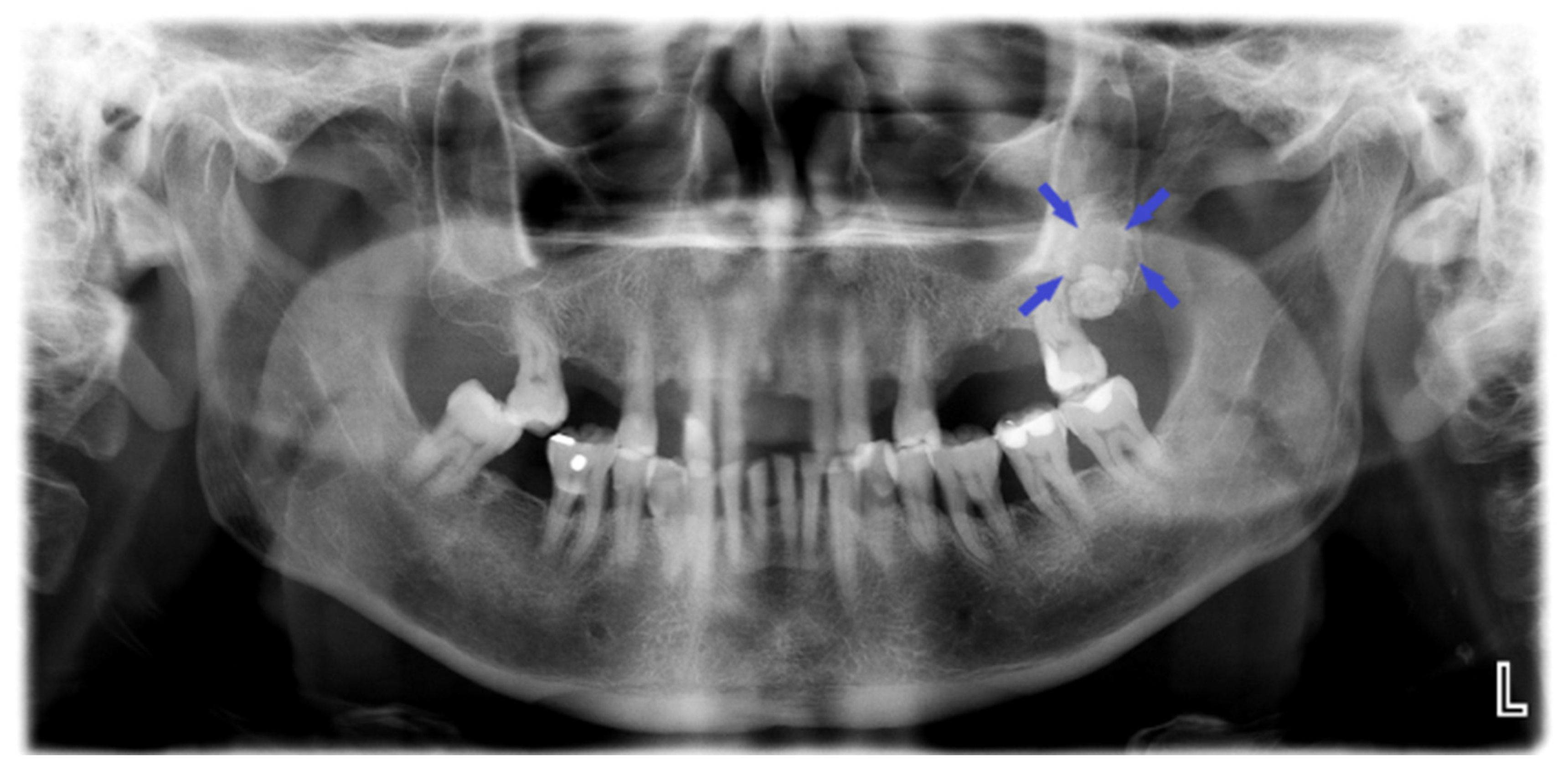
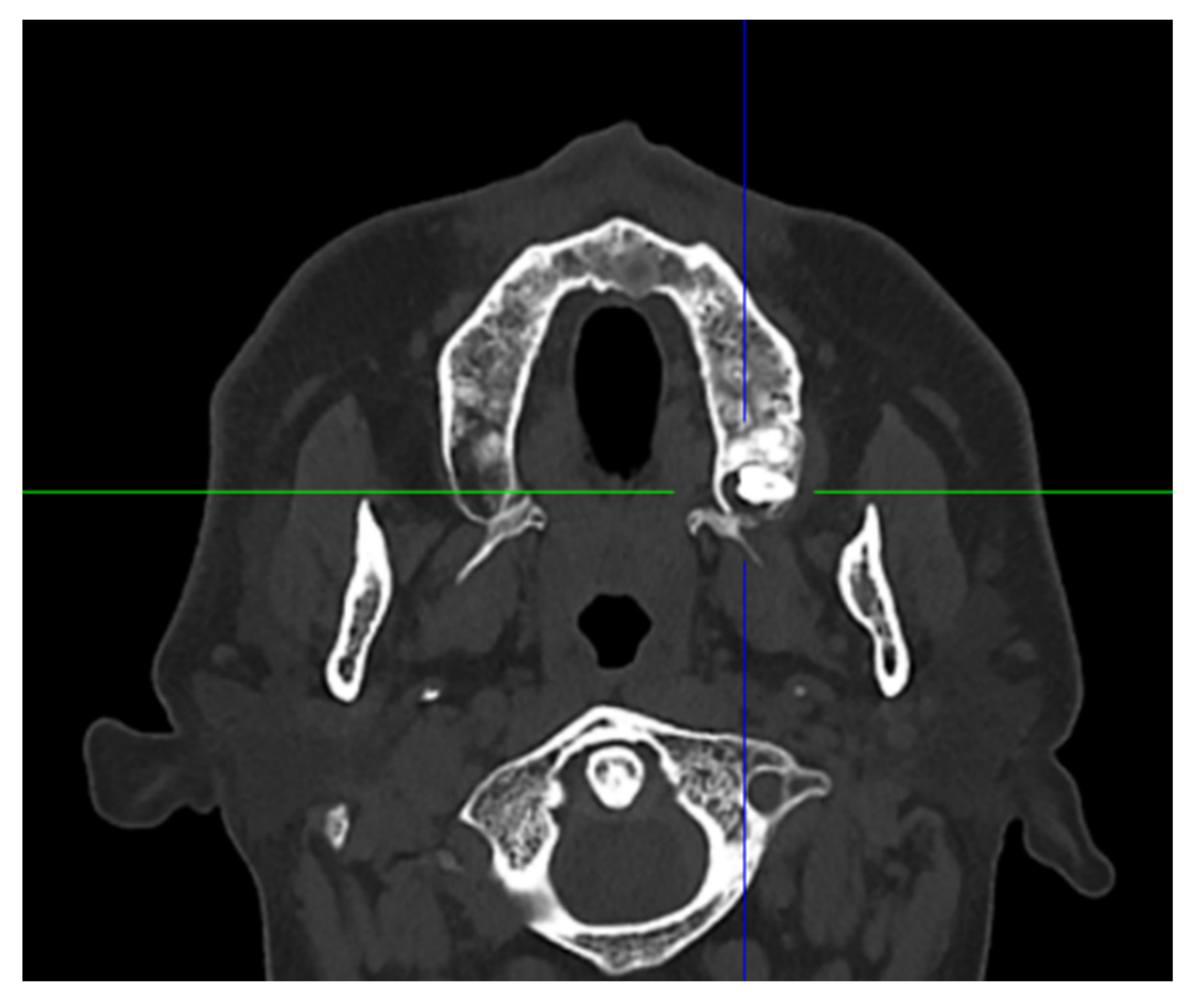
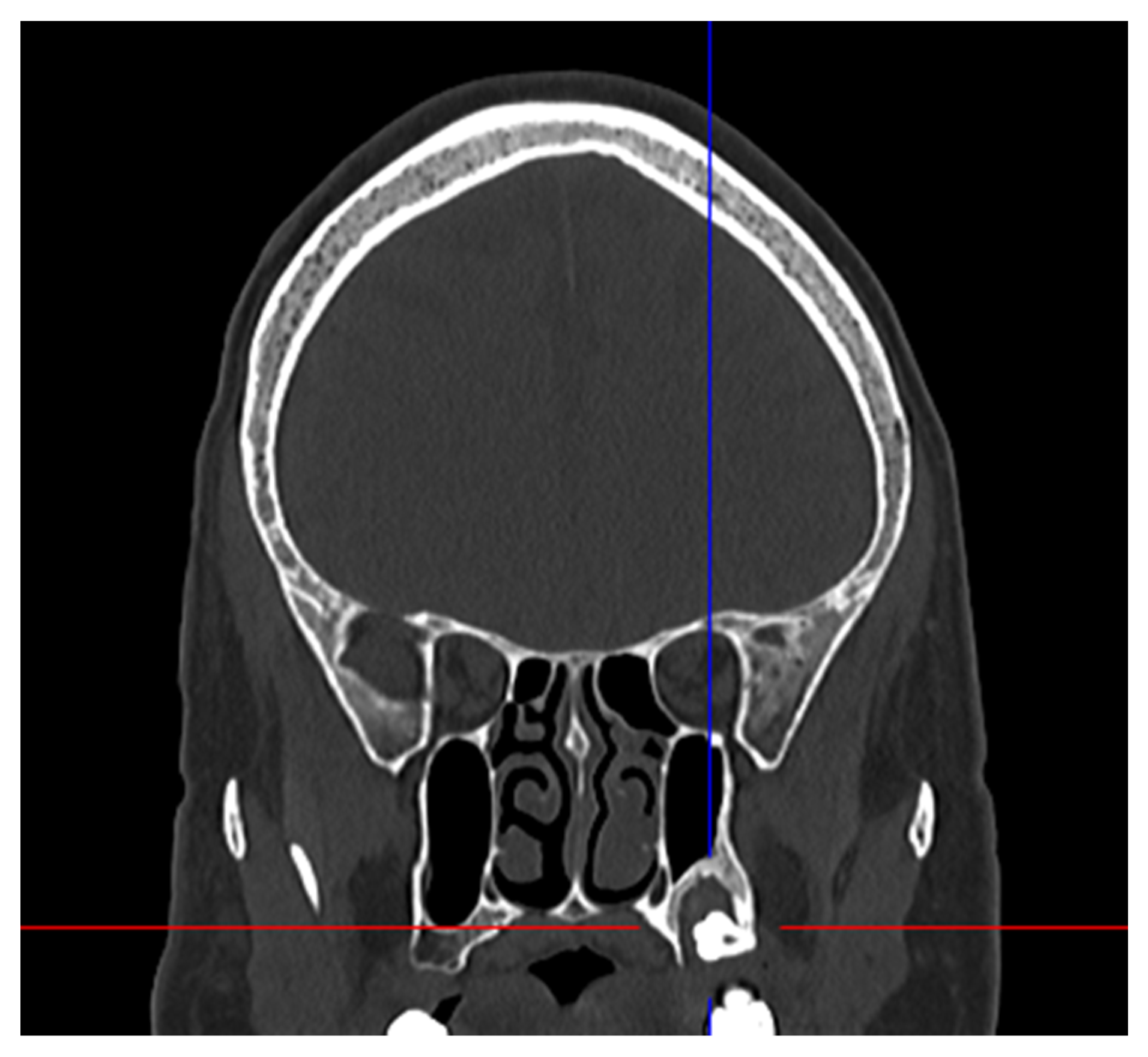
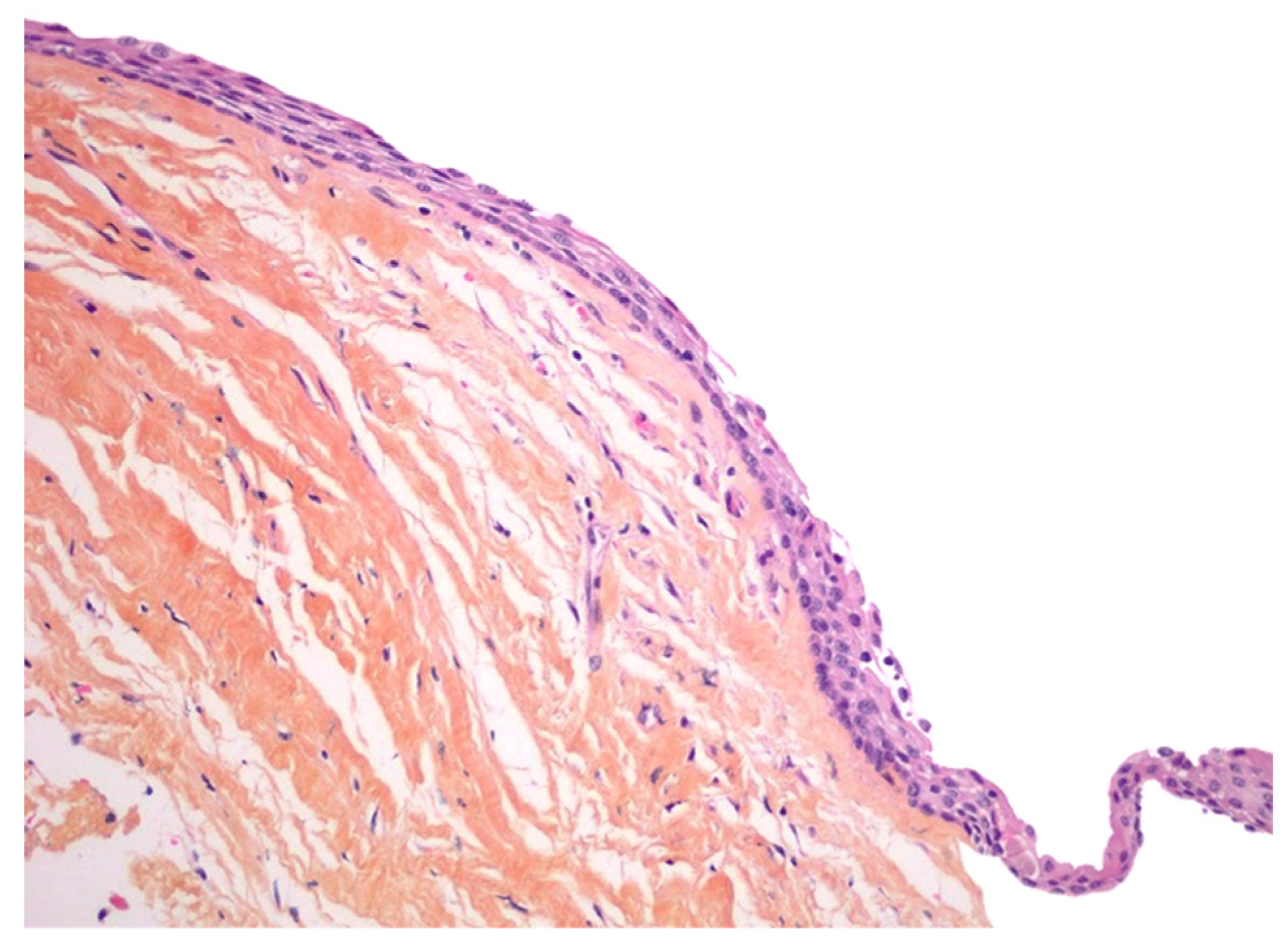
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arandi, N. Distomolars: An overview and 3 case reports. Dent. Oral Craniofac. Res. 2017, 4, 1–3. [Google Scholar] [CrossRef]
- Kurt, H.; Suer, T.B.; Senel, B.; Avsever, H. A retrospective observational study of the frequency of distomolar teeth in a population. Cumhur. Dent. J. 2015, 18, 335–342. [Google Scholar]
- Thomas, S.A.; Sherubin, E.; Pillai, K.S. A study on the Prevalence and Characteristics of Distomolar among 1000 Panoramix Ragiographs. J. Indian Acad. Oral Med. Radiol. 2013, 3, 169–172. [Google Scholar]
- Mitsea, A.; Vardas, E.; Papachatzopoulou, A.; Kalfountzos, G.; Leventis, M.; Tsiklakis, K. The frequency of non-syndromic distomolar teeth in a Greek population sample? J. Clin. Exp. Dent. 2015, 5, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.A.; Folwarczna, M.A. Mesiodens diagnosis and management of a common supernumerary tooth. J. Can. Dent. Assoc. 2003, 6, 362–366. [Google Scholar]
- Lustmann, J.; Bodner, L. Dentigerous cysts associated with supernumerary teeth. Int. J. Oral Maxillofac. Surg. 1988, 2, 100–102. [Google Scholar] [CrossRef]
- Pippi, R. Odontomas and supernumerary teeth: Is there a common origin? Int. J. Med. Sci. 2014, 12, 1282–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parolia, A.; Kundabala, M.; Dahal, M.; Mohan, M.; Thomas, M.S. Management of supernumerary teeth. J. Conserv. Dent. 2011, 3, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Demiriz, L.; Durmuşlar, M.C.; Mısır, A.F. Prevalence and characteristics of supernumerary teeth: A survey on 7348 people. J. Int. Soc. Prev. Community Dent. 2015, 1, 39–43. [Google Scholar]
- Lubinsky, M.; Kantaputra, P.N. Syndromes with supernumerary teeth. Am. J. Med. Genet. A 2016, 10, 2611–2616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajab, L.D.; Hamdan, M.A. Supernumerary teeth: Review of the literature and a survey of 152 cases. Int. J. Paediatr. Dent. 2002, 4, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Mallineni, S.K. Supernumerary teeth: Review of the literature with recent updates. In Conference Paper in Science; Hindawi: London, UK, 2014; pp. 1–6. [Google Scholar]
- Johnson, N.R.; Gannon, O.M.; Savage, N.W.; Batstone, M.D. Frequency of odontogenic cysts and tumours: A systematic review. J. Investig. Clin. Dent. 2014, 1, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.V.; Craig, G.T.; Franklin, C.D. Range and demographics of odontogenic cysts diagnosed in a UK population over a 30-year period. J. Oral Pathol. Med. 2006, 8, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.D. Dentigerous cyst. Ear Nose Throat 2018, 3, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasouka, T.; Yonemoto, K.; Kato, Y.; Tatematsu, N. Squamous cell carcinoma arisingin dental cyst. J. Oral Maxillofac. Surg. 2000, 58, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Nimonkar, P.V.; Nimonkara, S.V.; Mandlekara, G.P.; Borleb, R.M.; Gadbailba, A.R. Ameloblastoma arising in a dentigerous cyst: Report of three cases. J. Oral Maxillofac. Surg. Med. Pathol. 2012, 2, 233–237. [Google Scholar] [CrossRef]
- Wright, J.M.; Vered, M. Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Odontogenic and Maxillofacial Bone Tumors. Head Neck Pathol. 2017, 1, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro, D.M.; Capote, J.A.M. Distomolar Supernumerary in the mandibular ramus associated with a dentigerous cyst. A case presentation. Rev. Habanera Cienc. Medicas 2018, 17, 255–264. [Google Scholar]
- Hara, K.; Tsuchiya, S.; Hagiwara, S.; Fujio, M.; Sayo, A.; Hideharu, H. A dentigerous cyst associated with a supernumerary tooth (fourth molar) in the mandibular ramus: A case report. J. Oral Maxillofac. Surg. Med. Pathol. 2019, 2, 98–102. [Google Scholar] [CrossRef]
- Filho, M.J.S.F.; de Andrade, R.; Prestes, T.P.; Cavalcante, F.A.; do Nascimento, J.R.; Aguiar, J.L.; Milério, L.R.; Barro, D.N.R. A dentigerous cyst associated with a supernumerary fourth molar in the mandibular ramus: A case report. Braz. J. Dev. 2020, 6, 93220–93229. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Gender | Patient Age (Years) | Symptoms | Site | Treatment |
|---|---|---|---|---|---|
| Morales ND 2018 [19] | F | 34 | Swelling, Pain | Mandibular Distomolar | Enucleation |
| Hara et al. 2019 [20] | F | 43 | Asymptomatic | Mandibular Distomolar | Enucleation |
| Filho et al. 2020 [21] | M | 30 | Pain | Mandibular Distomolar | Enucleation |
| Present Case | M | 46 | Pain | Maxillary distomolar | Enucleation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Donna, E.; Keller, L.M.; Neri, A.; Perez, A.; Lombardi, T. Maxillary Distomolar Associated with Dentigerous Cyst: An Unusual Entity. Oral 2022, 2, 1-6. https://doi.org/10.3390/oral2010001
Di Donna E, Keller LM, Neri A, Perez A, Lombardi T. Maxillary Distomolar Associated with Dentigerous Cyst: An Unusual Entity. Oral. 2022; 2(1):1-6. https://doi.org/10.3390/oral2010001
Chicago/Turabian StyleDi Donna, Edouard, Loïc Mahé Keller, Annika Neri, Alexandre Perez, and Tommaso Lombardi. 2022. "Maxillary Distomolar Associated with Dentigerous Cyst: An Unusual Entity" Oral 2, no. 1: 1-6. https://doi.org/10.3390/oral2010001
APA StyleDi Donna, E., Keller, L. M., Neri, A., Perez, A., & Lombardi, T. (2022). Maxillary Distomolar Associated with Dentigerous Cyst: An Unusual Entity. Oral, 2(1), 1-6. https://doi.org/10.3390/oral2010001