
White Sponge Nevus, a Rare but Important Entity


Abstract
:
1. Introduction
2. Case Report
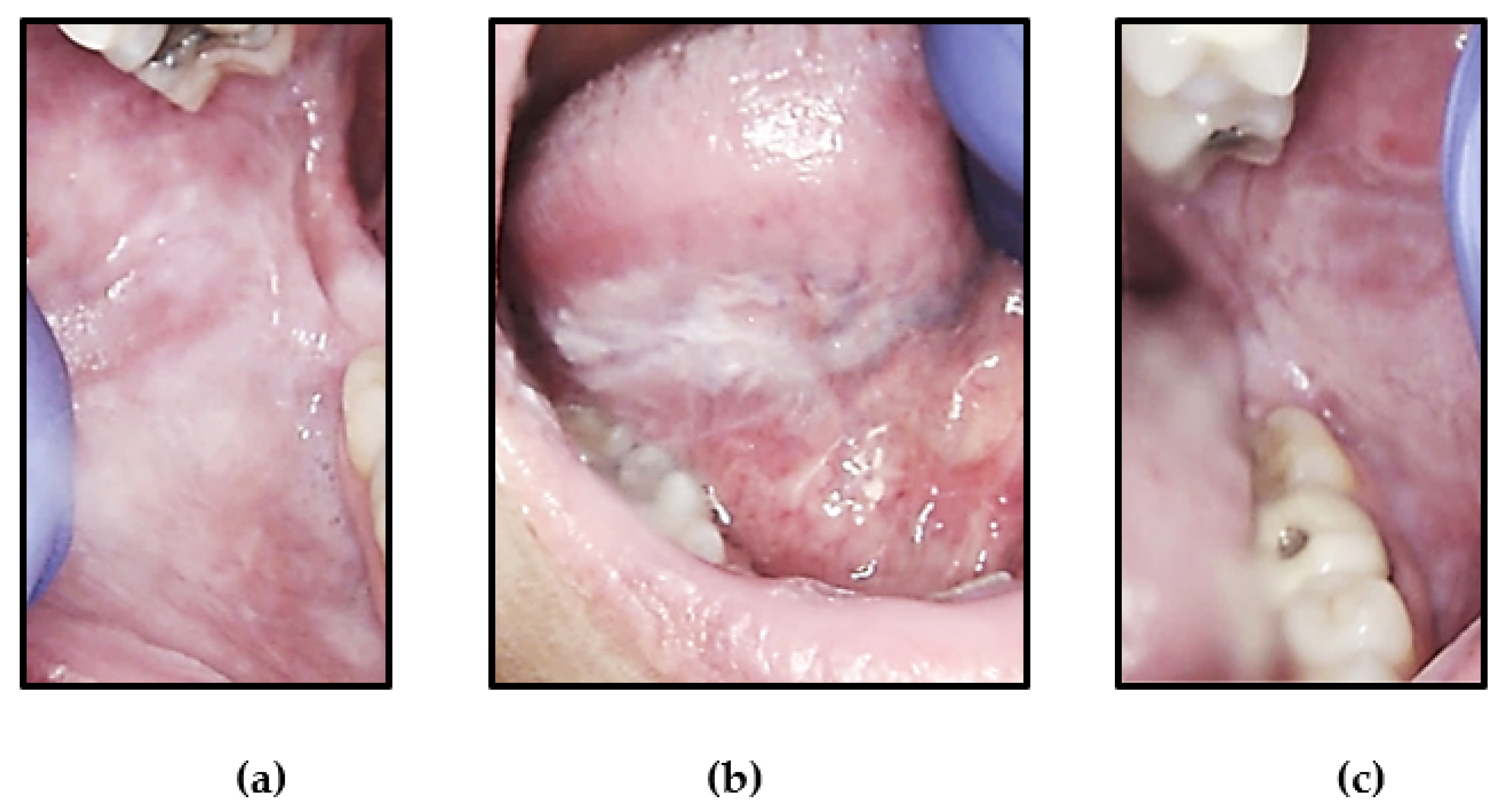
2.1. Case 1
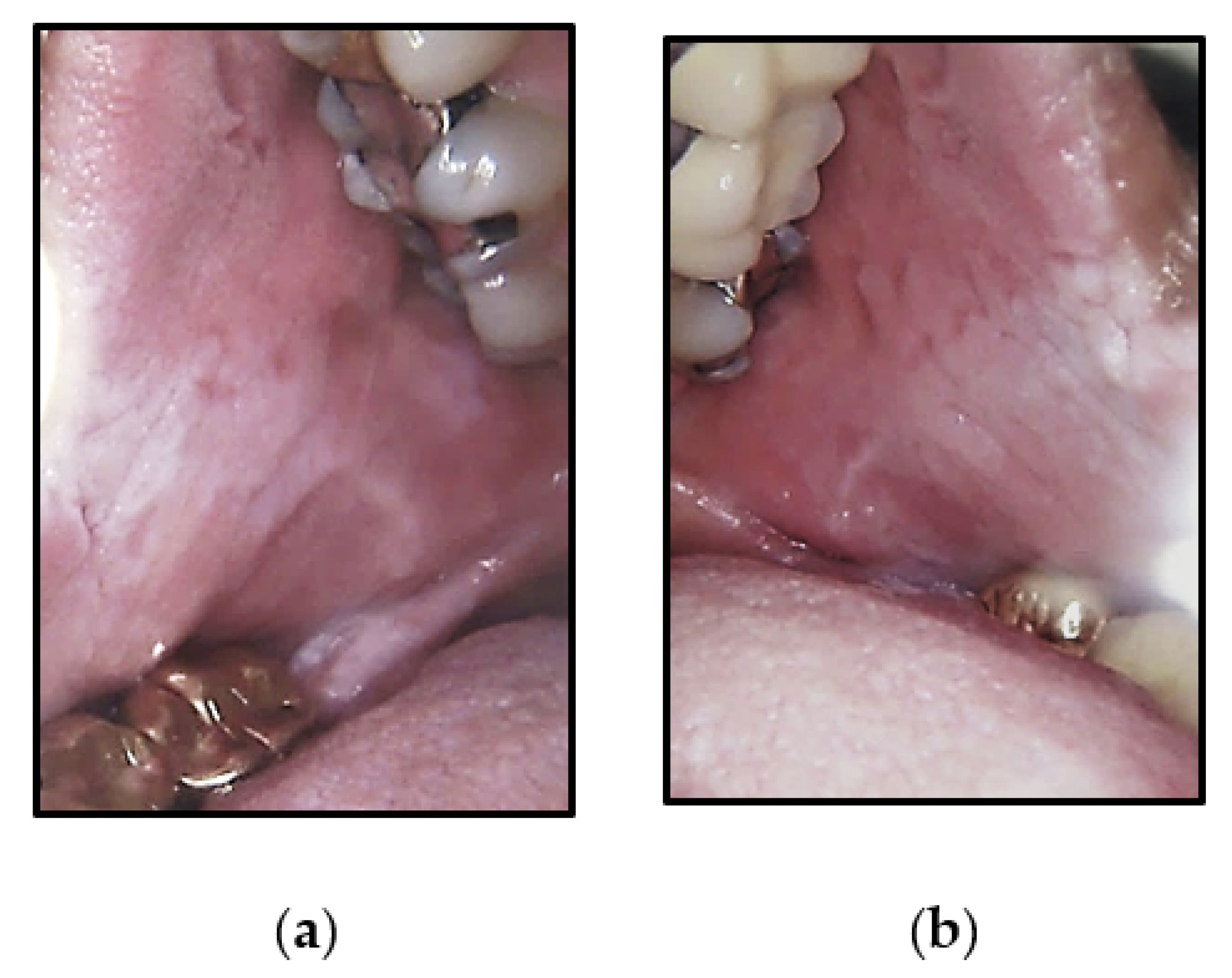
2.2. Case 2
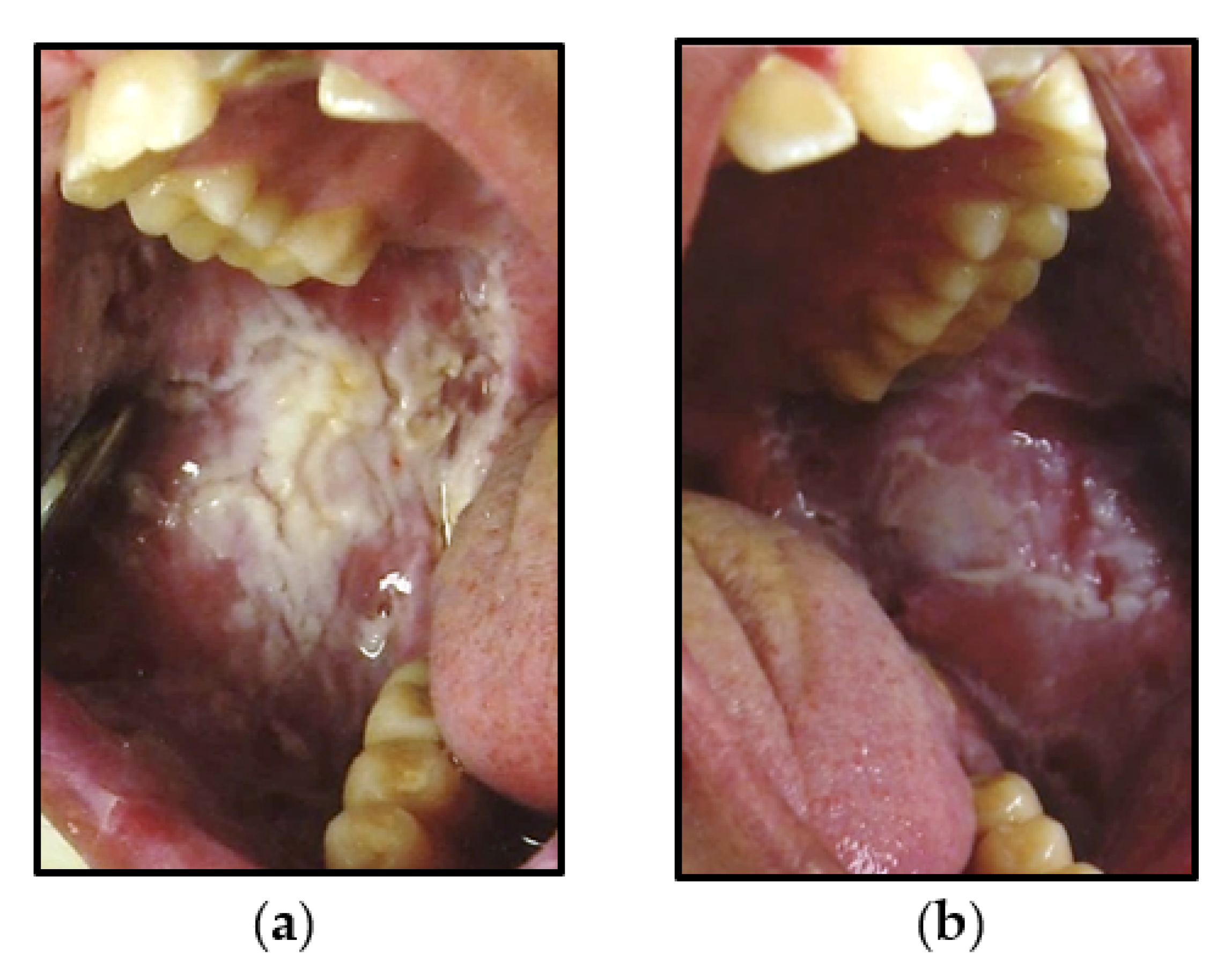
2.3. Case 3
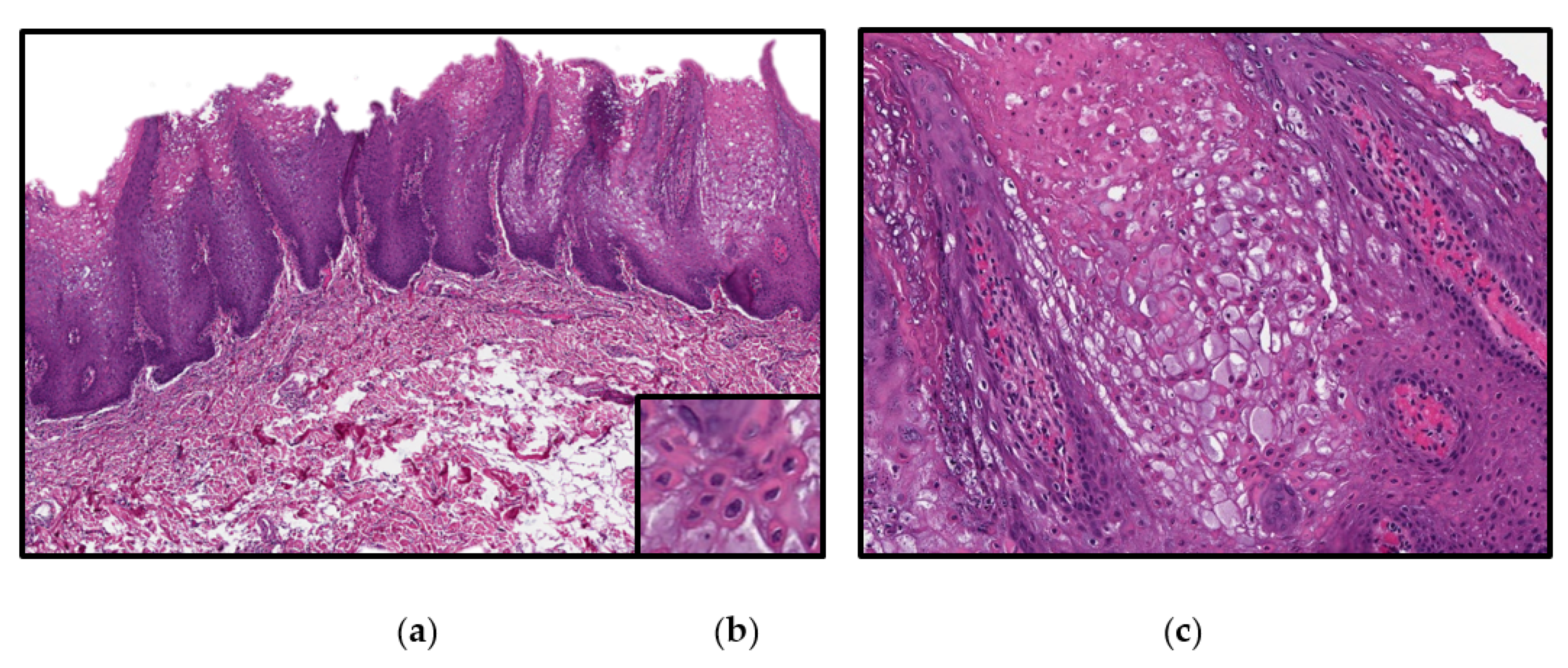
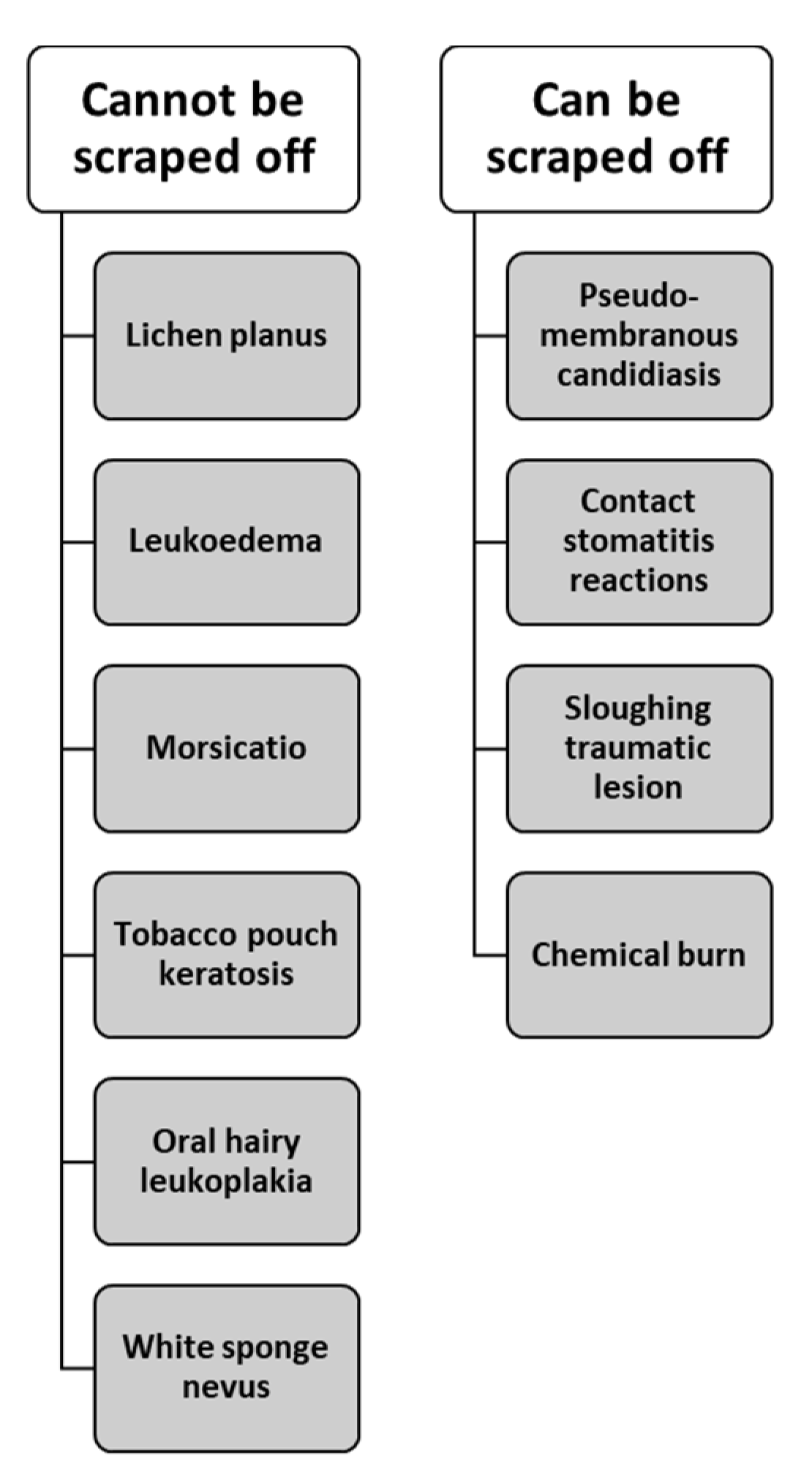
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bezerra, K.T.; Leite, T.C.; Roza, A.L.O.C.; Araújo, R.; Israel, M.S.; Canedo, N.H.S.; Agostini, M.; Benevenuto de Andrade, B.A.; Romañach, M.J. White sponge nevus: A condition not always clinically suspected. J. Cutan Pathol. 2020, 47, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Neville, B.W.; Damm, D.D.; Allen, C.M.; Chi, A.C. Oral and Maxillofacial Pathology, 4th ed.; Elsevier: St. Louis, MO, USA, 2016; 912p. [Google Scholar]
- Cannon, A.B. White Sponge Nevus of the Mucosa (Naevus spongiosus albus mucosae). Arch. Dermatol. Syphilol. 1935, 31, 365–370. [Google Scholar] [CrossRef]
- Martelli, H.; Pereira, S.M.; Rocha, T.M.; Nogueira dos Santos, P.L.; Batista de Paula, A.M.; Bonan, P.R. White sponge nevus: Report of a three-generation family. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Jorgenson, R.J.; Levin, S. White sponge nevus. Arch. Dermatol. 1981, 117, 73–76. [Google Scholar] [CrossRef]
- Rugg, E.L.; McLean, W.H.; Allison, W.E.; Lunny, D.P.; Macleod, R.I.; Felix, D.H.; Lane, E.B.; Munro, C.S. A mutation in the mucosal keratin K4 is associated with oral white sponge nevus. Nat. Genet. 1995, 11, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Terrinoni, A.; Candi, E.; Oddi, S.; Gobello, T.; Camaione, D.B.; Mazzanti, C.; Zambruno, G.; Knight, R.; Melino, G. A glutamine insertion in the 1A alpha helical domain of the keratin 4 gene in a familial case of white sponge nevus. J. Investig. Dermatol. 2000, 114, 388–391. [Google Scholar] [CrossRef]
- Lucchese, A.; Favia, G. White sponge naevus with minimal clinical and histological changes: Report of three cases. J. Oral Pathol. Med. 2006, 35, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Aghbali, A.; Pouralibaba, F.; Eslami, H.; Pakdel, F.; Jamali, Z. White sponge nevus: A case report. J. Dent. Res. Dent. Clin. Dent. Prospect. 2009, 3, 70–72. [Google Scholar] [CrossRef]
- Kürklü, E.; Öztürk, Ş.; Cassidy, A.J.; Ak, G.; Koray, M.; Çefle, K.; Palandüz, Ş.; Güllüoğlu, M.G.; Tanyeri, H.; McLean, W.H. Clinical features and molecular genetic analysis in a Turkish family with oral white sponge nevus. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e144–e150. [Google Scholar] [CrossRef]
- Sanjeeta, N.; Nandini, D.B.; Premlata, T.; Banerjee, S. White sponge nevus: Report of three cases in a single family. J. Oral Maxillofac. Pathol. 2016, 20, 300–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Songu, M.; Adibelli, H.; Diniz, G. White sponge nevus: Clinical suspicion and diagnosis. Pediatr. Dermatol. 2012, 29, 495–497. [Google Scholar] [CrossRef] [PubMed]
- Shibuya, Y.; Zhang, J.; Yokoo, S.; Umeda, M.; Komori, T. Constitutional mutation of keratin 13 gene in familial white sponge nevus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2003, 96, 561–565. [Google Scholar] [CrossRef]
- Woo, S.-B. Oral Pathology, A Comprehensive Atlas and Text, 1st ed.; Elsevier: Philadelphia, PA, USA, 2012; p. 442. [Google Scholar]
- Wood, N.; Goaz, P. Differential Diagnosis of Oral and Maxillofacial Lesions; Elsevier: Amsterdam, The Netherlands, 1997; p. 656. [Google Scholar]
- Regezi, J.A.; Sciubba, J.J.; Jordan, R.C. Oral Pathology Clinical Pathologic Correlations; Elsevier Health Sciences: Edinburgh, UK; London, UK; Oxford, UK, 2017; p. 496. [Google Scholar]
- Elfatoiki, F.Z.; Capatas, S.; Skali, H.D.; Hali, F.; Attar, H.; Chiheb, S. Oral White Sponge Nevus: An Exceptional Differential Diagnosis in Childhood. Case Rep. Dermatol. Med. 2020, 2020, 9296768. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Sex | Intra-Oral Locations | Family History | Extra-Oral Lesions | Duration |
|---|---|---|---|---|---|---|
| 1 | 48 | F | Bilateral buccal mucosa Bilateral ventral tongue | Yes | No | 8+ years |
| 2 | 63 | F | Bilateral buccal mucosa | Yes | No | 10+ years |
| 3 | 18 | M | Bilateral buccal mucosa | Yes | No | 1+ years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belknap, A.N.; Bhattacharyya, I.; Islam, M.N.; Cohen, D.M. White Sponge Nevus, a Rare but Important Entity. Oral 2021, 1, 307-312. https://doi.org/10.3390/oral1040030
Belknap AN, Bhattacharyya I, Islam MN, Cohen DM. White Sponge Nevus, a Rare but Important Entity. Oral. 2021; 1(4):307-312. https://doi.org/10.3390/oral1040030
Chicago/Turabian StyleBelknap, Austin N., Indraneel Bhattacharyya, Mohammed N. Islam, and Donald M. Cohen. 2021. "White Sponge Nevus, a Rare but Important Entity" Oral 1, no. 4: 307-312. https://doi.org/10.3390/oral1040030
APA StyleBelknap, A. N., Bhattacharyya, I., Islam, M. N., & Cohen, D. M. (2021). White Sponge Nevus, a Rare but Important Entity. Oral, 1(4), 307-312. https://doi.org/10.3390/oral1040030