1. Introduction
Drug-influenced gingival enlargement (DIGE) is overgrowth of gingival tissue as a side effect associated with use of systemic medication [
1]. Currently, more than 35 prescription medications have been implicated to cause gingival enlargement [
1,
2,
3] (
Table 1). Out of these, calcium channel blockers (CCBs) are some of the most common causative agents of DIGE. CCBs act by binding to and blocking the L-type calcium channels found in myocardial and vascular smooth muscles [
4]. Since muscle contraction is dependent on extracellular calcium influx into the myocyte, this inhibition of calcium flow causes arterial vasodilation and decreased peripheral resistance, resulting in reduced blood pressure, decrease in myocardial force (negative inotropic effect), heart rate (negative chronotropic effect), and flow velocity within the heart (negative dromotropic effect) [
4]. Based on their chemical structure and effects on smooth muscle, they are classified into three groups: dihydropyridines (e.g., nifedipine, amlodipine, isradipine) are powerful vasodilators; phenylalkylamines (e.g., verapamil) are potent myocardial depressants; and benzothiazopines (e.g., diltiazem) are moderate vasodilators and myocardial depressants [
4]. CCBs are also categorized based on formula and duration of action [
5]. Nifedipine, verapamil, and diltiazemare short-acting, first-generation CCBs; manidipine and nicardipine are second-generation CCBs and have longer duration of action; amlodipine and isradipine are third-generation CCBs and are long-acting drugs whose prolonged action is due to sustained blood concentrations and long half-life [
5]. Newer-generation CCBs were created due to the strong side effects of first-generation CCBs, such as tachycardia, headaches, and peripheral edema [
5]. However, CCBs across generations have been associated with gingival enlargement (GE) [
1,
2]. CCB-influenced gingival enlargement occurs when the periodontium becomes an unintended target of the drug. The development, clinical, and histological presentation is very similar to GE caused by other drugs. Nonetheless, it is attributed with some unique features. The literature on CCB-influenced gingival enlargements conflicting and at times, confusing. The aim of the present review is to elucidate its pathogenesis and treatment.
2. Prevalence
DIGE was first reported as far back as 1939 by Kimball, who described the condition in patients using phenytoin for epilepsy [
6]. Drugs that cause GE are mainly grouped as anti-epileptic drugs, immunosuppressive drugs, and CCBs, although drugs such as oral contraceptives and erythromycin have also been implicated [
1,
2,
3]. The prevalence of DIGE reported in literature is wide and varied. The prevalence of DIGE ranges between 3–20% of GE cases [
7]. The prevalence of DIGE among patients using the three types of drugs is 90% [
8]. The prevalence of phenytoin-influenced GE is about 10–83% among patients using phenytoin [
9], cyclosporine-influenced GE is 25–30% among patients using cyclosporine [
2], and CCB-influenced GE is about 30–50% in CCB users [
9]. Gingival enlargement associated with nifedipine (NIGE) was first reported in 1984 [
10,
11]. Amlodipine-influenced gingival enlargement (AIGE) was first reported in 1994 by Seymour et al. [
12]. Among CCBs, nifedipine appears to have the highest prevalence rate of 6–15% [
13] The prevalence of GE is 5–20% in patients taking diltiazem, 5% in users of verapamil, and 3.3% in patients taking amlodipine, although due to the surge in long-term use for hypertension and angina, the prevalence in patients taking amlodipine has been reported to be as high as 26.7% [
13]. An increased incidence of CCB-influenced DIGE has been associated with concurrent medications, such as cyclosporine [
14,
15,
16], phenytoin [
7], and statins [
17]. Diltiazem, nicardipine, nitrendipine, manidipine [
1,
2,
3], and felodipine [
18] are also associated with GE.
Table 1 enumerates the drugs that have been reported to cause GE.
3. Pathophysiology
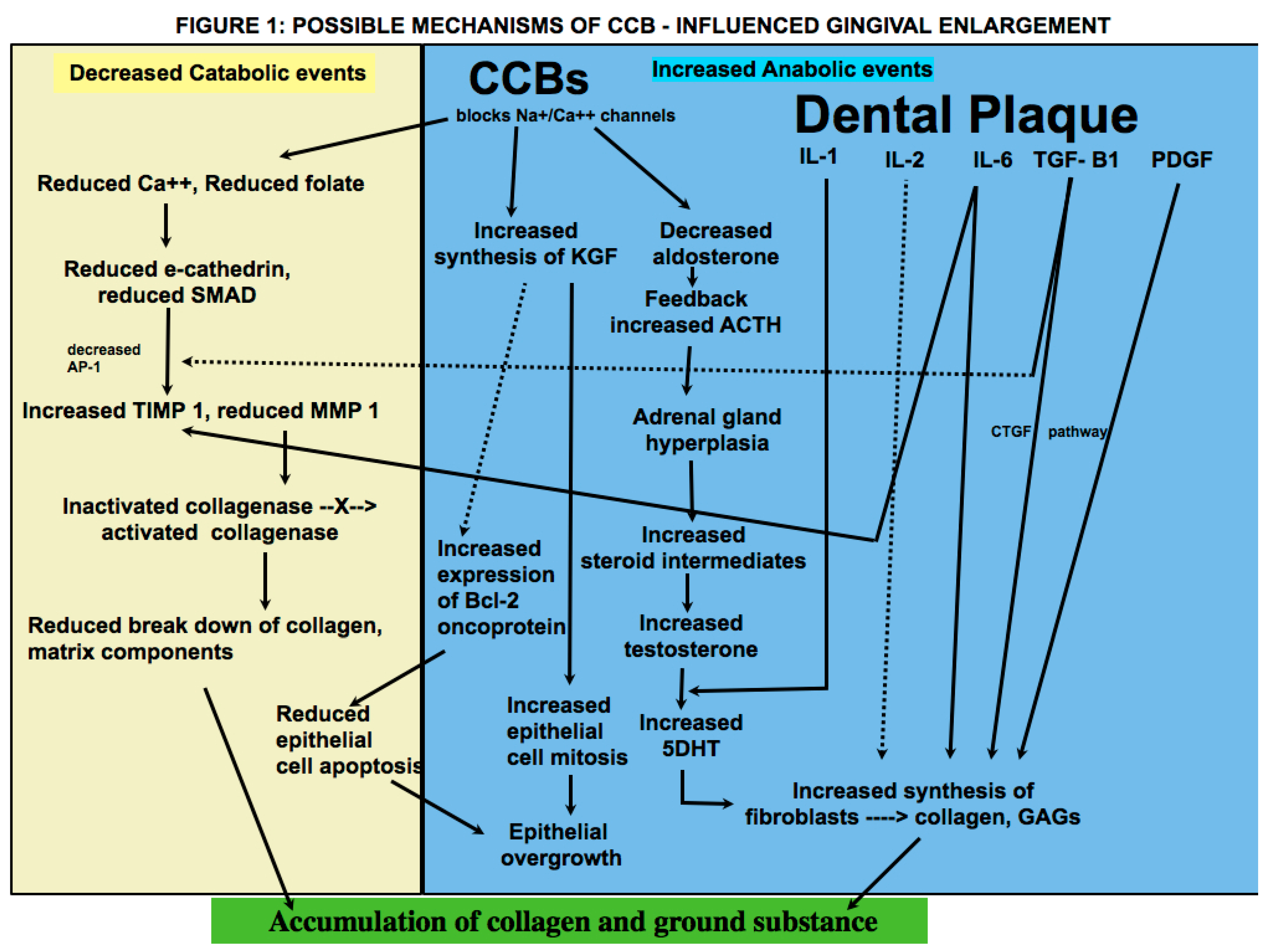
At the cellular level, drugs across genres associated with GE appear to have a similar mechanism of action [
1,
9]. Brown et al. presented a hypothesis that consolidates previous theories on the pathogenesis of DIGE [
9]. These drugs have an inhibitory effect on sodium/calcium cation channels (Na/Ca++), which results in blockage of influx of calcium ions into fibroblasts [
9]. Due to regulatory effect of calcium channels on folate (FA) uptake, this results in reduced uptake of FA into fibroblasts [
9]. This in turn causes a decline in e-cathedrin, a calcium-dependent gene molecule crucial for epithelial cell to cell adhesion, and SMAD (Small Mothers Against Decapentaplegic) gene, a transducer-signaling protein for transforming growth factor-beta 1 (TGF beta1) [
9]. The TGF-beta family of growth factors regulates cell development and proliferation via an incredibly complex system of cross-talking signaling pathways of which the SMAD pathway appears to play a key role in DIGO through its action on tissue inhibitor of metalloproteinase-1 (TIMP-1) and matrix metalloproteinases (MMPs) [
9]. Interleukin-6 (IL6), a pleotropic cytokine, also acts on TIMP-1 [
8]. There is a resultant increase in TIMP-1 and a decrease in MMP-1 [
8,
9], which is required to activate collagenase. The reduced collagenase activity results in decreased collagen breakdown, and accumulation of collagen and other extra cellular matrix (ECM) content occurs as a consequence. In addition, nifedipine has been demonstrated to cause an increased synthesis of keratinocyte growth factor (KGF) by fibroblasts in vitro [
9]. KGF is known to regulate epithelial growth by stimulating cell mitosis and reducing apoptosis of epithelial cells [
9,
13]. Increased synthesis of B-cell lymphoma 2 (BCl2) oncoprotein, which inhibits apoptosis of keratinocytes, has also been found in amlodipine-associated GO [
9]. It is also important to remember that gingiva is a target tissue for androgen metabolism and contains receptors for 5-alpha-dihidrotestosterone (DHT). Nyska et al. proposed a mechanism by which CCB-influenced GO developed in a canine model [
19]. CCBs block aldosterone synthesis due to their calcium flux inhibiting properties, which creates a feedback increase in pituitary ACTH secretion [
19]. This causes adrenal gland hyperplasia and increased synthesis of steroids, such as pregnenolone [
19]. There is a resultant increase in production of testosterone, an anabolic steroid that causes proliferation of fibroblasts and collagen via DHT receptors [
19]. Sooryamurthy et al. similarly reported exaggerated DHT production from testosterone by gingival fibroblasts in patients with GE who were on nifedipine and/or cyclosporine [
20].
Figure 1 shows the possible mechanisms of CCB influenced gingival overgrowth.
A plethora of studies have shown that presence of dental plaque is critical in the development and manifestation of DIGE [
1,
7,
9,
13,
21]. Bacterial plaque in gingival crevicular fluid (GCF) causes an increase in synthesis of both pro inflammatory cytokines, such as interleukins IL-1 [
1], IL-2 [
21], 1L-6 [
8], and anti-inflammatory cytokines and mitogens, such as TGF-beta 1 [
22], platelet-derived growth factor (PDGF), and insulin-like growth factor (IGF) [
23]. It has been proposed that stimulation of gingival fibroblasts occurs when they are exposed to CCBs and pro-inflammatory cytokines, such as IL-1 [
1,
8]. Kasasa et al. reported that IL-1 caused an increase in production of 5DHT from labelled testosterone in human gingiva and periodontal ligament (PDL) [
24]. In addition, increased expression of IL6 has been found in cyclosporin-, phenytoin-, and nifedipine-influenced GE [
8]. IL-6, which has pro- as well as anti-inflammatory tendencies, causes an increase in fibroblast proliferation and glycosaminoglycans synthesis by targeting fibroblasts and accumulation of connective tissue (CT) components by increasing TIMP-1 synthesis [
8]. Growth factors, such as TGF-beta, connective tissue growth factor (CTGF), and PDGF, regulate fibroblast proliferation and collagen synthesis and reduce cell apoptosis [
25]. Taken together, DIGE appears to be a result of an imbalance between anabolic and catabolic events, and the cumulative effect is accumulation of gingival collagen and ground substance. There is conflicting evidence on whether CCBs have a direct or indirect effect on gingival fibroblasts. Nishikawa et al. demonstrated in an in vitro study that in lower doses, nifedipine did not have any effect on fibroblast growth and proliferation [
21]. They concluded that the effect of nifedipine is indirect, as the presence of local inflammatory factors is necessary for nifedipine to stimulate cytokine and/or DHT production by gingival fibroblasts, resulting in increased collagen synthesis. [
21]. On the other hand, it has been theorized that inflammation may develop as a result of direct effects of the drug in gingival crevicular fluid (GCF) [
9].
Effect of Dose on Pathogenesis
The dose of the drug is considered to be an important factor in the development and severity of DIGE by some authors who noted that the severity of the condition was directly related to the dose [
7,
13], while others have disproved the theory due to presence of the condition even in some patients who were taking relatively lower doses [
26,
27].
It has been shown that GE occurs when nifedipine is taken at a dose of 5 mg/day, 10 mg/day, or 20–40 mg/day [
7,
21,
22,
28]. The condition is either noticed or treated about 2–18 months after medication is started [
21]. Amlodipine has been associated with GE even in doses as low as 2.5 mg/day taken over a longer duration of time [
13]. Khzam et al. reported a case of DIGE that occurred within a few days after use of felodipine 400 mg for hypertension [
18]. Ikawa reported a case where gingival enlargement was seen in a patient taking manidipine at a dose of 20 mg/day for several months before surgical intervention [
29]. The range of dose and time of occurrence may be attributed to factors such as the drug used, oral hygiene habits, concurrent use of medication, such as statins, and other existing diseases, such as diabetes mellitus. The appearance of DIGE even in low doses should be factored in while determining the possibility of drug modulation as the initial course of treatment.
4. Clinical Features
The clinical presentation of GE is similar among various drugs [
7]. In general, DIGE is observed at an average of three months after commencement of the drug regime [
30]. The condition usually begins as a nodule in the interdental papilla, which gradually enlarges, involving the facial and palatal/lingual margins [
1]. The interdental papillae eventually coalesce with the enlarged gingival margins and may result in a massive tissue fold over the tooth surfaces, impeding masticatory function and/or speech [
1]. It may extend to the crowns, causing extensive disfigurement of gingiva [
28]. The gingival enlargement in the early stages appears to be painless; however, in more advanced cases, it can cause considerable discomfort during mastication. A feeling of heaviness has been reported in severe cases [
28].
DIGO is described as a diffuse, generalized swelling affecting anterior, posterior, labial, and lingual surfaces of maxilla and mandibular gingiva [
12]. Typically, it is more severe in the maxillary and mandibular anterior facial/labial surfaces [
28].
The clinical observation that DIGO usually begins in the interdental papillae can be explained by the theory that the interdental papillae provide a more suitable nidus for GO to develop [
25]. This may be due to the greater expression of CTGF and integrins in papillary epithelium, which are important for regulating fibroblast synthesis of collagen and GAGs [
25].
When plaque-induced gingival inflammation is not superimposed with DIGE, the lesion has been described as a pink, mulberry shaped, fibrotic-lobulated mass, which is often pedunculated [
1,
7,
28]. In severe cases, when the enlargement extends to attached gingiva, a loss of scalloping is observed [
28]. Lafzi et al. described the lesion to be an outward advancement of gingival tissue rather than a vertical one in that the mean probing depth was only 2.4 mm [
31]. Typically, however, the condition is described to cause ‘pseudo’ pockets due to enlargement of gingiva from beneath the gingival margin with an increase in the probing depths and little or no clinical attachment loss [
30].
In the presence of inflammation, gingival tissue appears edematous, soft, and fluctuant. Newman et al. noted that these secondary inflammatory changes cause an increase in the size of the gingiva, which appears to have a bluish or reddish tinge [
32]. Ikawa et al. described the lesion as being shiny and erythematous in areas where greater excrement of dental plaque was observed [
29]. Spontaneous gingival bleeding and bleeding on probing is present [
1]. Difficulty in mastication leads to further development of pseudo pockets, bacterial in-growth, and calculus excrements. This is more pronounced in the mandibular anterior region due to greater accumulation of plaque and calculus [
28]. Uninhibited bacterial plaque may further cause clinical attachment loss and vertical and horizontal bone loss [
7,
28,
29]. In advanced cases, mobility of teeth [
7] is observed, possibly due to clinical attachment loss. Purulent discharge from the gingival crevices may sometimes be detected [
7,
29].
The 2017 World Workshop defined DIGE by its extent and severity as localized if it involves one tooth or a group of teeth, generalized if it involves most or all the teeth, mild if it involves only the papilla, moderate if it involves the papilla and margin, and severe if it involves the attached gingiva as well [
33].
To define the extent and degree of severity of phenytoin-induced GE, Seymour et al. (1985) devised an index which has been used to define various DIGE in clinical studies [
34]. They designated vertical and horizontal (i.e., labio-lingual) components to the labial and lingual gingiva; the vertical component of which can be categorized as (0) no enlargement of interdental papilla on to tooth surface, (1) mild enlargement resulting in a blunted papilla, (2) moderate enlargement involving lateral spread of interdental papilla onto the tooth surface of up to a quarter of tooth width, and (3) marked encroachment of papilla over greater than a quarter of tooth width [
34]; and the horizontal component as (0) normal thickness of gingival margin, (1) mild increase in thickness less than 2 mm from the normal, and (3) marked increase in thickness greater than 2 mm from the normal [
34]. The Seymour index is an indirect and partial mouth index, as study models are used for assessment, and six maxillary and six mandibular anterior teeth are selected for measurement. Hence, there are 20 gingival units in total that are measured in each patient. The sum of vertical and horizontal components provides the score for each gingival unit, which can be a maximum of 5 [
34]. The sum of the scores for each gingival unit provides the overall score, a maximum of which can be 100, and therefore can be expressed as a percentage [
34]. A GO score of 30% or greater is considered clinically significant GE requiring surgical intervention [
34]. Various methods have been used to define the extent of severity of GE, some using photographic analysis [
35], laser scanners [
27], and histopathological analysis [
1,
7]. The reliability, reproducibility, subjectivity, and validity of GE indices have rarely been studied [
27,
35] and merit further analysis.
CCB-influenced gingival enlargement is sometimes seen in relation to implants [
36], edentulous areas [
37], and deciduous teeth [
38]. A common feature of all DIGE is that it regresses following extraction of teeth in the area [
1].
5. Histopathology and Microbiology
The histopathology amongst various DIGE is very similar and can be differentiated from normal gingival tissue [
1]. In general, it is characterized by acanthotic, stratified squamous epithelium with parakeratosis [
31] and irregular, proliferating, elongated rete pegs [
6,
21,
22].
Aldemir et al. observed a fusion in the rete pegs in their report on AIGE [
22]. The underlying connective tissue consists of increased number of collagen fibers [
21] and ground substance containing a mixture of dense and loose fibers [
7,
39]. Spindle-shaped gingival fibroblasts are plump and abundant, containing sulfated mucopolysaccharides, considered to be secretory granules of inactive MMPs that form a network [
7]. The vascularization is increased and blood vessels appear dilated due to the effect of CCB on the vascular walls [
1,
10]. Perivascular chronic inflammatory cell infiltration consisting of plasma cells and lymphocytes is often present [
7]. In a case of manidipine-influenced GE, Ikawa et al. described an increase in round cell infiltrate and edema [
29]. NIGE is histologically similar to phenytoin-associated GE due to the presence of dense connective tissue and less inflammatory infiltrate [
21]. NIGE may be distinguished from cyclosporine-associated GE on the basis of greater collagen volume, intact elastic fibers, and presence of fibronectins [
21]. Khzam et al. reported fibrous epulis and isolated areas of osseous metaplasia surrounded by heavy chronic cell infiltrate in felodipine-influenced GE, which they attributed to pre-existing chronic periodontitis [
18]. Sanjeev et al. described the presence of calcified areas in the stromal tissue in amlodipine-influenced GE [
39]. In a patient who was on amlodipine for hypertension and acute angina and presented with GE, Pasupuleti et al. detected
Aggregatibacter actinomycetemcomitans,
Porphyromonas gingivalis, and
Prevotella intermedia in areas with greater probing depths [
7]. A reduction in ECM and inflammatory cells has been observed after scaling and/or root planing (SRP) [
1].
7. Treatment
CCBs are often taken for serious medical conditions and are considered to be life saving drugs. However, to provide holistic care, it is prudent to caution patients of all possible adverse drug reactions (ADRs), including DIGE, prior to starting allopathic therapy. This is especially true for CCBs, since many of these drugs are intended to be taken on a long-term basis, and hence, medical and dental professionals should be aware of this well-known but often overlooked side effect and create an effective treatment strategy.
There are various treatment modalities for drug-induced gingival enlargement; however, they share a common path. Treatment begins from the very first dental visit when, after seeking medical history, the dentist identifies the oral pathosis to be associated with medication. From there on, the dentist and periodontist must work closely with the patient and physician to construct a treatment plan that is customized to the patient’s needs, taking into consideration the patient’s systemic health, oral hygiene habits, and compliance factors to avoid recurrence.
7.1. Initial/Non-Surgical Treatment
Initial treatment should be comprised of meticulous oral hygiene measures, which includes oral hygiene instructions (OHI) and full mouth debridement (FMD) [
49] or scaling and root planing (SRP, in the presence of greater probing depths and bone loss) in multiple sessions. Dental conditions that cause a nidus for bacterial growth, such as faulty restorations and ill-fitting dentures, should be replaced, and teeth with severe clinical attachment loss must be extracted to ameliorate patient discomfort. In the presence of debilitating health conditions, consultation with the attending physician prior to treatment is required. Hancock and Swan reported a marked regression by SRP [
50]. Dannewitz et al. applied the FMD concept as described by Quirynen [
51] in a group of 11 patients with CCB- or cyclosporine-influenced GE [
49]. Sub gingival debridement was performed by scaling and root planing of all teeth under local anesthesia within 24 h [
49]. Those taking cyclosporine were pre-medicated with antibiotics due to increased risk of infection from immune suppression [
49].
Chlorhexidine was placed sub gingivally in the pockets in all patients and was used as a rinse after the procedure and post visit daily for two weeks [
49]. A reduction in all clinical parameters, including GE, probing depths, and gingival bleeding, was noted at two and four months [
49]. Following FMD and regular supportive periodontal treatment programs specific for each patient, the need for periodontal surgery was reduced to three patients [
49]. Furthermore, no recurrence was noted during recall after 28 months [
49]. Hence, plaque-control measures are important not only in the initial phase but also in the maintenance phase [
47,
49].
Cessation of the offending drug and/or substitution with another is the ideal treatment option that has been found to be effective in reducing GE [
1,
7,
45]. Since halting CCB therapy may not be systemically beneficial in the long term for some patients, substitution with a drug that provides similar cardiovascular benefits with fewer side effects may be an effective initial treatment option. Studies report an improvement in gingival health following a switch to a drug that does not cause GE [
18,
22,
42]. This is often combined with a stringent plaque removal regime [
18,
22,
42]. Westbrook reported a reduction in gingival overgrowth and probing depths after 12 weeks of substituting nifedipine with isradipine, a third-generation CCB of the same class, without causing significant change in systemic blood pressure [
42]. The reduced probing depth was attributed to the reduction in the inflammation by scaling and root planing at baseline and recession of the gingival margins [
42]. Similarly, other antihypertensive drugs, such as angiotensin converting enzyme (ACE) inhibitorslike captopril and moxonidine, an alpha 2/imadazoline receptor agonist, which acts on the central nervous system and inhibits the sympathetic nervous system, have been used as substitutes [
1,
18]. This strategy of changing the drug regime has been reported to be effective in other forms of DIGE as well: tacrolimus has been used as an alternative to cyclosporine in organ transplant recipients; carbamazepine is used to replace phenytoin in the management of epilepsy [
1,
7]. Only the physician can make pharmacologic decisions after weighing the benefits versus the risk. Studies have reported an improvement in clinical parameters of phenytoin-influenced DIGO with the use of topical and systemic folic acid (FA), although greater efficacy has been reported with the use of topical than systemic FA [
9]. The regression of GO after use of FA may be explained by the theory that when active transport of FA into the cell is inhibited, presence of high concentration of FA in the GCF recreates a concentration gradient and resumes FA cellular uptake [
9]. Whether this strategy can be used as a therapeutic measure in CCB and other DIGE needs to be further explored. Systemic use of NSAIDs that control inflammation, androgen receptor inhibitors that block collagen production via the androgen receptor-dependent CTGF/CCN2-collagen cascade, azithromycin, and topical use of anti-fungal drugs to alleviate symptoms have also been suggested [
1,
9].
Literature on the combination of various non-surgical treatment strategies is contradictory. Some studies have reported a complete regression of DIGE by SRP alone without the need for drug replacement [
49,
50,
52], whereas Westbrook et al. reported that without the switch from nifedipine to isradipine, oral hygiene measures were not effective [
42]. Although the strategy of drug replacement by itself may be successful, a treatment plan consisting of FMD or SRP and OHI has been found to have more predictable results with less chance of recurrence [
25,
42,
47,
48]. When pharmacotherapy is modulated to improve gingival and oral health, it is advisable to wait for at least six months following the change in the drug before determining the need for surgical intervention [
1].
Regression is usually seen in four weeks following drug replacement with adequate plaque control [
24]. Long-term results with complete regression following initial phase of treatment have been reported [
49,
51]. In some studies, however, it has been reported that even aggressive plaque control measures and/or drug replacement therapy without surgical intervention may be insufficient for complete resolution of GE [
42].
7.2. Surgical Treatment
When oral hygiene and pharmacotherapeutic measures are unsuccessful in complete resolution of DIGE, periodontal surgery is necessary to reestablish gingival architecture and restore function and esthetics. It is important to reiterate that surgical phase should not be attempted prior to the hygienic phase for several reasons. First, professional oral hygiene care is necessary to alleviate some of the symptoms caused by bacterial plaque. Second, following plaque control measures, the subsidence of inflammation will make surgical correction easier and more predictable. Third, complete resolution of the condition may be observed after plaque control and drug modulation, which obviates the need for surgery [
49,
50,
52]. In some patients on CCB medication, invasive treatment may be contraindicated. The patient’s systemic health must be considered, and consultation with the physician prior to performing periodontal surgery is necessary. The surgical technique employed is dependent on periodontal condition and clinical presentation of the condition; at times, different therapeutic modes may be employed at different sites in the oral cavity of the same patient [
45]. Often, 0.12% Chlorhexidine gluconate is used during and after periodontal surgery to promote healing [
45]. Gingivectomy is undertaken to remove excess keratinized tissue. The procedure as described by Glickman [
53] employs a scalloped external bevel incision using Kirkland’s knife or 15 BP blade [
45]. Gingivoplasty is done in areas where only minor modifications of gingival contour are necessary [
32]. Gingivectomy re-establishes the gingival architecture and creates a smoother contour than flap procedures [
53]. Although healing is by secondary intention, it is considered the gold standard for surgery for GE [
54]. Periodontal flap surgery is performed in lieu of gingivectomy when there is presence of inadequate keratinized tissue, osseous defects, and/or clinical attachment loss (CAL) or when large areas are involved (≥6 teeth) [
32]. Periodontal flap surgery is performed to remove inflamed connective tissue, reduce pocket depths, and correct osseous defects [
1,
32]. Modified Widman flap [
29], flap with 90-degree incision [
32,
47], and apically positioned flap procedure are commonly performed [
45]. Following flap surgery, the wound heals by primary intention [
45].
Lasers may be used to remove excess gingival tissue. Use of Nd:Yag with 1065 nm wavelength, diode laser with 810 nm wavelength and CO
2 laser with 10,600 nm wavelength has been described [
1,
54]. Laser surgery has the advantage of a relatively dry field during the procedure and less hemorrhage and discomfort postoperatively [
54] as compared to gingivectomy and flap procedures. High-energy lasers inhibit collagen production and result in the formation of slough or scab that protects the underlying tissue [
54]. Electrosurgery has also been used for surgical correction of DIGE. It is especially useful in adolescent patients, patients with mental disabilities, or impaired bleeding or clotting mechanisms when conventional modes for surgery are contraindicated [
1].
In a study by Pilloni et al., probing depths were found to be reduced following flap surgery as compared to gingivectomy at 6 and 12 months [
45]. The authors suggested that this was due to the extensive open wound that was created following gingivectomy as compared to the thin incision line resulting from flap surgery [
45]. Furthermore, the healing pattern is different following the two procedures, with the healing beginning from within connective tissue in the flap procedure resulting in slower clinical manifestation of GE [
45]. Conflictingly, in a split mouth study, Mavrogiannis et al. reported no difference in rate of recurrence of DIGE between gingivectomy and flap procedure after six months [
54]. However, when compared with laser excision, there was greater recurrence of GE following conventional gingivectomy [
54]. Similar to flap surgery, mitotic activity begins from within connective tissue following laser surgery; hence, more time may be required for clinical manifestation of recurrence [
54]. From the data above, it can be deduced that the surgical technique employed has an impact in the clinical outcome of treatment.
7.3. Maintenance and Recurrence
A supportive periodontal maintenance program with regular recall appointments for follow up is recommended following active periodontal therapy to monitor oral health, reinforce home care instructions, and perform in-office plaque control measures. Ilgenli reported 43% recurrence 18 months after periodontal therapy in nifedipine-associated GE and overall 34% recurrence of GO in patients who were on cyclosporine or nifedipine [
47]. Poor attendance at recall appointments was associated with increased risk of recurrence [
47]. A significant association was found between gingival inflammation detected at 18 months and recurrence [
47]. An inverse correlation of recurrence with age of the patient was also observed [
47]. Pernu et al. reported that 13 of the 27 renal transplant patients on CsA showed recurrence 15 months following periodontal therapy [
15]. It must be noted that in this study, supportive periodontal maintenance therapy was not provided after surgery, and this may explain the higher recurrence rate of GE than in the Ilgenli study [
15,
47]. On the other hand, in a more recent study, it was observed that 47.2% of patients using CCB who underwent periodontal treatment experienced recurrence in spite of undergoing supportive periodontal maintenance [
55]. Recurrence can be seen within six months of periodontal surgery [
45,
54]; however, in general, the results of surgery are said to be maintained for an average of 12 months after surgery [
1]. The diversity in recurrence rates among different drugs and factors associated with recurrence warrants further investigation.
Figure 2 illustrates a treatment strategy for minimizing recurrence of GO.
8. Conclusions
When enlargement of an organ occurs due to an increase in the number of cells, the condition is referred to as hyperplasia, whereas when enlargement occurs due to increase in the size of the cells, it is referred to as hypertrophy. What was termed as drug-induced gingival hyperplasia is now known as drug-influenced gingival enlargement, categorized under “dental biofilm induced gingivitis” in the most recent classification scheme for periodontal diseases [
33]. This change in terminology reflects an evolution in understanding of the pathogenesis and development of DIGE. Whereas earlier studies focused on the theory that DIGE is caused by an increase in connective tissue elements, more recent studies suggest that it is a result of an imbalance between catabolic and anabolic mechanisms that are necessary for regulating the periodontium [
9]. Historically, the pathogenesis of DIGE has been described as being caused by inflammatory and non-inflammatory mechanisms; however, they are not distinct or separate; rather, the pathways appear to be confluent in various steps of the disease. In addition, there is insurmountable evidence that dental plaque is necessary for the development and progress of the condition and that the offending drug mainly alters the response of the periodontium to plaque bacteria. It is also important to remember that plaque-induced gingival inflammation does not only contribute to the occurrence of DIGE but is also a consequence of it due to limited access for oral hygiene.
The literature involving pathogenesis of CCB-influenced GE, treament, and clinical outcome of various treatment modalities is conflicting. Nevertheless, the subject is of great relevance due to the widespread use of the drugs that cause it, the pervasiveness of the systemic diseases that require their use, and the functional and cosmetic implications of DIGE. Within the limitation of this article, it may be inferred that genetic makeup, plaque-induced gingival inflammation, type of drug used, duration of drug use, lifestyle and oral hygiene habits, treatment modalities utilized, and patient compliance are important prognostic factors that affect the prevalence and severity of the condition, long-term clinical outcome, and risk of recurrence following periodontal treatment. More studies that focus on predisposing factors should be undertaken that will aid in identifying individuals who are at greater risk for developing DIGE. Patients taking these drugs must be forewarned about this side effect so that they take adequate oral hygiene measures that will help prevent or at least minimize the condition. Longitudinal studies on causes of recurrence will help shed light on why periodontal therapy is successful in some patients, whereas in others, there is recrudescence of gingival enlargement.







{kind=link}
{kind=link}
{kind=link}
{kind=link}