
Bulk-Fill Direct Restorative Materials: An In Vitro Assessment of Their Physio-Mechanical Properties

 , and
, and
Abstract
1. Introduction
2. Experimental Section
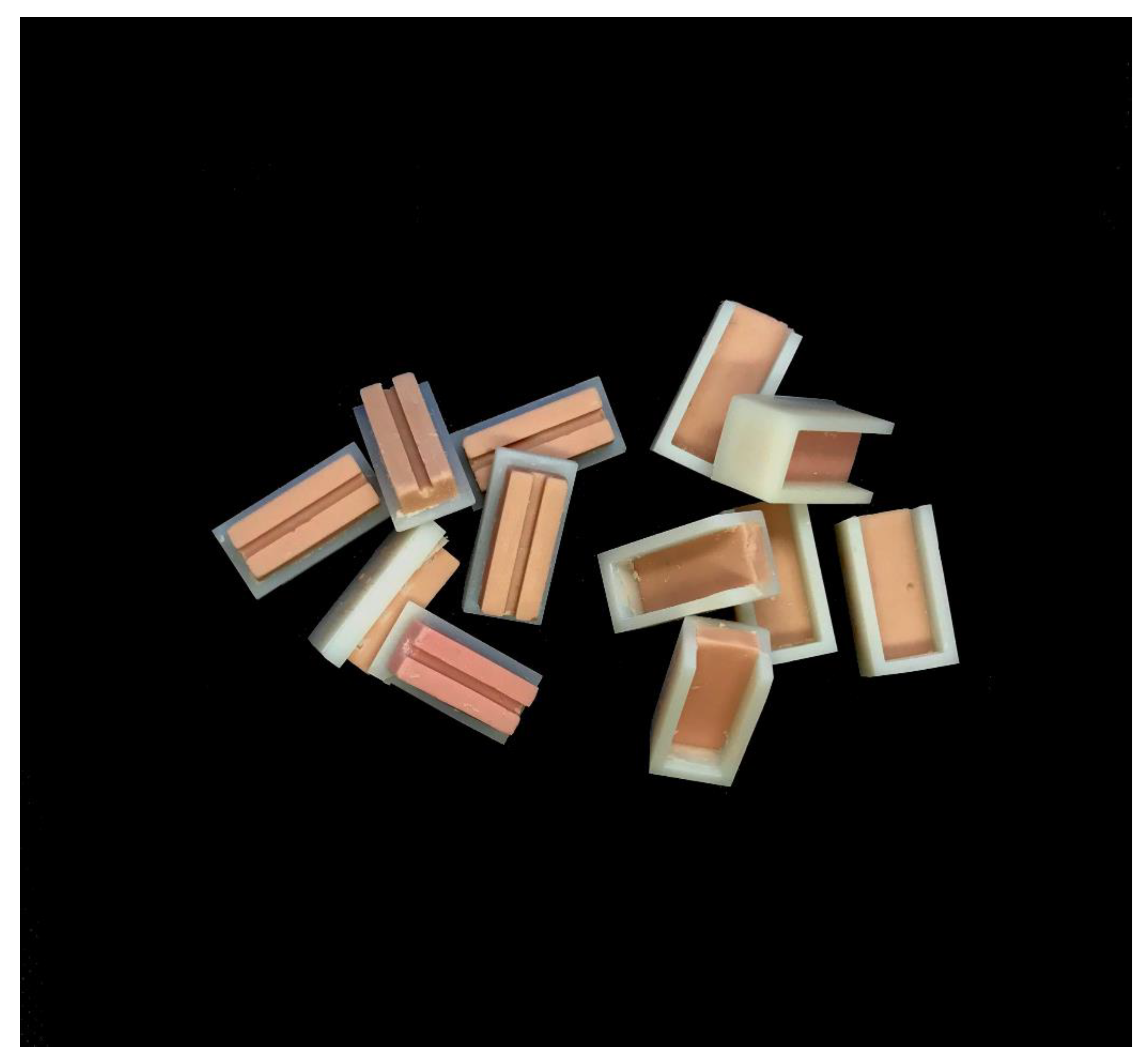
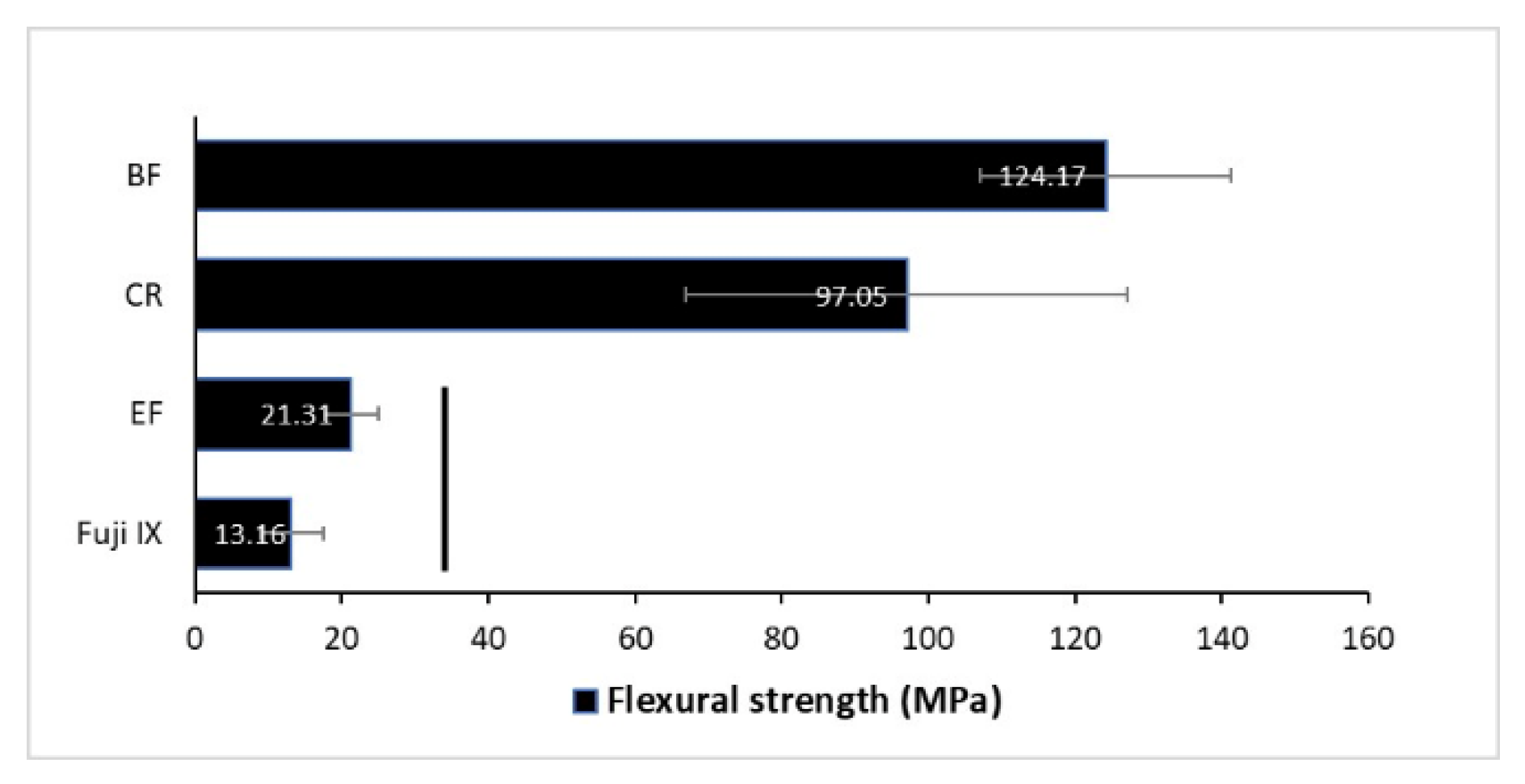
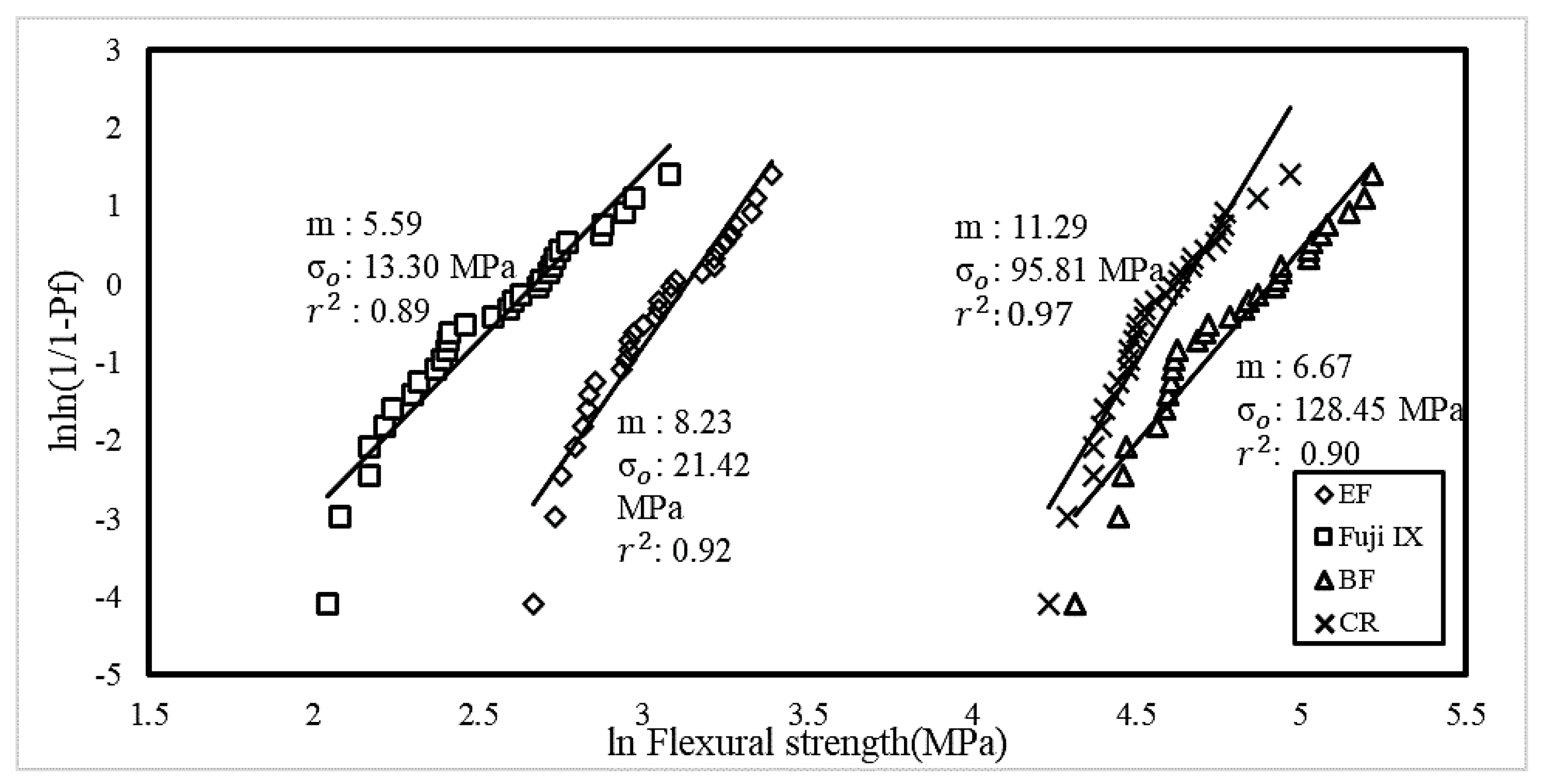
2.1. Flexural Strength Testing
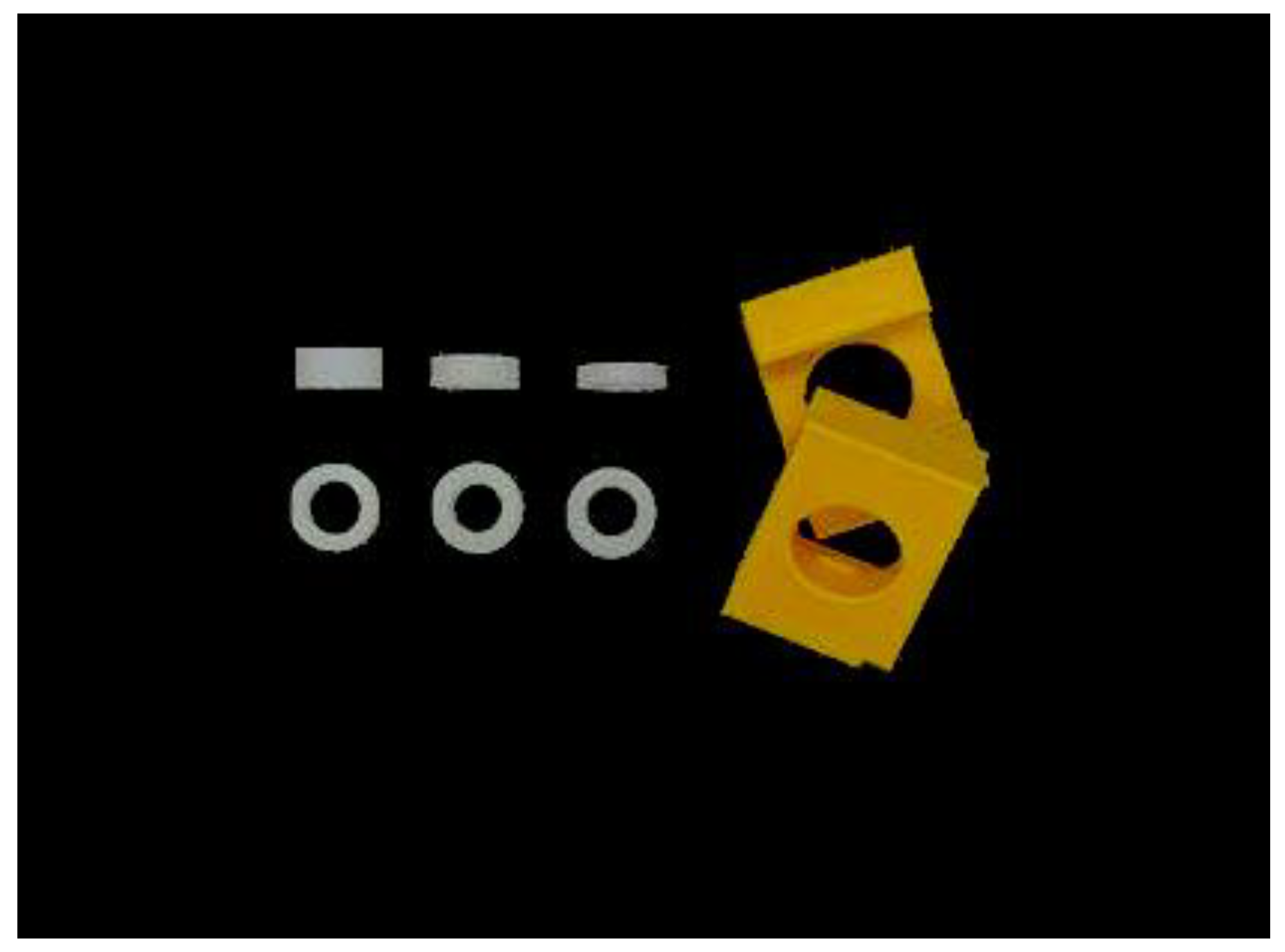
2.2. Elastic Modulus and Hardness
2.3. Depth of Cure
2.4. Wearing Testing
2.5. Translucency
2.6. Statistics
3. Results
4. Discussion
5. Conclusions
- Bulk-fill composites were found to have significantly higher flexural strength compared to conventional composite resin, Fuji IX and EQUIA Forte.
- Fuji IX had the highest elastic modulus follow by EF no coat, CR and BF.
- Filtek bulk-fill has sufficient DC at 4 mm with both 20 s and 40 s light-curing time, but significantly improved DC at 40 s.
- CR and BF had a TP value closest to that of enamel.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, K.H.S.; Mai, Y.; Kim, H.; Tong, K.C.T.; Ng, D.; Hsiao, J.C.M. Review: Resin Composite Filling. Materials 2010, 3, 1228–1243. [Google Scholar] [CrossRef]
- AlShaafi, M.M. Factors affecting polymerization of resin-based composites: A literature review. Saudi Dent. J. 2017, 29, 48–58. [Google Scholar] [CrossRef]
- Yadav, K.D.; Prasad, R.S.; Chaganti, H.; Saleem, M.; Pai, A. Techniques in Direct Composite Restoration. Mod. Approaches Dent. Oral Heal. Care 2018, 3, 307–309. [Google Scholar] [CrossRef]
- Versluis, A.; Douglas, W.; Cross, M.; Sakaguchi, R. Does an Incremental Filling Technique Reduce Polymerization Shrinkage Stresses? J. Dent. Res. 1996, 75, 871–878. [Google Scholar] [CrossRef]
- Menees, T.S.; Lin, C.P.; Kojic, D.D.; Burgess, J.O.; Lawson, N.C. Depth of cure of bulk fill composites with monowave and polywave curing lights. Am. J. Dent. 2015, 28, 357–361. [Google Scholar]
- Ravi, R.; Mandava, J.; Vegesna, D.-P.; Uppalapati, L.-V.; Ghazanfaruddin, M.D.; Boddeda, M.-R. Microtensile bond strength of bulk-fill restorative composites to dentin. J. Clin. Exp. Dent. 2017, 9, e1023–e1028. [Google Scholar]
- 3M Dental Products, FiltekTM One Bulk Fill Restorative, Technical Product Profile. 2016. Available online: https://multimedia.3m.com/mws/media/1317671O/3m-filtek-one-bulk-fill-restorative-technical-product-profile.pdf (accessed on 20 August 2020).
- Mitra, S.B.; Wu, D.; Holmes, B.N. An application of nanotechnology in advanced dental materials. J. Am. Dent. Assoc. 2003, 134, 1382–1390. [Google Scholar] [CrossRef]
- Yazici, A.R.; Antonson, S.A.; Kutuk, Z.B.; Ergin, E. Thirty-Six-Month Clinical Comparison of Bulk Fill and Nanofill Composite Restorations. Oper. Dent. 2017, 42, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Moshaverinia, M.; Navas, A.; Jahedmanesh, N.; Shah, K.C.; Moshaverinia, A.; Ansari, S. Comparative evaluation of the physical properties of a reinforced glass ionomer dental restorative material. J. Prosthet. Dent. 2019, 122, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Ausiello, P.; Piva, A.D.; Borges, A.; Lanzotti, A.; Zamparini, F.; Epifania, E.; Tribst, J.M. Effect of Shrinking and No Shrinking Dentine and Enamel Replacing Materials in Posterior Restoration: A 3D-FEA Study. Appl. Sci. 2021, 11, 2215. [Google Scholar] [CrossRef]
- Fuhrmann, D.; Murchison, D.; Whipple, S.; Vandewalle, K. Properties of New Glass-Ionomer Restorative Systems Marketed for Stress-Bearing Areas. Oper. Dent. 2020, 45, 104–110. [Google Scholar] [CrossRef]
- Ilie, N.; Bucuta, S.; Draenert, M. Bulk-fill Resin-based Composites: An In Vitro Assessment of Their Mechanical Performance. Oper. Dent. 2013, 38, 618–625. [Google Scholar] [CrossRef]
- Leprince, J.G.; Palin, W.M.; Vanacker, J.; Sabbagh, J.; Devaux, J.; Leloup, G. Physico-mechanical characteristics of commercially available bulk-fill composites. J. Dent. 2014, 42, 993–1000. [Google Scholar] [CrossRef]
- Guimarães, T.; Gushiken, N.; Braga, R. Degree of conversion, flexural modulus and polymerization stress of “Bulk Fill” composites. Dent. Mater. 2013, 29, 43. [Google Scholar] [CrossRef]
- Yap, A.U.J.; Pandya, M.; Toh, W.S. Depth of cure of contemporary bulk-fill resin-based composites. Dent. Mater. J. 2016, 35, 503–510. [Google Scholar] [CrossRef]
- Oliver, W.; Pharr, G. An improved technique for determining hardness and elastic modulus using load and displacement sensing indentation experiments. J. Mater. Res. 1992, 7, 1564–1583. [Google Scholar] [CrossRef]
- Chung, S.M.; Yap, A.U.J.; Koh, W.K.; Tsai, K.T.; Lim, C.T. Measurement of Poisson’s ratio of dental composite restorative materials. Biomaterials 2004, 25, 2455–2460. [Google Scholar] [CrossRef]
- Suit, S.R.; Gibbs, C.H.; Benz, S.T. Study of Gliding Tooth Contacts during Mastication. J. Periodontol. 1976, 47, 331–334. [Google Scholar] [CrossRef]
- Heintze, S.D. How to qualify and validate wear simulation devices and methods. Dent. Mater. 2006, 22, 712–734. [Google Scholar] [CrossRef]
- Lohbauer, U. Dental Glass Ionomer Cements as Permanent Filling Materials?—Properties, Limitations and Future Trends. Materials 2009, 3, 76–96. [Google Scholar] [CrossRef]
- Prosser, H.; Powis, D.; Wilson, A. Glass-ionomer Cements of Improved Flexural Strength. J. Dent. Res. 1986, 65, 146–148. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.U.J.; Teoh, S.H. Comparison of flexural properties of composite restoratives using the ISO and mini-flexural tests. J. Oral Rehabilitation 2003, 30, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Junior, S.A.R.; Zanchi, C.H.; De Carvalho, R.V.; Demarco, F.F. Flexural strength and modulus of elasticity of different types of resin-based composites. Braz. Oral Res. 2007, 21, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Asmussen, E.; Peutzfeldt, A. Influence of UEDMA, BisGMA and TEGDMA on selected mechanical properties of experimental resin composites. Dent. Mater. 1998, 14, 51–56. [Google Scholar] [CrossRef]
- Monteiro, G.Q.D.M.; Montes, M.A.J.R. Evaluation of linear polymerization shrinkage, flexural strength and modulus of elasticity of dental composites. Mater. Res. 2010, 13, 51–55. [Google Scholar] [CrossRef][Green Version]
- 3M Dental Products, Filtek XTE Technical Product Profile. Available online: https://multimedia.3m.com/mws/media/922726O/filtek-supreme-xte-technical-product-profile-anz.pdf (accessed on 2 February 2021).
- Czasch, P.; Ilie, N. In vitro comparison of mechanical properties and degree of cure of bulk fill composites. Clin. Oral Investig. 2012, 17, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Ilie, N.; Rencz, A.; Hickel, R. Investigations towards nano-hybrid resin-based composites. Clin. Oral Investig. 2012, 17, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Zorzin, J.; Maier, E.; Harre, S.; Fey, T.; Belli, R.; Lohbauer, U.; Petschelt, A.; Taschner, M. Bulk-fill resin composites: Polymerization properties and extended light curing. Dent. Mater. 2015, 31, 293–301. [Google Scholar] [CrossRef]
- McCabe, J.; Carrick, T. A statistical approach to the mechanical testing of dental materials. Dent. Mater. 1986, 2, 139–142. [Google Scholar] [CrossRef]
- Della Bona, A.; Anusavice, K.J.; DeHoff, P.H. Weibull analysis and flexural strength of hot-pressed core and veneered ceramic structures. Dent. Mater. 2003, 19, 662–669. [Google Scholar] [CrossRef]
- Junior, S.A.R.; Ferracane, J.L.; Della Bona, Á. Flexural strength and Weibull analysis of a microhybrid and a nanofill composite evaluated by 3- and 4-point bending tests. Dent. Mater. 2008, 24, 426–431. [Google Scholar] [CrossRef]
- Gurgan, S.; Kutuk, Z.B.; Ergin, E.; Oztas, S.S.; Cakir, F.Y. Clinical performance of a glass ionomer restorative system: A 6-year evaluation. Clin. Oral Investig. 2016, 21, 2335–2343. [Google Scholar] [CrossRef]
- Diem, V.T.K.; Tyas, M.J.; Ngo, H.C.; Phuong, L.H.; Khanh, N.D. The effect of a nano-filled resin coating on the 3-year clinical performance of a conventional high-viscosity glass-ionomer cement. Clin. Oral Investig. 2013, 18, 753–759. [Google Scholar] [CrossRef]
- Türkün, L.S.; Kanik, Ö. A Prospective Six-Year Clinical Study Evaluating Reinforced Glass Ionomer Cements with Resin Coating on Posterior Teeth: Quo Vadis? Oper. Dent. 2016, 41, 587–598. [Google Scholar] [CrossRef] [PubMed]
- Combe, E.; Shaglouf, A.-M.; Watts, D.; Wilson, N. Mechanical properties of direct core build-up materials. Dent. Mater. 1999, 15, 158–165. [Google Scholar] [CrossRef]
- Ong, J.; Yap, A.U.; Hong, J.Y.; Eweis, A.H.; Yahya, N.A. Viscoelastic Properties of Contemporary Bulk-fill Restoratives: A Dynamic-mechanical Analysis. Oper. Dent. 2018, 43, 307–314. [Google Scholar] [CrossRef]
- Moore, B.K.; Platt, J.A.; Borges, G.; Chu, T.-M.G.; Katsilieri, I. Depth of Cure of Dental Resin Composites: ISO 4049 Depth and Microhardness of Types of Materials and Shades. Oper. Dent. 2008, 33, 408–412. [Google Scholar] [CrossRef]
- Sideridou, I.; Tserki, V.; Papanastasiou, G. Effect of chemical structure on degree of conversion in light-cured dimethacrylate-based dental resins. Biomaterials 2002, 23, 1819–1829. [Google Scholar] [CrossRef]
- Flury, S.; Hayoz, S.; Peutzfeldt, A.; Hüsler, J.; Lussi, A. Depth of cure of resin composites: Is the ISO 4049 method suitable for bulk fill materials? Dent. Mater. 2012, 28, 521–528. [Google Scholar] [CrossRef]
- Alrahlah, A.; Silikas, N.; Watts, D. Post-cure depth of cure of bulk fill dental resin-composites. Dent. Mater. 2014, 30, 149–154. [Google Scholar] [CrossRef]
- Alshali, R.Z.; Silikas, N.; Satterthwaite, J.D. Degree of conversion of bulk-fill compared to conventional resin-composites at two time intervals. Dent. Mater. 2013, 29, e213–e217. [Google Scholar] [CrossRef] [PubMed]
- Ogle, R.E.; Davis, E.L. Clinical wear study of three commercially available artificial tooth materials: Thirty-six month results. J. Prosthet. Dent. 1998, 79, 145–151. [Google Scholar] [CrossRef]
- Miličević, A.; Goršeta, K.; Van Duinen, R.N.; Glavina, D. Surface Roughness of Glass Ionomer Cements after Application of Different Polishing Techniques. Acta Stomatol. Croat. 2018, 52, 314–321. [Google Scholar] [CrossRef]
- Turssi, C.P.; Ferracane, J.L.; Vogel, K. Filler features and their effects on wear and degree of conversion of particulate dental resin composites. Biomaterials 2005, 26, 4932–4937. [Google Scholar] [CrossRef]
- Barkmeier, W.; Takamizawa, T.; Erickson, R.; Tsujimoto, A.; Latta, M.; Miyazaki, M. Localized and Generalized Simulated Wear of Resin Composites. Oper. Dent. 2015, 40, 322–335. [Google Scholar] [CrossRef]
- Lazaridou, D.; Belli, R.; Krämer, N.; Petschelt, A.; Lohbauer, U. Dental materials for primary dentition: Are they suitable for occlusal restorations? A two-body wear study. Eur. Arch. Paediatr. Dent. 2014, 16, 165–172. [Google Scholar] [CrossRef]
- Hotta, M.; Hirukawa, H. Abrasion Resistance of Restorative Glass-Ionomer Cements with a Light-cured Surface Coating. Oper. Dent. 1994, 19, 42–46. [Google Scholar]
- Arsecularatne, J.; Chung, N.; Hoffman, M. An in vitro study of the wear behaviour of dental composites. Biosurf. Biotribol. 2016, 2, 102–113. [Google Scholar] [CrossRef]
- Peutzfeldt, A.; García-Godoy, F.; Asmussen, E. Surface hardness and wear of glass ionomers and compomers. Am. J. Dent. 1997, 10, 15–17. [Google Scholar]
- Lee, Y.-K. Criteria for clinical translucency evaluation of direct esthetic restorative materials. Restor. Dent. Endod. 2016, 41, 159. [Google Scholar] [CrossRef]
- Villarroel, M.; Fahl, N.; De Sousa, A.M.; De Oliveira, O.B. Direct Esthetic Restorations Based on Translucency and Opacity of Composite Resins. J. Esthet. Restor. Dent. 2011, 23, 73–87. [Google Scholar] [CrossRef]
- Pekkan, G. Radiopacity of Dental Materials: An Overview. Avicenna J. Dent. Res. 2016, 8. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material (Manufecturer) | Composition | Powder to Liquid Ratio (g) | Particle Size (µm) |
|---|---|---|---|
| Fuji IX (GC, Tokyo, Japan) | Powder:
| 0.35:0.10 | 10 |
| EQUIA Forte Fil (GC) | Powder:
| 0.40:0.13 | 10 |
| EQUIA Coat (GC) |
| ||
| Resin matrix (Photoinitiator) | Filler | Filler fraction (wt%/vol%) | |
| Filtek One bulk fill restorative (3M ESPE, Seedfeld, Germany) | UDMA, 1,12-DDMA, AFM, AUDMA (CQ) | 76.5/58.4 | 20 nm silica, 4–11 nm zirconia, ytterbium trifluoride filler consisting of agglomerate 100 nm particles |
| Filtek Z350 composite (3M ESPE) | Bis-GMA, UDMA, TEGDMA, PEGDMA, Bis-EMA (CQ) | 78.5/63.3 | 20 nm silica, 4–11 nm zirconia, 0.6–10 microns cluster |
| Material | Mean Hardness Value (Gpa ± S.D) |
|---|---|
| EF | 0.47 ± 0.02 |
| EF no coat | 0.38 ± 0.10 |
| Fuji IX | 0.79 ± 0.13 |
| BF | 0.85 ± 0.03 |
| CR | 1.05 ± 0.05 |
| Material | Thickness (mm) | Curing Time (s) | Bottom Hardness (Gpa ± S.D) | Top Hardness (Gpa ± S.D) | Hardness Ratio (HVBottom-Top Ratio)% |
|---|---|---|---|---|---|
| BF | 4 | 40 | 0.80 ± 0.05 | 0.83 ± 0.08 | 96.8 |
| 4 | 20 | 0.72 ± 0.02 | 0.85 ± 0.03 | 85.0 | |
| 3 | 20 | 0.80 ± 0.04 | 0.90 ± 0.04 | 88.3 | |
| 2 | 20 | 0.81 ± 0.05 | 0.89 ± 0.03 | 90.3 | |
| CR | 2 | 20 | 0.84 ± 0.07 | 1.05 ± 0.05 | 80.0 |
| Material | Month(s) | Mass Loss (g) | Coefficient of Friction (±S.D) | Wear Loss (mm ± S.D) |
|---|---|---|---|---|
| Fuji IX | 3 | 0.01 | 0.002 ± 0.001 | 0.045 ± 0.022 |
| 6 | 0.01 | 0.011 ± 0.003 | 0.066 ± 0.019 | |
| 12 | 0.02 | 0.003 ± 0.003 | 0.167 ± 0.023 | |
| EF | 3 | 0.01 | 0.010 ± 0.009 | 0.130 ± 0.014 |
| 6 | 0.01 | 0.024 ± 0.001 | 0.100 ± 0.013 | |
| 12 | 0.01 | 0.011 ± 0.001 | 0.015 ± 0.009 | |
| BF | 3 | 0 | 0.003 ± 0.002 | 0.020 ± 0.006 |
| 6 | 0 | 0.015 ± 0.002 | 0.001 ± 0.007 | |
| 12 | 0 | 0.014 ± 0.002 | 0.047 ± 0.006 | |
| CR | 3 | 0 | 0.010 ± 0.009 | 0.013 ± 0.020 |
| 6 | 0 | 0.013 ± 0.002 | 0.080 ± 0.009 | |
| 12 | 0 | 0.018 ± 0.002 | 0.002 ± 0.007 |
| Material | Translucency Parameter |
|---|---|
| EF | 5.30 |
| Fuji IX | 3.22 |
| BF | 15.73 |
| CR | 16.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeo, H.W.; Loo, M.Y.; Alkhabaz, M.; Li, K.C.; Choi, J.J.E.; Barazanchi, A. Bulk-Fill Direct Restorative Materials: An In Vitro Assessment of Their Physio-Mechanical Properties. Oral 2021, 1, 75-87. https://doi.org/10.3390/oral1020008
Yeo HW, Loo MY, Alkhabaz M, Li KC, Choi JJE, Barazanchi A. Bulk-Fill Direct Restorative Materials: An In Vitro Assessment of Their Physio-Mechanical Properties. Oral. 2021; 1(2):75-87. https://doi.org/10.3390/oral1020008
Chicago/Turabian StyleYeo, Hui Woon, May Yeh Loo, Mariam Alkhabaz, Kai Chun Li, Joanne Jung Eun Choi, and Abdullah Barazanchi. 2021. "Bulk-Fill Direct Restorative Materials: An In Vitro Assessment of Their Physio-Mechanical Properties" Oral 1, no. 2: 75-87. https://doi.org/10.3390/oral1020008
APA StyleYeo, H. W., Loo, M. Y., Alkhabaz, M., Li, K. C., Choi, J. J. E., & Barazanchi, A. (2021). Bulk-Fill Direct Restorative Materials: An In Vitro Assessment of Their Physio-Mechanical Properties. Oral, 1(2), 75-87. https://doi.org/10.3390/oral1020008