
Efficacy of an Anticoagulation Clinic in Low-Income Brazilian Patients with Heart Disease: A Randomized Clinical Trial

 , , , ,
, , , ,
Abstract
1. Background
2. Methods
2.1. Design and Setting
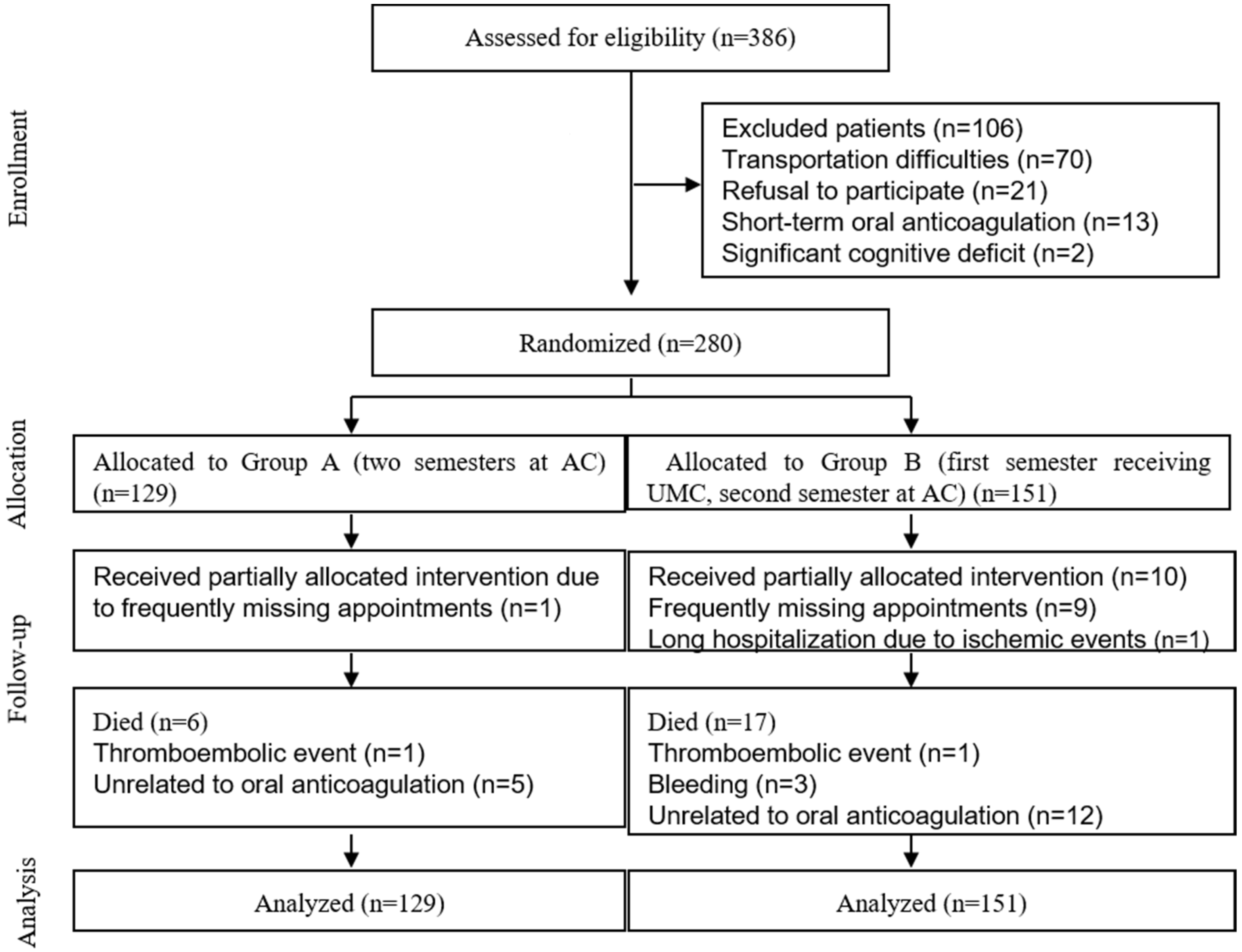
2.2. Recruitment and Randomization
2.3. Data Collection
2.4. Interventions
2.5. Outcomes
2.6. Sample Size
2.7. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- You, J.J.; Singer, D.E.; Howard, P.A.; Lane, D.A.; Eckman, M.H.; Fang, M.C.; Hylek, E.M.; Schulman, S.; Go, A.S.; Hughes, M.; et al. Antithrombotic therapy for atrial fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e531S–e575S. [Google Scholar] [CrossRef]
- Whitlock, R.P.; Sun, J.C.; Fremes, S.E.; Rubens, F.D.; Teoh, K.H. Antithrombotic and Thrombolytic Therapy for Valvular Disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e576S–e600S. [Google Scholar] [CrossRef] [PubMed]
- Carod-Artal, F.J.; Gascon, J. Chagas disease and stroke. Lancet Neurol. 2010, 9, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Mourão, A.D.O.M.; Gomes, K.B.; Reis, E.A.; Souza, R.P.; Campos, E.I.D.F.; Ribeiro, D.D.; Rocha, M.O.D.C.; Martins, M.A.P. Algorithm for predicting low maintenance doses of warfarin using age and polymorphisms in genes CYP2C9 and VKORC1 in Brazilian subjects. Pharmacogenom. J. 2020, 20, 104–113. [Google Scholar] [CrossRef]
- Moustafa, F.; Dopeux, L.; Mulliez, A.; Boirie, Y.; Morand, C.; Gentes, E.; Farigon, N.; Richard, D.; Lebreton, A.; Teissandier, D.; et al. Severe undernutrition increases bleeding risk on vitamin-K antagonists. Clin. Nutr. 2021, 40, 2237–2243. [Google Scholar] [CrossRef]
- Vianna, M.S.; Praxedes, M.F.D.S.; de Araújo, V.E.; Ferreira, C.B.; de Sousa, W.J.F.N.; Viana, C.C.; Martins, M.A.P. Self-report instruments for assessing adherence to warfarin therapy: A systematic review. Eur. J. Clin. Pharmacol. 2021, 77, 1765–1781. [Google Scholar] [CrossRef]
- Martins, M.A.P.; Carlos, P.P.S.; Ribeiro, D.D.; Nobre, V.A.; César, C.C.; Rocha, M.O.C.; Ribeiro, A.L.P. Warfarin drug interactions: A comparative evaluation of the lists provided by five information sources. Eur. J. Clin. Pharmacol. 2011, 67, 1301–1308. [Google Scholar] [CrossRef]
- Ageno, W.; Gallus, A.S.; Wittkowsky, A.; Crowther, M.; Hylek, E.M.; Palareti, G. Oral Anticoagulant Therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e44S–e88S. [Google Scholar] [CrossRef] [PubMed]
- Oake, N.; Jennings, A.; Forster, A.J.; Fergusson, D.; Doucette, S.; van Walraven, C. Anticoagulation intensity and outcomes among patients prescribed oral anticoagulant therapy: A systematic review and meta-analysis. CMAJ 2008, 179, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.; Andreotti, F.; Fauchier, L.; Huber, K.; Hylek, E.; Knight, E.; Lane, D.; Levi, M.; Marín, F.; Palareti, G.; et al. Bleeding risk assessment and management in atrial fibrillation patients. Executive Summary of a Position Document from the European Heart Rhythm Association (EHRA), endorsed by the European Society of Cardiology (ESC) Working Group on Thrombosis. Thromb. Haemost. 2011, 106, 997–1011. [Google Scholar]
- Connolly, S.J.; Pogue, J.; Eikelboom, J.; Flaker, G.; Commerford, P.; Franzosi, M.G.; Healey, J.S.; Yusuf, S. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation 2008, 118, 2029–2037. [Google Scholar] [CrossRef] [PubMed]
- de Lima Silva, R.G.; Bertollo, C.M.; Ferreira, I.G.; Brant, L.C.; Martins, M.A.P. Assessment of oral anticoaguation control at two pharmacist managed clinics in Brazil. Int. J. Clin. Pharm. 2017, 39, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Nieuwlaat, R.; Connolly, B.J.; Hubers, L.M.; Cuddy, S.M.; Eikelboom, J.W.; Yusuf, S.; Connolly, S.J. Quality of individual INR control and the risk of stroke and bleeding events in atrial fibrillation patients: A nested case control analysis of the ACTIVE W study. Thromb. Res. 2012, 129, 715–719. [Google Scholar] [CrossRef]
- White, H.D.; Gruber, M.; Feyzi, J.; Kaatz, S.; Tse, H.F.; Husted, S.; Albers, G.W. Comparison of outcomes among patients randomized to warfarin therapy according to anticoagulant control: Results from SPORTIF III and V. Arch. Intern Med. 2007, 167, 239–245. [Google Scholar] [CrossRef] [PubMed]
- van Walraven, C.; Jennings, A.; Oake, N.; Fergusson, D.; Forster, A.J. Effect of study setting on anticoagulation control: A systematic review and metaregression. Chest 2006, 129, 1155–1166. [Google Scholar] [CrossRef]
- Wofford, J.L.; Wells, M.D.; Singh, S. Best strategies for patient education about anticoagulation with warfarin: A systematic review. BMC Health Serv. Res. 2008, 8, 40. [Google Scholar] [CrossRef]
- Baker, W.L.; Cios, D.A.; Sander, S.D.; Coleman, C.I. Meta-analysis to assess the quality of warfarin control in atrial fibrillation patients in the United States. J. Manag. Care Pharm. 2009, 15, 244–252. [Google Scholar] [CrossRef]
- Costa, G.L.d.B.; Ferreira, D.C.; Valacio, R.A.; Moreira, M.d.C.V. Quality of management of oral anticoagulation as assessed by time in therapeutic INR range in elderly and younger patients with low mean years of formal education: A prospective cohort study. Age Ageing 2011, 40, 375–381. [Google Scholar] [CrossRef]
- Navgren, M.; Forsblad, J.; Wieloch, M. Bleeding complications related to warfarin treatment: A descriptive register study from the anticoagulation clinic at Helsingborg Hospital. J. Thromb. Thrombolysis 2014, 38, 98–104. [Google Scholar] [CrossRef]
- Chiquette, E.; Amato, M.G.; Bussey, H.I. Comparison of an anticoagulation clinic with usual medical care: Anticoagulation control, patient outcomes, and health care costs. Arch. Intern Med. 1998, 158, 1641–1647. [Google Scholar] [CrossRef]
- Wilson, S.J.-A.; Wells, P.S.; Kovacs, M.J.; Lewis, G.M.; Martin, J.; Burton, E.; Anderson, D.R. Comparing the quality of oral anticoagulant management by anticoagulation clinics and by family physicians: A randomized controlled trial. CMAJ 2003, 169, 293–298. [Google Scholar]
- Nichol, M.B.; Knight, T.K.; Dow, T.; Wygant, G.; Borok, G.; Hauch, O.; O’Connor, R. Quality of anticoagulation monitoring in nonvalvular atrial fibrillation patients: Comparison of anticoagulation clinic versus usual care. Ann. Pharmacother. 2008, 42, 62–70. [Google Scholar] [CrossRef]
- Young, S.; Bishop, L.; Twells, L.; Dillon, C.; Hawboldt, J.; O’Shea, P. Comparison of pharmacist managed anticoagulation with usual medical care in a family medicine clinic. BMC Fam. Pract. 2011, 12, 88. [Google Scholar] [CrossRef] [PubMed]
- Nomenclature and Criteria for Diagnosis of Ischemic Heart Disease. Report of the Joint International Society and Federation of Cardiology/World Health Organization Task Force on Standardization of Clinical Nomenclature. Circulation 1979, 59, 607–609. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.A.P.; Ribeiro, D.D.; Nobre, V.A.; Pereira, F.R.; César, C.C.; Rocha, M.O.C.; Ribeiro, A.L.P. Agreement among four drug information sources for the occurrence of warfarin drug interactions in Brazilian heart disease patients with a high prevalence of Trypanosoma cruzi infection. Eur. J. Clin. Pharmacol. 2013, 69, 919–928. [Google Scholar] [CrossRef]
- Garcia, D.A.; Witt, D.M.; Hylek, E.; Wittkowsky, A.K.; Nutescu, E.A.; Jacobson, A.; Moll, S.; Merli, G.J.; Crowther, M.; Earl, L.; et al. Delivery of optimized anticoagulant therapy: Consensus statement from the Anticoagulation Forum. Ann. Pharmacother. 2008, 42, 979–988. [Google Scholar] [CrossRef]
- Ansell, J.; Hirsh, J.; Hylek, E.; Jacobson, A.; Crowther, M.; Palareti, G. Pharmacology and Management of the Vitamin K Antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008, 133, 160S–198S. [Google Scholar] [CrossRef]
- Rosendaal, F.R.; Cannegieter, S.C.; van der Meer, F.J.M.; Briët, E. A method to determine the optimal intensity of oral anticoagulant therapy. Thromb. Haemost. 1993, 69, 236–239. [Google Scholar] [CrossRef]
- Abdelhafiz, A.H.; Wheeldon, N.M. Results of an open-label, prospective study of anticoagulant therapy for atrial fibrillation in an outpatient anticoagulation clinic. Clin. Ther. 2004, 26, 1470–1478. [Google Scholar] [CrossRef] [PubMed]
- Holm, T.; Deutch, S.; Lassen, J.F.; Jastrup, B.; Husted, S.E.; Heickendorff, L. Prospective evaluation of the quality of oral anticoagulation management in an outpatient clinic and in general practices. Thromb. Res. 2002, 105, 103–108. [Google Scholar] [CrossRef]
- Menzin, J.; Boulanger, L.; Hauch, O.; Friedman, M.; Marple, C.B.; Wygant, G.; Hurley, J.S.; Pezzella, S.; Kaatz, S. Quality of anticoagulation control and costs of monitoring warfarin therapy among patients with atrial fibrillation in clinic settings: A multi-site managed-care study. Ann. Pharmacother. 2005, 39, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Heneghan, C.; Perera, R.; Roberts, N.; Hollowell, J.; Glasziou, P.; Bankhead, C.; Xu, Y. Anticoagulation control and prediction of adverse events in patients with atrial fibrillation: A systematic review. Circ. Cardiovasc. Qual. Outcomes 2008, 1, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Willey, M.L.; Chagan, L.; Sisca, T.S.; Chapple, K.J.; Callahan, A.K.; Crain, J.L.; Kitenko, L.E.; Martin, T.; Spedden, K.D. A pharmacist-managed anticoagulation clinic: Six-year assessment of patient outcomes. Am. J. Health Syst. Pharm. 2003, 60, 1033–1037. [Google Scholar] [CrossRef] [PubMed]
- Chan, F.W.H.; Wong, R.S.M.; Lau, W.-H.; Chan, T.Y.K.; Cheng, G.; You, J.H.S. Management of Chinese patients on warfarin therapy in two models of anticoagulation service—A prospective randomized trial. Br. J. Clin. Pharmacol. 2006, 62, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Dias, J.C. Globalization, inequity and Chagas disease. Cad. Saude Publica 2007, 23 (Suppl. S1), S13–S22. [Google Scholar] [CrossRef]
- Matchar, D.; Samsa, G.P.; Cohen, S.J.; Oddone, E.Z.; Jurgelski, A.E. Improving the Quality of Anticoagulation of Patients with Atrial Fibrillation in Managed Care Organizations: Results of the Managing Anticoagulation Services Trial. Am. J. Med. 2002, 113, 42–51. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Group A | Group B |
|---|---|---|---|
| (n = 280) | (n = 129) | (n = 151) | |
| Female sex, n (%) | 153 (54.6) | 73 (56.6) | 80 (53.0) |
| Age, mean (standard deviation) | 56.8 (13.1) | 57.4 (12.2) | 56.3 (13.9) |
| Skin color, n (%) | |||
| White | 62 (22.1) | 32 (24.8) | 30 (19.9) |
| Non-White | 218 (77.8) | 97 (75.2) | 121 (80.1) |
| Body mass index (kg/m2) (Percentiles 25; 50; 75) | 22.7; 25.8; 29.1 | 22.3; 26.0; 30.5 | 22.3; 25.8; 28.9 |
| Marital status, n (%) | |||
| Single | 41 (14.6) | 20 (15.5) | 21 (13.9) |
| Married | 185 (66.1) | 87 (67.5) | 98 (64.9) |
| Divorced | 23 (8.2) | 7 (5.4) | 16 (10.6) |
| Widowed | 31 (11.1) | 15 (11.6) | 16 (10.6) |
| Education, n (%) | |||
| No literacy | 27 (9.6) | 13 (10.1) | 14 (9.3) |
| Incomplete elementary school | 166 (59.3) | 81 (62.8) | 85 (56.3) |
| Elementary school | 34 (12.1) | 15 (11.6) | 19 (12.5) |
| Incomplete high school | 15 (5.4) | 4 (3.1) | 11 (7.3) |
| High school | 35 (12.5) | 14 (10.8) | 21 (13.9) |
| Incomplete college | 3 (1.1) | 2 (1.6) | 1 (0.7) |
| Occupation, n (%) | |||
| Employed | 45 (16.1) | 21 (16.3) | 24 (15.9) |
| Unemployed | 18 (6.4) | 12 (9.3) | 6 (4.0) |
| Retired | 217 (77.5) | 96 (74.4) | 121 (80.1) |
| Monthly income—US dollars (Percentiles 25; 50; 75) | 279; 464; 710 | 279; 470; 710 | 279; 492; 710 |
| Characteristics | Total | Group A | Group B |
|---|---|---|---|
| (n = 280) | (n = 129) | (n = 151) | |
| Indications for anticoagulation therapy | |||
| Atrial fibrillation/Flutter, n (%) | 178 (63.6) | 86 (66.7) | 92 (60.9) |
| Stroke, n (%) | 65 (23.2) | 26 (20.2) | 39 (25.8) |
| Mitral mechanical valve, n (%) | 62 (22.1) | 28 (21.7) | 34 (22.5) |
| Aortic mechanical valve, n (%) | 42 (15.0) | 19 (14.7) | 23 (15.2) |
| Tricuspid mechanical valve, n (%) | 1 (0.4) | 0 (0.0) | 1 (0.7) |
| Heart thrombus, n (%) | 35 (12.5) | 15 (11.6) | 20 (13.2) |
| DVT/PE, n (%) | 22 (7.9) | 12 (9.3) | 10 (6.6) |
| Pulmonary artery hypertension, n (%) | 5 (1.8) | 3 (2.3) | 2 (1.3) |
| Other systemic thromboembolism, n (%) | 2 (0.7) | 1 (0.8) | 1 (0.7) |
| Length of warfarin use—years (Percentiles 25; 50; 75) | 1.7; 3.0; 5.3 | 1.7; 2.8; 4.7 | 1.8; 3.3; 5.8 |
| Target-INR, n (%) | |||
| 2.0–3.0 | 198 (70.7) | 92 (71.3) | 106 (70.2) |
| 2.5–3.5 | 82 (29.3) | 37 (28.7) | 45 (29.8) |
| Number of drugs in chronic use (Percentiles 25; 50; 75) | 4; 6; 7 | 4; 5; 7 | 4; 6; 7 |
| Comorbidities, n (%) | 273 (97.5) | 125 (96.9) | 148 (98.0) |
| Systemic arterial hypertension, n (%) | 168 (60.0) | 77 (59.7) | 91 (60.3) |
| Heart failure, n (%) | 168 (60.0) | 72 (55.8) | 96 (63.6) |
| Dyslipidemia, n (%) | 103 (36.8) | 45 (34.9) | 58 (38.4) |
| Chagas disease, n (%) | 84 (30.0) | 38 (29.5) | 46 (30.5) |
| Valve diseases, n (%) | 55 (19.6) | 25 (19.4) | 30 (19.9) |
| Kidney dysfunction, n (%) | 55 (19.6) | 20 (15.5) | 35 (23.2) |
| Hematological diseases, n (%) | 42 (15.0) | 18 (14.0) | 24 (15.9) |
| Respiratory diseases, n (%) | 42 (15.0) | 19 (14.7) | 23 (15.2) |
| Hypothyroidism, n (%) | 38 (13.6) | 16 (12.4) | 22 (14.6) |
| Neuropsychiatric disorders, n (%) | 36 (12.9) | 16 (12.4) | 20 (13.2) |
| Coronary artery disease, n (%) | 33 (11.8) | 15 (11.6) | 18 (11.9) |
| Rheumatic diseases, n (%) | 27 (9.6) | 17 (13.2) | 10 (6.6) |
| Osteoarticular diseases, n (%) | 24 (8.6) | 9 (7.0) | 15 (9.9) |
| Gastrointestinal disease, n (%) | 18 (6.4) | 9 (7.0) | 9 (6.0) |
| Neoplasias, n (%) | 12 (4.3) | 4 (3.1) | 8 (5.3) |
| Peripheral vascular disease, n (%) | 8 (2.9) | 4 (3.1) | 4 (2.6) |
| Liver dysfunction, n (%) | 6 (2.1) | 1 (0.8) | 5 (3.3) |
| Groups | INR Tests, Percentiles 25; 50; 75 (n α) | Interval between INR Tests (Days), Percentiles 25; 50; 75 (n α) | TTR, Mean ± SD (n α) | p Value |
|---|---|---|---|---|
| A1 | 8; 9; 11 (129) | 16; 20; 24 (129) | 62.4 ± 20.8 (129) | 0.014 β |
| B1 | 5; 7; 10 (151) | 15; 22; 34 (147) | 55.1 ± 28.5 (149) | |
| A1 | 8; 9; 11 (129) | 16; 20; 24 (129) | 63.3 ± 20.2 (125) | 0.059 χ |
| A2 | 7; 9; 10 (125) | 20; 23; 27 (125) | 67.3 ± 21.1 (125) | |
| B1 | 5; 7; 10 (151) | 15; 22; 34 (147) | 55.5 ± 28.1 (135) | 0.008 χ |
| B2 | 8; 10; 11 (135) | 19; 23; 28 (135) | 62.2 ± 23.1 (135) |
| Comparison | Adverse Events, Incidence Rate per Patients-Year (CI, 95%), IRR (CI, 95%), p Value | |||
|---|---|---|---|---|
| Minor Bleeding | Major Bleeding | Total Bleeding | Thromboembolism | |
| A1 vs. B1; A1, n = 129; B1, n = 150 | A1: 1.79 (1.49–2.14) | A1: 0.06 (0.02–0.16) | A1: 1.85 (1.55–2.21) | A1: 0.02 (0.00–0.11) |
| B1: 2.27 (1.95–2.65) | B1: 0.08 (0.04–0.18) | B1: 2.36 (2.03–2.74) | B1: 0.12 (0.06–0.24) | |
| IRR: 0.79 (0.62–0.99) | IRR: 0.74 (0.21–2.62) | IRR: 0.78 (0.62–0.99) | IRR: 0.12 (0.02–0.97) | |
| p = 0.046 | p = 0.639 | p = 0.041 | p = 0.047 | |
| B2 vs. B1; n = 142 | B2: 1.31 (1.07–1.62) | B2: 0.06 (0.02–0.16) | B2: 1.37 (1.12–1.69) | B2: 0.04 (0.01–0.14) |
| B1: 2.27 (1.95–2.65) | B1: 0.08 (0.04–0.18) | B1: 2.36 (2.03–2.74) | B1: 0.12 (0.06–0.24) | |
| IRR: 0.58 (0.45–0.75) | IRR: 0.72 (0.20–2.56) | IRR: 0.58 (0.45–0.75) | IRR: 0.36 (0.10–1.34) | |
| p = 0.000 | p = 0.616 | p < 0.001 | p = 0.127 | |
| A2 vs. A1; n = 127 | A2: 1.04 (0.81–1.34) | A2: 0.03 (0.01–0.14) | A2: 1.07 (0.84–1.37) | A2 α: - A1: 0.02 (0.00–0.11) IRR: - |
| A1: 1.79 (1.49–2.14) | A1: 0.06 (0.02–0.16) | A1: 1.85 (1.55–2.21) | ||
| IRR: 0.58 (0.43–0.79) | IRR: 0.56 (0.10–3.05) | IRR: 0.58 (0.43–0.79) | ||
| p = 0.001 | p = 0.501 | p < 0.001 | ||
| Warfarin-Related Events | Group A | Group B | ||
|---|---|---|---|---|
| A1 | A2 | B1 | B2 | |
| Minor Bleeding | ||||
| Hematoma | 51 | 31 | 69 | 32 |
| Intraocular bleeding | - | 3 | 3 | 1 |
| Ear bleeding | 1 | - | 1 | 1 |
| Epistaxis | 16 | 7 | 32 | 26 |
| Hemoptysis | 3 | 1 | 7 | 6 |
| Gum bleeding | 19 | 7 | 18 | 6 |
| Hematemesis | - | 1 | - | - |
| Upper gastrointestinal bleeding | - | - | 5 | 4 |
| Lower gastrointestinal bleeding | 2 | 1 | 2 | - |
| Hematuria | 7 | 6 | 7 | 2 |
| Hypermenorrhea/Increased menstrual flow | 5 | - | 12 | 3 |
| Vaginal bleeding | 7 | 2 | 4 | - |
| Easy bruising | 6 | 2 | 5 | 4 |
| Rectal bleeding | - | - | - | 3 |
| Total minor bleeding | 117 | 61 | 165 | 88 |
| Major bleeding | ||||
| Hematoma | 1 | 1 | - | - |
| Gum bleeding | - | - | - | 1 |
| Hematemesis | 1 | - | - | - |
| Upper gastrointestinal bleeding | 1 | - | 2 | 2 |
| Hematuria | - | - | - | 1 |
| Hemorrhagic stroke | - | 1 | 3 α, β | - |
| Intra-abdominal bleeding | 1 | - | 1 χ | - |
| Total major bleeding | 4 | 2 | 6 | 4 |
| Total bleeding non-fatal fatal | 121 - | 63 - | 168 3 | 92 - |
| Thromboembolism | ||||
| TIA | - | - | 5 | 1 |
| Stroke | - | - | 2 ε | 1 |
| Mesenteric thrombosis | 1 δ | - | - | - |
| Thrombus in the prosthesis | - | - | 1 | - |
| Heart thrombus | - | - | 1 | - |
| Arterial thrombosis | - | - | 1 | - |
| Total thromboembolisms non-fatal fatal | - 1 | - - | 9 1 | 2 - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martins, M.A.P.; Oliveira, J.A.d.Q.; Ribeiro, D.D.; César, C.C.; Nobre, V.A.; Palhares, D.M.F.; Rocha, M.O.d.C.; Ribeiro, A.L.P. Efficacy of an Anticoagulation Clinic in Low-Income Brazilian Patients with Heart Disease: A Randomized Clinical Trial. Hemato 2023, 4, 227-239. https://doi.org/10.3390/hemato4030018
Martins MAP, Oliveira JAdQ, Ribeiro DD, César CC, Nobre VA, Palhares DMF, Rocha MOdC, Ribeiro ALP. Efficacy of an Anticoagulation Clinic in Low-Income Brazilian Patients with Heart Disease: A Randomized Clinical Trial. Hemato. 2023; 4(3):227-239. https://doi.org/10.3390/hemato4030018
Chicago/Turabian StyleMartins, Maria Auxiliadora Parreiras, João Antonio de Queiroz Oliveira, Daniel Dias Ribeiro, Cibele Comini César, Vandack Alencar Nobre, Daniel Moore Freitas Palhares, Manoel Otávio da Costa Rocha, and Antonio Luiz Pinho Ribeiro. 2023. "Efficacy of an Anticoagulation Clinic in Low-Income Brazilian Patients with Heart Disease: A Randomized Clinical Trial" Hemato 4, no. 3: 227-239. https://doi.org/10.3390/hemato4030018
APA StyleMartins, M. A. P., Oliveira, J. A. d. Q., Ribeiro, D. D., César, C. C., Nobre, V. A., Palhares, D. M. F., Rocha, M. O. d. C., & Ribeiro, A. L. P. (2023). Efficacy of an Anticoagulation Clinic in Low-Income Brazilian Patients with Heart Disease: A Randomized Clinical Trial. Hemato, 4(3), 227-239. https://doi.org/10.3390/hemato4030018