
LDH Isotyping for Checkpoint Inhibitor Response Prediction in Patients with Metastatic Melanoma

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Response Assessment
2.3. Blood Collection and Plasma Collection
2.4. Total LDH Levels and LDH Isotyping
2.5. Circulating Tumor DNA
2.6. Statistics
3. Results
3.1. Patient Characteristics and Samples
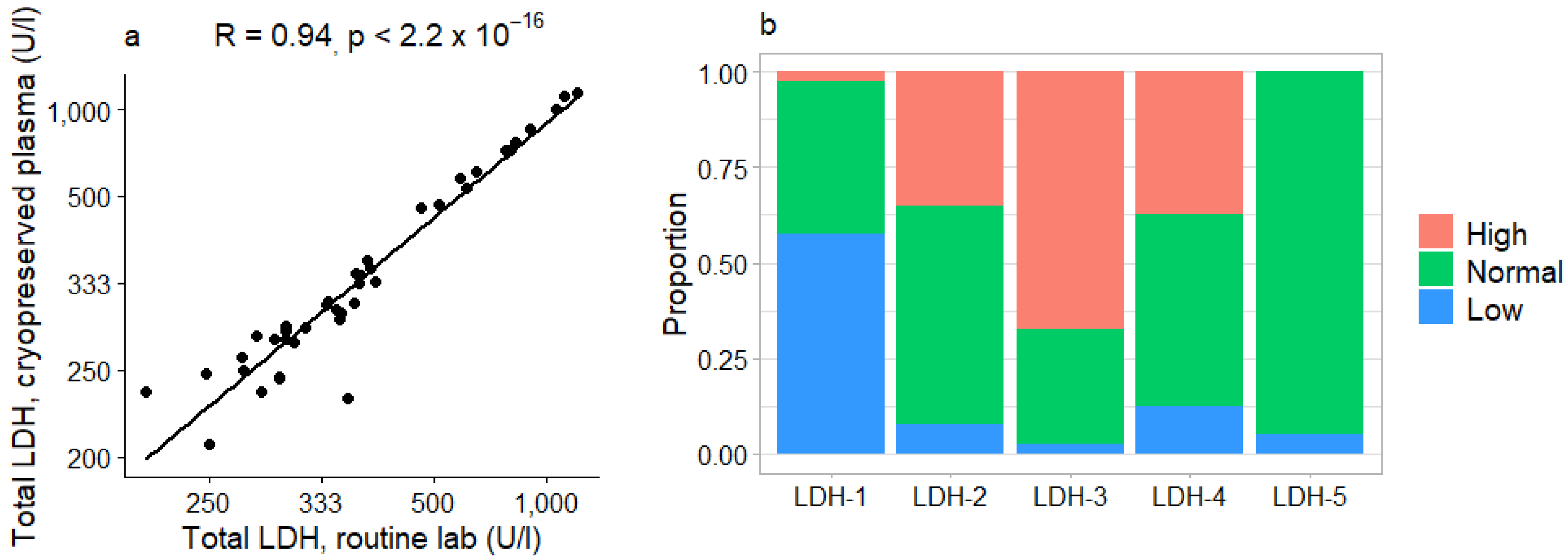
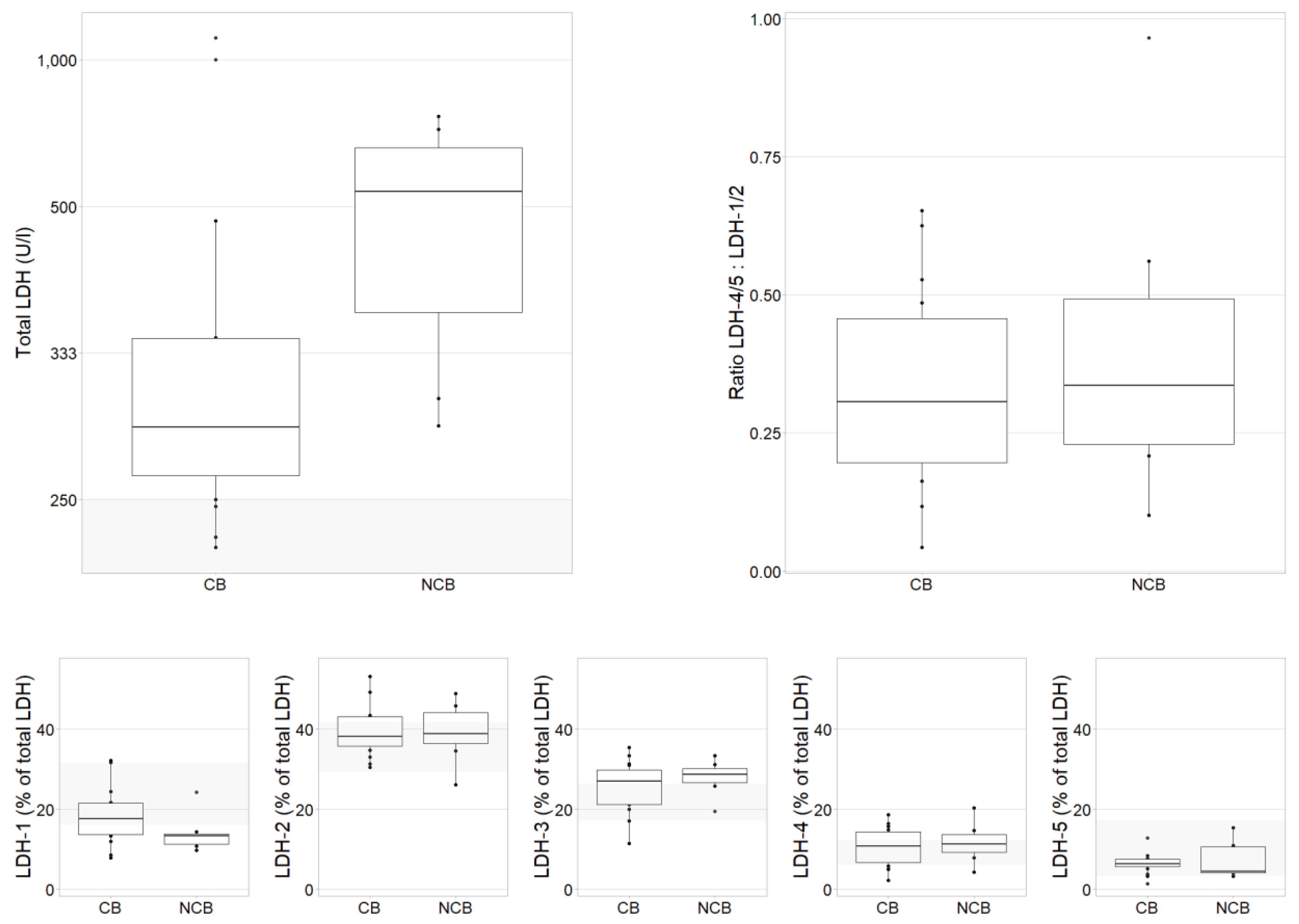
3.2. LDH at Baseline
3.3. Relationship between LDH Isotypes and Response to ICIs
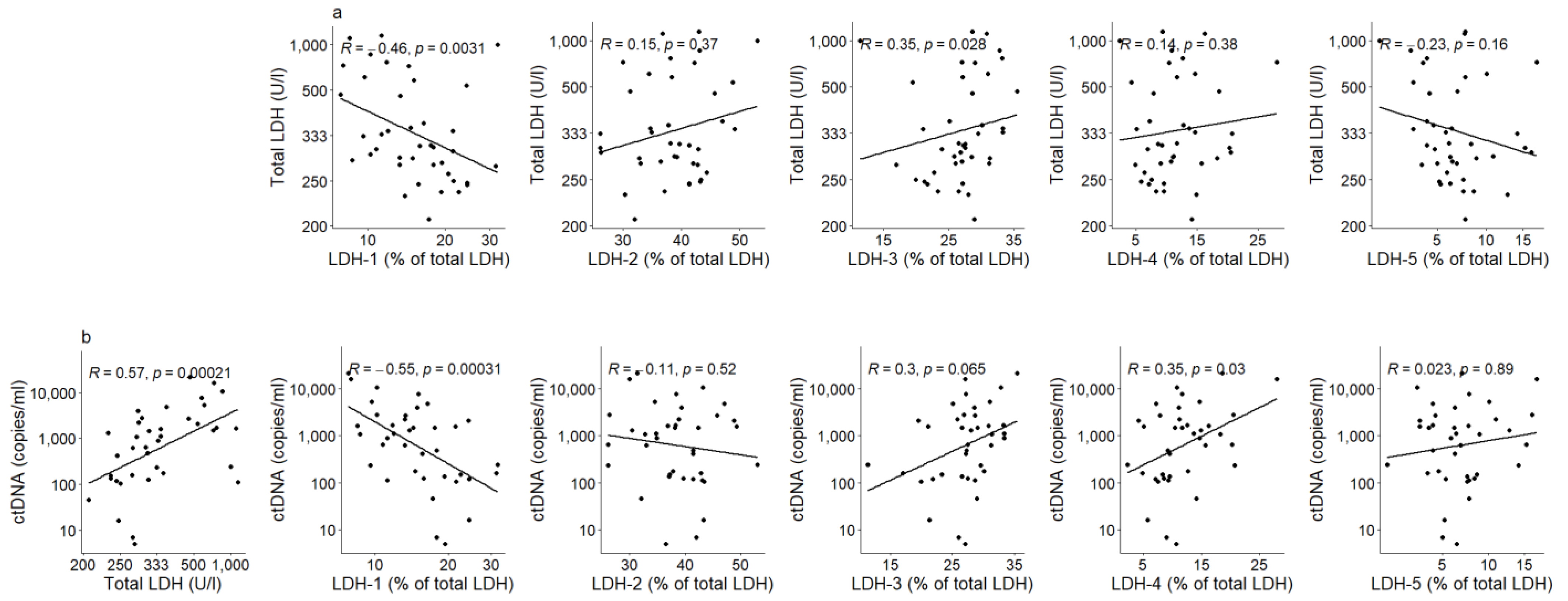
3.4. LDH Isotypes in Relation to Tumor Burden and Total LDH Levels
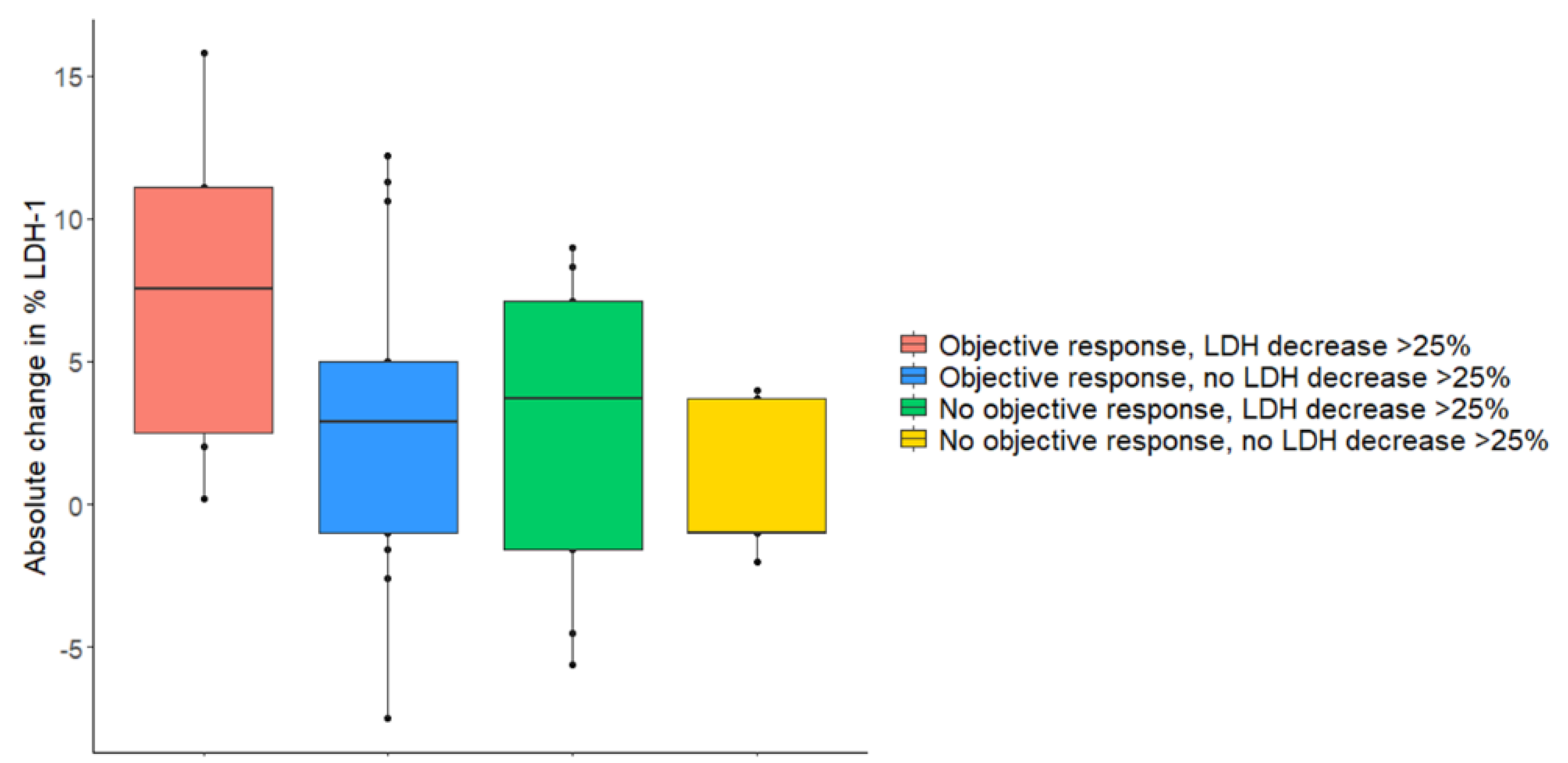
3.5. Changes during Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Xu, J.; Du, C.; Wu, Y.; Xia, D.; Lv, W.; Hu, J. The Predictive Value of Tumor Mutation Burden on Efficacy of Immune Checkpoint Inhibitors in Cancers: A Systematic Review and Meta-Analysis. Front. Oncol. 2019, 9, 1161. [Google Scholar] [CrossRef] [PubMed]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.M.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Ardito, R.; Merelli, B.; Lonati, V.; Cabiddu, M.; Seghezzi, S.; Barni, S.; Ghidini, A. Prognostic and predictive role of elevated lactate dehydrogenase in patients with melanoma treated with immunotherapy and BRAF inhibitors: A systematic review and meta-analysis. Melanoma Res. 2019, 29, 1–12. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.; Cowey, C.; Lao, C.; Wagstaff, J.; Hogg, D.; Hill, A.; Carlino, M.; et al. 3303 Efficacy and safety in key patient subgroups of nivolumab (NIVO) alone or combined with ipilimumab (IPI) versus IPI alone in treatment-naïve patients with advanced melanoma (MEL) (CheckMate 067). Eur. J. Cancer 2015, 51, S664–S665. [Google Scholar] [CrossRef]
- Van Wilpe, S.; Koornstra, R.; Den Brok, M.; De Groot, J.W.; Blank, C.; De Vries, J.; Gerritsen, W.; Mehra, N. Lactate dehydrogenase: A marker of diminished antitumor immunity. Oncoimmunology 2020, 9, 1731942. [Google Scholar] [CrossRef]
- Chang, C.-H.; Curtis, J.D.; Maggi, L.B.; Faubert, B.; Villarino, A.V.; O’Sullivan, D.; Huang, S.C.-C.; Van Der Windt, G.J.; Blagih, J.; Qiu, J.; et al. Posttranscriptional Control of T Cell Effector Function by Aerobic Glycolysis. Cell 2013, 153, 1239–1251. [Google Scholar] [CrossRef]
- Chang, C.-H.; Qiu, J.; O’Sullivan, D.; Buck, M.D.; Noguchi, T.; Curtis, J.D.; Chen, Q.; Gindin, M.; Gubin, M.M.; Van Der Windt, G.J.; et al. Metabolic Competition in the Tumor Microenvironment Is a Driver of Cancer Progression. Cell 2015, 162, 1229–1241. [Google Scholar] [CrossRef]
- Brand, A.; Singer, K.; Koehl, G.E.; Kolitzus, M.; Schoenhammer, G.; Thiel, A.; Matos, C.; Bruss, C.; Klobuch, S.; Peter, K.; et al. LDHA-Associated Lactic Acid Production Blunts Tumor Immunosurveillance by T and NK Cells. Cell Metab. 2016, 24, 657–671. [Google Scholar] [CrossRef]
- Husain, Z.; Huang, Y.; Seth, P.; Sukhatme, V.P. Tumor-Derived Lactate Modifies Antitumor Immune Response: Effect on Myeloid-Derived Suppressor Cells and NK Cells. J. Immunol. 2013, 191, 1486–1495. [Google Scholar] [CrossRef]
- Colegio, O.R.; Chu, N.-Q.; Szabo, A.L.; Chu, T.; Rhebergen, A.M.; Jairam, V.; Cyrus, N.; Brokowski, C.E.; Eisenbarth, S.C.; Phillips, G.M.; et al. Functional polarization of tumour-associated macrophages by tumour-derived lactic acid. Nature 2014, 513, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, L.; Scolyer, R.A.; Murali, R.; McCarthy, S.W.; Zhang, X.D.; Thompson, J.F.; Hersey, P. Lactate dehydrogenase 5 expression in melanoma increases with disease progression and is associated with expression of Bcl-XL and Mcl-1, but not Bcl-2 proteins. Mod. Pathol. 2009, 23, 45–53. [Google Scholar] [CrossRef]
- Feichtinger, R.G.; Lang, R.; Geilberger, R.; Rathje, F.; Mayr, J.A.; Sperl, W.; Bauer, J.W.; Hauser-Kronberger, C.; Kofler, B.; Emberger, M. Melanoma tumors exhibit a variable but distinct metabolic signature. Exp. Dermatol. 2018, 27, 204–207. [Google Scholar] [CrossRef]
- Giatromanolaki, A.; Koukourakis, I.M.; Balaska, K.; Mitrakas, A.G.; Harris, A.L.; Koukourakis, M.I. Programmed death-1 receptor (PD-1) and PD-ligand-1 (PD-L1) expression in non-small cell lung cancer and the immune-suppressive effect of anaerobic glycolysis. Med Oncol. 2019, 36, 76. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.H.; Litière, S.; De Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1—Update and clarification: From the RECIST committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Leung, F.Y.; Henderson, A.R. Influence of hemolysis on the serum lactate dehydrogenase-1/lactate dehydrogenase-2 ratio as determined by an accurate thin-layer agarose electrophoresis procedure. Clin. Chem. 1981, 27, 1708–1711. [Google Scholar] [CrossRef] [PubMed]
- Wróblewski, F.; Gregory, K.F. Lactic dehydrogenase isozymes and their distribution in normal tissues and plasma and in disease states. Ann. N. Y. Acad. Sci. 1961, 94, 912–932. [Google Scholar] [CrossRef]
- McEvoy, A.C.; Warburton, L.; Al-Ogaili, Z.; Celliers, L.; Calapre, L.; Pereira, M.R.; Khattak, M.A.; Meniawy, T.M.; Millward, M.; Ziman, M.; et al. Correlation between circulating tumour DNA and metabolic tumour burden in metastatic melanoma patients. BMC Cancer 2018, 18, 726. [Google Scholar] [CrossRef]
- Ho, J.; De Moura, M.B.; Lin, Y.; Vincent, G.; Thorne, S.; Duncan, L.M.; Hui-Min, L.; Kirkwood, J.M.; Becker, D.; Van Houten, B.; et al. Importance of glycolysis and oxidative phosphorylation in advanced melanoma. Mol. Cancer 2012, 11, 76. [Google Scholar] [CrossRef] [PubMed]
- Kluza, J.; Corazao-Rozas, P.; Touil, Y.; Jendoubi, M.; Maire, C.; Guerreschi, P.; Jonneaux, A.; Ballot, C.; Balayssac, S.; Valable, S.; et al. Inactivation of the HIF-1α/PDK3 Signaling Axis Drives Melanoma toward Mitochondrial Oxidative Metabolism and Potentiates the Therapeutic Activity of Pro-Oxidants. Cancer Res. 2012, 72, 5035–5047. [Google Scholar] [CrossRef]
- Cascone, T.; McKenzie, J.A.; Mbofung, R.M.; Punt, S.; Wang, Z.; Xu, C.; Williams, L.J.; Wang, Z.; Bristow, C.A.; Carugo, A.; et al. Increased Tumor Glycolysis Characterizes Immune Resistance to Adoptive T Cell Therapy. Cell Metab. 2018, 27, 977–987.e4. [Google Scholar] [CrossRef] [PubMed]
- Brooks, G.A. The Science and Translation of Lactate Shuttle Theory. Cell Metab. 2018, 27, 757–785. [Google Scholar] [CrossRef] [PubMed]
- Boyd, J.W. The rates of disappearance of l-lactate dehydrogenase isoenzymes from plasma. BBA Enzymol. 1967, 132, 221–231. [Google Scholar] [CrossRef]
- Zander, J.; Bruegel, M.; Kleinhempel, A.; Becker, S.; Petros, S.; Kortz, L.; Dorow, J.; Kratzsch, J.; Baber, R.; Ceglarek, U.; et al. Effect of biobanking conditions on short-term stability of biomarkers in human serum and plasma. Clin. Chem. Lab. Med. 2014, 52, 629–639. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort 1 (n = 22) | Cohort 1 + 2 (n = 40) | |
|---|---|---|
| Age–median (range) | 69 (28–80) | 63 (28–80) |
| Sex–no. (%) | ||
| Male | 15 (68.2) | 28 (70) |
| Female | 7 (31.8) | 12 (30) |
| ECOG–no. (%) | ||
| 0 | 13 (59.1) | 24 (60) |
| 1 | 6 (27.3) | 13 (32.5) |
| 2 | 3 (13.6) | 3 (7.5) |
| M status–no (%) | ||
| M1a | 3 (13.6) | 8 (20) |
| M1b | - | - |
| M1c | 14 (63.6) | 23 (57.5) |
| M1d | 5 (22.7) | 9 (22.5) |
| Lymph node or lung metastases–no (%) | 21 (95.5) | 39 (97.5) |
| Lymph node metastases–no. (%) | 15 (68.2) | 31 (77.5) |
| Lung metastases–no (%) | 15 (68.2) | 23 (57.5) |
| Liver metastases–no. (%) | 8 (36.4) | 14 (35) |
| LDH (U/l)–median (range) * | 366 (219–1197) | 358 (219–1400) |
| ALAT (U/l)–median (range) | 22.5 (10–175) | 22 (8–370) |
| ASAT (U/l)–median (range) | 25.5 (14–86) | 28 (13–314) |
| Bilirubin (µmol/l)–median (range) | 7 (4–23) | 7 (3–277) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Wilpe, S.; Tolmeijer, S.H.; de Vries, I.J.M.; Koornstra, R.H.T.; Mehra, N. LDH Isotyping for Checkpoint Inhibitor Response Prediction in Patients with Metastatic Melanoma. Immuno 2021, 1, 67-77. https://doi.org/10.3390/immuno1020005
van Wilpe S, Tolmeijer SH, de Vries IJM, Koornstra RHT, Mehra N. LDH Isotyping for Checkpoint Inhibitor Response Prediction in Patients with Metastatic Melanoma. Immuno. 2021; 1(2):67-77. https://doi.org/10.3390/immuno1020005
Chicago/Turabian Stylevan Wilpe, Sandra, Sofie H. Tolmeijer, I. Jolanda M. de Vries, Rutger H. T. Koornstra, and Niven Mehra. 2021. "LDH Isotyping for Checkpoint Inhibitor Response Prediction in Patients with Metastatic Melanoma" Immuno 1, no. 2: 67-77. https://doi.org/10.3390/immuno1020005
APA Stylevan Wilpe, S., Tolmeijer, S. H., de Vries, I. J. M., Koornstra, R. H. T., & Mehra, N. (2021). LDH Isotyping for Checkpoint Inhibitor Response Prediction in Patients with Metastatic Melanoma. Immuno, 1(2), 67-77. https://doi.org/10.3390/immuno1020005