
Causes and Risk Factor of Post-Traumatic Stress Disorder in Adult Asylum Seekers and Refugees

Abstract
:1. Introduction
1.1. Asylum Seekers and Refugees
1.2. Demography
1.3. Post-Traumatic Stress Disorder
1.4. Why Is the Study Needed?
Others Papers/Previous Research
1.5. Aim of Study
2. Methodology
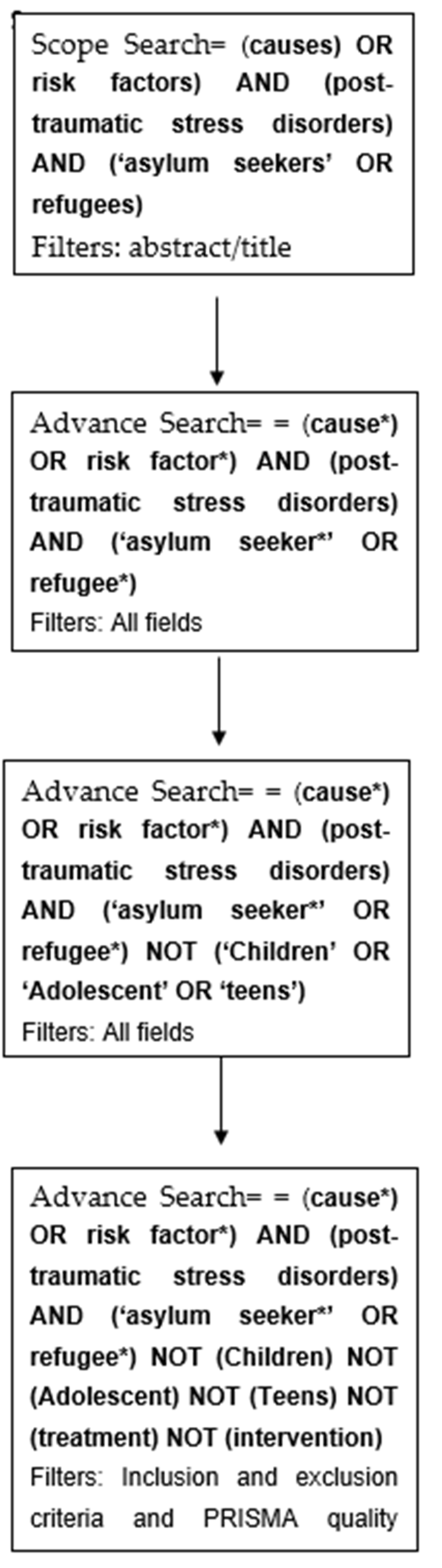
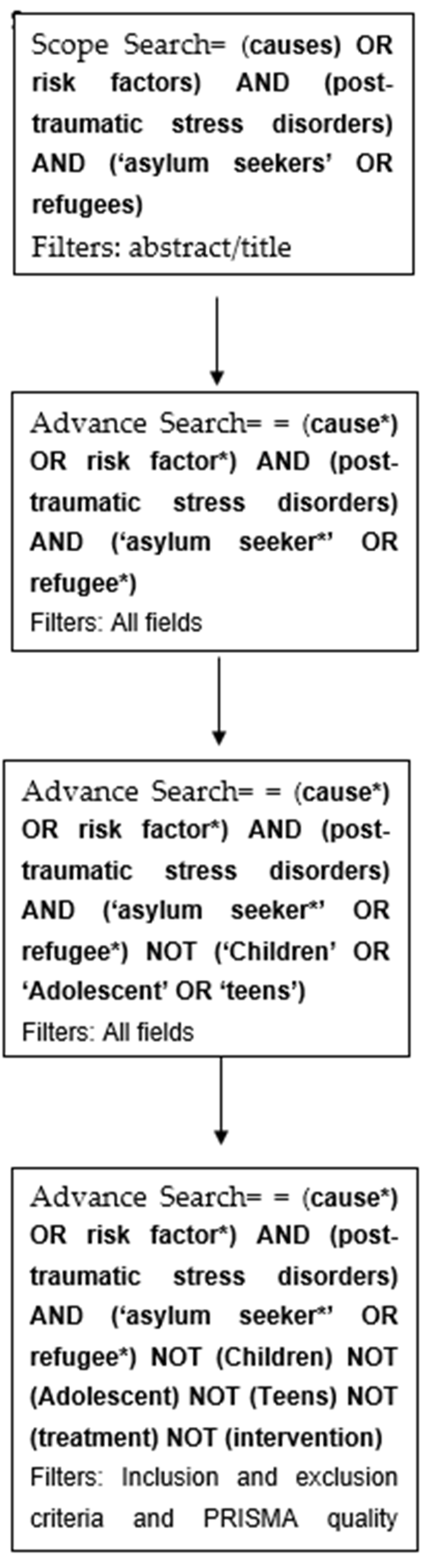
2.1. Search Methods
2.2. Study Selection: Inclusion/Exclusion Criteria
2.3. Quality Assessment and Data Extraction
3. Results
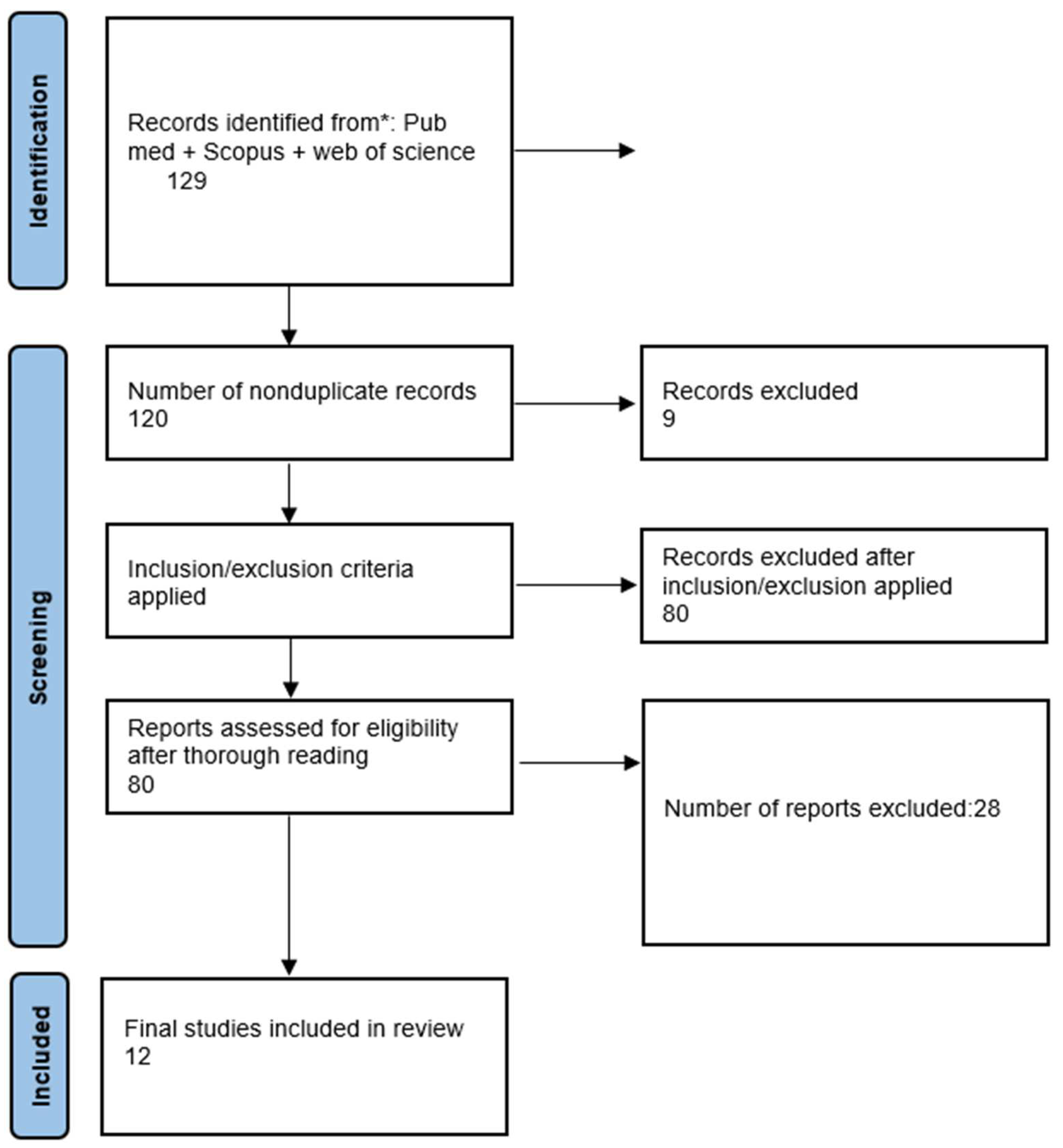
3.1. Search Results
3.2. Study Characteristics
3.3. Main Causes of PTSD in Asylum Seekers and Refugees: Primary Aim
3.4. Comparison of Risk Factors between Male and Female Refugees: Secondary Aim
4. Discussion
4.1. Summary of Findings
4.2. Strengths and Limitations of Study
4.3. What this Study Adds/Comparison with Other Studies
4.4. Practical Application of Findings
4.5. Future Research
- The need for more randomised studies investigating the causes/risk factors of PTSD in asylum seekers/refugees in order to reduce recall bias.
- The use of questionnaire/sampling instruments that are specifically designed for the chosen population in order to increase confidence in the results.
- The need for more studies comparing the risk factors of non-immigrants with PTSD and asylum seekers/refugees.
- Adoption of a validated diagnostic algorithms when assessing potential PTSD diagnosis.
- Research into the exact mechanism and pathway of how relevant causes of PTSD manifest, which could further advance intervention options.
- A larger sample size, preferably more than 500 participants, when examining displaced persons for PTSD causes/risk factors.
- More research/studies are needed that have similar objectives to this review to further enhance confidence in our findings.
5. Conclusions
5.1. What Is Already Known on This Topic
5.2. What This Study Adds
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Office of the United Nations High Commissioner for Refugees. Asylum in the UK. 2014. Available online: http://www.unhcr.org/uk/asylum-in-the-uk.html (accessed on 5 February 2018).
- United Nations High Commissioner for Refugees. Asylum-Seekers. 2014. Available online: http://www.unhcr.org/uk/asylum-seekers.html (accessed on 5 February 2018).
- United Nations Refugee Agency. Global Trends. 2016. Available online: http://www.unhcr.org/globaltrends2016/ (accessed on 5 February 2018).
- Refugee Council of Australia. UNHCR Global Trends. 2015—How Australia Compares with the World. 2015. Available online: https://www.refugeecouncil.org.au/getfacts/statistics/unchr2015/ (accessed on 7 February 2018).
- Refugee Council UK. Quarterly Asylum Statistics. 2016. Available online: https://www.refugeecouncil.org.uk/assets/0004/2697/Asylum_Statistics_Feb_2018.pdf (accessed on 11 February 2018).
- Eurostat Statistics. Asylum Statistics. 2018. Available online: http://ec.europa.eu/eurostat/statistics-explained/index.php/Asylum_statistics (accessed on 11 February 2018).
- Phillip, C. Asylum Seeker Demography: Young and Male. 2013. Available online: http://www.pewglobal.org/2016/08/02/4-asylum-seeker-demography-young-and-male/ (accessed on 1 March 2018).
- The United Nations Children’s Fund. Latest Statistics and Graphics on Refugee and Migrant Children. 2010. Available online: https://www.unicef.org/eca/what-we-do/emergencies/latest-statistics-and-graphics-refugee-and-migrant-children (accessed on 3 March 2018).
- Fletcher, E. Changing Support for Asylum Seekers: An Analysis of Legislation and Parliamentary Debates. SCMR 2008, 1, 1–20. [Google Scholar]
- Frantziou, E.; Staiger, U.; Chaytor, S. Refugee Protection, Migration and Human Rights in Europe. 2014. Available online: https://www.ucl.ac.uk/european-institute/ei-publications/europe-briefing-refugee.pdf (accessed on 5 March 2018).
- National Healthcare Service. Post-Traumatic Stress Disorder (PTSD). 2016. Available online: https://www.nhs.uk/conditions/post-traumatic-stress-disorder-ptsd/ (accessed on 25 March 2018).
- Knaevelsrud, C.; Stammel, N.; Olff, M. Traumatized refugees: Identifying needs and facing challenges for mental health care. Eur. J. Psychotraumatol. 2017, 8, 1388103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Departement of Veterans Affairs. PTSD: National Center for PTSD. 2013. Available online: https://www.ptsd.va.gov/professional/ptsd-overview/dsm5_criteria_ptsd.asp (accessed on 24 March 2018).
- Gourieroux, C. Conn’s Translational Neuroscience; Lowa State Princeton University Press: New Jersey, NJ, USA, 2016. [Google Scholar]
- Tufan, A.E.; Alkin, M.; Bosgelmez, S. Post-traumatic stress disorder among asylum seekers and refugees in Istanbul may be predicted by torture and loss due to violence. Nord. J. Psychiatry 2013, 67, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Nose, M.; Ballette, F.; Bighelli, I.; Turrini, G.; Purgato, M.; Tol, W.; Priebe, S.; Barbui, C. Psychosocial interventions for post-traumatic stress disorder in refugees and asylum seekers resettled in high-income countries: Systematic review and meta-analysis. PLoS ONE 2017, 12, e0171030. [Google Scholar] [CrossRef] [PubMed]
- Reavell, J.; Fazil, Q. The epidemiology of PTSD and depression in refugee minors who have resettled in developed countries. J. Ment. Health 2017, 26, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Hynie, M. The Social Determinants of Refugee Mental Health in the Post-Migration Context: A Critical Review. Can. J. Psychiatry 2018, 63, 297–303. [Google Scholar] [CrossRef] [PubMed]
- PRISMA. PRISMA Checklist. 2009. Available online: http://prisma-statement.org/documents/PRISMA%202009%20checklist.pdf (accessed on 6 April 2018).
- Salford, U.O. Evaluation Tool for Qualitative Studies. 2002. Available online: http://usir.salford.ac.uk/id/eprint/12970/1/Evaluation_Tool_for_Qualitative_Studies.pdf (accessed on 12 February 2019).
- PRISMA. PRISMA Flow Diagram 2009. Available online: http://prisma.thetacollaborative.ca/ (accessed on 12 February 2019).
- Thela, L.; Tomita, A.; Maharaj, V.; Mhlongo, M.; Burns, J.K. Counting the cost of Afrophobia: Post-migration adaptation and mental health challenges of African refugees in South Africa. Transcult. Psychiatry 2017, 54, 715–732. [Google Scholar] [CrossRef] [PubMed]
- Silove, D.; Steel, Z.; McGorry, P.; Mohan, P. Trauma exposure, postmigration stressors, and symptoms of anxiety, depression and post-traumatic stress in Tamil asylum-seekers: Comparison with refugees and immigrants. Acta Psychiatr. Scand. 1998, 97, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Knipscheer, J.W.; Kleber, R.J. The relative contribution of posttraumatic and acculturative stress to subjective mental health among Bosnian refugees. J. Clin. Psychol. 2006, 62, 339–353. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, A.; Nguyen, L.; Wilkinson, J.; Vundla, S.; Raghavan, S.; Miller, K.E.; Keller, A.S. Rates and impact of trauma and current stressors among Darfuri refugees in Eastern Chad. Am. J. Orthopsychiatry 2010, 80, 227–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steel, Z.; Silove, D.; Bird, K.; McGorry, P.; Mohan, P. Pathways from war trauma to posttraumatic stress symptoms among Tamil asylum seekers, refugees, and immigrants. J. Trauma. Stress 1999, 12, 421–435. [Google Scholar] [CrossRef] [PubMed]
- Oren, L.; Possick, C. Is ideology a risk factor for PTSD symptom severity among Israeli political evacuees? J. Trauma. Stress 2010, 23, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Slewa-Younan, S.; Guajardo, M.G.U.; Yaser, A.; Mond, J.; Smith, M.; Milosevic, D.; Smith, C.; Lujic, S.; Jorm, A.F. Causes of and risk factors for posttraumatic stress disorder: The beliefs of Iraqi and Afghan refugees resettled in Australia. Int. J. Ment. Health Syst. 2017, 11, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, H.; Hassan, C.Q. Post-traumatic Stress Disorder Symptoms Resulting from Torture and Other Traumatic Events among Syrian Kurdish Refugees in Kurdistan Region, Iraq. Front. Psychol. 2017, 8, 241. [Google Scholar] [CrossRef] [PubMed]
- Aragona, M.; Pucci, D.; Mazzetti, M.; Geraci, S. Post-migration living difficulties as a significant risk factor for PTSD in immigrants: A primary care study. Ital. J. Public Health 2012, 9, e7525–e7528. [Google Scholar] [CrossRef]
- Hinton, D.E.; Peou, S.; Joshi, S.; Nickerson, A.; Simon, N.M. Normal Grief and Complicated Bereavement among Traumatized Cambodian Refugees: Cultural Context and the Central Role of Dreams of the Dead. Cult. Med. Psychiatry 2013, 37, 427–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinton, D.E.; Hinton, A.L.; Pich, V.; Loeum, J.R.; Pollack, M.H. Nightmares Among Cambodian Refugees: The Breaching of Concentric Ontological Security. Cult. Med. Psychiatry 2009, 33, 219–265. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, A.A.; Bramsen, I.; Deville, W.; van Willigen, L.H.; Hovens, J.E.; van der Ploeg, H.M. Physical and mental health of Afghan, Iranian and Somali asylum seekers and refugees living in the Netherlands. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Hameed, S.; Sadiq, A.; Din, A.U. The Increased Vulnerability of Refugee Population to Mental Health Disorders. Kans. J. Med. 2018, 11, 20–23. [Google Scholar] [CrossRef] [Green Version]
- Li, S.S.Y.; Liddell, B.J.; Nickerson, A. The Relationship between Post-Migration Stress and Psychological Disorders in Refugees and Asylum Seekers. Curr. Psychiatry Rep. 2016, 18, 82. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Limitation | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Age | Adults (over 18) | Less than 18 |
| Relevance | Causes and risk factors of PTSD in asylum seekers and refugees | Treatment and interventions of PTSD in asylum seekers and refugees |
| Study design | Primary research | Systematic review |
| Study Number | Author(s) & Year | Study Type | Examples of Questions Asked | Study Sample, Gender & Mean Age | Participants’ Country of Origin | Location of Study | Title/Aim of Study | Main Causes/Findings |
|---|---|---|---|---|---|---|---|---|
| 1 | Lindokuhle et al. [22] (2017) | Survey study | 25-item Hopkins Symptom Checklist + 30-item Harvard Trauma Questionnaire | Study sample = 355 Males = 188 Females = 167 Mean age = 32.8 | Democratic Republic of Congo, Zimbabwe, Rwanda, Malawi, Ghana, Uganda populations | South Africa | Finding out the extent of causation of post-migration factors on 3 mental health outcomes (depression, anxiety, PTSD) | 1-Shorter time span since migrating increased the likelihood of PTSD. 2-Prolonged exposure to discrimination increased the likelihood of PTSD. |
| 2 | Silove et at. [23] (1998) | Survey study | 30-item Harvard Trauma Questionnaire | Study sample = 62 Males = 48 Females = 14 Mean age = 35.3 | Tamil population | Australia | Comparison of post migration stress factors, Anxiety, depression and PTSD levels between asylum seekers and refugees | 1-Larger number of post-migration stress factors (i.e., delays in processing application and no permission to work) were found in asylum seekers compared to refugees. 2-Higher prevalence of torture in asylum seekers (6.7 ± 3.3) compared to refugees (6.3 ± 5.7) index of mean trauma exposure. |
| 3 | Knipscheer et al. [24] (2006) | Survey study | No details | Sample size = 78 Males = 48 Females = 30 Mean age = 42.9 | Bosnian population | Holland | The contribution of post migration trauma and acculturation stress to the health of the Bosnian refugees in Holland | 1-War experiences increased the likelihood of developing mental health problems. 2-Inability to practice and preserve religious traditions was associated with an increase in mental health problems. |
| 4 | Rasmussen et al. [25] (2011) | A case study questionnaire/interview conducted alongside the United Nations High Commissioner for Refugees (UNHCR) psychosocial programme | 30-item Harvard Trauma Questionnaire | Sample size = 848 Males = 296 Females = 552 Mean age = Not specified | Darfuri population | Eastern Chad | The impact of past trauma and everyday stressors on the mental and psychological wellbeing of refugees and asylum seekers | 1-The lack of basic needs and not feeling safe were strongly associated with PTSD development. 2-Pre-migration stressors, such as being chased, shot or bombed were strongly associated with PTSD. 3-Religion and ideologies played an important role in whether Refugees developed PTSD (mainly females).where a strong ideologies or religious beliefs increased their likelihood of PTSD |
| 5 | Steel et al. [26] (1999) | Case study | 30-item Harvard Trauma Questionnaire | Sample size = 196 Males = 135 Females = 61 Mean age = 43.7 | Tamil population | Australia | The role of Pre migration and post migration stressor in developing PTSD symptoms in the Tamil population living in Australia | 1-Being held in detention and enduring sexual/physical abuse were strongly linked to PTSD symptoms. 2-The inability to adapt to new surroundings increased symptoms of PTSD. |
| 6 | Hinton et al. [31] (2013) | Case report | Not clear | Not specified Mean age = 49.4 | Cambodian population | USA | How grief and complicated bereavement of Cambodian refugees play a role in PTSD symptoms | 1-Recall of the dead and its connotations interpreted in Cambodian culture are a strong indicator for PTSD. |
| 7 | Oren et al. [27] (2010) | Survey study | 30-item Harvard Trauma Questionnaire | Sample size = 326 Males = 114 Females = 212 Mean age = 32.5 | Evacuated Israelis | Western Bank | The role of ideology as a cause for PTSD symptoms and severity | 1-Firm ideologies and political stances within a stressful environment linked to the development of PTSD symptoms. 2-The older the person with strong ideological beliefs, the more likely that they will develop PTSD (females). |
| 8 | Hinton et al. [32] (2009) | Case report | Not clear | Not specified | Cambodian population | USA | The role of nightmares within the Cambodian refugee population and its potential role in causing PTSD | 1-Those who suffer from nightmares/flashbacks within the Cambodian population exhibit higher levels of PTSD. |
| 9 | Slewa-Younan et al. [28] (2017) | Survey study | The mental health literacy survey | Sample size = 375 Males= 169 Female = 206 Mean age = 32.5 | Iraqi and Afghanistan population | Australia | The viewpoints and beliefs of the Iraqi and Afghan refugees concerning the causes and risk factors of PTSD | 1-Prolonged exposure to being beaten up and abused, either physically or mentally, were the most common beliefs to cause PTSD. 2-Being born in a ‘war-filled environment’ was a common belief held by the Iraqi and Afghan refugees to causing PTSD. |
| 10 | Ibrahim et al. [29] (2017) | Survey study | Demographic Data Questionnaire + 30-item Harvard Trauma Questionnaire | Sample size = 91 Males = 51 Females = 40 Mean age = 29.9 | Syrian Kurdish | Kurdistan (Iraq) | The link between traumatic events and PTSD development in the Syrian Kurdish population living in Kurdistan | 1-Positive correlation between frequency of torture and severity of PTSD. 2-Strong link between number of trauma events (near-death experiences or witnessing death) and PTSD symptoms. |
| 11 | Aragona et al. [30] (2012) | Qualitative study | 30-item Harvard Trauma Questionnaire | Sample size = 339 Males = 245 Females = 94 Mean age = 37.8 | Mostly Romanian, Chinese and Bangladesh populations | Italy | The link between post migration stressors and PTSD development in immigrants | 1-Inability to work was the most commonly reported link to developing PTSD (survey results). 2-The higher the number of post-migration stressors, the stronger the association with PTSD. |
| 12 | Gerritsen et al. [33] (2006) | Qualitative study | Harvard Trauma Questionnaire and the Hopkins Symptoms Checklist-25 + short form 36 | Sample size = 410 Males = 241 Females = 169 Mean age = 37.0 | Afghanistan, Iran and Somalia | Hollands | The prevalence rates and risk factors for physical and mental wellbeing (including PTSD) | 1-Female gender was strongly linked to the development of PTSD. 2-Strong link between number of trauma events and PTSD symptoms. 3-Asylum seekers had a higher PTSD prevalence rate than the refugee population. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlRefaie, A.; Dowrick, C. Causes and Risk Factor of Post-Traumatic Stress Disorder in Adult Asylum Seekers and Refugees. Psychiatry Int. 2021, 2, 410-423. https://doi.org/10.3390/psychiatryint2040032
AlRefaie A, Dowrick C. Causes and Risk Factor of Post-Traumatic Stress Disorder in Adult Asylum Seekers and Refugees. Psychiatry International. 2021; 2(4):410-423. https://doi.org/10.3390/psychiatryint2040032
Chicago/Turabian StyleAlRefaie, Abdullah, and Christopher Dowrick. 2021. "Causes and Risk Factor of Post-Traumatic Stress Disorder in Adult Asylum Seekers and Refugees" Psychiatry International 2, no. 4: 410-423. https://doi.org/10.3390/psychiatryint2040032
APA StyleAlRefaie, A., & Dowrick, C. (2021). Causes and Risk Factor of Post-Traumatic Stress Disorder in Adult Asylum Seekers and Refugees. Psychiatry International, 2(4), 410-423. https://doi.org/10.3390/psychiatryint2040032