
The Recognition of Attention Deficit Hyperactivity Disorder, Autism Spectrum Disorder and Conduct Disorder in Adolescents and Adults—Assessing Differences in Mental Health Literacy

Abstract
:1. Introduction
1.1. Personal Factors
1.2. Childhood Disorders
2. Materials and Methods
2.1. Participants
2.2. Instrument
2.3. Procedure
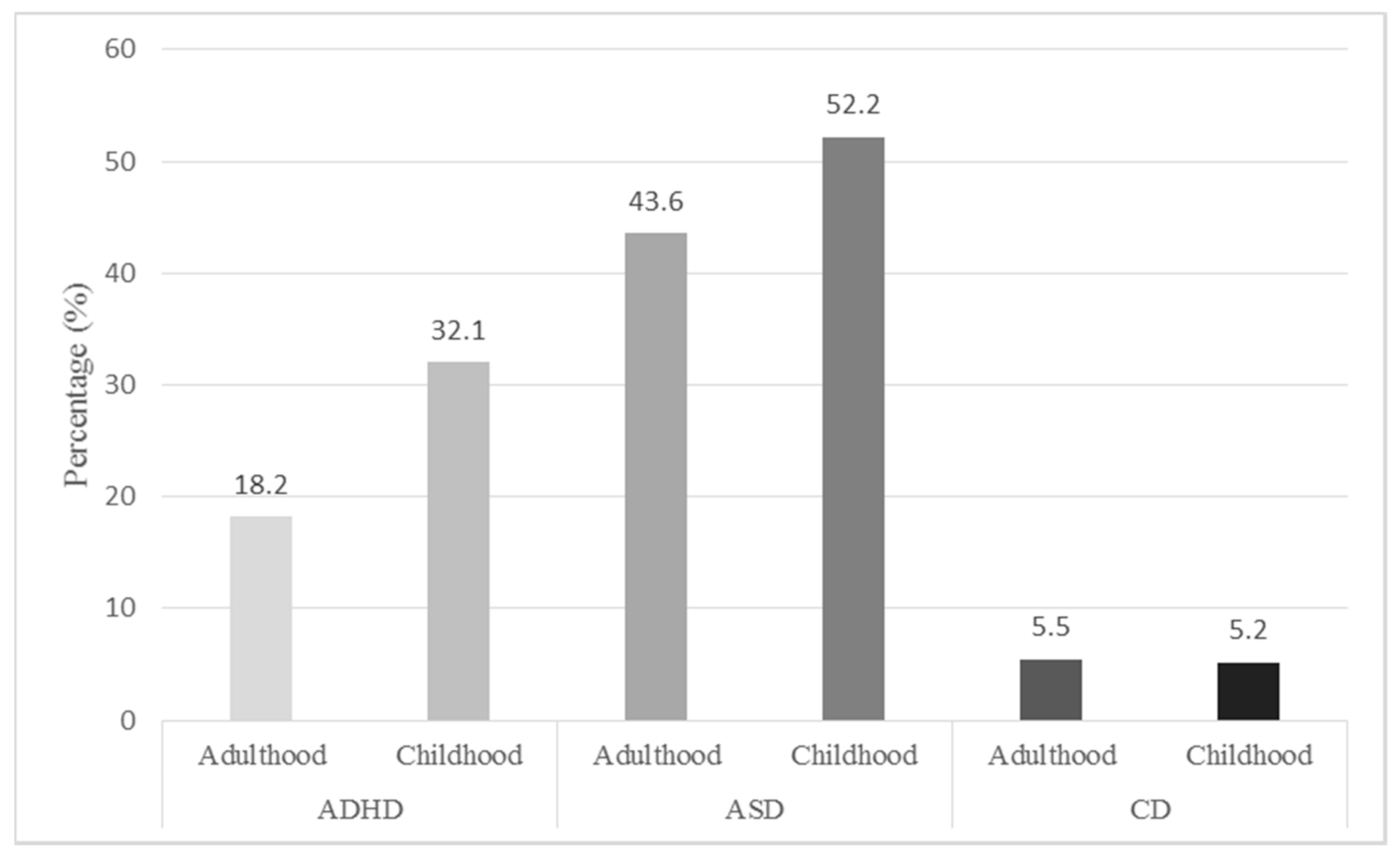
3. Results
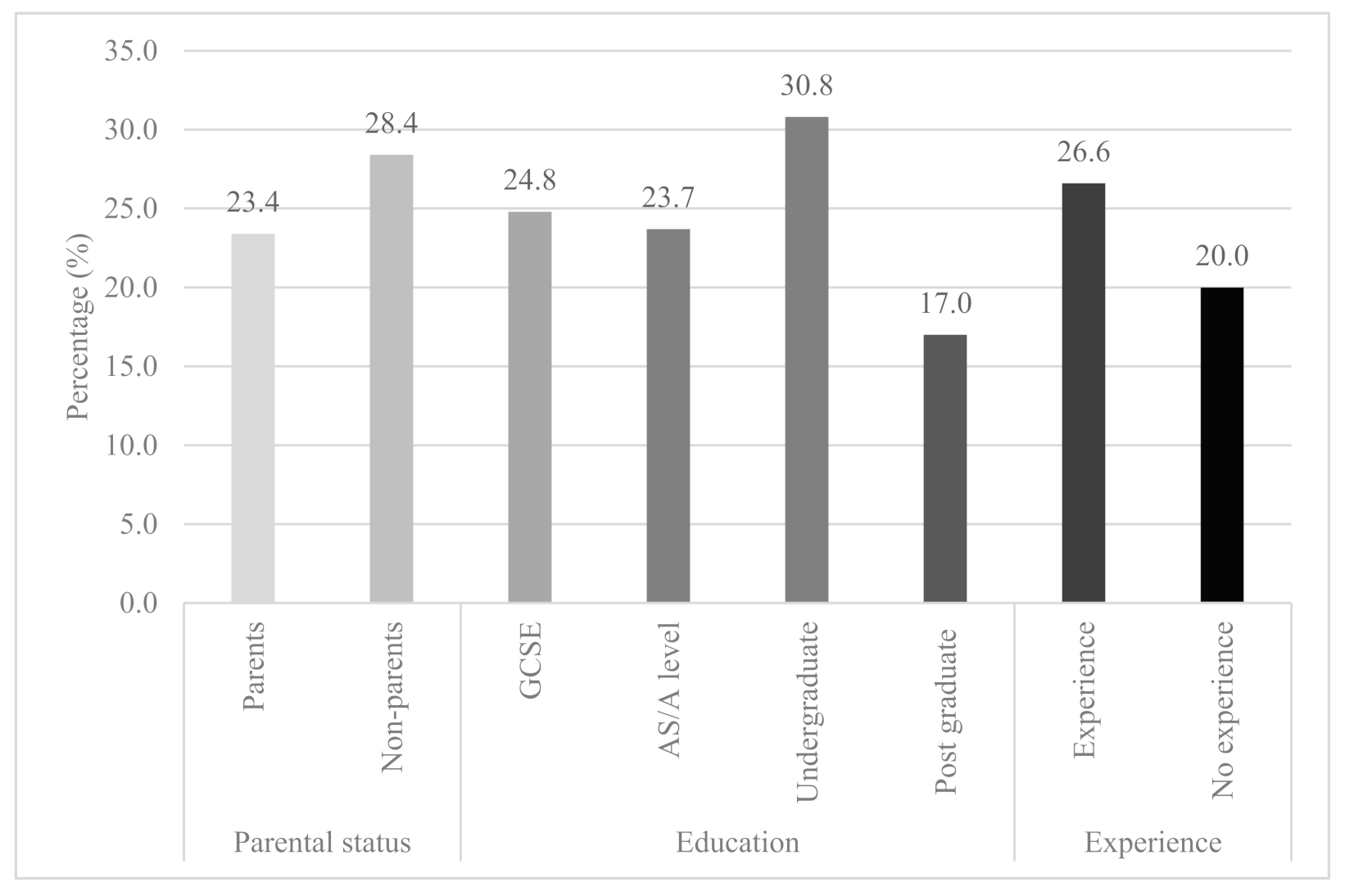
3.1. ADHD
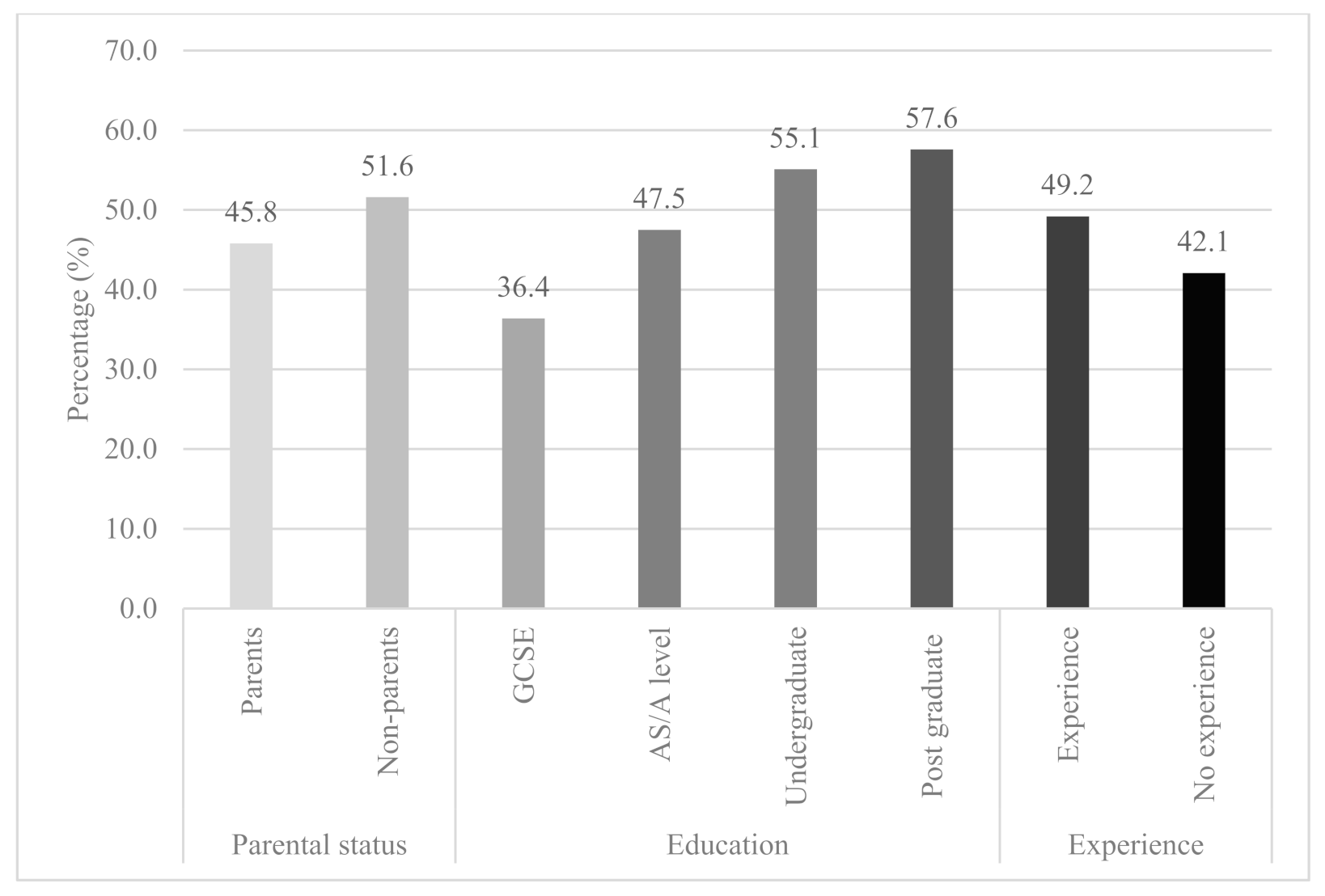
3.2. ASD
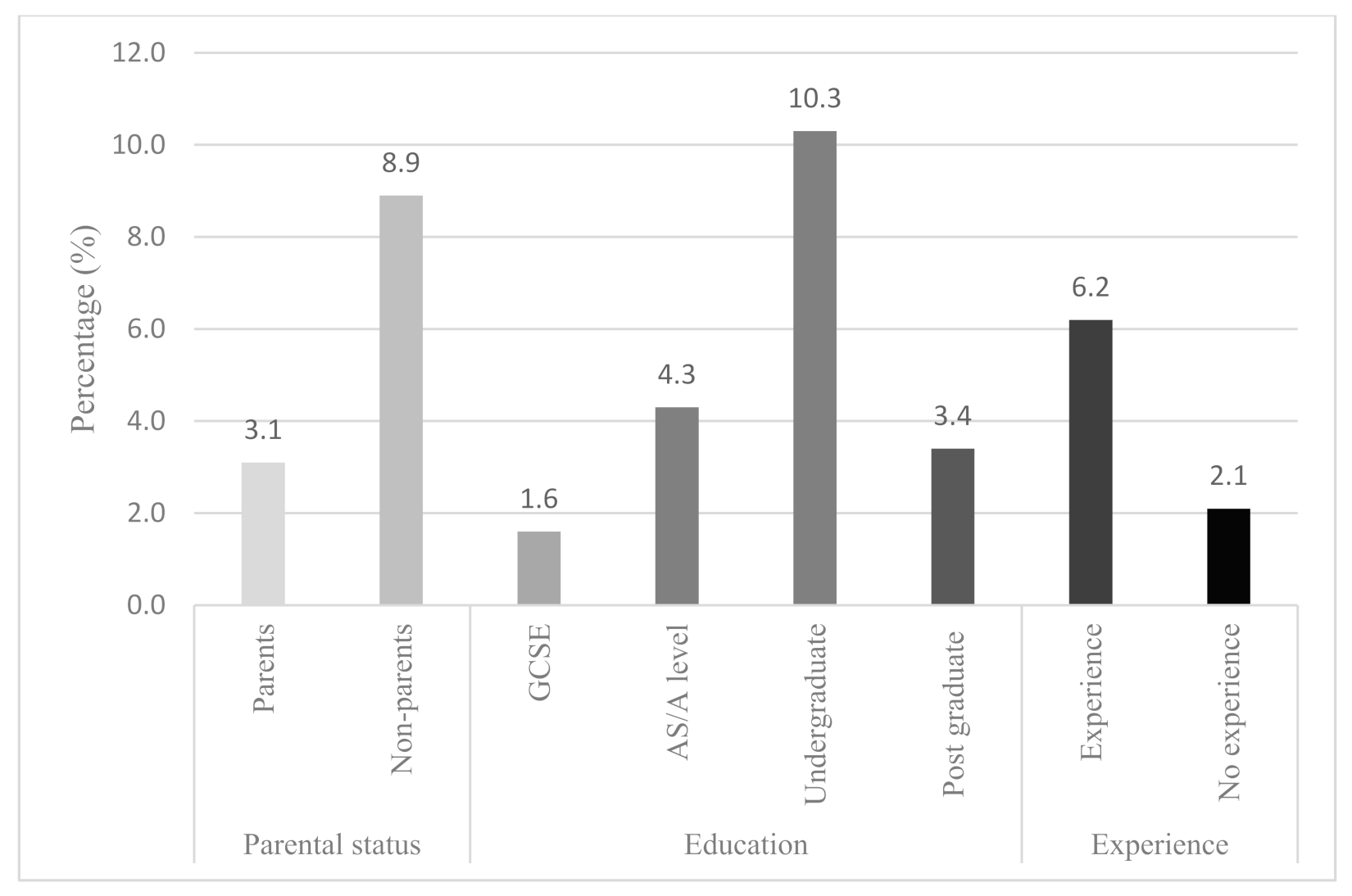
3.3. CD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Jorm, A.F.; Korten, E.A.; Jacomb, A.P.; Christensen, H.; Rodgers, B.; Pollitt, P. “Mental health literacy”: A survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Med. J. Aust. 1997, 166, 182–186. [Google Scholar] [CrossRef]
- Kelly, C.M.; Jorm, A.F.; Wright, A. Improving mental health literacy as a strategy to facilitate early intervention for mental disorders. Med. J. Aust. 2007, 187, S26–S30. [Google Scholar] [CrossRef]
- Rüsch, N.; Evans-Lacko, S.E.; Henderson, C.; Flach, C.; Thornicroft, G. Knowledge and Attitudes as Predictors of Intentions to Seek Help for and Disclose a Mental Illness. Psychiatr. Serv. 2011, 62, 675–678. [Google Scholar] [CrossRef]
- Furnham, A.; Hamid, A. Mental health literacy in non-western countries: A review of the recent literature. Ment. Health Rev. J. 2014, 19, 84–98. [Google Scholar] [CrossRef]
- Kutcher, S.; Wei, Y.; Coniglio, C. Mental Health Literacy. Can. J. Psychiatry 2016, 61, 154–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorm, A. Why do we need the concept of “Mental Health Literacy”. Health Commun. 2015, 30, 1166–1168. [Google Scholar] [CrossRef] [PubMed]
- Furnham, A.; Swami, V. Mental Health Literacy: A Review of What It Is and Why It Matters. Int. Perspect. Psychol. Res. Pract. Consult. 2018, 7, 240–257. [Google Scholar] [CrossRef]
- Furnham, A.; Petropoulou, K. Mental health literacy, sub-clinical personality disorders and job fit. J. Ment. Health 2018, 28, 249–254. [Google Scholar] [CrossRef]
- Born, C.G.; McClelland, A.; Furnham, A. Mental health literacy for autism spectrum disorder and depression. Psychiatry Res. 2019, 279, 272–277. [Google Scholar] [CrossRef]
- Swami, V.; Barron, D.; Smith, L.; Furnham, A. Mental health literacy of maternal and paternal postnatal (postpartum) depression in British adults. J. Ment. Health 2019, 29, 217–224. [Google Scholar] [CrossRef]
- Angermeyer, M.C.; Dietrich, S. Public beliefs about and attitudes towards people with mental illness: A review of population studies. Acta Psychiatr. Scand. 2006, 113, 163–179. [Google Scholar] [CrossRef] [PubMed]
- Coles, M.E.; Coleman, S.L. Barriers to treatment seeking for anxiety disorders: Initial data on the role of mental health literacy. Depress. Anxiety 2010, 27, 63–71. [Google Scholar] [CrossRef]
- Link, B.G.; Phelan, J.C.; Bresnahan, M.; Stueve, A.; A Pescosolido, B. Public conceptions of mental illness: Labels, causes, dangerousness, and social distance. Am. J. Public Health 1999, 89, 1328–1333. [Google Scholar] [CrossRef] [Green Version]
- Reavley, N.J.; McCann, T.V.; Jorm, A.F. Mental health literacy in higher education students. Early Interv. Psychiatry 2011, 6, 45–52. [Google Scholar] [CrossRef]
- Wright, A.; Jorm, A.F.; Harris, M.G.; McGorry, P.D. What’s in a name? Is accurate recognition and labelling of mental disorders by young people associated with better help-seeking and treatment preferences? Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 244–250. [Google Scholar] [CrossRef]
- Furnham, A.; Winceslaus, J. Psychiatric Literacy and the Personality Disorders. Psychopathology 2012, 45, 29–41. [Google Scholar] [CrossRef]
- Rim, S.J.; Park, S.; Lee, Y.; Kim, C.E. Mental Health Literacy of Autism Spectrum Disorder in Korea: Recognition, Etiology, Treatment. Psychiatry Investig. 2019, 16, 213–219. [Google Scholar] [CrossRef]
- Vovou, F.; Hull, L.; Petrides, K.V. Mental health literacy of ADHD, autism, schizophrenia, and bipolar disorder: A cross-cultural investigation. J. Ment. Health 2020, 1–11. [Google Scholar] [CrossRef]
- Gulliver, A.; Griffiths, K.M.; Christensen, H. Perceived barriers and facilitators to mental health help-seeking in young people: A systematic review. BMC Psychiatry 2010, 10, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shurka, E. Attitudes of Israeli Arabs Towards the Mentally Ill. Int. J. Soc. Psychiatry 1983, 29, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Lauber, C.; Ajdacic-Gross, V.; Fritschi, N.; Stulz, N.; Rössler, W. Mental health literacy in an educational elite–An online survey among university students. BMC Public Health 2005, 5, 44. [Google Scholar] [CrossRef] [Green Version]
- Wright, A.; Jorm, A.F. Labels Used by Young People to Describe Mental Disorders: Factors Associated with Their Development. Aust. N. Z. J. Psychiatry 2009, 43, 946–955. [Google Scholar] [CrossRef]
- Belfer, M.L. Child and adolescent mental disorders: The magnitude of the problem across the globe. J. Child Psychol. Psychiatry 2008, 49, 226–236. [Google Scholar] [CrossRef]
- De Berardis, D.; De Filippis, S.; Masi, G.; Vicari, S.; Zuddas, A. A Neurodevelopment Approach for a Transitional Model of Early Onset Schizophrenia. Brain Sci. 2021, 11, 275. [Google Scholar] [CrossRef]
- Furnham, A.; Leno, V.C. Psychiatric literacy and the conduct disorders. Res. Dev. Disabil. 2012, 33, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, D.; Musso, P.; Verrocchio, M.C.; Manna, G.; Kopala-Sibley, D.C.; De Berardis, D.; De Santis, S.; Falgares, G. Childhood maltreatment, personality vulnerability profiles, and borderline personality disorder symptoms in adolescents. Dev. Psychopathol. 2021, 26, 1–14. [Google Scholar] [CrossRef]
- Ullah, I.; Razzaq, A.; De Berardis, D.; Ori, D.; Adiukwu, F.; Shoib, S. Mental health problems in children & pandemic: Dangers lurking around the Corner and possible management. Int. J. Soc. Psychiatry 2021, 7, 2816. [Google Scholar] [CrossRef]
- Horton-Salway, M. Repertoires of ADHD in UK newspaper Med.ia. Health Interdiscip. J. Soc. Study Health Illn. Med. 2011, 15, 533–549. [Google Scholar] [CrossRef]
- Able, S.L.; Johnston, J.A.; Adler, L.A.; Swindle, R.W. Functional and psychosocial impairment in adults with undiagnosed ADHD. Psychol. Med. 2006, 37, 97–107. [Google Scholar] [CrossRef]
- Kooij, S.J.; Bejerot, S.; Blackwell, A.; Caci, H.; Casas-Brugué, M.; Carpentier, P.J.; Edvinsson, D.; Fayyad, J.; Foeken, K.; Fitzgerald, M.; et al. European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD. BMC Psychiatry 2010, 10, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekle, B. Knowledge and attitudes about Attention-Deficit Hyperactivity Disorder (ADHD): A comparison between practicing teachers and undergraduate education students. J. Atten. Disord. 2004, 7, 151–161. [Google Scholar] [CrossRef]
- Brugha, T.; Cooper, S.A.; McManus, S.; Purdon, S.; Smith, J.; Scott, F.J.; Tyrer, F. Estimating the Prevalence of Autism Spectrum Conditions in Adults: Extending the 2007 Adult Psychiatric Morbidity Survey. The Health and Social Care Information Centre (NHS). 2012. Available online: http://www.wecommunities.org/MyNurChat/archive/LDdownloads/Est_Prev_Autism_Spec_Cond_in_Adults_Report.pdf (accessed on 1 July 2020).
- Koyama, T.; Tachimori, H.; Sawamura, K.; Koyama, A.; Naganuma, Y.; Makino, H.; Takeshima, T. Mental health literacy of autism spectrum disorders in the Japanese general population. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 44, 651–657. [Google Scholar] [CrossRef]
- Furnham, A.; Buck, C. A comparison of lay-beliefs about autism and obsessive-compulsive disorder. Int. J. Soc. Psychiatry 2003, 49, 287–307. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: New York, NY, USA, 2013. [Google Scholar]
- Fischer, M.; Barkley, R.A.; Smallish, L.; Fletcher, K. Young Adult Follow-Up of Hyperactive Children: Self-Reported Psychiatric Disorders, Comorbidity, and the Role of Childhood Conduct Problems and Teen CD. J. Abnorm. Child Psychol. 2002, 30, 463–475. [Google Scholar] [CrossRef]
- Kelly, C.M.; Jorm, A.F. Stigma and mood disorders. Curr. Opin. Psychiatry 2007, 20, 13–16. [Google Scholar] [CrossRef]
- Cotton, S.M.; Wright, A.; Harris, M.G.; Jorm, A.F.; McGorry, P.D. Influence of Gender on Mental Health Literacy in Young Australians. Aust. N. Z. J. Psychiatry 2006, 40, 790–796. [Google Scholar] [CrossRef]
- De Boer, A.; Pijl, S.J. The acceptance and rejection of peers with ADHD and ASD in general secondary education. J. Educ. Res. 2016, 109, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Gong, A.T.; Furnham, A. Mental health literacy: Public knowledge and beliefs about mental disorders in mainland China. PsyCh J. 2014, 3, 144–158. [Google Scholar] [CrossRef] [PubMed]
- Swami, V. Mental health literacy of attention-deficit hyperactivity disorder (ADHD). In Health Literacy: Developments, Issues, and Outcomes; Moore, R., Perry, D., Eds.; Nova Science Publishers: Hauppauge, NY, USA, 2013. [Google Scholar]
- Kim-Cohen, J.; Caspi, A.; Moffitt, T.E.; Harrington, H.; Milne, B.J.; Poulton, R. Prior Juvenile Diagnoses in Adults With Mental Disorder. Arch. Gen. Psychiatry 2003, 60, 709–717. [Google Scholar] [CrossRef]
- Evans-Lacko, S.; Corker, E.; Williams, P.; Henderson, C.; Thornicroft, G. Effect of the Time to Change anti-stigma campaign on trends in mental-illness-related public stigma among the English population in 2003–2013: An analysis of survey data. Lancet Psychiatry 2014, 1, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Möller-Leimkühler, A.M. The gender gap in suicide and premature death or: Why are men so vulnerable? Eur. Arch. Psychiatry Clin. Nuerosci. 2003, 253, 1–8. [Google Scholar] [CrossRef]
- McKeon, P.; Carrick, S. Public attitudes to depression: A national survey. Ir. J. Psychol. Med. 1991, 8, 116–121. [Google Scholar] [CrossRef]
- Jorm, A.F.; Korten, A.E.; Jacomb, P.A.; Rodgers, B.; Pollitt, P.; Christensen, H.; Henderson, S. Helpfulness of interventions for mental disorders: Beliefs of health professionals compared with the general public. Br. J. Psychiatry 1997, 171, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Sai, G.; Furnham, A. Identifying depression and schizophrenia using vignettes: A methodological note. Psychiatry Res. 2013, 210, 357–362. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dependent Variables | |||
|---|---|---|---|
| Seriousness | Likelihood of Disorder | ||
| ADHD | Adulthood | M = 64.53 (SD = 18.67) | M = 62.73 (SD = 24.25) |
| Childhood | M = 64.52 (SD = 20.67) | M = 53.00 (SD = 27.01) | |
| ASD | Adulthood | M = 50.53 (SD = 23.83) | M = 56.20 (SD = 28.37) |
| Childhood | M = 58.35 (SD = 23.24) | M = 59.75 (SD =27.19) | |
| CD | Adulthood | M = 79.99 (SD = 20.08) | M = 59.27 (SD = 30.50) |
| Childhood | M = 79.49 (SD = 19.20) | M = 55.78 (SD = 27.89) | |
| Dependent Variables | |||
|---|---|---|---|
| Seriousness | Likelihood of Disorder | ||
| Parental Status | Parents | M = 67.51 (SD = 19.47) | M = 58.30 (SD = 26.52) |
| Non-parents | M = 59.88 (SD = 19.21) | M = 56.86 (SD = 25.58) | |
| Education Level | GCSE/10th Grade | M = 66.93 (SD = 20.36) | M = 57.40 (SD = 28.42) |
| AS/A level 12th Grade | M = 63.94 (SD = 21.35) | M = 58.10 (SD = 25.09) | |
| Undergraduate | M = 62.13 (SD = 17.80) | M = 57.94 (SD = 25.11) | |
| Post graduate | M = 66.83 (SD = 18.83) | M = 58.19 (SD = 26.03) | |
| Experience | Experience | M = 65.11 (SD = 19.32) | M = 58.74 (SD = 25.89) |
| No experience | M = 62.86 (SD = 20.94) | M = 53.6 (SD = 26.79) | |
| Dependent Variables | |||
|---|---|---|---|
| Seriousness | Likelihood of Disorder | ||
| Parental Status | Parents | M = 56.73 (SD = 24.14) | M = 57.94 (SD = 28.08) |
| Non-parents | M = 51.15 (SD = 22.99) | M = 58.15 (SD = 27.43) | |
| Education Level | GCSE/10th Grade | M = 54.98 (SD = 22.85) | M = 56.33 (SD = 25.90) |
| AS/A level 12th Grade | M = 52.86 (SD = 25.45) | M = 57.47 (SD = 29.24) | |
| Undergraduate | M = 52.71 (SD = 22.50) | M = 59.44 (SD = 27.19) | |
| Post graduate | M = 63.69 (SD = 22.97) | M = 61.17 (SD = 28.66) | |
| Experience | Experience | M = 55.29 (SD = 24.34) | M = 58.38 (SD = 27.82) |
| No experience | M = 51.46 (SD = 21.72) | M = 56.18 (SD = 28.25) | |
| Dependent Variables | |||
|---|---|---|---|
| Seriousness | Likelihood of Disorder | ||
| Parental Status | Parents | M = 81.24 (SD = 19.49) | M = 59.60 (SD = 29.06) |
| Non-parents | M = 77.55 (SD = 19.57) | M = 54.15 (SD = 29.19) | |
| Education Level | GCSE | M = 79.82 (SD = 21.09) | M = 60.24 (SD = 29.64) |
| AS/A level | M = 80.08 (SD = 20.30) | M = 56.94 (SD = 30.93) | |
| Undergraduate | M = 80.57 (SD = 16.50) | M = 56.56 (SD = 26.61) | |
| Post graduate | M = 77.14 (SD = 22.23) | M = 56.36 (SD = 30.56) | |
| Experience | Experience | M = 79.84 (SD = 19.49) | M = 58.24 (SD = 29.15) |
| No experience | M = 78.99 (SD= 20.18) | M = 54.27 (SD= 29.76) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peters, B.; Furnham, A. The Recognition of Attention Deficit Hyperactivity Disorder, Autism Spectrum Disorder and Conduct Disorder in Adolescents and Adults—Assessing Differences in Mental Health Literacy. Psychiatry Int. 2021, 2, 145-158. https://doi.org/10.3390/psychiatryint2020011
Peters B, Furnham A. The Recognition of Attention Deficit Hyperactivity Disorder, Autism Spectrum Disorder and Conduct Disorder in Adolescents and Adults—Assessing Differences in Mental Health Literacy. Psychiatry International. 2021; 2(2):145-158. https://doi.org/10.3390/psychiatryint2020011
Chicago/Turabian StylePeters, Baylee, and Adrian Furnham. 2021. "The Recognition of Attention Deficit Hyperactivity Disorder, Autism Spectrum Disorder and Conduct Disorder in Adolescents and Adults—Assessing Differences in Mental Health Literacy" Psychiatry International 2, no. 2: 145-158. https://doi.org/10.3390/psychiatryint2020011
APA StylePeters, B., & Furnham, A. (2021). The Recognition of Attention Deficit Hyperactivity Disorder, Autism Spectrum Disorder and Conduct Disorder in Adolescents and Adults—Assessing Differences in Mental Health Literacy. Psychiatry International, 2(2), 145-158. https://doi.org/10.3390/psychiatryint2020011