Abstract
Background: Studies have shown an increased risk of asthma in patients with psoriasis and vice versa. Thus, we conducted a meta-analysis to estimate the pooled association between these two chronic inflammatory diseases. Methods: A systematic search of the literature was conducted through March 2023. Risk ratios (RRs) and prevalence were calculated. Results: A total of 11 studies comprising 110,978 patients with psoriasis and 1,898,071 controls were included in the first meta-analysis. The prevalence of asthma in patients with psoriasis was 9.2% (0.075, 0.110), and the pooled risk ratio (RR) was 1.43 (1.23,1.66). Subgroup analysis showed that older patients (≥50 years) have a higher pooled risk of asthma [RR 1.59 (1.41, 1.79)] than younger patients (20–49 years) [RR 1.23 (1.07,1.41)]. In addition, a significantly higher risk of asthma was seen in patients with moderate to severe psoriasis [RR 1.48 (1.17, 1.88)) when compared to their controls than those with mild psoriasis [RR 1.28 (1.14, 1.44)]. A total of 3 studies comprising 468,869 asthma patients and 11,063,349 control were included in the second meta-analysis. The prevalence of psoriasis in asthma patients was 1.3%, 0.004, 0.029), and the pooled risk ratio was 1.23 (1.02,1.47). Conclusions: This meta-analysis provides clear evidence for the bidirectional association between asthma and psoriasis.
1. Introduction
Psoriasis is a chronic immune-mediated inflammatory disease (IMID) that affects the skin and sometimes the joints and has been postulated as a systemic disease [1]. Psoriasis affects approximately 3% of adults and 0.1% of children and adolescents in the U.S.A [2,3] and ranges from 0.09% to 11.4%, most commonly in the 50–69 age group of the worldwide population [4]. Numerous studies have provided compelling evidence for a genetic predisposition to psoriasis [5,6], which has been shown to be associated with several comorbidities [7,8,9], and other IMIDs [10].
The immunopathogenesis of psoriasis involves an inflammatory response with T-helper (Th1 and Th17) activation with resulting production of interleukin (IL)-23/17 [11,12]. Recent studies have found an association between psoriasis and asthma [13], a chronic condition that affects the airways in the lung. Recently, based on the status of Th2 inflammation, the disease has been classified into Th2-high asthma (increased blood eosinophil counts or elevations of fractional exhaled nitric oxide (FeNo)); Th2-low asthma (neutrophilic asthma and paucigranulocytic asthma); and mixed granulocytic asthma (eosinophilic and neutrophilic airway inflammation) [14]. In contrast to psoriasis, Th2 inflammation is the most important immunopathological process in asthma, with approximately 50% of mild-to-moderate asthma and a large portion of severe asthma induced by Th2-dependent inflammation [15]. The downstream pathways of Th2-high asthma include the generation of IL-4, IL-13, eosinophilia, and IgE production, and this is the asthma type in which T2 biologics that block the IgE, IL-5, and IL-4/IL-13 pathways are most likely to achieve clinical efficacy [16]. In non-Th2-high asthma, IL-17A is a major characteristic cytokine [17,18]. IL-17 immunity has been associated with asthma exacerbation [19,20], but it is not clear if this association is part of the asthma phenotype or just a response to insult [21]. Choy et al., in a study of 51 asthma patients with a range of clinical severities, demonstrated that asthma could be divided into three immunological clusters: Th2-high (regulated by IL-13), Th17-high (regulated by IL-17A), and Th2/17-low. Th2-high and Th17-high were inversely correlated in this cohort, and observations in animal models demonstrated that neutralizing one signature promoted the other, suggesting they could be mutually exclusive [22]. More recent evidence shows that inflammation-independent processes also contribute to asthma pathogenesis [15].
Epidemiological studies and meta-analyses have shown the association between asthma and psoriasis and vice-versa [9,10,13,23,24,25,26,27,28,29,30,31,32,33]. Furthermore, the Th-17–high (IL-7-high) asthma phenotype has been found to resemble the immunophenotype of psoriasis. For example, in a study by Ostling et al., expressed genes in patients with IL-17-high asthma were shared with those reported as altered in psoriasis lesions and included genes regulating epithelial barrier function and defense mechanisms [21]. The role of IL-17 in asthma is less well-defined than the role of the Th2-high type, but in general, this type seems to be characterized by neutrophilic airway inflammation and a diminished responsiveness to corticosteroids [34]. One potential shared pathological mechanism between asthma and psoriasis includes the IL-23/Th17 axis, summarized in Figure 1, which involves antigen-induced neutrophil recruitment into the epithelial airway and skin as well as the enhancement of Th2 cell-mediated eosinophil recruitment into the airways [35]. Even though IL-23 is not critical for the polarization of naïve T-cells CD4+ to Th17, IL-23 is important for Th17 survival and effector function [36,37]. Th17 produces IL-17A and IL-17F, which are elevated in some individuals with asthma and may be responsible for the neutrophilic inflammation seen in steroid-resistant asthma [38,39]. Although primarily involved in neutrophil recruitment, the IL-23/Th17 pathway may also enhance eosinophilic inflammation, as observed in animal models [40]. In psoriasis, the efficacy of the anti-IL-12/23 biologic agent (ustekinumab) in clinical trials demonstrates the importance of this pathway in the treatment of adults with moderate to severe plaque psoriasis [41,42,43,44,45].
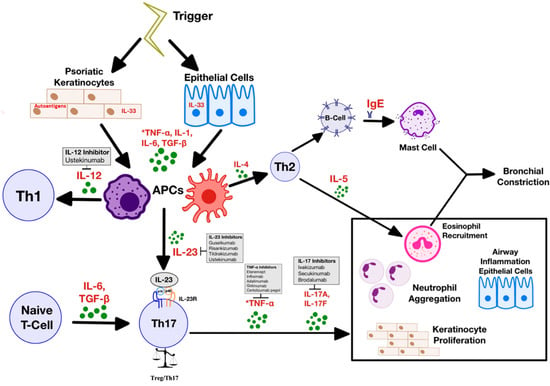
Figure 1.
Shared chronic inflammation pathways in psoriasis and asthma. Once triggered, psoriatic keratinocytes and airway epithelial cells become a source of innate immune mediators, notably dendritic cells [46]. In psoriasis, a Th1 response dominates the adaptive immune response that follows, while in asthma, in most cases, a Th2 response dominates. IL-23 derived from DCs and macrophages [47,48,49], but also bronchial epithelial cells [50] and keratinocytes [51], is involved in the proliferation of IL-17-producing Th17 cells [52]. IL-17 enhances keratinocyte proliferation in psoriatic patients, neutrophil aggregation, and Th2-cell-mediated eosinophil recruitment in airway inflammation [35]. Neutrophil aggregation in keratinocyte regions and airway epithelial cells may amplify the IL-17 environment [36]. Biological medications that target specific parts of the pathway are shown.
In this study, we updated the previous meta-analysis [13] on asthma in patients with psoriasis vs. controls and included a new meta-analysis on psoriasis in patients with asthma vs. controls to show the potential bidirectionality of the association.
2. Materials and Methods
This systematic review and meta-analysis was completed according to the PRISMA guidelines [53], and the protocol was pre-registered and published in PROSPERO (CRD42023405801).
2.1. Data Sources and Search Strategy
A comprehensive search on MEDLINE and SCOPUS was conducted to assess the prevalence of asthma in patients with psoriasis and vice-versa, using the keywords of (asthma) AND (psoriasis). The search was restricted to English but was not limited by date.
2.2. Study Selection and Eligibility
Citations from each database were merged into Zotero, and duplicates were removed. The titles and abstracts were screened by two reviewers (M.E.R. and P.R.) for eligibility, after which the full text of articles meeting the inclusion criteria were further examined for inclusion in this review. Any differences in study eligibility were resolved through discussion. The selection criteria for included studies in the meta-analysis were as follows: (1) cohort, case-control, or cross-sectional design; (2) analyzed the prevalence or incidence of asthma in patients with psoriasis or vice versa; (3) inclusion of a reference group. The exclusion criteria were: (1) publications based on cell or animal models; (2) reviews, comments, abstracts, and case reports.
2.3. Data Extraction
Two independent reviewers (M.E.R., P.R.) extracted the following information from eligible studies: first author, study design, study source and site, study design, ethnicity, diagnostic criteria, number of cases of asthma in psoriatic vs. controls and cases of psoriasis in asthma vs. control, and age of patients.
2.4. Quality Assessment
The quality of eligible studies, which was assessed using the Newcastle–Ottawa Scale [54] by two independent reviewers (M.E.R., P.R.), included selection, comparability, and outcome. The number of scored points ranged from 0 to 9 (≥7, high quality; 4–6, medium quality, <4, low quality).
2.5. Statistical Analysis
The data were analyzed using the OpenMeta [Analyst] software for prevalence and the Cochrane Collaboration software Review Manager 5.4.1 (The Cochrane Collaboration, 2014; The Nordic Cochrane Centre, Copenhagen, Denmark) for risk ratios. Pooled risk ratios (RRs) and 95% confidence intervals (CIs) were used to analyze the risk of asthma susceptibility in patients with psoriasis and vice versa. A statistical test was performed based on the Cochrane Q-test and the I2 index to assess the heterogeneity among the eligible studies. Studies with an I2 statistic > 50% were considered to have significant heterogeneity. A random effects model was selected to pool the data. Pooled analyses were considered statistically significant when the p-value < 0.05. Sensitivity analysis was performed by sequentially omitting an individual study to evaluate each study’s influence on the global effect. Potential publication bias was assessed through visual inspection of funnel plots created in Revman 5.4.1.
3. Results
3.1. Characteristics of Identified Studies
As illustrated in Figure 2, the titles and abstracts of 986 articles were screened for eligibility, of which 18 met the eligibility criteria for full-text review. After further screening, 14 studies met the inclusion criteria for the systematic review.
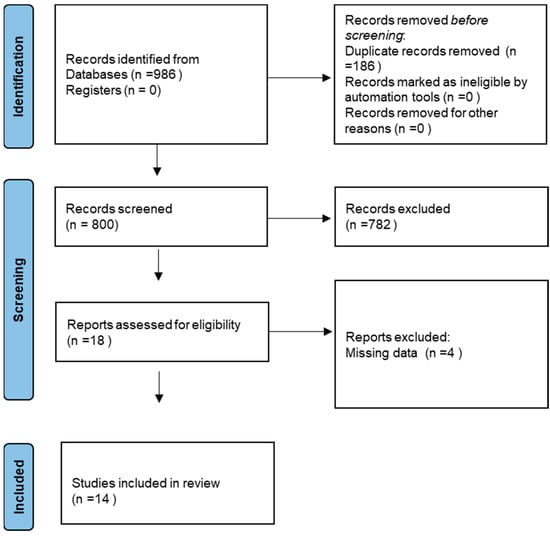
Figure 2.
Flow diagram of the included studies.
Characteristics of the 14 studies included in the meta-analysis appear in Table 1 for psoriasis patients vs. control group and Table 2 for asthma patients vs. control group.

Table 1.
Characteristics of the eleven studies on the prevalence of asthma in psoriatic patients vs. control.
Table 2.
Characteristics of the three studies on the prevalence of psoriasis in asthma patients vs. control.
3.2. Asthma in Psoriasis Patients
A total of 11 studies [9,10,23,24,25,26,27,28,29,30,55] comprising 110,978 patients with psoriasis and 1,898,071 controls were included in the meta-analysis. Figure 3 presents the forest plot of the pooled prevalence of asthma in patients with psoriasis: 9.2% (95% CI [0.075, 0.110]; I2 = 99.6%; p < 0.001). The prevalence of individual studies ranged from 1.7% [9,10] to 26% [30].
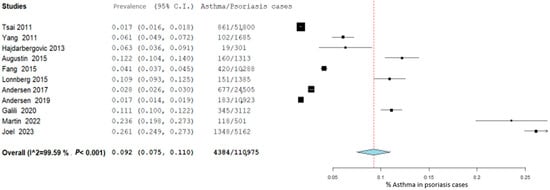
Figure 3.
Pooled prevalence of asthma in patients with psoriasis. Square boxes represent individual studies; horizontal lines represent 95% confidence intervals (CIs); and diamond-shaped figures represent 95% CIs of pooled estimate.
Figure 4 illustrates the forest plot of the risk of asthma in patients with psoriasis. The pooled risk ratio was 1.43 (95% CI [1.23, 1.66]; I2 = 95%; p < 0.001). The RR of individual studies ranged from 0.6 [24] to 2.02 [30].
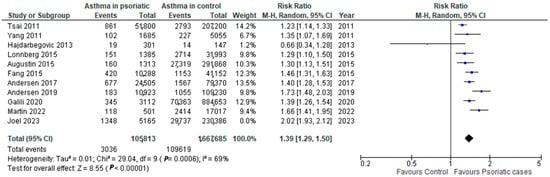
Figure 4.
Pooled risk of asthma in patients with psoriasis. Square boxes represent individual studies; horizontal lines represent 95% confidence intervals (CIs); and diamond-shaped figures represent 95% CIs of pooled estimate.
Sensitivity analysis based on (a) study design did not show this as a source of heterogeneity (cross-sectional studies: I2 = 95%, p < 0.0005; cohort studies: I2 = 83%, p < 0.00001) (Figure 5), and (b) region of the study showed that a small part of the heterogeneity comes from studies conducted in America (Europe: I2 = 65%, p < 0.00001; Asia: I2 = 67%, p < 005; America: I2 = 81%, p < 00001) (Figure 6).
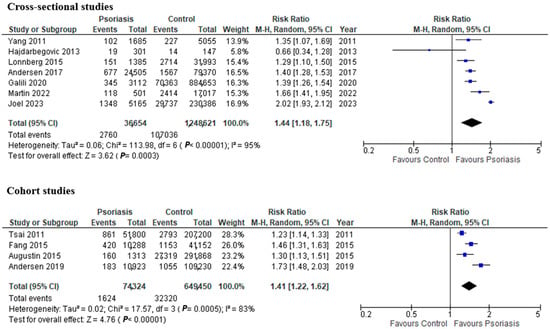
Figure 5.
Pooled risk of asthma in patients with psoriasis by study design. Square boxes represent individual studies; horizontal lines represent 95% confidence; and diamond-shaped figures are 95% CIs of pooled estimate.
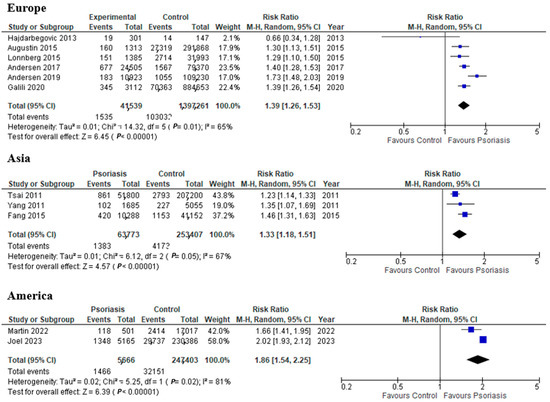
Figure 6.
Pooled risk of asthma in psoriatic patients by region. Square boxes represent individual studies; horizontal lines represent 95% confidence intervals (CIs); and diamond-shaped figures represent 95% CIs of pooled estimate.
Subgroup analysis of studies, based on the severity of psoriasis cases, shows a significantly higher risk of asthma in patients with moderate to severe psoriasis compared to their controls than in mild psoriasis (mild psoriasis: RR 1.28 [95% CI 1.14, 1.44], p = 0.04; moderate/severe psoriasis: RR 1.48 [95% CI 1.17, 1.88], p = 0.01) (Figure 7).
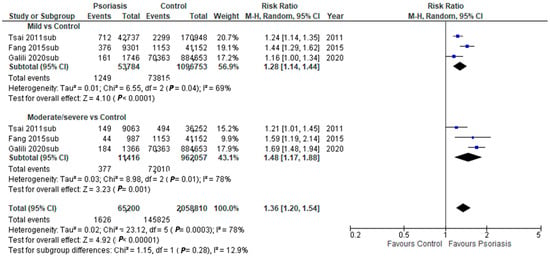
Figure 7.
Pooled risk of asthma in psoriatic patients by disease severity. Square boxes represent individual studies; horizontal lines represent 95% confidence intervals (CIs); and diamond-shaped figures represent 95% CIs of pooled estimate.
Sub-analysis by age was conducted in two ways: (a) studies with age range ≥ 18 years vs. ≤18 years of age (Figure 8) (≥18 years:1.55 [95% CI 1.31, 1.83], p < 0.00001; ≤18 years: 1.36 [95% CI 1.26, 1.48], p = 0.00001); and b) as a subgroup of studies with data by age (Figure 9) (≥50 years: 1.59 [95% CI 1.41, 1.79], p < 00001; 20–49 years: 1.23 [95% CI 1.07, 1.41], p = 0.004 showing a significantly higher risk of asthma in the older populations.
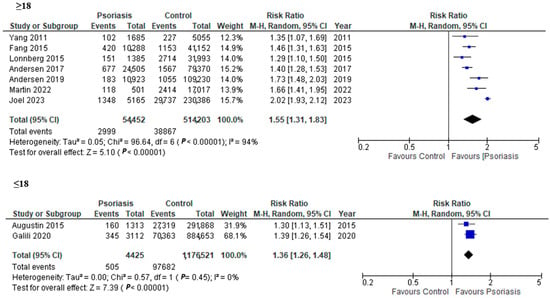
Figure 8.
Pooled risk of asthma in patients with psoriasis by age group. Square boxes represent individual studies; horizontal lines represent 95% confidence intervals (CIs); and diamond-shaped figures 95% CIs of pooled estimate.
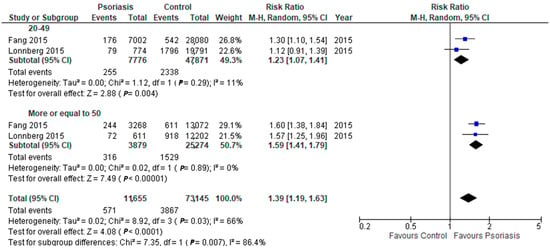
Figure 9.
Pooled risk of asthma in patients with psoriasis by age group. Square boxes represent individual studies; horizontal lines represent 95% confidence intervals (CIs); and diamond-shaped figures represent 95% CIs of pooled estimate.
3.3. Psoriasis in Asthma Patients
A total of 3 studies [31,32,33] comprising 468,869 asthma patients and 11,063,349 control were included in the meta-analysis. Figure 10 presents the forest plot of the pooled prevalence of psoriasis in asthma patients at 1.3% (95% CI [−0.004, 0.029]; I2 = 99.96%; p < 0.001). The prevalence of individual studies ranged from 0.4% [31] to 3.0% [33]. Figure 11 illustrates the forest plot of the risk of psoriasis in asthma patients. The pooled risk ratio was 1.23 (95% CI [1.02, 1.47]; I2 = 100%; p < 0.00001). The RR of individual studies ranged from 0.9 [31] to 1.42 [33] (Figure 5).

Figure 10.
Pooled prevalence of psoriasis in asthma patients. Square boxes represent individual studies; horizontal lines represent 95% confidence intervals (CIs); and diamond-shaped figures represent 95% CIs of the pooled estimate.

Figure 11.
Pooled risk of psoriasis in asthma patients. Square boxes represent individual studies; horizontal lines represent 95% confidence intervals (CIs); and diamond-shaped figures represent 95% CIs of pooled estimate.
A subgroup analysis of studies where hazard ratios were provided is presented in Figure 12. The pooled hazard ratio was 1.30 (95% CI [1.27, 1.33]; I2 = 0%; p < 0.00001). The RR of individual studies ranged from 0.9 [31] to 1.42 [33]. Other subgroup analyses were not possible with the data presented by these studies.

Figure 12.
Hazard ratios of psoriasis in asthma patients. Square boxes represent individual studies; horizontal lines represent 95% confidence intervals (CIs); and diamond-shaped figures represent 95% CIs of pooled estimate.
3.4. Quality Assessment and Publication Bias
The risk of bias based on individual studies using the Newcastle–Ottawa Scale is shown in Table 3. A total of 8 of the studies were high quality (≥7), and 6 were moderate quality (4–6).
Table 3.
Risk of bias and quality assessment of studies according to the Newcastle–Ottawa Scale.
Visual inspection of the funnel plots for each set of comparisons is shown in Figure 13. No significant asymmetry, or therefore, publication bias, for the studies was observed.
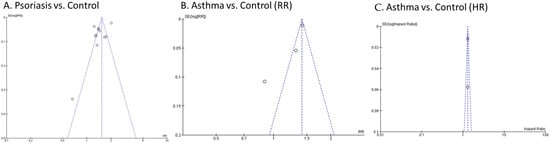
Figure 13.
Funnel plot for publication bias on selected studies. (A) Psoriasis vs. control, (B) Asthma vs. control. (C) Asthma vs. control hazard ratios.
4. Discussion
This systematic review and meta-analysis provides clear evidence that patients with psoriasis have an increased risk of asthma and vice versa. In patients with psoriasis, older age played a significant role in the association with asthma, as previously reported in a study by Wang et al. [13]. Furthermore, there is a higher risk of developing asthma in patients with moderate to severe psoriasis with respect to their controls than in patients with mild psoriasis.
One of the main issues with all the studies that assessed the association between psoriasis and asthma is the lack of consistent data on the status of some common risk factors for sub-analysis. The lack of adjustments for common risk factors may affect the outcome of this meta-analysis. Among the most important risk factors for these two chronic conditions are the following [56]: (A) Smoking status. Smoking has been associated with psoriasis [57] and asthma [58] and might be a factor influencing the association between asthma and psoriasis. (B) Obesity and low physical activity. Obesity has been associated with both severity of psoriasis [59,60] and is one of the main risk factors for the development of asthma [61]. (C) Infections. Infections can play a role in both asthma [62] and psoriasis [63]. One example is HIV; the prevalence of asthma in people living with HIV is higher than in those without HIV [64]. In HIV-infected patients, psoriasis may have a higher incidence, present atypical clinical features, and is often resistant to treatment [65]. (D) Allergies. Significantly higher concentration of total E immunoglobulin has been observed in the patients with psoriasis [66]. Similarly, continuous allergen exposure can increase the risk of asthma and other allergic diseases [67]. (E) Dysbiosis. Changes in the intestinal microbiota can influence the incidence of chronic inflammatory diseases. Microbiome dysbiosis, characterized by altered diversity and composition, has been identified as a possible trigger for recurrent episodes of psoriasis [68] and also asthma [69]. (F) Metabolic syndrome. Higher prevalence of hyperlipidemia, hypertension, and diabetes has been shown in psoriasis [70,71,72] and also in asthma [73]. (G) Medications. Some medications seem to trigger both psoriasis and asthma, such as ACE inhibitors, beta-blockers, and NSAIDs [74,75,76,77,78]. (H) Subtyping of both psoriasis and asthma types to determine shared chronic inflammatory pathways or molecules [56,79]; for example, psoriasis is mediated by Th1, Th17, Th22, and Th9 [12], and similarly, neutrophilic inflammation in severe or corticoid-resistant asthma is mediated by Th1 and Th17 cells [80]. Additionally, Th17 cells produce IL-17A, IL-17F, and IL-22, inflammatory cytokines that induce the keratinocyte activation and proliferation seen in psoriasis [81,82], and the increased activity of these cytokines is also observed in patients with asthma [83], but not all subtypes share these molecules. (I) Genetic links. Single-nucleotide polymorphism (SNP) based genome-wide association studies (GWASs) have identified common variants determining susceptibility to both psoriasis and asthma [84,85,86]. Other common risk factors may also be at play.
The hypothesis that the immune components, particularly the IL-23/Th17 axis for the association between asthma and psoriasis, is critical to understanding their relationship is substantiated by the high efficacy of psoriasis biologic treatments targeting the IL-23/Th17 axis, and TNF-α signaling [41,87,88,89]. However, the initial clinical trials targeting IL-23 and IL-17 in asthma yielded unfavorable results [90,91], but a high percentage of participants in the IL-23 trial [90] were categorized as having allergic asthma (61.9%), which will be less likely to benefit from this targeted treatment [36]. Studies that include more selected patients, particularly those with treatment-resistant diseases, are needed.
There are a few limitations in this meta-analysis. Firstly, there is high heterogeneity among the studies. Sensitivity analysis eliminating one study at a time indicates that the study by Joel et al. [30] introduces most of the heterogeneity (data not shown) but does not explain it completely. In general, the American-region studies introduce a significant part of the heterogeneity, indicating a higher risk of the development of asthma in patients with psoriasis. Secondly, there is a lack of information on the phenotype of asthma reported. Finally, there is a potential for overlapping among studies by region, and this cannot be excluded.
5. Conclusions
This review provides clear evidence for the bidirectional association between asthma and psoriasis. However, this association seems to be affected by age, the severity of psoriasis, study region, ethnicities of patients, and potentially other characteristics not included in this meta-analysis. Having pooled estimates of the prevalence and risk of asthma in psoriasis and vice versa, and understanding their underlying mechanisms, can help develop appropriate preventative and therapeutic strategies in these patients.
Author Contributions
M.E.R.-N., conceptualization, methodology, investigation, formal analysis, writing, project administrator. A.G., conceptualization, investigation, editing. P.V.A.K.R., data curation, review, and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data is provided in the review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Korman, N.J. Management of Psoriasis as a Systemic Disease: What Is the Evidence? Br. J. Dermatol. 2020, 182, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Rachakonda, T.D.; Schupp, C.W.; Armstrong, A.W. Psoriasis Prevalence among Adults in the United States. J. Am. Acad. Dermatol. 2014, 70, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.S.; Singh, R.; Cloutier, M.; Gauthier-Loiselle, M.; Emond, B.; Guérin, A.; Ganguli, A. Prevalence of Psoriasis in Children and Adolescents in the United States: A Claims-Based Analysis. J. Drugs Dermatol. 2018, 17, 187–194. [Google Scholar]
- World Health Organization. Global Report on Psoriasis; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-156518-9. [Google Scholar]
- Henseler, T.; Christophers, E. Psoriasis of Early and Late Onset: Characterization of Two Types of Psoriasis Vulgaris. J. Am. Acad. Dermatol. 1985, 13, 450–456. [Google Scholar] [CrossRef]
- Schön, M.P.; Boehncke, W.-H. Psoriasis. N. Engl. J. Med. 2005, 352, 1899–1912. [Google Scholar] [CrossRef]
- Oliveira, M.; de, F.S.P.d.; Rocha, B.d.O.; Duarte, G.V. Psoriasis: Classical and Emerging Comorbidities. An. Bras. Dermatol. 2015, 90, 9–20. [Google Scholar] [CrossRef]
- Bu, J.; Ding, R.; Zhou, L.; Chen, X.; Shen, E. Epidemiology of Psoriasis and Comorbid Diseases: A Narrative Review. Front. Immunol. 2022, 13, 880201. [Google Scholar] [CrossRef]
- Tsai, T.-F.; Wang, T.-S.; Hung, S.-T.; Tsai, P.I.-C.; Schenkel, B.; Zhang, M.; Tang, C.-H. Epidemiology and Comorbidities of Psoriasis Patients in a National Database in Taiwan. J. Dermatol. Sci. 2011, 63, 40–46. [Google Scholar] [CrossRef]
- Andersen, Y.M.F.; Wu, J.J.; Thyssen, J.P.; Egeberg, A. Chronologic Order of Appearance of Immune-Mediated Inflammatory Diseases Relative to Diagnosis of Psoriasis. J. Am. Acad. Dermatol. 2019, 81, 1283–1291. [Google Scholar] [CrossRef]
- Elloso, M.M.; Gomez-Angelats, M.; Fourie, A.M. Targeting the Th17 Pathway in Psoriasis. J. Leukoc. Biol. 2012, 92, 1187–1197. [Google Scholar] [CrossRef]
- Diani, M.; Altomare, G.; Reali, E. T Helper Cell Subsets in Clinical Manifestations of Psoriasis. J. Immunol. Res. 2016, 2016, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ke, R.; Shi, W.; Yan, X.; Wang, Q.; Zhang, Q.; Chai, L.; Li, M. Association between Psoriasis and Asthma Risk: A Meta-Analysis. Allergy Asthma Proc. 2018, 39, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Fahy, J.V. Type 2 Inflammation in Asthma—Present in Most, Absent in Many. Nat. Rev. Immunol. 2015, 15, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Habib, N.; Pasha, M.A.; Tang, D.D. Current Understanding of Asthma Pathogenesis and Biomarkers. Cells 2022, 11, 2764. [Google Scholar] [CrossRef] [PubMed]
- Israel, E.; Reddel, H.K. Severe and Difficult-to-Treat Asthma in Adults. N. Engl. J. Med. 2017, 377, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Gurczynski, S.J.; Moore, B.B. IL-17 in the Lung: The Good, the Bad, and the Ugly. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2018, 314, L6–L16. [Google Scholar] [CrossRef]
- Roos, A.B.; Sethi, S.; Nikota, J.; Wrona, C.T.; Dorrington, M.G.; Sandén, C.; Bauer, C.M.T.; Shen, P.; Bowdish, D.; Stevenson, C.S.; et al. IL-17A and the Promotion of Neutrophilia in Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2015, 192, 428–437. [Google Scholar] [CrossRef]
- Alnahas, S.; Hagner, S.; Raifer, H.; Kilic, A.; Gasteiger, G.; Mutters, R.; Hellhund, A.; Prinz, I.; Pinkenburg, O.; Visekruna, A.; et al. IL-17 and TNF-α Are Key Mediators of Moraxella Catarrhalis Triggered Exacerbation of Allergic Airway Inflammation. Front. Immunol. 2017, 8, 1562. [Google Scholar] [CrossRef]
- Ricciardolo, F.L.M.; Sorbello, V.; Folino, A.; Gallo, F.; Massaglia, G.M.; Favatà, G.; Conticello, S.; Vallese, D.; Gani, F.; Malerba, M.; et al. Identification of IL-17F/Frequent Exacerbator Endotype in Asthma. J. Allergy Clin. Immunol. 2017, 140, 395–406. [Google Scholar] [CrossRef]
- Östling, J.; van Geest, M.; Schofield, J.P.R.; Jevnikar, Z.; Wilson, S.; Ward, J.; Lutter, R.; Shaw, D.E.; Bakke, P.S.; Caruso, M.; et al. IL-17–High Asthma with Features of a Psoriasis Immunophenotype. J. Allergy Clin. Immunol. 2019, 144, 1198–1213. [Google Scholar] [CrossRef]
- Choy, D.F.; Hart, K.M.; Borthwick, L.A.; Shikotra, A.; Nagarkar, D.R.; Siddiqui, S.; Jia, G.; Ohri, C.M.; Doran, E.; Vannella, K.M.; et al. T H2 and Th17 Inflammatory Pathways Are Reciprocally Regulated in Asthma. Sci. Transl. Med. 2015, 7. [Google Scholar] [CrossRef]
- Yang, Y.-W.; Keller, J.J.; Lin, H.-C. Medical Comorbidity Associated with Psoriasis in Adults: A Population-Based Study. Br. J. Dermatol. 2011, 165, 1037–1043. [Google Scholar] [CrossRef]
- Hajdarbegovic, E.; Nijsten, T.; Westgeest, A.; Habraken, F.; Hollestein, L.; Thio, B. Decreased Prevalence of Atopic Features in Patients with Psoriatic Arthritis, but Not in Psoriasis Vulgaris. J. Am. Acad. Dermatol. 2013, 68, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Radtke, M.A.; Glaeske, G.; Reich, K.; Christophers, E.; Schaefer, I.; Jacobi, A. Epidemiology and Comorbidity in Children with Psoriasis and Atopic Eczema. Dermatology 2015, 231, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.-Y.; Liao, W.-C.; Lin, C.-L.; Chen, C.-H.; Kao, C.-H. Association between Psoriasis and Asthma: A Population-Based Retrospective Cohort Analysis. Br. J. Dermatol. 2015, 172, 1066–1071. [Google Scholar] [CrossRef]
- Lønnberg, A.S.; Skov, L.; Skytthe, A.; Kyvik, K.O.; Pedersen, O.B.; Meteran, H.; Backer, V.; Thomsen, S.F. Asthma in Patients with Psoriasis. Br. J. Dermatol. 2015, 172, 1660–1661. [Google Scholar] [CrossRef] [PubMed]
- Andersen, Y.M.F.; Egeberg, A.; Gislason, G.H.; Skov, L.; Thyssen, J.P. Burden of Respiratory Comorbidities in Patients with Atopic Dermatitis and Psoriasis. Br. J. Dermatol. 2017, 177, e145–e146. [Google Scholar] [CrossRef] [PubMed]
- Galili, E.; Barzilai, A.; Twig, G.; Caspi, T.; Daniely, D.; Shreberk-Hassidim, R.; Astman, N. Allergic Rhinitis and Asthma Among Adolescents with Psoriasis: A Population-Based Cross-Sectional Study. Acta Derm. Venereol. 2020, 100. [Google Scholar] [CrossRef] [PubMed]
- Joel, M.Z.; Fan, R.; Damsky, W.; Cohen, J.M. Psoriasis Associated with Asthma and Allergic Rhinitis: A US-Based Cross-Sectional Study Using the All of US Research Program. Arch. Derm. Res. 2023. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Egeberg, A.; Khalid, U.; Gislason, G.H.; Mallbris, L.; Skov, L.; Hansen, P.R. Risk of Psoriasis in Patients with Childhood Asthma: A Danish Nationwide Cohort Study. Br. J. Dermatol. 2015, 173, 159–164. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Increased Risk of Psoriasis in Children and Elderly Patients with Asthma: A Longitudinal Follow-up Study Using a National Sample Cohort. Int. Forum Allergy Rhinol. 2019, 9, 1304–1310. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Bang, C.H.; Han, K.; Ryu, J.Y.; Lee, J.Y.; Park, Y.M.; Lee, J.H. The Risk of Psoriasis in Patients with Allergic Diseases: A Nationwide Population-Based Cohort Study. Allergy Asthma Immunol. Res. 2021, 13, 638. [Google Scholar] [CrossRef] [PubMed]
- Busse, W.W. Asthma and Psoriasis: What Do They Have in Common? IL-17A! J. Allergy Clin. Immunol. 2019, 144, 1169–1171. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, H.; Hirose, K. Role of IL-23 and Th17 Cells in Airway Inflammation in Asthma. Immune Netw. 2010, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.Y.; Peebles, R.S. The Emerging Role of IL-23 in Asthma and Its Clinical Implications. Expert. Rev. Clin. Immunol. 2023, 19, 1–5. [Google Scholar] [CrossRef]
- Taherian, M.; Razavi, A.R.; Izad, M.; Boghozian, R.; Namdari, H.; Ghayedi, M.; Rahimzadeh, P.; Bidad, K.; Salehi, E. The Role of Interleukin-23 in Stability of in Vitro T Helper-17 Cells. Iran. J. Allergy Asthma Immunol. 2014, 13, 131–137. [Google Scholar]
- Al-Ramli, W.; Préfontaine, D.; Chouiali, F.; Martin, J.G.; Olivenstein, R.; Lemière, C.; Hamid, Q. TH17-Associated Cytokines (IL-17A and IL-17F) in Severe Asthma. J. Allergy Clin. Immunol. 2009, 123, 1185–1187. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Wills-Karp, M. The Potential Role of Interleukin-17 in Severe Asthma. Curr. Allergy Asthma Rep. 2011, 11, 388–394. [Google Scholar] [CrossRef]
- Peng, J.; Yang, X.O.; Chang, S.H.; Yang, J.; Dong, C. IL-23 Signaling Enhances Th2 Polarization and Regulates Allergic Airway Inflammation. Cell. Res. 2010, 20, 62–71. [Google Scholar] [CrossRef]
- Frieder, J.; Kivelevitch, D.; Haugh, I.; Watson, I.; Menter, A. Anti-IL-23 and Anti-IL-17 Biologic Agents for the Treatment of Immune-Mediated Inflammatory Conditions. Clin. Pharmacol. Ther. 2018, 103, 88–101. [Google Scholar] [CrossRef]
- Langley, R.G.; Lebwohl, M.; Krueger, G.G.; Szapary, P.O.; Wasfi, Y.; Chan, D.; Hsu, M.C.; You, Y.; Poulin, Y.; Korman, N.; et al. Long-term Efficacy and Safety of Ustekinumab, with and without Dosing Adjustment, in Patients with Moderate-to-severe Psoriasis: Results from the PHOENIX 2 Study through 5 Years of Follow-up. Br. J. Dermatol. 2015, 172, 1371–1383. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, A.; Kato, T.; Kato, M.; Song, M.; Nakagawa, H.; The Japanese Ustekinumab Study Group. Efficacy and Safety of Ustekinumab in Japanese Patients with Moderate-to-Severe Plaque-Type Psoriasis: Long-Term Results from a Phase 2/3 Clinical Trial: Ustekinumab in Japanese Psoriasis Patients. J. Dermatol. 2012, 39, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.-F.; Ho, J.-C.; Song, M.; Szapary, P.; Guzzo, C.; Shen, Y.-K.; Li, S.; Kim, K.-J.; Kim, T.-Y.; Choi, J.-H.; et al. Efficacy and Safety of Ustekinumab for the Treatment of Moderate-to-Severe Psoriasis: A Phase III, Randomized, Placebo-Controlled Trial in Taiwanese and Korean Patients (PEARL). J. Dermatol. Sci. 2011, 63, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Zheng, M.; Song, M.; Shen, Y.-K.; Chan, D.; Szapary, P.O.; Wang, B. LOTUS Investigators Efficacy and Safety of Ustekinumab in Chinese Patients with Moderate to Severe Plaque-Type Psoriasis: Results from a Phase 3 Clinical Trial (LOTUS). J. Drugs Dermatol. 2013, 12, 166–174. [Google Scholar] [PubMed]
- Albanesi, C.; Madonna, S.; Gisondi, P.; Girolomoni, G. The Interplay Between Keratinocytes and Immune Cells in the Pathogenesis of Psoriasis. Front. Immunol. 2018, 9, 1549. [Google Scholar] [CrossRef]
- Zaba, L.C.; Suárez-Fariñas, M.; Fuentes-Duculan, J.; Nograles, K.E.; Guttman-Yassky, E.; Cardinale, I.; Lowes, M.A.; Krueger, J.G. Effective Treatment of Psoriasis with Etanercept Is Linked to Suppression of IL-17 Signaling, Not Immediate Response TNF Genes. J. Allergy Clin. Immunol. 2009, 124, 1022–1030.e395. [Google Scholar] [CrossRef]
- Zaba, L.C.; Fuentes-Duculan, J.; Eungdamrong, N.J.; Johnson-Huang, L.M.; Nograles, K.E.; White, T.R.; Pierson, K.C.; Lentini, T.; Suárez-Fariñas, M.; Lowes, M.A.; et al. Identification of TNF-Related Apoptosis-Inducing Ligand and Other Molecules That Distinguish Inflammatory from Resident Dendritic Cells in Patients with Psoriasis. J. Allergy Clin. Immunol. 2010, 125, 1261–1268.e9. [Google Scholar] [CrossRef]
- Fuentes-Duculan, J.; Suárez-Fariñas, M.; Zaba, L.C.; Nograles, K.E.; Pierson, K.C.; Mitsui, H.; Pensabene, C.A.; Kzhyshkowska, J.; Krueger, J.G.; Lowes, M.A. A Subpopulation of CD163-Positive Macrophages Is Classically Activated in Psoriasis. J. Investig. Dermatol. 2010, 130, 2412–2422. [Google Scholar] [CrossRef]
- Lee, H.S.; Park, D.-E.; Lee, J.-W.; Chang, Y.; Kim, H.Y.; Song, W.-J.; Kang, H.-R.; Park, H.-W.; Chang, Y.-S.; Cho, S.-H. IL-23 Secreted by Bronchial Epithelial Cells Contributes to Allergic Sensitization in Asthma Model: Role of IL-23 Secreted by Bronchial Epithelial Cells. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2017, 312, L13–L21. [Google Scholar] [CrossRef]
- Li, H.; Yao, Q.; Mariscal, A.G.; Wu, X.; Hülse, J.; Pedersen, E.; Helin, K.; Waisman, A.; Vinkel, C.; Thomsen, S.F.; et al. Epigenetic Control of IL-23 Expression in Keratinocytes Is Important for Chronic Skin Inflammation. Nat. Commun. 2018, 9, 1420. [Google Scholar] [CrossRef]
- Halwani, R.; Sultana, A.; Vazquez-Tello, A.; Jamhawi, A.; Al-Masri, A.A.; Al-Muhsen, S. Th-17 Regulatory Cytokines IL-21, IL-23, and IL-6 Enhance Neutrophil Production of IL-17 Cytokines during Asthma. J. Asthma 2017, 54, 893–904. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberatî, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Thatiparthi, A.; Liu, J.; Ge, S.; Egeberg, A.; Wu, J.J. Association between Psoriasis and Asthma among United States Adults in the 2009-2014 National Health and Nutrition Examination Survey. J. Am. Acad. Dermatol. 2022, 86, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Mleczko, M.; Gerkowicz, A.; Krasowska, D. Chronic Inflammation as the Underlying Mechanism of the Development of Lung Diseases in Psoriasis: A Systematic Review. IJMS 2022, 23, 1767. [Google Scholar] [CrossRef] [PubMed]
- Richer, V.; Roubille, C.; Fleming, P.; Starnino, T.; McCourt, C.; McFarlane, A.; Siu, S.; Kraft, J.; Lynde, C.; Pope, J.E.; et al. Psoriasis and Smoking: A Systematic Literature Review and Meta-Analysis with Qualitative Analysis of Effect of Smoking on Psoriasis Severity. J. Cutan. Med. Surg. 2016, 20, 221–227. [Google Scholar] [CrossRef]
- Cerveri, I.; Cazzoletti, L.; Corsico, A.G.; Marcon, A.; Niniano, R.; Grosso, A.; Ronzoni, V.; Accordini, S.; Janson, C.; Pin, I.; et al. The Impact of Cigarette Smoking on Asthma: A Population-Based International Cohort Study. Int. Arch. Allergy Immunol. 2012, 158, 175–183. [Google Scholar] [CrossRef]
- Fleming, P.; Kraft, J.; Gulliver, W.P.; Lynde, C. The Relationship of Obesity with the Severity of Psoriasis: A Systematic Review. J. Cutan. Med. Surg. 2015, 19, 450–456. [Google Scholar] [CrossRef]
- Jacobi, A.; Langenbruch, A.; Purwins, S.; Augustin, M.; Radtke, M.A. Prevalence of Obesity in Patients with Psoriasis: Results of the National Study PsoHealth3. Dermatology 2015, 231, 231–238. [Google Scholar] [CrossRef]
- Peters, S. The Impact of Comorbid Atopic Disease on Asthma: Clinical Expression and Treatment. J. Asthma 2007, 44, 149–161. [Google Scholar] [CrossRef]
- Huang, Y.J. The Respiratory Microbiome and Innate Immunity in Asthma. Curr. Opin. Pulm. Med. 2015, 21, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Rademaker, M.; Agnew, K.; Anagnostou, N.; Andrews, M.; Armour, K.; Baker, C.; Foley, P.; Gebauer, K.; Gupta, M.; Marshman, G.; et al. Psoriasis and Infection. A Clinical Practice Narrative. Australas. J. Derm. 2019, 60, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Kirenga, B.J.; Mugenyi, L.; De Jong, C.; Lucian Davis, J.; Katagira, W.; Van Der Molen, T.; Kamya, M.R.; Boezen, M. The Impact of HIV on the Prevalence of Asthma in Uganda: A General Population Survey. Respir. Res. 2018, 19, 184. [Google Scholar] [CrossRef]
- Alpalhão, M.; Borges-Costa, J.; Filipe, P. Psoriasis in HIV Infection: An Update. Int. J. STD AIDS 2019, 30, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Weryńska-Kalemba, M.; Filipowska-Grońska, A.; Kalemba, M.; Krajewska, A.; Grzanka, A.; Bożek, A.; Jarząb, J. Analysis of Selected Allergic Reactions among Psoriatic Patients. PDIA 2016, 1, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Baxi, S.N.; Phipatanakul, W. The Role of Allergen Exposure and Avoidance in Asthma. Adolesc. Med. State Art. Rev. 2010, 21, 57–71. [Google Scholar] [PubMed]
- Kapoor, B.; Gulati, M.; Rani, P.; Gupta, R. Psoriasis: Interplay between Dysbiosis and Host Immune System. Autoimmun. Rev. 2022, 21, 103169. [Google Scholar] [CrossRef] [PubMed]
- Hufnagl, K.; Pali-Schöll, I.; Roth-Walter, F.; Jensen-Jarolim, E. Dysbiosis of the Gut and Lung Microbiome Has a Role in Asthma. Semin. Immunopathol. 2020, 42, 75–93. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. The Association between Psoriasis and Hypertension: A Systematic Review and Meta-Analysis of Observational Studies. J. Hypertens. 2013, 31, 433–443. [Google Scholar] [CrossRef]
- Coto-Segura, P.; Eiris-Salvado, N.; González-Lara, L.; Queiro-Silva, R.; Martinez-Camblor, P.; Maldonado-Seral, C.; García-García, B.; Palacios-García, L.; Gomez-Bernal, S.; Santos-Juanes, J.; et al. Psoriasis, Psoriatic Arthritis and Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Br. J. Dermatol. 2013, 169, 783–793. [Google Scholar] [CrossRef]
- Salihbegovic, E.; Hadzigrahic, N.; Suljagic, E.; Kurtalic, N.; Hadzic, J.; Zejcirovic, A.; Bijedic, M.; Handanagic, A. Psoriasis and Dyslipidemia. Mater. Sociomed. 2015, 27, 15. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, S.F.; Quesenberry, C.P.; Van Den Eeden, S.K.; Shan, J.; Ferrara, A. Patients Diagnosed with Diabetes Are at Increased Risk for Asthma, Chronic Obstructive Pulmonary Disease, Pulmonary Fibrosis, and Pneumonia but Not Lung Cancer. Diabetes Care 2010, 33(1), 55–60. [Google Scholar] [CrossRef] [PubMed]
- Song, W.-J.; Niimi, A. Angiotensin-Converting Enzyme Inhibitors, Asthma, and Cough: Relighting the Torch. J. Allergy Clin. Immunol. Pract. 2021, 9, 3440–3441. [Google Scholar] [CrossRef] [PubMed]
- Balak, D.; Hajdarbegovic, E. Drug-Induced Psoriasis: Clinical Perspectives. PTT 2017, 7, 87–94. [Google Scholar] [CrossRef]
- Rongioletti, F.; Fiorucci, C.; Parodi, A. Psoriasis Induced or Aggravated by Drugs. J. Rheumatol. Suppl. 2009, 83, 59–61. [Google Scholar] [CrossRef]
- Ohyama, K.; Arai, H.; Sugiura, M.; Hori, Y. Psoriasis Associated with ACE Inhibitors: An Analysis of the FAERS Database. Pharmazie 2020, 75, 524–526. [Google Scholar]
- Wu, S.; Han, J.; Qureshi, A. Use of Aspirin, Non-Steroidal Anti-Inflammatory Drugs, and Aceta minophen (Paracetamol), and Risk of Psoriasis and Psoriatic Arthritis: A Cohort Study. Acta Derm. Venerol. 2015, 95, 217–222. [Google Scholar] [CrossRef]
- Reich, K. The Concept of Psoriasis as a Systemic Inflammation: Implications for Disease Management: Systemic Disease and Therapy for Psoriasis. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 3–11. [Google Scholar] [CrossRef]
- Chang, H.S.; Lee, T.-H.; Jun, J.A.; Baek, A.R.; Park, J.-S.; Koo, S.-M.; Kim, Y.-K.; Lee, H.S.; Park, C.-S. Neutrophilic Inflammation in Asthma: Mechanisms and Therapeutic Considerations. Expert. Rev. Respir. Med. 2017, 11, 29–40. [Google Scholar] [CrossRef]
- Lowes, M.A.; Russell, C.B.; Martin, D.A.; Towne, J.E.; Krueger, J.G. The IL-23/T17 Pathogenic Axis in Psoriasis Is Amplified by Keratinocyte Responses. Trends Immunol. 2013, 34, 174–181. [Google Scholar] [CrossRef]
- Singh, T.P.; Schön, M.P.; Wallbrecht, K.; Gruber-Wackernagel, A.; Wang, X.-J.; Wolf, P. Involvement of IL-9 in Th17-Associated Inflammation and Angiogenesis of Psoriasis. PLoS ONE 2013, 8, e51752. [Google Scholar] [CrossRef] [PubMed]
- Bullens, D.M.; Truyen, E.; Coteur, L.; Dilissen, E.; Hellings, P.W.; Dupont, L.J.; Ceuppens, J.L. IL-17 MRNA in Sputum of Asthmatic Patients: Linking T Cell Driven Inflammation and Granulocytic Influx? Respir. Res. 2006, 7, 135. [Google Scholar] [CrossRef] [PubMed]
- Elder, J.T. Genome-Wide Association Scan Yields New Insights into the Immunopathogenesis of Psoriasis. Genes. Immun. 2009, 10, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Weidinger, S.; Willis-Owen, S.; Kamatani, Y.; Baurecht, H.; Morar, N.; Liang, L.; Edser, P.; Street, T.; Rodriguez, E.; O’Regan, G.M.; et al. A Genome-Wide Association Study of Atopic Dermatitis Identifies Loci with Overlapping Effects on Asthma and Psoriasis. Hum. Mol. Genet. 2013, 22, 4841–4856. [Google Scholar] [CrossRef] [PubMed]
- Kere, J. Mapping Genes for Asthma and Psoriasis. Novartis Found. Symp. 2008, 360, 46–56. [Google Scholar] [CrossRef]
- Rendon, A.; Schäkel, K. Psoriasis Pathogenesis and Treatment. IJMS 2019, 20, 1475. [Google Scholar] [CrossRef]
- Sofen, H.; Smith, S.; Matheson, R.T.; Leonardi, C.L.; Calderon, C.; Brodmerkel, C.; Li, K.; Campbell, K.; Stanley, J.M., Jr.; Wasfi, Y.; et al. Guselkumab (an IL-23-Specific MAb) Demonstrates Clinical and Molecular Response in Patients with Moderate-to-Severe Psoriasis. J. Allergy Clin. Immunol. 2014, 133, 1032–1040. [Google Scholar] [CrossRef]
- Liu, T.; Li, S.; Ying, S.; Tang, S.; Ding, Y.; Li, Y.; Qiao, J.; Fang, H. The IL-23/IL-17 Pathway in Inflammatory Skin Diseases: From Bench to Bedside. Front. Immunol. 2020, 11, 594735. [Google Scholar] [CrossRef]
- Brightling, C.E.; Nair, P.; Cousins, D.J.; Louis, R.; Singh, D. Risankizumab in Severe Asthma—A Phase 2a, Placebo-Controlled Trial. N. Engl. J. Med. 2021, 385, 1669–1679. [Google Scholar] [CrossRef]
- Busse, W.W.; Holgate, S.; Kerwin, E.; Chon, Y.; Feng, J.; Lin, J.; Lin, S.-L. Randomized, Double-Blind, Placebo-Controlled Study of Brodalumab, a Human Anti–IL-17 Receptor Monoclonal Antibody, in Moderate to Severe Asthma. Am. J. Respir. Crit. Care Med. 2013, 188, 1294–1302. [Google Scholar] [CrossRef]













Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).