
Quantification of Metronidazole in Tablets: Combining Thin-Layer Chromatography in the GPHF-Minilab™ with Image Processing Using Open-Source ImageJ Software

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. TLC Method
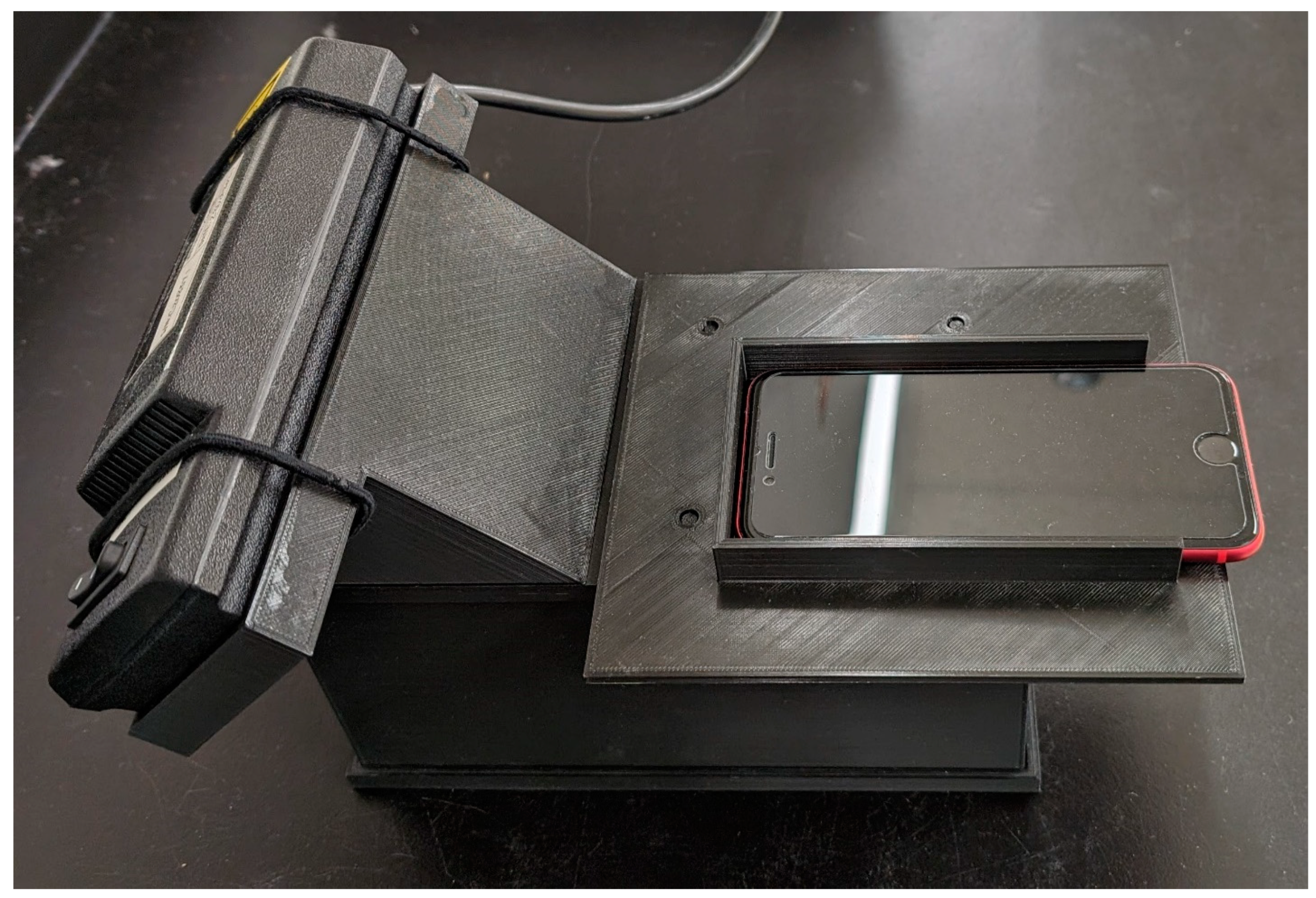
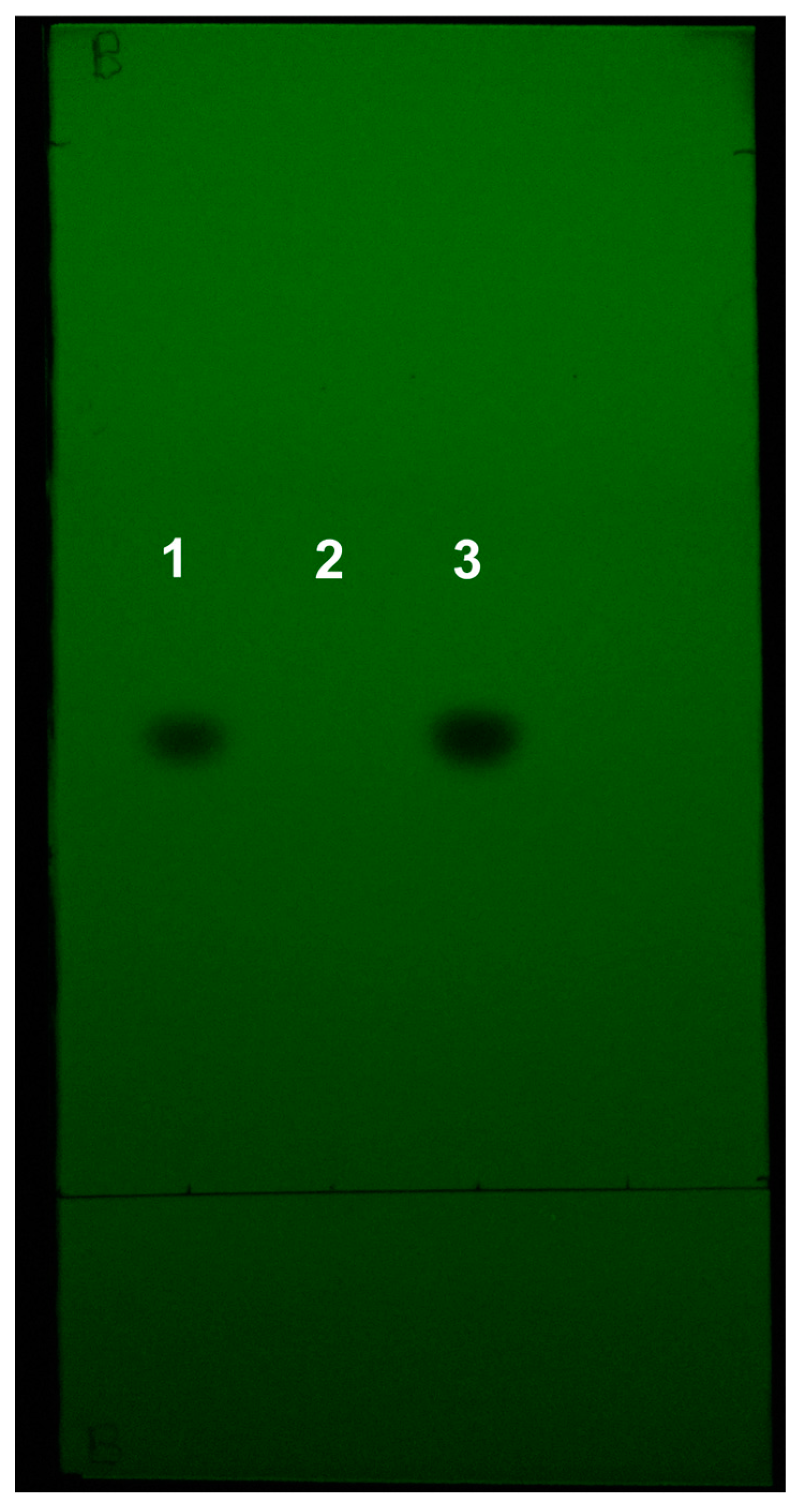
2.2. Image Acquisition and Analysis
2.3. HPLC Method
2.4. Validation
2.4.1. Linearity and Range
2.4.2. Accuracy and Precision
2.4.3. Repeatability and Intermediate Precision
2.4.4. Specificity
2.4.5. Robustness
3. Results
3.1. Linearity and Range
3.2. Accuracy and Precision
3.3. Repeatability and Intermediate Precision
3.4. Specificity
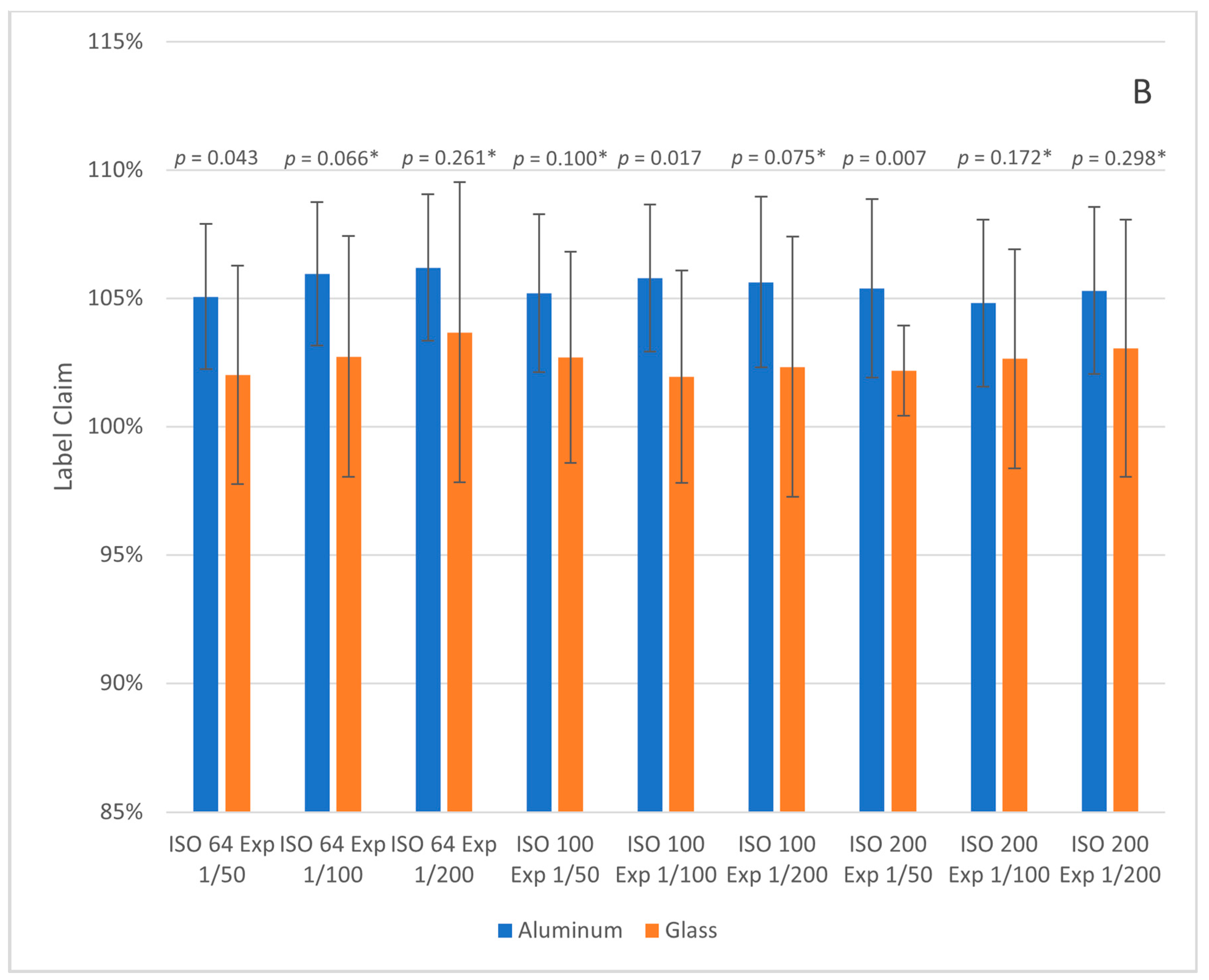
3.5. Robustness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Metronidazole. Available online: https://list.essentialmeds.org/medicines/313 (accessed on 4 June 2024).
- Tebano, G.; Li, G.; Beovic, B.; Bielicki, J.; Brink, A.; Enani, M.A.; Godman, B.; Hinrichsen, S.L.; Kibuule, D.; Gabriel, L.-H.; et al. Essential and Forgotten Antibiotics: An Inventory in Low- and Middle-Income Countries. Int. J. Antimicrob. Agents 2019, 54, 273–282. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). WHO Global Surveillance and Monitoring System for Substandard and Falsified Medical Products; World Health Organization: Geneva, Switzerland, 2017; ISBN 978-92-4-151342-5. [Google Scholar]
- Tchounga, C.A.W.; Sacré, P.-Y.; Hamuli, P.C.; Mballa, R.N.; Bleye, C.D.; Ziemons, E.; Hubert, P.; Djang’eing’a, R.M. Prevalence of Poor Quality Ciprofloxacin and Metronidazole Tablets in Three Cities in Cameroon. Am. J. Trop. Med. Hyg. 2023, 108, 403. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Metronidazole Tablets (Metronidazoli Compressi). In The International Pharmacopoeia, 11th ed.; World Health Organization: Geneva, Switzerland, 2022; Volume 6. [Google Scholar]
- United States Pharmacopoeia (USP). Metronidazole Tablets. In USP-NF; USP: Rockville, MD, USA, 2023. [Google Scholar] [CrossRef]
- Kaale, E.; Manyanga, V.; Makori, N.; Jenkins, D.; Michael Hope, S.; Layloff, T. High-performance thin layer chromatography to assess pharmaceutical product quality. Trop. Med. Int. Health 2014, 19, 747–751. [Google Scholar] [CrossRef]
- Pyka-Pająk, A. TLC–Densitometric Analysis of Selected 5-Nitroimidazoles. Processes 2023, 11, 170. [Google Scholar] [CrossRef]
- Meshram, D.; Bagade, S.; Tajne, M. TLC-Densitometric Analysis of Clotrimazole and Metronidazole in Combined Dosage Forms. J. Planar Chromatogr.–Mod. TLC 2008, 21, 277–282. [Google Scholar] [CrossRef]
- Meshram, D.B.; Bagade, S.B.; Tajne, M.R. Simultaneous Determination of Metronidazole and Miconazole Nitrate in Gel by HPTLC. Pak. J. Pharm. Sci. 2009, 22, 323–328. [Google Scholar]
- Elkady, E.F.; Mahrouse, M.A. Reversed-Phase Ion-Pair HPLC and TLC-Densitometric Methods for the Simultaneous Determination of Ciprofloxacin Hydrochloride and Metronidazole in Tablets. Chromatographia 2011, 73, 297–305. [Google Scholar] [CrossRef]
- Ali, N.W.; Gamal, M.; Abdelkawy, M. Chromatographic Methods for Simultaneous Determination of Diiodohydroxyquinoline and Metronidazole in Their Binary Mixture. Pak. J. Pharm. Sci. 2013, 26, 865–871. [Google Scholar] [PubMed]
- Johnson, M.E. Rapid, Simple Quantitation in Thin-Layer Chromatography Using a Flatbed Scanner. J. Chem. Educ. 2000, 77, 368. [Google Scholar] [CrossRef]
- Hess, A.V.I. Digitally Enhanced Thin-Layer Chromatography: An Inexpensive, New Technique for Qualitative and Quantitative Analysis. J. Chem. Educ. 2007, 84, 842. [Google Scholar] [CrossRef]
- Soponar, F.; Moţ, A.C.; Sârbu, C. Quantitative Determination of Some Food Dyes Using Digital Processing of Images Obtained by Thin-Layer Chromatography. J. Chromatogr. A 2008, 1188, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Gad, A.G.; Mohammed Fayez, Y.; Kelani, K.M.; Mahmoud, A.M. TLC-Smartphone in Antibiotics Determination and Low-Quality Pharmaceuticals Detection. RSC Adv. 2021, 11, 19196–19202. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.-T.; Zhao, J.; Li, S.-P. Application of Smartphone in Detection of Thin-Layer Chromatography: Case of Salvia Miltiorrhiza. J. Chromatogr. A 2021, 1637, 461826. [Google Scholar] [CrossRef]
- Fichou, D.; Morlock, G.E. quanTLC, an Online Open-Source Solution for Videodensitometric Quantification. J. Chromatogr. A 2018, 1560, 78–81. [Google Scholar] [CrossRef]
- Mac Fhionnlaoich, N.; Ibsen, S.; Serrano, L.A.; Taylor, A.; Qi, R.; Guldin, S. A Toolkit to Quantify Target Compounds in Thin-Layer-Chromatography Experiments. J. Chem. Educ. 2018, 95, 2191–2196. [Google Scholar] [CrossRef]
- Jähnke, R.W.; Dwornik, K. A Concise Quality Control Guide on Essential Drugs and Other Medicines; Manual issued by the Global Pharma Health Fund (GPHF) for its GPHF-Minilab™, GPHF: Giessen, Germany, 2008. [Google Scholar]
- Global Use of the GPHF-MinilabTM. Available online: https://www.gphf.org/en/minilab/einsatzgebiete.htm (accessed on 13 May 2024).
- Petersen, A.; Held, N.; Heide, L. Surveillance for Falsified and Substandard Medicines in Africa and Asia by Local Organizations Using the Low-Cost GPHF Minilab. PLoS ONE 2017, 12, e0184165. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; Ba-Thein, W. Diagnostic Accuracy of Global Pharma Health Fund MinilabTM in Assessing Pharmacopoeial Quality of Antimicrobials. Am. J. Trop. Med. Hyg. 2018, 98, 344–348. [Google Scholar] [CrossRef]
- Sherma, J.; Rabel, F. Advances in the Thin Layer Chromatographic Analysis of Counterfeit Pharmaceutical Products: 2008–2019. J. Liq. Chromatogr. Relat. Technol. 2019, 42, 367–379. [Google Scholar] [CrossRef]
- Risha, P.; Msuya, Z.; Ndomondo-Sigonda, M.; Layloff, T. Proficiency Testing as a Tool to Assess the Performance of Visual TLC Quantitation Estimates. J. AOAC Int. 2006, 89, 1300–1304. [Google Scholar] [CrossRef]
- Kovacs, S.; Hawes, S.E.; Maley, S.N.; Mosites, E.; Wong, L.; Stergachis, A. Technologies for Detecting Falsified and Substandard Drugs in Low and Middle-Income Countries. PLoS ONE 2014, 9, e90601. [Google Scholar] [CrossRef]
- Vickers, S.; Bernier, M.; Zambrzycki, S.; Fernandez, F.M.; Newton, P.N.; Caillet, C. Field Detection Devices for Screening the Quality of Medicines: A Systematic Review. BMJ Glob. Health 2018, 3, e000725. [Google Scholar] [CrossRef] [PubMed]
- Zambrzycki, S.C.; Caillet, C.; Vickers, S.; Bouza, M.; Donndelinger, D.V.; Geben, L.C.; Bernier, M.C.; Newton, P.N.; Fernández, F.M. Laboratory Evaluation of Twelve Portable Devices for Medicine Quality Screening. PLoS Negl. Trop. Dis. 2021, 15, e0009360. [Google Scholar] [CrossRef] [PubMed]
- Opuni, K.F.-M.; Nettey, H.; Larbi, M.A.; Amartey, S.N.A.; Nti, G.; Dzidonu, A.; Owusu-Danso, P.; Owusu, N.A.; Nyarko, A.K. Usefulness of Combined Screening Methods for Rapid Detection of Falsified and/or Substandard Medicines in the Absence of a Confirmatory Method. Malar. J. 2019, 18, 403. [Google Scholar] [CrossRef] [PubMed]
- Kaale, E.; Risha, P.; Reich, E.; Layloff, T.P. An Interlaboratory Investigation on the Use of High-Performance Thin Layer Chromatography to Perform Assays of Lamivudine-Zidovudine, Metronidazole, Nevirapine, and Quinine Composite Samples. J. AOAC Int. 2010, 93, 1836–1843. [Google Scholar] [CrossRef]
- Zhang, D.; Armour, E.; Sherma, J. Development of Quantitative HPTLC–Densitometry Methods Following a Model Approach for Transfer of TLC Screening Methods for Pharmaceutical Products of Cefixime, Cefuroxime Axetil, cephalexin⋅H2O, Ciprofloxacin HCl, Levofloxacin, and Metronidazole. Acta Chromatogr. 2017, 29, 484–486. [Google Scholar] [CrossRef]
- Hauk, C.; Boss, M.; Gabel, J.; Schäfermann, S.; Lensch, H.P.A.; Heide, L. An Open-Source Smartphone App for the Quantitative Evaluation of Thin-Layer Chromatographic Analyses in Medicine Quality Screening. Sci. Rep. 2022, 12, 13433. [Google Scholar] [CrossRef]
- Sowers, M.E.; Ambrose, R.; Bethea, E.; Harmon, C.; Jenkins, D. Quantitative Thin Layer Chromatography for the Determination of Medroxyprogesterone Acetate Using a Smartphone and Open-Source Image Analysis. J. Chromatogr. A 2022, 1669, 462942. [Google Scholar] [CrossRef]
- Yu, H.; Le, H.M.; Kaale, E.; Long, K.D.; Layloff, T.; Lumetta, S.S.; Cunningham, B.T. Characterization of Drug Authenticity Using Thin-Layer Chromatography Imaging with a Mobile Phone. J. Pharm. Biomed. Anal. 2016, 125, 85–93. [Google Scholar] [CrossRef]
- Sowers, M.E.; Bethea, E.; Xiao, W.; Phase, N.; Harmon, C.; Jenkins, D. Quantification of Isoniazid in Tablets for Tuberculosis Treatment by Thin Layer Chromatography with Smartphone Image Capture and ImageJ Analysis. Microchem. J. 2024, 202, 110796. [Google Scholar] [CrossRef]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An Open-Source Platform for Biological-Image Analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef]
- Rueden, C.T.; Hiner, M.C.; Evans, E.L.; Pinkert, M.A.; Lucas, A.M.; Carpenter, A.E.; Cimini, B.A.; Eliceiri, K.W. PyImageJ: A Library for Integrating ImageJ and Python. Nat. Methods 2022, 19, 1326–1327. [Google Scholar] [CrossRef] [PubMed]
- United States Pharmacopoeia (USP). 〈1850〉 Evaluation of Screening Technologies for Assessing Medicine Quality. In USP-NF; USP: Rockville, MD, USA, 2023. [Google Scholar] [CrossRef]
- González, A.G.; Herrador, M.Á.; Asuero, A.G. Intra-Laboratory Assessment of Method Accuracy (Trueness and Precision) by Using Validation Standards. Talanta 2010, 82, 1995–1998. [Google Scholar] [CrossRef] [PubMed]
- Jähnke, R. Letter to the Editor on Previously Published GPHF-Minilab Assessment. Am. J. Trop. Med. Hyg. 2018, 98, 1880. [Google Scholar] [CrossRef] [PubMed]
- Boulgakov, A.A.; Moor, S.R.; Jo, H.H.; Metola, P.; Joyce, L.A.; Marcotte, E.M.; Welch, C.J.; Anslyn, E.V. Next-Generation TLC: A Quantitative Platform for Parallel Spotting and Imaging. J. Org. Chem. 2020, 85, 9447–9453. [Google Scholar] [CrossRef]
- Woortman, D.V.; Haack, M.; Mehlmer, N.; Brück, T.B. Additive Analytics: Easy Transformation of Low-Cost Fused Deposition Modeling Three-Dimensional Printers for HPTLC Sample Application. ACS Omega 2020, 5, 11147–11150. [Google Scholar] [CrossRef]
- TLCyzer. Available online: https://tlcyzer.github.io/ (accessed on 4 June 2024).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reagent | Grade | CAS Number | Manufacturer |
|---|---|---|---|
| Potassium Dihydrogen Phosphate | ACS | 7778-77-0 | VWR (Radnor, PA, USA) |
| Colloidal Anhydrous Silica/Colloidal Silicon Dioxide | NF, EP | 7631-86-9 | Spectrum Chemical (New Brunswick, NJ, USA) |
| Crospovidone/Povidone | USP | 9003-39-8 | Spectrum Chemical (New Brunswick, NJ, USA) |
| Magnesium Stearate | NF, EP, BP, JP | 557-04-0 | Spectrum Chemical (New Brunswick, NJ, USA) |
| Maize Starch | Lab | 9005-25-8 | Ward’s Science (Rochester, NY, USA) |
| Microcrystalline Cellulose | NF | 9004-34-6 | Spectrum Chemical (New Brunswick, NJ, USA) |
| Sodium Edetate | 98% Pure | 194491-31-1 | Acros Organics (Geel, Belgium) |
| Stearic Acid | 98% Pure | 57-11-4 | Beantown Chemical (Hudson, NH, USA) |
| Calcium Hydrogen Phosphate | 98% Pure | 7789-77-7 | Beantown Chemical (Hudson, NH, USA) |
| Croscarmellose Sodium | NF | 74811-65-7 | Spectrum Chemical (New Brunswick, NJ, USA) |
| Lactose Monohydrate | NF | 64044-51-5 | J.T. Baker (Phillipsburg, NJ, USA) |
| Mannitol | ACS | 69-65-8 | VWR (Radnor, PA, USA) |
| Pregelatinized Starch | ACS | 9005-84-9 | MP Biomedicals (Santa Ana, CA, USA) |
| Purified Talc | BP, EP, USP | 14807-96-6 | J.T. Baker (Phillipsburg, NJ, USA) |
| Google Pixel 4a 5G | Apple iPhone SE (2020) | |||||||
|---|---|---|---|---|---|---|---|---|
| 75/100/125% Standards | 50/100/150% Standards | 75/100/125% Standards | 50/100/150% Standards | |||||
| Avg | RSD | Avg | RSD | Avg | RSD | Avg | RSD | |
| Slope | 50,174 | 9.4% | 47,914 | 3.0% | 32,019 | 10.8% | 30,033 | 3.6% |
| Int. | 131,870 | 13.6% | 123,765 | 6.3% | 77,544 | 18.9% | 79,928 | 10.1% |
| R2 | 0.992 | 0.7% | 0.982 | 0.4% | 0.990 | 0.9% | 0.975 | 1.0% |
| Google Pixel 4a 5G | Apple iPhone SE (2020) | |||||||
|---|---|---|---|---|---|---|---|---|
| Label Claim | RSD | % Recovery | RSD | Label Claim | RSD | % Recovery | RSD | |
| 75% | 98.7% | 8.3% | 99.1% | 9.6% | 101.2% | 9.2% | 100.8% | 7.9% |
| 100% | 98.3% | 1.4% | 96.7% | 1.4% | 99.2% | 2.8% | 99.1% | 2.2% |
| 125% | 95.3% | 3.2% | 95.6% | 3.7% | 94.7% | 2.9% | 94.4% | 2.7% |
| Overall | 97.4% | 5.4% | 97.2% | 6.7% | 99.7% | 6.3% | 99.4% | 5.2% |
| Camera | Sample Concentration (% Label Claim) | Sr | RSDr | SIP | RSDIP |
|---|---|---|---|---|---|
| Google Pixel 4a 5G | 75% | 6.3% | 6.4% | 6.1% | 6.2% |
| 100% | 3.2% | 3.1% | 5.4% | 5.2% | |
| 125% | 3.0% | 3.1% | 4.4% | 4.4% | |
| Pooled | 4.2% | 4.2% | 5.6% | 5.6% | |
| Apple iPhone SE (2020) | 75% | 6.3% | 6.3% | 6.2% | 6.2% |
| 100% | 3.2% | 3.1% | 5.4% | 5.3% | |
| 125% | 2.9% | 3.0% | 4.1% | 4.2% | |
| Pooled | 4.2% | 4.2% | 5.5% | 5.4% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harmon, C.L.; Butts, S.; Sowers, M.E.; Bethea, E.; Jenkins, D. Quantification of Metronidazole in Tablets: Combining Thin-Layer Chromatography in the GPHF-Minilab™ with Image Processing Using Open-Source ImageJ Software. Analytica 2024, 5, 538-551. https://doi.org/10.3390/analytica5040036
Harmon CL, Butts S, Sowers ME, Bethea E, Jenkins D. Quantification of Metronidazole in Tablets: Combining Thin-Layer Chromatography in the GPHF-Minilab™ with Image Processing Using Open-Source ImageJ Software. Analytica. 2024; 5(4):538-551. https://doi.org/10.3390/analytica5040036
Chicago/Turabian StyleHarmon, Christopher L., Sean Butts, Mary Elizabeth Sowers, Ed Bethea, and David Jenkins. 2024. "Quantification of Metronidazole in Tablets: Combining Thin-Layer Chromatography in the GPHF-Minilab™ with Image Processing Using Open-Source ImageJ Software" Analytica 5, no. 4: 538-551. https://doi.org/10.3390/analytica5040036
APA StyleHarmon, C. L., Butts, S., Sowers, M. E., Bethea, E., & Jenkins, D. (2024). Quantification of Metronidazole in Tablets: Combining Thin-Layer Chromatography in the GPHF-Minilab™ with Image Processing Using Open-Source ImageJ Software. Analytica, 5(4), 538-551. https://doi.org/10.3390/analytica5040036