Comparing World Health Organization/International Society of Urological Pathology Grading and Fuhrman Grading with the Prognostic Value of Nuclear Area in Patients with Renal Cell Carcinoma



Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion of Patients
2.2. Evaluation of Pathological Parameters
2.3. Stereological Assessment of Nuclear Area
2.4. Statistics
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chawla, S.N.; Crispen, P.L.; Hanlon, A.L.; Greenberg, R.E.; Chen, D.Y.; Uzzo, R.G. The natural history of observed enhancing renal masses: Meta-analysis and review of the world literature. J. Urol. 2006, 175, 425–431. [Google Scholar] [CrossRef]
- Amin, M.B.; Amin, M.B.; Tamboli, P.; Javidan, J.; Stricker, H.; de-Peralta Venturina, M.; Deshpande, A.; Menon, M. Prognostic impact of histologic subtyping of adult renal epithelial neoplasms: An experience of 405 cases. Am. J. Surg. Pathol. 2002, 26, 281–291. [Google Scholar] [CrossRef]
- Frank, I.; Blute, M.L.; Cheville, J.C.; Lohse, C.M.; Weaver, A.L.; Zincke, H. An outcome prediction model for patients with clear cell renal cell carcinoma treated with radical nephrectomy based on tumor stage, size, grade and necrosis: The SSIGN score. J. Urol. 2002, 168, 2395–2400. [Google Scholar] [CrossRef]
- Delahunt, B.; McKenney, J.K.; Lohse, C.M.; Leibovich, B.C.; Thompson, R.H.; Boorjian, S.A.; Cheville, J.C. A novel grading system for clear cell renal cell carcinoma incorporating tumor necrosis. Am. J. Surg. Pathol. 2013, 37, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Fuhrman, S.A.; Lasky, L.C.; Limas, C. Prognostic significance of morphologic parameters in renal cell carcinoma. Am. J. Surg. Pathol. 1982, 6, 655–663. [Google Scholar] [CrossRef]
- Delahunt, B. Advances and controversies in grading and staging of renal cell carcinoma. Mod. Pathol. 2009, 22, S24–S36. [Google Scholar] [CrossRef]
- Delahunt, B.; Egevad, L.; Samaratunga, H.; Martignoni, G.; Nacey, J.N.; Srigley, J.R. Gleason and Fuhrman no longer make the grade. Histopathology 2016, 68, 475–481. [Google Scholar] [CrossRef]
- Delahunt, B.; Cheville, J.C.; Martignoni, G.; Humphrey, P.A.; Magi-Galluzzi, C.; McKenney, J.; Egevad, L.; Algaba, F.; Moch, H.; Grignon, D.J.; et al. The International Society of Urological Pathology (ISUP) grading system for renal cell carcinoma and other prognostic parameters. Am. J. Surg. Pathol. 2013, 37, 1490–1504. [Google Scholar] [CrossRef] [Green Version]
- Moch, H.; Humphrey, P.A.; Ulbright, T.M.; Reuter, V.E. (Eds.) WHO Classification of Tumours of the Urinary System and Male Genital Organs, 4th ed.; IARC: Lyon, France, 2016; Volume 8.
- Delahunt, B.; Sika-Paotonu, D.; Bethwaite, P.B.; McCredie, M.R.; Martignoni, G.; Eble, J.N.; Jordan, T.W. Fuhrman grading is not appropriate for chromophobe renal cell carcinoma. Am. J. Surg. Pathol. 2007, 31, 957–960. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Fernandez-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2019 Update. Eur. Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef]
- Dagher, J.; Delahunt, B.; Rioux-Leclercq, N.; Egevad, L.; Coughlin, G.; Dunglison, N.; Gianduzzo, T.; Kua, B.; Malone, G.; Martin, B.; et al. Assessment of tumour-associated necrosis provides prognostic information additional to World Health Organization/International Society of Urological Pathology grading for clear cell renal cell carcinoma. Histopathology 2019, 74, 284–290. [Google Scholar] [CrossRef]
- Khor, L.Y.; Dhakal, H.P.; Jia, X.; Reynolds, J.P.; McKenney, J.K.; Rini, B.I.; Magi-Galluzzi, C.; Przybycin, C.G. Tumor Necrosis Adds Prognostically Significant Information to Grade in Clear Cell Renal Cell Carcinoma: A Study of 842 Consecutive Cases From a Single Institution. Am. J. Surg. Pathol. 2016, 40, 1224–1231. [Google Scholar] [CrossRef]
- Katz, M.D.; Serrano, M.F.; Grubb, R.L., 3rd; Skolarus, T.A.; Gao, F.; Humphrey, P.A.; Kibel, A.S. Percent microscopic tumor necrosis and survival after curative surgery for renal cell carcinoma. J. Urol. 2010, 183, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Pichler, M.; Hutterer, G.C.; Chromecki, T.F.; Jesche, J.; Kampel-Kettner, K.; Rehak, P.; Pummer, K.; Zigeuner, R. Histologic tumor necrosis is an independent prognostic indicator for clear cell and papillary renal cell carcinoma. Am. J. Clin. Pathol. 2012, 137, 283–289. [Google Scholar] [CrossRef] [Green Version]
- Carducci, M.A.; Piantadosi, S.; Pound, C.R.; Epstein, J.I.; Simons, J.W.; Marshall, F.F.; Partin, A.W. Nuclear morphometry adds significant prognostic information to stage and grade for renal cell carcinoma. Urology 1999, 53, 44–49. [Google Scholar] [CrossRef]
- Ozer, E.; Yorukoglu, K.; Sagol, O.; Mungan, U.; Demirel, D.; Tuzel, E.; Kirkali, Z. Prognostic significance of nuclear morphometry in renal cell carcinoma. BJU Int. 2002, 90, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Dagher, J.; Delahunt, B.; Rioux-Leclercq, N.; Egevad, L.; Srigley, J.R.; Coughlin, G.; Dunglinson, N.; Gianduzzo, T.; Kua, B.; Malone, G.; et al. Clear cell renal cell carcinoma: Validation of World Health Organization/International Society of Urological Pathology grading. Histopathology 2017, 71, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Q.; Yi, X.; Guan, X.; Yin, H.; Wang, C.; Zhang, L.; Pang, Y.; Li, M.; Gong, G.; Chen, D.; et al. Validation of the World Health Organization/International Society of Urological Pathology grading for Chinese patients with clear cell renal cell carcinoma. Transl. Androl. Urol. 2020, 9, 2665–2674. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr.; Califf, R.M.; Pryor, D.B.; Lee, K.L.; Rosati, R.A. Evaluating the yield of medical tests. JAMA 1982, 247, 2543–2546. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr.; Lee, K.L.; Califf, R.M.; Pryor, D.B.; Rosati, R.A. Regression modelling strategies for improved prognostic prediction. Stat. Med. 1984, 3, 143–152. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Kottner, J.; Audige, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hrobjartsson, A.; Roberts, C.; Shoukri, M.; Streiner, D.L. Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were proposed. J. Clin. Epidemiol. 2011, 64, 96–106. [Google Scholar] [CrossRef]
- Lang, H.; Lindner, V.; de Fromont, M.; Molinie, V.; Letourneux, H.; Meyer, N.; Martin, M.; Jacqmin, D. Multicenter determination of optimal interobserver agreement using the Fuhrman grading system for renal cell carcinoma: Assessment of 241 patients with > 15-year follow-up. Cancer 2005, 103, 625–629. [Google Scholar] [CrossRef]
- Bektas, S.; Bahadir, B.; Kandemir, N.O.; Barut, F.; Gul, A.E.; Ozdamar, S.O. Intraobserver and interobserver variability of Fuhrman and modified Fuhrman grading systems for conventional renal cell carcinoma. Kaohsiung J. Med. Sci. 2009, 25, 596–600. [Google Scholar] [CrossRef] [Green Version]
- Cornejo, K.M.; Dong, F.; Zhou, A.G.; Wu, C.L.; Young, R.H.; Braaten, K.; Sadow, P.M.; Nielsen, G.P.; Oliva, E. Papillary renal cell carcinoma: Correlation of tumor grade and histologic characteristics with clinical outcome. Hum. Pathol. 2015, 46, 1411–1417. [Google Scholar] [CrossRef]
- Kanamaru, H.; Akino, H.; Suzuki, Y.; Noriki, S.; Okada, K. Prognostic value of nuclear area index in combination with the World Health Organization grading system for patients with renal cell carcinoma. Urology 2001, 57, 257–261. [Google Scholar] [CrossRef]
- Montironi, R.; Santinelli, A.; Pomante, R.; Mazzucchelli, R.; Colanzi, P.; Filho, A.L.; Scarpelli, M. Morphometric index of adult renal cell carcinoma. Comparison with the Fuhrman grading system. Virchows Arch. 2000, 437, 82–89. [Google Scholar] [CrossRef]
- Sheela Devi, C.S.; Suchitha, S.; Veerendrasagar, R.S. Evaluation of Nuclear Morphometry and Ki-67 Index in Clear Cell Renal Cell Carcinomas: A Five-Year Study. Iran J. Pathol. 2017, 12, 150–157. [Google Scholar]
- Verine, J.; Colin, D.; Nheb, M.; Prapotnich, D.; Ploussard, G.; Cathelineau, X.; Desgrandchamps, F.; Mongiat-Artus, P.; Feugeas, J.P. Architectural Patterns are a Relevant Morphologic Grading System for Clear Cell Renal Cell Carcinoma Prognosis Assessment: Comparisons with WHO/ISUP Grade and Integrated Staging Systems. Am. J. Surg. Pathol. 2018, 42, 423–441. [Google Scholar] [CrossRef]
- Delahunt, B.; Eble, J.N.; Egevad, L.; Samaratunga, H. Grading of renal cell carcinoma. Histopathology 2019, 74, 4–17. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grading System | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
|---|---|---|---|---|
| Fuhrman | Small (≈10 μm) round uniform nuclei with absent or inconspicuous nucleoli | Larger (≈15 μm) nuclei with irregularities in outline and with nucleoli visible at ×400 magnification | Even larger nuclei (≈20 μm) with an obvious irregular outline and nucleoli visible at ×100 magnification | Cells large, pleomorphic with bizarre multilobed giant cells and heavy chromatin clumps, extreme irregular outlines |
| WHO/ISUP | Absent or basophilic, inconspicuous nucleoli at ×400 magnification | Nucleoli conspicuous and eosinophilic at ×400 magnification and visible, but not prominent at ×100 magnification | Nucleoli conspicuous and eosinophilic at ×100 magnification | Rhabdoid or sarcomatous differentiation, tumor giant cells and extreme nuclear pleomorphism with clumping of chromatin |
| Delahunt [4] | ISUP G1 with/without necrosis and ISUP G2 without necrosis | ISUP G2 with necrosis and ISUP G3 without necrosis | ISUP G3 with necrosis and ISUP G4 without necrosis | ISUP G4 with necrosis or sarcomatoid/rhabdoid features |
| Mean (SD) Variable | N (%) | MNA µm2 (SD) | p-Value | MNA-10 µm2 (SD) | p-Value |
|---|---|---|---|---|---|
| Sex * | |||||
| Male | 75 (60) | 42.9 (13.8) | 0.8 | 80.3 (27.1) | 0.7 |
| Female | 49 (40) | 42.2 (16.2) | 82.1 (35.1) | ||
| Histology ** | |||||
| ccRCC | 101 (81) | 41.7 (15.2) | 0.06 | 80.9 (32.2) | 0.38 |
| Papillary type 1 | 14 (11) | 42.3 (10.3) | 74.7 (19.9) | ||
| Papillary type 2 | 9 (8) | 53.8(11.42) | 92.6 (18.8) | ||
| Stage ** | |||||
| pT1 | 57 (46) | 39.2 (13.7) | 0.1 | 73.4 (26.7) | 0.07 |
| pT2 | 22 (18) | 44.8 (12.9) | 87.2 (26.3) | ||
| pT3 | 40 (33) | 46.4 (16.6) | 87.1 (33.8) | ||
| pT4 | 4 (3) | 45.0 (14.8) | 95.0 (52.8) | ||
| Necrosis * | |||||
| Absent | 79 | 37.6 (10.9) | <0.0001 | 69.6 (19.9) | <0.0001 |
| Present | 45 | 51.6 (16.4) | 100.9 (35.3) | ||
| Grading Systems | WHO/ISUP | Total | |||
|---|---|---|---|---|---|
| Fuhrman | 1 | 2 | 3 | 4 | |
| 1 | 5 | 0 | 0 | 0 | 5 |
| 2 | 21 | 38 | 2 | 0 | 61 |
| 3 | 0 | 9 | 34 | 0 | 43 |
| 4 | 0 | 0 | 1 | 14 | 15 |
| Total | 26 | 47 | 37 | 14 | |
| Models | Groups | AUC-ROC (95% CI) | Harrell’s C-index (95% CI) |
|---|---|---|---|
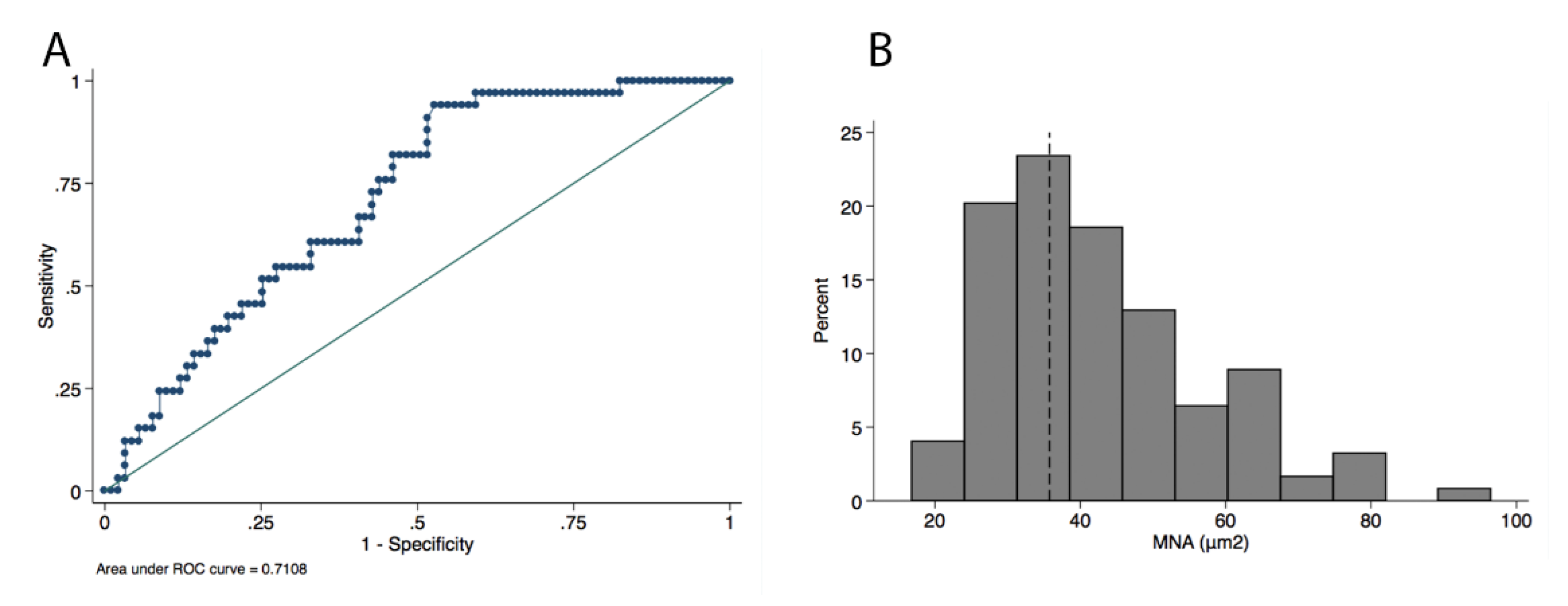
| MNA | MNA low vs high | 0.71 (0.62–0.82) | 0.7 (0.62–0.79) |
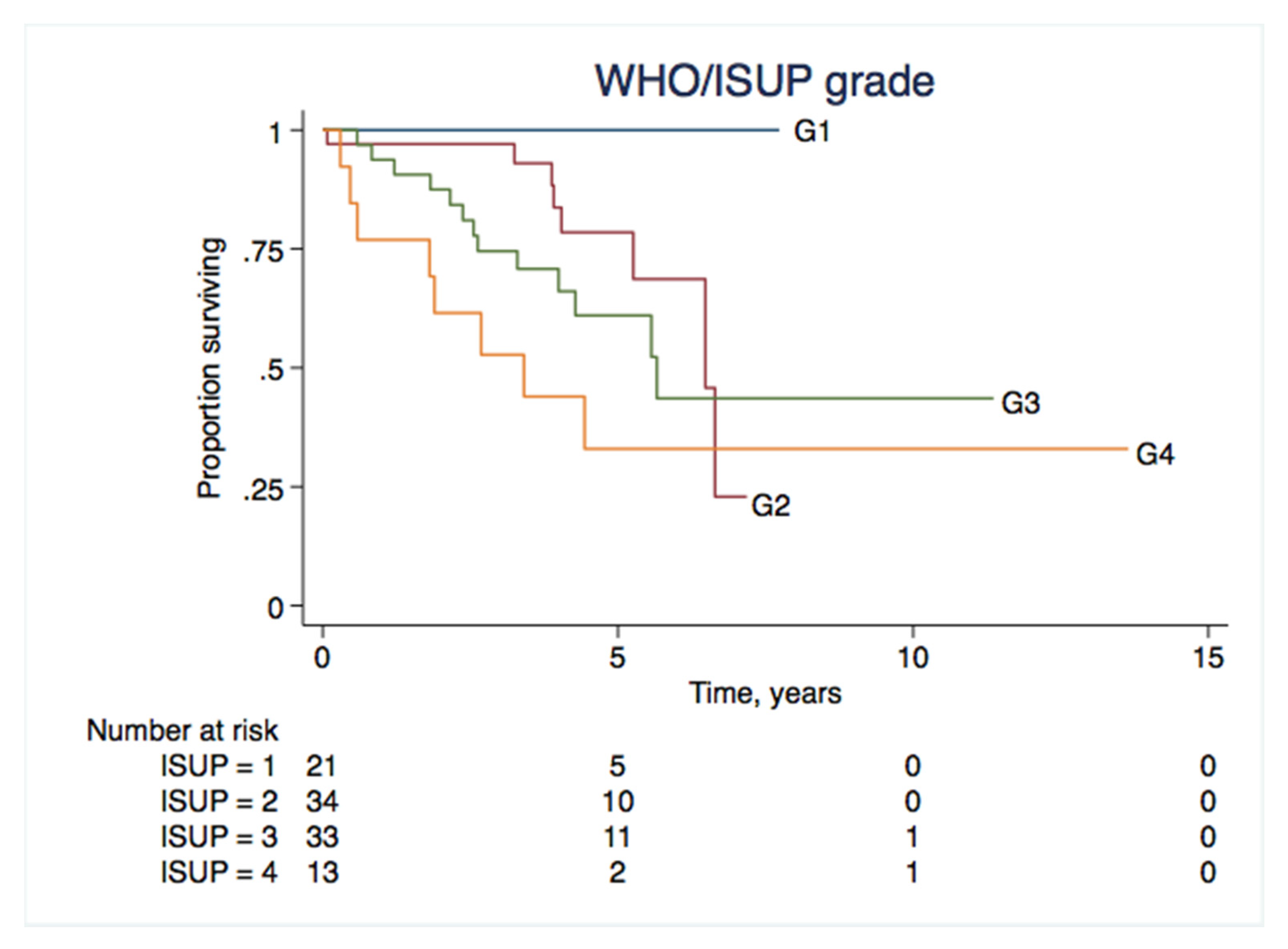
| WHO/ISUP | G1-G4 | 0.75 (0.66–0.84) | 0.74 (0.66–0.83) |
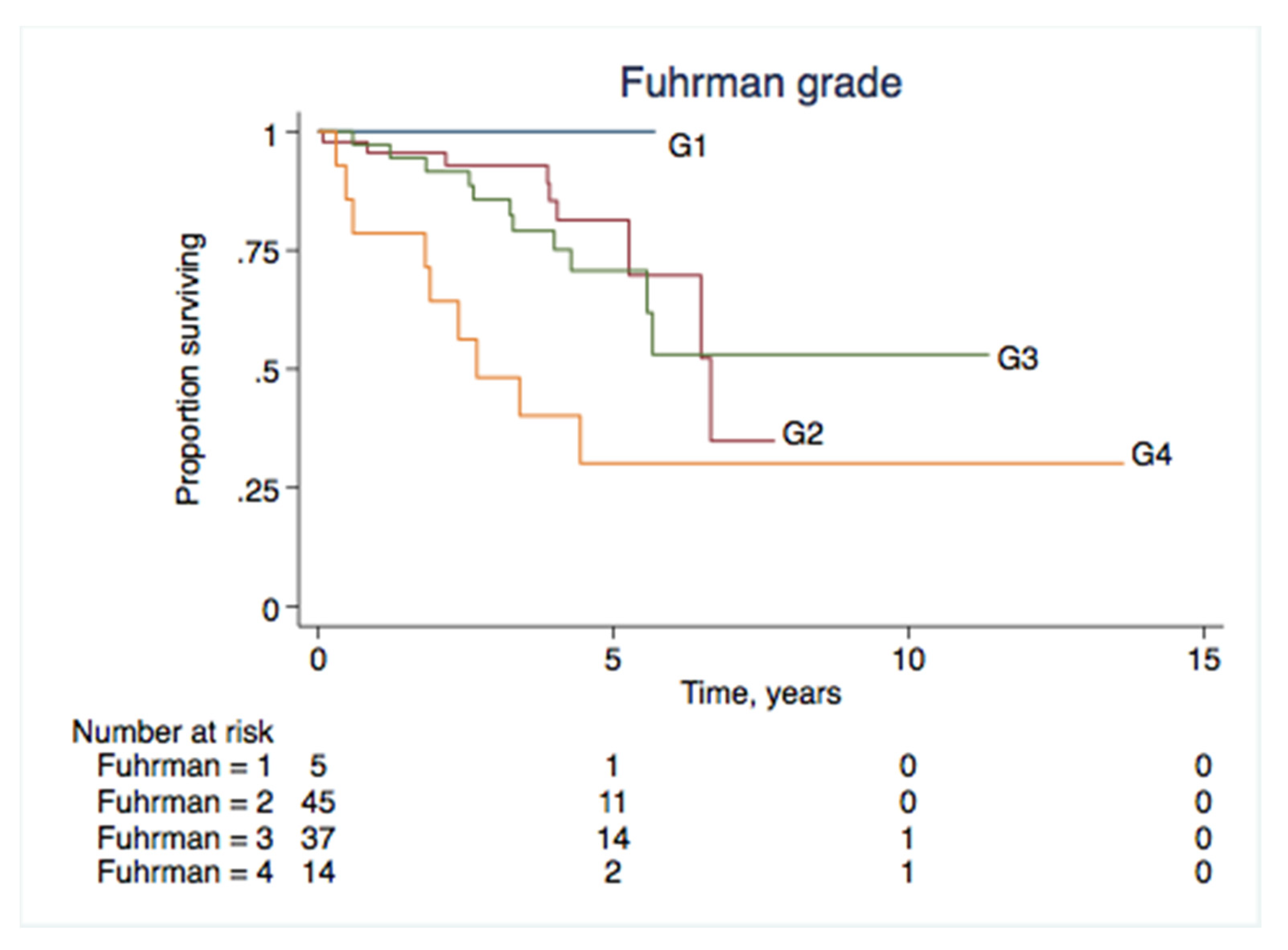
| Fuhrman | G1-G4 | 0.68 (0.57–0.79) | 0.68 (0.58–0.79) |
| Novel Models | |||
| MNA and tumor necrosis | |||
| Grade 1 | MNA low/no necrosis | 0.8 (0.72–0.88) | 0.76 (0.68–0.83) |
| Grade 2 | MNA low/with necrosis | ||
| Grade 3 | MNA high/no necrosis | ||
| Grade 4 | MNA high/with necrosis | ||
| Delahunt modified groups [4] | |||
| Grade 1 | ISUP G1/no necrosis | 0.76 (0.65–0.86) | 0.75 (0.66–0.85) |
| ISUP G1/with necrosis | |||
| ISUP G2/no necrosis | |||
| Grade 2 | ISUP G2/ with necrosis | ||
| ISUP G3/ no necrosis | |||
| Grade 3 | ISUP G3/ with necrosis | ||
| ISUP G4/no necrosis | |||
| Grade 4 | ISUP G4/ with necrosis or sarkomatoid differentiation | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rabjerg, M.; Gerke, O.; Engvad, B.; Marcussen, N. Comparing World Health Organization/International Society of Urological Pathology Grading and Fuhrman Grading with the Prognostic Value of Nuclear Area in Patients with Renal Cell Carcinoma. Uro 2021, 1, 2-13. https://doi.org/10.3390/uro1010002
Rabjerg M, Gerke O, Engvad B, Marcussen N. Comparing World Health Organization/International Society of Urological Pathology Grading and Fuhrman Grading with the Prognostic Value of Nuclear Area in Patients with Renal Cell Carcinoma. Uro. 2021; 1(1):2-13. https://doi.org/10.3390/uro1010002
Chicago/Turabian StyleRabjerg, Maj, Oke Gerke, Birte Engvad, and Niels Marcussen. 2021. "Comparing World Health Organization/International Society of Urological Pathology Grading and Fuhrman Grading with the Prognostic Value of Nuclear Area in Patients with Renal Cell Carcinoma" Uro 1, no. 1: 2-13. https://doi.org/10.3390/uro1010002
APA StyleRabjerg, M., Gerke, O., Engvad, B., & Marcussen, N. (2021). Comparing World Health Organization/International Society of Urological Pathology Grading and Fuhrman Grading with the Prognostic Value of Nuclear Area in Patients with Renal Cell Carcinoma. Uro, 1(1), 2-13. https://doi.org/10.3390/uro1010002