
Child Marriage and Later-Life Risk of Obesity in Women: A Cohort Analysis Using Nationally Representative Repeated Cross-Sectional Data from Tajikistan


Abstract
1. Introduction
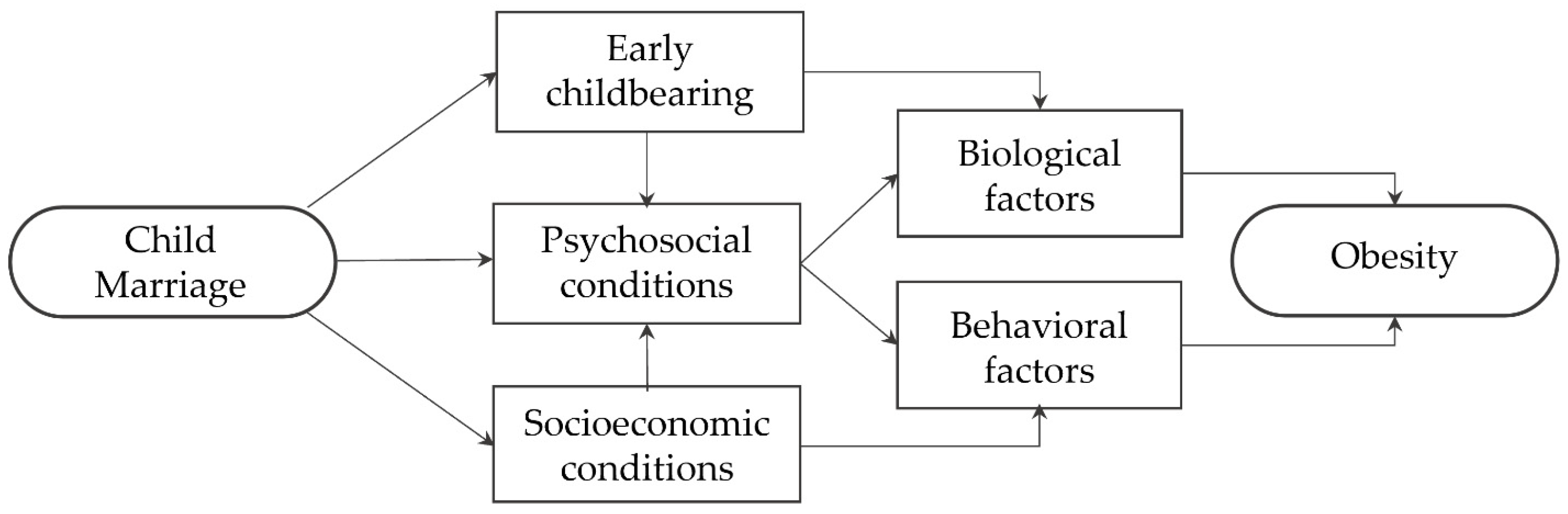
1.1. Conceptual Framework
1.2. Aim
2. Results
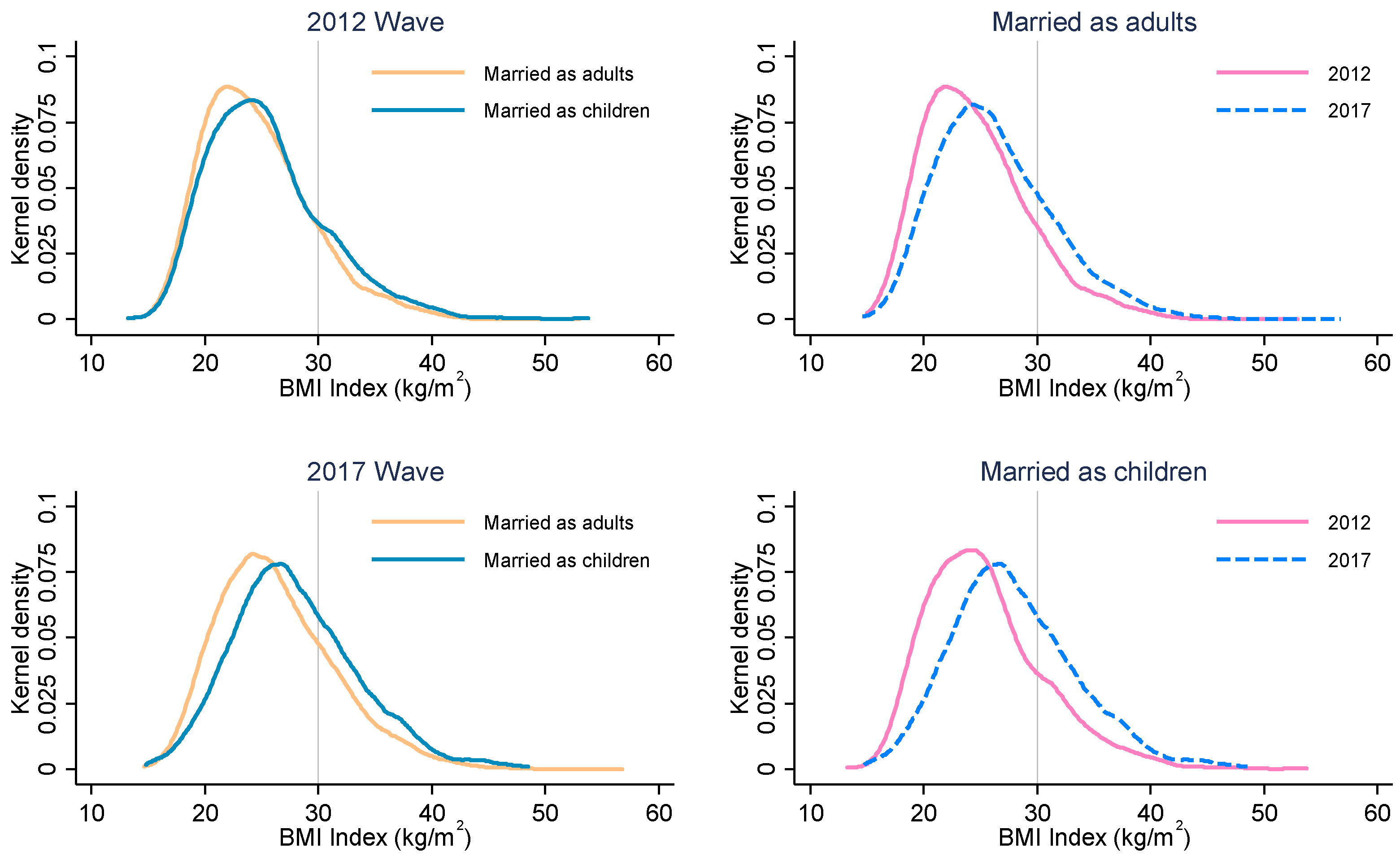
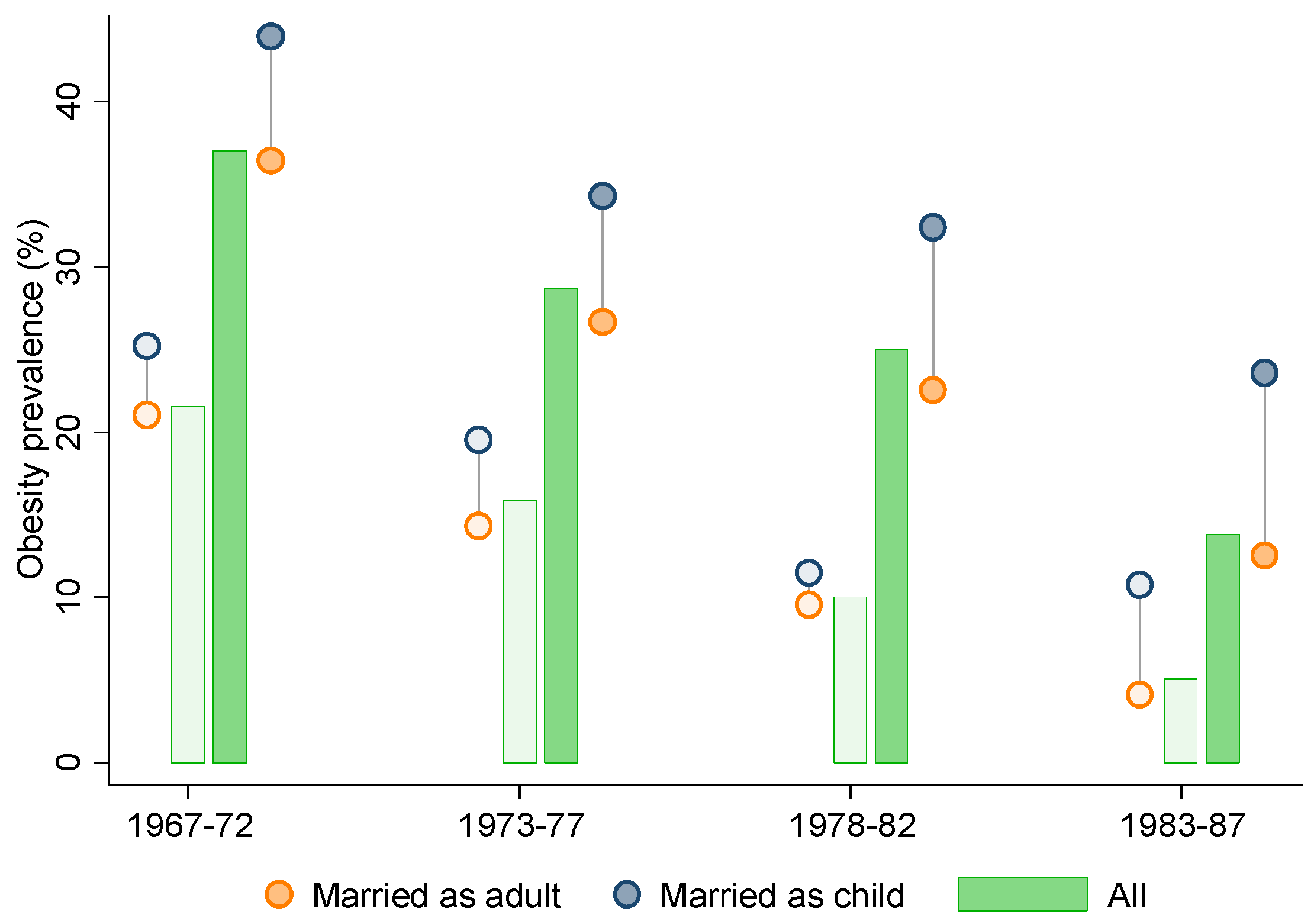
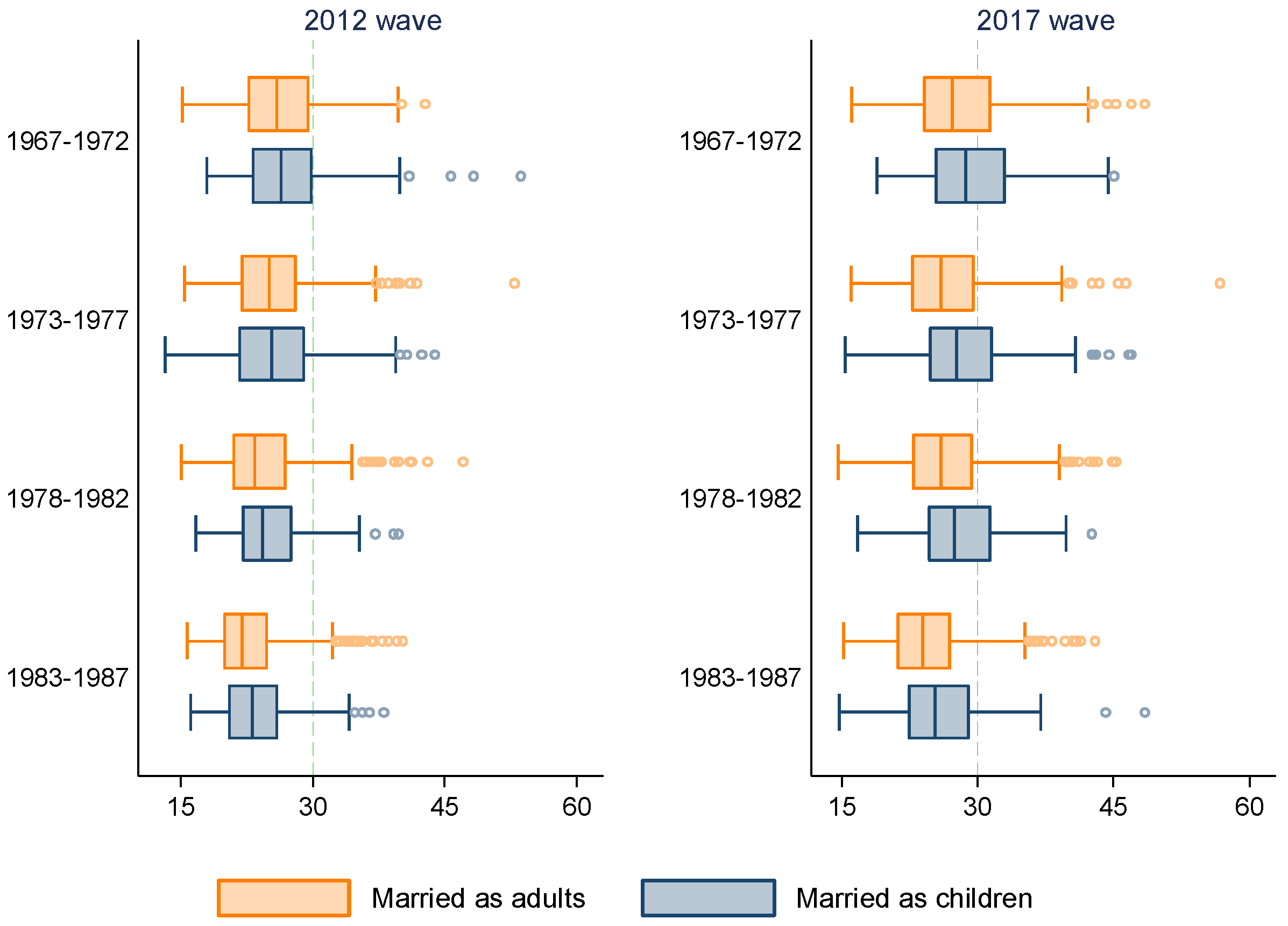
2.1. Descriptive Results
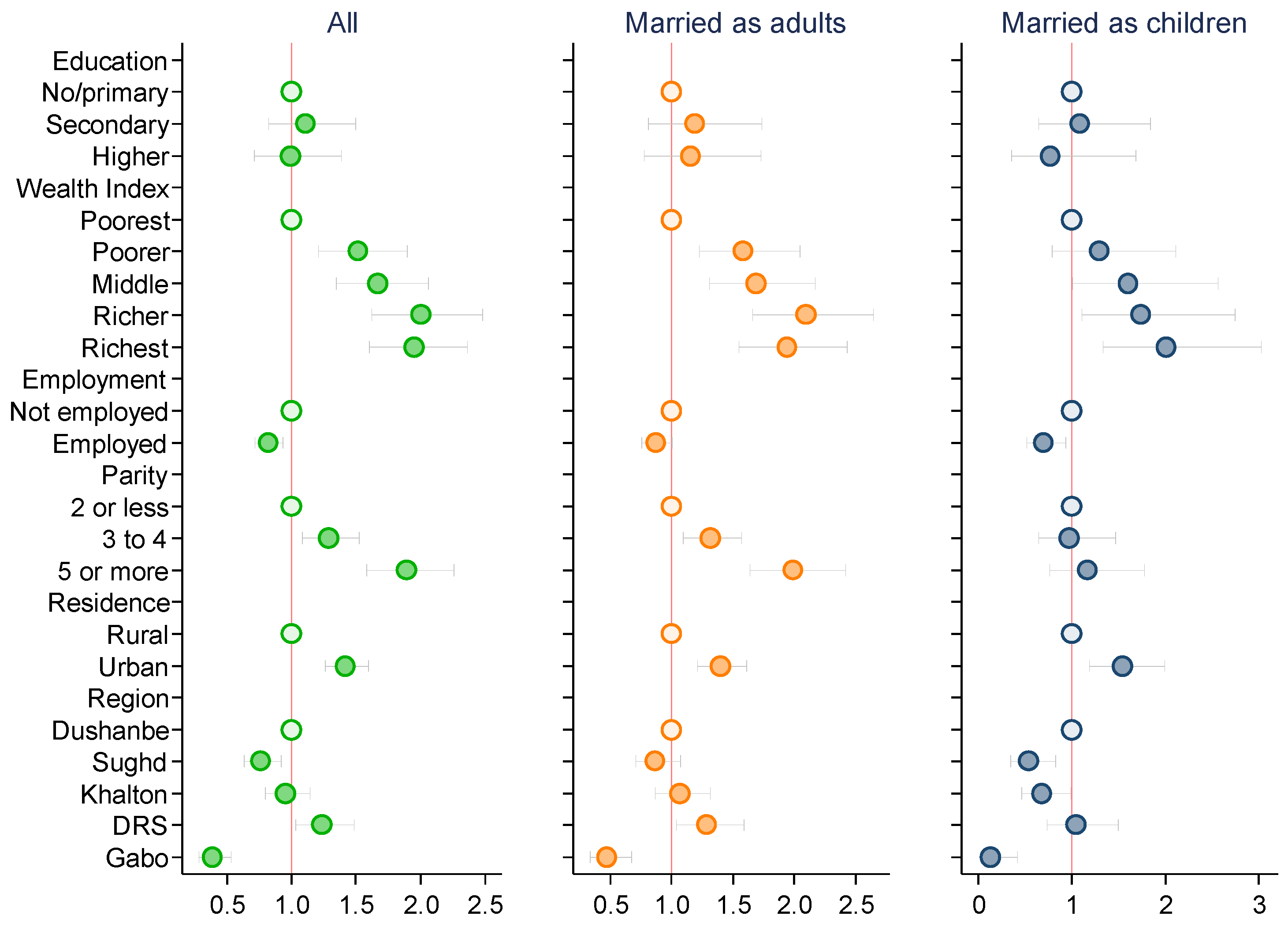
2.2. Relationship between Obesity and Sociodemographic Correlates
2.3. Regression Results
3. Discussion
4. Materials and Methods
4.1. Data
4.2. Measures
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ford, N.D.; Patel, S.A.; Narayan, K.M.V. Obesity in Low- and Middle-Income Countries: Burden, Drivers, and Emerging Challenges. Annu. Rev. Public Health 2017, 38, 145–164. [Google Scholar] [CrossRef]
- Kanguru, L.; McCaw-Binns, A.; Bell, J.; Yonger-Coleman, N.; Wilks, R.; Hussein, J. The Burden of Obesity in Women of Reproductive Age and in Pregnancy in a Middle-Income Setting: A Population Based Study from Jamaica. PLoS ONE 2017, 12, e0188677. [Google Scholar] [CrossRef]
- Kulie, T.; Slattengren, A.; Redmer, J.; Counts, H.; Eglash, A.; Schrager, S. Obesity and Women’s Health: An Evidence-Based Review. J. Am. Board Fam. Med. 2011, 24, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Newton, S.; Braithwaite, D.; Akinyemiju, T.F. Socio-Economic Status over the Life Course and Obesity: Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0177151. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.-J.R.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E.; European Union Working Group on Socioeconomic Inequalities in Health. Socioeconomic Inequalities in Health in 22 European Countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef]
- Reyes Matos, U.; Mesenburg, M.A.; Victora, C.G. Socioeconomic Inequalities in the Prevalence of Underweight, Overweight, and Obesity among Women Aged 20-49 in Low- and Middle-Income Countries. Int. J. Obes. 2020, 44, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Barth-Jaeggi, T.; Zandberg, L.; Bahruddinov, M.; Kiefer, S.; Rahmarulloev, S.; Wyss, K. Nutritional Status of Tajik Children and Women: Transition towards a Double Burden of Malnutrition. Matern. Child Nutr. 2020, 16, e12886. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.R.; Dearing, E.; Usher, N.; Trifiletti, S.; Zaichenko, L.; Ollen, E.; Brinkoetter, M.T.; Crowell-Doom, C.; Joung, K.; Park, K.H.; et al. Detailed Assessments of Childhood Adversity Enhance Prediction of Central Obesity Independent of Gender, Race, Adult Psychosocial Risk and Health Behaviors. Metabolism 2014, 63, 199–206. [Google Scholar] [CrossRef]
- United Nations Children’s Fund (UNICEF). Early Marriage—A Harmful Traditional Practice—A Statistical Exploration; UNICEF: New York, NY, USA, 2005; Available online: https://data.unicef.org/resources/early-marriage-a-traditional-harmful-practice-a-statistical-exploration/ (accessed on 10 September 2022).
- Fan, S.; Koski, A. The Health Consequences of Child Marriage: A Systematic Review of the Evidence. BMC Public Health 2022, 22, 309. [Google Scholar] [CrossRef]
- Santhya, K.; Jejeebhoy, S. Sexual and reproductive health needs of married adolescent girls. Econ. Political Wkly. 2003, 38, 4370–4377. [Google Scholar]
- Clark, S.; Bruce, J.; Dude, A. Protecting Young Women from HIV/AIDS: The Case against Child and Adolescent Marriage. Int. Fam. Plan. Perspect. 2006, 32, 79–88. [Google Scholar] [CrossRef]
- Parsons, J.; Edmeades, J.; Kes, A.; Petroni, S.; Sexton, M.; Wodon, Q. Economic Impacts of Child Marriage: A Review of the Literature. Rev. Faith Int. Aff. 2015, 13, 12–22. [Google Scholar] [CrossRef]
- Martin, M.A.; Lippert, A.M. Feeding Her Children, but Risking Her Health: The Intersection of Gender, Household Food Insecurity and Obesity. Soc. Sci. Med. 2012, 74, 1754–1764. [Google Scholar] [CrossRef]
- Basiotis, P.; Lino, M. Food insufficiency and prevalence of overweight among adult women. Fam. Econ. Nutr. Rev. 2003, 15, 55–58. [Google Scholar]
- Townsend, M.S.; Peerson, J.; Love, B.; Achterberg, C.; Murphy, S.P. Food Insecurity Is Positively Related to Overweight in Women. J. Nutr. 2001, 131, 1738–1745. [Google Scholar] [CrossRef]
- Keats, E.C.; Rappaport, A.I.; Shah, S.; Oh, C.; Jain, R.; Bhutta, Z.A. The Dietary Intake and Practices of Adolescent Girls in Low- and Middle-Income Countries: A Systematic Review. Nutrients 2018, 10, 1978. [Google Scholar] [CrossRef]
- Yaya, S.; Odusina, E.K.; Bishwajit, G. Prevalence of Child Marriage and Its Impact on Fertility Outcomes in 34 Sub-Saharan African Countries. BMC Int. Health Hum. Rights 2019, 19, 33. [Google Scholar] [CrossRef]
- Statistical Agency under the President of the Republic of Tajikistan (SA); Ministry of Health of Tajikistan (MOH); ICF International. Tajikistan Demographic and Health Survey 2012; SA: Dushanbe, Tajikistan; MOH: Dushanbe, Tajikistan; ICF: Calverton, MD, USA, 2013; Available online: https://dhsprogram.com/pubs/pdf/FR279/FR279.pdf (accessed on 10 September 2022).
- Statistical Agency under the President of the Republic of Tajikistan (SA); Ministry of Health of the Republic of Tajikistan (MOHSP); ICF International. Tajikistan Demographic and Health Survey 2017; SA: Dushanbe, Tajikistan; MOH: Dushanbe, Tajikistan; ICF: Calverton, MD, USA, 2018; Available online: https://dhsprogram.com/pubs/pdf/FR341/FR341.pdf (accessed on 10 September 2022).
- Datta, B.K.; Haider, M.R.; Tiwari, A.; Jahan, M. The Risk of Hypertension among Child Brides and Adolescent Mothers at Age 20 s, 30 s, and 40 s: Evidence from India. J. Hum. Hypertens. 2022. [Google Scholar] [CrossRef]
- Datta, B.; Tiwari, A. Adding to Her Woes: Child Bride’s Higher Risk of Hypertension at Young Adulthood. J. Public Health 2022, fdac026. [Google Scholar] [CrossRef]
- Datta, B.; Tiwari, A. Early Marriage in Adolescence and Risk of High Blood Pressure and High Blood Glucose in Adulthood: Evidence from India. Women 2022, 2, 189–203. [Google Scholar] [CrossRef]
- Datta, B.; Tiwari, A.; Glenn, L. Stolen Childhood Taking a Toll at Young Adulthood: The Higher Risk of High Blood Pressure and High Blood Glucose Comorbidity among Child Brides. PLoS Glob. Public Health 2022, 2, e0000638. [Google Scholar] [CrossRef]
- Efevbera, Y.; Bhabha, J.; Farmer, P.; Fink, G. Girl Child Marriage, Socioeconomic Status, and Undernutrition: Evidence from 35 Countries in Sub-Saharan Africa. BMC Med. 2019, 17, 55. [Google Scholar] [CrossRef]
- Datta, B.K.; Haider, M.R. The Double Burden of Overweight or Obesity and Anemia among Women Married as Children in India: A Case of the Simpson’s Paradox. Obes. Res. Clin. Pract. 2022, 16, 364–372. [Google Scholar] [CrossRef]
- Gunderson, E.P.; Abrams, B.; Selvin, S. The Relative Importance of Gestational Gain and Maternal Characteristics Associated with the Risk of Becoming Overweight after Pregnancy. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1660–1668. [Google Scholar] [CrossRef]
- van den Broek, T.; Fleischmann, M. The Causal Effect of Number of Children on Later-Life Overweight and Obesity in Parous Women. An Instrumental Variable Study. Prev. Med. Rep. 2021, 24, 101528. [Google Scholar] [CrossRef]
- Burgess, R.A.; Jeffery, M.; Odero, S.A.; Rose-Clarke, K.; Devakumar, D. Overlooked and Unaddressed: A Narrative Review of Mental Health Consequences of Child Marriages. PLoS Glob. Public Health 2022, 2, e0000131. [Google Scholar] [CrossRef]
- Tebb, K.P.; Brindis, C.D. Understanding the Psychological Impacts of Teenage Pregnancy through a Socio-Ecological Framework and Life Course Approach. Semin. Reprod. Med. 2022, 40, 107–115. [Google Scholar] [CrossRef]
- Thomas, K.; Nilsson, E.; Festin, K.; Henriksson, P.; Lowén, M.; Löf, M.; Kristenson, M. Associations of Psychosocial Factors with Multiple Health Behaviors: A Population-Based Study of Middle-Aged Men and Women. Int. J. Environ. Res. Public Health 2020, 17, 1239. [Google Scholar] [CrossRef]
- Moore, C.J.; Cunningham, S.A. Social Position, Psychological Stress, and Obesity: A Systematic Review. J. Acad. Nutr. Diet. 2012, 112, 518–526. [Google Scholar] [CrossRef]
- Hanna, B.; Kleinman, A. Unpacking Global Health: Theory and Critique. In Reimagining Global Health; University of California Press: Berkeley, CA, USA, 2013; pp. 15–32. [Google Scholar]
- Pervanidou, P.; Chrousos, G.P. Metabolic Consequences of Stress during Childhood and Adolescence. Metabolism 2012, 61, 611–619. [Google Scholar] [CrossRef]
- Cameron, A.J.; Spence, A.C.; Laws, R.; Hesketh, K.D.; Lioret, S.; Campbell, K.J. A Review of the Relationship Between Socioeconomic Position and the Early-Life Predictors of Obesity. Curr. Obes. Rep. 2015, 4, 350–362. [Google Scholar] [CrossRef]
- United Nations Population Fund (UNFPA). Girlhood, Not Motherhood: Preventing Adolescent Pregnancy; UNFPA: New York, NY, USA, 2015; Available online: https://www.unfpa.org/publications/girlhood-not-motherhood (accessed on 10 September 2022).
- Godha, D.; Hotchkiss, D.; Gage, A. Association between child marriage and reproductive health outcomes and service utilization: A multi-country study from South Asia. J. Adolesc. Health 2013, 52, 552–558. [Google Scholar] [CrossRef]
- Nour, N.M. Health Consequences of Child Marriage in Africa. Emerg. Infect. Dis. 2006, 12, 1644–1649. [Google Scholar] [CrossRef]
- Davis, E.M.; Zyzanski, S.J.; Olson, C.M.; Stange, K.C.; Horwitz, R.I. Racial, Ethnic, and Socioeconomic Differences in the Incidence of Obesity Related to Childbirth. Am. J. Public Health 2009, 99, 294–299. [Google Scholar] [CrossRef]
- Costa-Font, J.; Györi, M. The Weight of Patriarchy? Gender Obesity Gaps in the Middle East and North Africa (MENA). Soc. Sci. Med. 2020, 266, 113353. [Google Scholar] [CrossRef]
- Haberland, N.; Chong, E.L.; Bracken, H.J. A world apart: The disadvantage and social isolation of married adolescent girls. In Brief Based on Background Paper Prepared for the WHO/UNFPA/Population Council Technical Consultation on Married Adolescents; Population Council: New York, NY, USA, 2004; Available online: https://www.ohchr.org/sites/default/files/Documents/Issues/Women/WRGS/ForcedMarriage/NGO/PopulationCouncil28.pdf (accessed on 28 December 2022).
- Aitsi-Selmi, A.; Bell, R.; Shipley, M.J.; Marmot, M.G. Education Modifies the Association of Wealth with Obesity in Women in Middle-Income but Not Low-Income Countries: An Interaction Study Using Seven National Datasets, 2005–2010. PLoS ONE 2014, 9, e90403. [Google Scholar] [CrossRef]
- McCleary-Sills, J.; Hanmer, L.; Parsons, J.; Klugman, J. Child Marriage: A Critical Barrier to Girls’ Schooling and Gender Equality in Education. Rev. Faith Int. Aff. 2015, 13, 69–80. [Google Scholar] [CrossRef]
- Stanford, F.C.; Lee, M.; Hur, C. Race, Ethnicity, Sex, and Obesity: Is It Time to Personalize the Scale? Mayo Clin. Proc. 2019, 94, 362–363. [Google Scholar] [CrossRef]
- Cottino, G. Obesity “Epidemic” in the Kingdom of Tonga: Critical Notes on the “Right” Body Size. J. Anthropol. 2014, 138–139, 65–87. [Google Scholar] [CrossRef]
- Karlson, K.B.; Holm, A.; Breen, R. Comparing Regression Coefficients Between Same-Sample Nested Models Using Logit and Probit: A New Method. Sociol. Methodol. 2012, 42, 286–313. [Google Scholar] [CrossRef]
- Minocher, R.; Ross, C.T. Spousal Age-Gaps, Partner Preferences, and Consequences for Well-Being in Four Colombian Communities. Evol. Hum. Behav. 2022, 43, 394–407. [Google Scholar] [CrossRef]
- Wilson, S.E. Marriage, Gender and Obesity in Later Life. Econ. Hum. Biol. 2012, 10, 431–453. [Google Scholar] [CrossRef]
- Mata, J.; Richter, D.; Schneider, T.; Hertwig, R. How Cohabitation, Marriage, Separation, and Divorce Influence BMI: A Prospective Panel Study. Health Psychol. 2018, 37, 948–958. [Google Scholar] [CrossRef] [PubMed]
- Batyra, E.; Pesando, L.M. Trends in Child Marriage and New Evidence on the Selective Impact of Changes in Age-at-Marriage Laws on Early Marriage. SSM—Popul. Health 2021, 14, 100811. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, S.J.; Hendi, J.M.; Marsillo, L. A Public Health Approach to Decreasing Obesity. JAMA 2002, 288, 2178. [Google Scholar] [CrossRef] [PubMed]
- Salam, R.A.; Padhani, Z.A.; Das, J.K.; Shaikh, A.Y.; Hoodbhoy, Z.; Jeelani, S.M.; Lassi, Z.S.; Bhutta, Z.A. Effects of Lifestyle Modification Interventions to Prevent and Manage Child and Adolescent Obesity: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2208. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All 1967–1987 | Birth Cohort | ||||
|---|---|---|---|---|---|
| 1967–1972 | 1973–1977 | 1978–1982 | 1983–1987 | ||
| N = 7005 | N = 1692 | N = 1654 | N = 1693 | N = 1966 | |
| Share of women (%) | |||||
| Outcome | |||||
| Obesity | 19.43 | 28.72 | 21.64 | 18.61 | 10.27 |
| Exposure | |||||
| Child marriage | 18.33 | 9.81 | 26.84 | 24.34 | 13.33 |
| Covariates | |||||
| Education | |||||
| No/primary | 4.40 | 1.83 | 2.06 | 3.13 | 9.66 |
| Secondary | 77.60 | 74.59 | 80.71 | 82.28 | 73.55 |
| Higher | 18.00 | 23.58 | 17.23 | 14.59 | 16.79 |
| Wealth Index Quintiles | |||||
| 1st: Poorest | 18.47 | 18.50 | 20.50 | 19.61 | 15.77 |
| 2nd: Poorer | 16.20 | 13.95 | 15.78 | 16.36 | 18.36 |
| 3rd: Middle | 17.13 | 15.96 | 15.30 | 16.83 | 19.94 |
| 4th: Richer | 18.83 | 19.98 | 17.78 | 18.37 | 19.13 |
| 5th: Richest | 29.36 | 31.62 | 30.65 | 28.82 | 26.81 |
| Employed | 31.72 | 38.89 | 34.70 | 28.88 | 25.48 |
| Parity | |||||
| 2 or less | 21.66 | 13.53 | 13.06 | 17.96 | 39.06 |
| 3 to 4 | 53.06 | 46.34 | 51.69 | 59.78 | 54.22 |
| 5 or more | 25.28 | 40.13 | 35.25 | 22.27 | 6.71 |
| Urban | 36.43 | 38.12 | 38.03 | 36.27 | 33.77 |
| Region | |||||
| Dushanbe | 16.87 | 17.08 | 18.02 | 16.66 | 15.92 |
| Sughd | 24.73 | 24.88 | 23.58 | 26.28 | 24.21 |
| Khalton | 26.47 | 26.77 | 25.94 | 25.99 | 27.06 |
| DRS | 22.91 | 20.33 | 21.89 | 24.22 | 24.87 |
| Gabo | 9.02 | 10.93 | 10.58 | 6.85 | 7.93 |
| Not Adjusted for Sociodemographic Correlates | Adjusted for Sociodemographic Correlates | |||||
|---|---|---|---|---|---|---|
| 2012 Wave | 2017 Wave | Both Waves | 2012 Wave | 2017 Wave | Both Waves | |
| Child marriage | 1.533 *** | 1.666 *** | 1.614 *** | 1.371 * | 1.509 *** | 1.468 *** |
| (1.202, 1.954) | (1.371, 2.024) | (1.393, 1.870) | (1.062, 1.770) | (1.232, 1.850) | (1.259, 1.711) | |
| Birth cohort | ||||||
| 1967–1972 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| 1973–1977 | 0.616 *** | 0.617 *** | 0.612 *** | 0.605 *** | 0.636 *** | 0.618 *** |
| (0.478, 0.793) | (0.497, 0.766) | (0.517, 0.726) | (0.467, 0.785) | (0.509, 0.794) | (0.519, 0.736) | |
| 1978–1982 | 0.405 *** | 0.585 *** | 0.508 *** | 0.394 *** | 0.562 *** | 0.499 *** |
| (0.308, 0.533) | (0.468, 0.730) | (0.429, 0.601) | (0.294, 0.529) | (0.446, 0.710) | (0.419, 0.594) | |
| 1983–1987 | 0.225 *** | 0.299 *** | 0.268 *** | 0.228 *** | 0.273 *** | 0.253 *** |
| (0.165, 0.306) | (0.236, 0.378) | (0.224, 0.320) | (0.160, 0.324) | (0.211, 0.353) | (0.209, 0.306) | |
| Survey wave | ||||||
| 2012 | Ref. | Ref. | ||||
| 2017 | 2.024 *** | 2.069 *** | ||||
| (1.798, 2.278) | (1.828, 2.340) | |||||
| Observations | 3426 | 3579 | 7005 | 3426 | 3579 | 7005 |
| Not Adjusted for Sociodemographic Correlates | Adjusted for Sociodemographic Correlates | |||||
|---|---|---|---|---|---|---|
| 2012 Wave | 2017 Wave | Both Waves | 2012 Wave | 2017 Wave | Both Waves | |
| A. ≥ 1.5 Std. Dev. | ||||||
| Child marriage | 1.736 *** | 1.706 *** | 1.721 *** | 1.491 ** | 1.481 ** | 1.505 *** |
| (1.324, 2.275) | (1.290, 2.256) | (1.409, 2.104) | (1.119, 1.985) | (1.111, 1.975) | (1.225, 1.849) | |
| B. ≥ 2.0 Std. Dev. | ||||||
| Child marriage | 2.318 *** | 2.022 *** | 2.183 *** | 1.982 *** | 1.728 ** | 1.894 *** |
| (1.625, 3.305) | (1.364, 2.997) | (1.685, 2.828) | (1.359, 2.891) | (1.152, 2.593) | (1.449, 2.476) | |
| Observations | 3426 | 3579 | 7005 | 3426 | 3579 | 7005 |
| Birth Cohorts | ||||
|---|---|---|---|---|
| Oldest: 1967–1972 | Older: 1973–1977 | Younger: 1978–1982 | Youngest: 1983–1987 | |
| A. Not adjusted | ||||
| Child marriage | 1.286 | 1.459 ** | 1.746 *** | 2.224 *** |
| (0.904, 1.830) | (1.126, 1.892) | (1.317, 2.315) | (1.532, 3.229) | |
| Survey wave | ||||
| 2012 | Ref. | Ref. | Ref. | Ref. |
| 2017 | 1.741 *** | 1.782 *** | 2.583 *** | 2.386 *** |
| (1.396, 2.171) | (1.396, 2.274) | (1.973, 3.381) | (1.753, 3.248) | |
| Observations | 1692 | 1654 | 1693 | 1966 |
| B. Adjusted | ||||
| Child marriage | 1.226 | 1.265 | 1.579 ** | 1.707 ** |
| (0.841, 1.787) | (0.955, 1.676) | (1.168, 2.135) | (1.138, 2.560) | |
| Survey wave | ||||
| 2012 | Ref. | Ref. | Ref. | Ref. |
| 2017 | 1.752 *** | 1.879 *** | 2.815 *** | 2.211 *** |
| (1.391, 2.206) | (1.454, 2.427) | (2.129, 3.720) | (1.579, 3.098) | |
| Observations | 1692 | 1654 | 1693 | 1966 |
| Birth Cohorts | ||||
|---|---|---|---|---|
| Oldest: 1967–1972 | Older: 1973–1977 | Younger: 1978–1982 | Youngest: 1983–1987 | |
| A. Not adjusted | ||||
| i. ≥ 1.5 Std. Dev. | ||||
| Child marriage | 1.635 | 1.804 ** | 1.528 * | 1.935 *** |
| (0.960, 2.785) | (1.245, 2.615) | (1.073, 2.175) | (1.326, 2.823) | |
| ii. ≥ 2.0 Std. Dev. | ||||
| Child marriage | 2.163 * | 2.838 *** | 1.282 | 2.839 *** |
| (1.080, 4.331) | (1.701, 4.736) | (0.749, 2.195) | (1.761, 4.578) | |
| B. Adjusted | ||||
| i. ≥ 1.5 Std. Dev. | ||||
| Child marriage | 1.461 | 1.723 ** | 1.219 | 1.500 |
| (0.835, 2.556) | (1.169, 2.538) | (0.817, 1.819) | (0.990, 2.271) | |
| ii. ≥ 2.0 Std. Dev. | ||||
| Child marriage | 1.911 | 2.482 ** | 1.084 | 2.073 ** |
| (0.987, 3.699) | (1.427, 4.319) | (0.614, 1.914) | (1.219, 3.526) | |
| Observations | 1692 | 1654 | 1693 | 1966 |
| All: 1967–1987 | Birth Cohorts | ||||
|---|---|---|---|---|---|
| Oldest: 1967–1972 | Older: 1973–1977 | Younger: 1978–1982 | Youngest: 1983–1987 | ||
| A. Employed | |||||
| Total Effect | 0.395 *** | 0.216 | 0.234 | 0.470 ** | 0.595 ** |
| (0.243, 0.547) | (−0.160, 0.592) | (−0.043, 0.510) | (0.181, 0.760) | (0.202, 0.989) | |
| Direct Effect | 0.399 *** | 0.212 | 0.242 | 0.472 ** | 0.602 ** |
| (0.247, 0.551) | (−0.164, 0.588) | (−0.035, 0.520) | (0.183, 0.762) | (0.207, 0.998) | |
| Indirect Effect | −0.003 | 0.004 | −0.009 | −0.002 | −0.007 |
| (−0.009, 0.002) | (−0.008, 0.016) | (−0.024, 0.007) | (−0.020, 0.016) | (−0.027, 0.013) | |
| B. Parity ≥ 5 | |||||
| Total Effect | 0.397 *** | 0.218 | 0.232 | 0.473 ** | 0.589 ** |
| (0.245, 0.549) | (−0.157, 0.593) | (−0.044, 0.509) | (0.185, 0.761) | (0.195, 0.983) | |
| Direct Effect | 0.378 *** | 0.212 | 0.230 | 0.445 ** | 0.543 ** |
| (0.225, 0.531) | (−0.164, 0.587) | (−0.047, 0.508) | (0.145, 0.744) | (0.141, 0.946) | |
| Indirect Effect | 0.019 * | 0.006 | 0.002 | 0.028 | 0.046 |
| (0.001, 0.037) | (−0.012, 0.024) | (−0.022, 0.026) | (−0.031, 0.087) | (−0.023, 0.115) | |
| C. Employed and Parity ≥ 5 | |||||
| Total Effect | 0.397 *** | 0.218 | 0.234 | 0.472 ** | 0.591 ** |
| (0.245, 0.549) | (−0.158, 0.594) | (−0.043, 0.511) | (0.182, 0.761) | (0.196, 0.985) | |
| Direct Effect | 0.382 *** | 0.208 | 0.241 | 0.453 ** | 0.552 ** |
| (0.229, 0.536) | (−0.169, 0.585) | (−0.038, 0.520) | (0.152, 0.753) | (0.146, 0.958) | |
| Indirect Effect | 0.014 | 0.010 | −0.007 | 0.019 | 0.039 |
| (−0.005, 0.034) | (−0.011, 0.031) | (−0.038, 0.024) | (−0.043, 0.081) | (−0.036, 0.113) | |
| Spousal Age Difference | ||||||
|---|---|---|---|---|---|---|
| All | 0–2 | 3–5 | 6–9 | 10+ | <0 | |
| Child mariage | 1.416 *** | 1.454 * | 1.307 * | 1.551 * | 1.400 | 6.679 |
| (1.202, 1.668) | (1.007, 2.099) | (1.002, 1.706) | (1.108, 2.171) | (0.725, 2.705) | (0.172, 259.234) | |
| Observations | 6437 | 2271 | 2454 | 1132 | 387 | 193 |
| Q25 | Q50 | Q75 | Q90 | |
|---|---|---|---|---|
| A. Not adjusted | ||||
| Child marriage | 0.975 *** | 1.070 *** | 1.490 *** | 2.020 *** |
| (0.616, 1.334) | (0.737, 1.403) | (0.976, 2.004) | (1.284, 2.756) | |
| Birth cohort | ||||
| 1967–1972 | Ref. | Ref. | Ref. | Ref. |
| 1973–1977 | −1.185 *** | −1.090 *** | −1.550 *** | −1.520 *** |
| (−1.551, −0.819) | (−1.491, −0.689) | (−2.073, −1.027) | (−2.256, −0.784) | |
| 1978–1982 | −1.400 *** | −1.920 *** | −2.230 *** | −2.740 *** |
| (−1.739, −1.061) | (−2.332, −1.508) | (−2.781, −1.679) | (−3.492, −1.988) | |
| 1983–1987 | −2.830 *** | −3.650 *** | −4.470 *** | −4.800 *** |
| (−3.137, −2.523) | (−4.027, −3.273) | (−4.981, −3.959) | (−5.499, −4.101) | |
| Survey wave | ||||
| 2012 | Ref. | Ref. | Ref. | Ref. |
| 2017 | 1.565 *** | 1.890 *** | 2.250 *** | 2.640 *** |
| (1.324, 1.806) | (1.629, 2.151) | (1.886, 2.614) | (2.118, 3.162) | |
| B. Adjusted | ||||
| Child marriage | 0.614 ** | 0.787 *** | 1.108 *** | 1.519 *** |
| (0.227, 1.000) | (0.426, 1.148) | (0.598, 1.618) | (0.756, 2.282) | |
| Birth cohort | ||||
| 1967–1972 | Ref. | Ref. | Ref. | Ref. |
| 1973–1977 | −0.928 *** | −1.094 *** | −1.423 *** | −1.496 *** |
| (−1.378, −0.477) | (−1.524, −0.664) | (−1.987, −0.860) | (−2.273, −0.719) | |
| 1978–1982 | −1.423 *** | −1.781 *** | −2.158 *** | −2.465 *** |
| (−1.842, −1.004) | (−2.204, −1.358) | (−2.766, −1.550) | (−3.228, −1.702) | |
| 1983–1987 | −2.798 *** | −3.509 *** | −4.251 *** | −4.612 *** |
| (−3.204, −2.391) | (−3.924, −3.095) | (−4.839, −3.663) | (−5.391, −3.833) | |
| Survey wave | ||||
| 2012 | Ref. | Ref. | Ref. | Ref. |
| 2017 | 1.505 *** | 1.861 *** | 2.313 *** | 2.566 *** |
| (1.241, 1.770) | (1.598, 2.125) | (1.929, 2.697) | (2.045, 3.086) |
| Q25 | Q50 | Q75 | Q90 | |
|---|---|---|---|---|
| A. Not adjusted | ||||
| I. 1967–1972 | ||||
| Child marriage | 0.800 | 0.910 | 1.170 | 1.690 |
| (−0.172, 1.772) | (−0.027, 1.847) | (−0.337, 2.677) | (−0.503, 3.883) | |
| II. 1967–1972 | ||||
| Child marriage | 0.630 | 0.910 ** | 1.510 ** | 2.110 ** |
| (−0.050, 1.310) | (0.302, 1.518) | (0.510, 2.510) | (0.539, 3.681) | |
| III. 1978–1982 | ||||
| Child marriage | 1.350 *** | 1.170 *** | 1.480 ** | 1.700 ** |
| (0.712, 1.988) | (0.530, 1.810) | (0.453, 2.507) | (0.463, 2.937) | |
| IV. 1983–1987 | ||||
| Child marriage | 0.930 ** | 1.350 *** | 1.720 *** | 2.810 ** |
| (0.274, 1.586) | (0.598, 2.102) | (0.728, 2.712) | (1.035, 4.585) | |
| B. Adjusted | ||||
| I. 1967–1972 | ||||
| Child marriage | 0.355 | 0.210 | 0.720 | 2.183 |
| (−0.562, 1.272) | (−0.801, 1.221) | (−0.954, 2.394) | (−0.102, 4.469) | |
| II. 1967–1972 | ||||
| Child marriage | 0.781 * | 0.537 | 0.840 | 2.053 * |
| (0.030, 1.532) | (−0.150, 1.224) | (−0.107, 1.787) | (0.432, 3.674) | |
| III. 1978–1982 | ||||
| Child marriage | 1.198 *** | 0.927 ** | 1.126 * | −0.063 |
| (0.529, 1.867) | (0.223, 1.630) | (0.162, 2.090) | (−1.236, 1.110) | |
| IV. 1983–1987 | ||||
| Child marriage | 0.440 | 0.757 * | 1.391 * | 1.770 * |
| (−0.385, 1.265) | (0.066, 1.448) | (0.287, 2.495) | (0.126, 3.414) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Datta, B.; Tiwari, A.; Attari, S. Child Marriage and Later-Life Risk of Obesity in Women: A Cohort Analysis Using Nationally Representative Repeated Cross-Sectional Data from Tajikistan. Women 2023, 3, 53-70. https://doi.org/10.3390/women3010004
Datta B, Tiwari A, Attari S. Child Marriage and Later-Life Risk of Obesity in Women: A Cohort Analysis Using Nationally Representative Repeated Cross-Sectional Data from Tajikistan. Women. 2023; 3(1):53-70. https://doi.org/10.3390/women3010004
Chicago/Turabian StyleDatta, Biplab, Ashwini Tiwari, and Sara Attari. 2023. "Child Marriage and Later-Life Risk of Obesity in Women: A Cohort Analysis Using Nationally Representative Repeated Cross-Sectional Data from Tajikistan" Women 3, no. 1: 53-70. https://doi.org/10.3390/women3010004
APA StyleDatta, B., Tiwari, A., & Attari, S. (2023). Child Marriage and Later-Life Risk of Obesity in Women: A Cohort Analysis Using Nationally Representative Repeated Cross-Sectional Data from Tajikistan. Women, 3(1), 53-70. https://doi.org/10.3390/women3010004