
Differentials in Maternal Mortality Pattern in Sub-Saharan Africa Countries: Evidence from Demographic and Health Survey Data

 , , , , and
, , , , and
Abstract
1. Background
2. Methods
Data Source
3. Selection and Measurement of Variables
3.1. Outcome
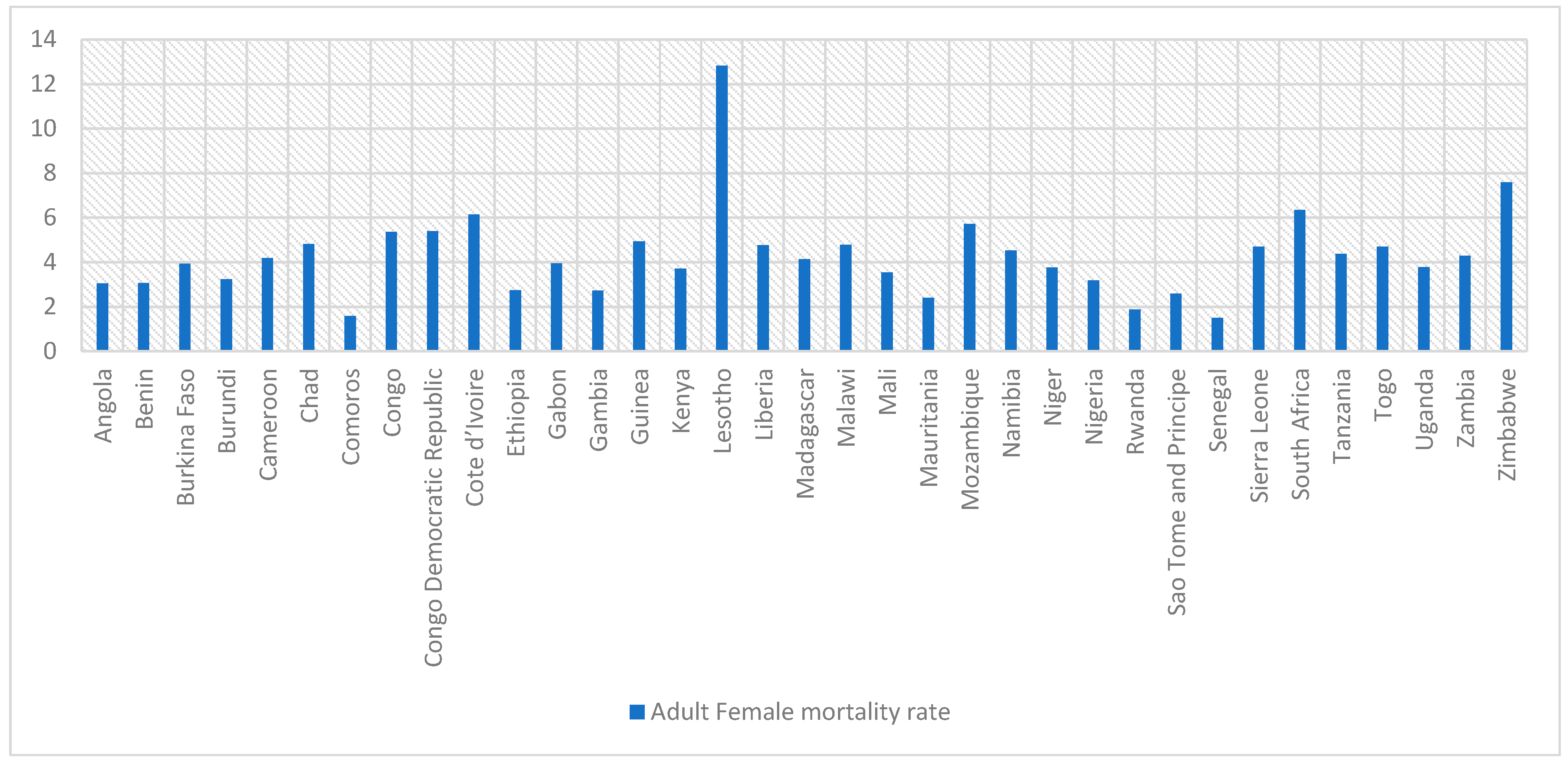
- Adult female mortality rate: the adult female mortality rate over the seven-year period prior to the survey, expressed as a percentage of 1000 women-years of exposure.
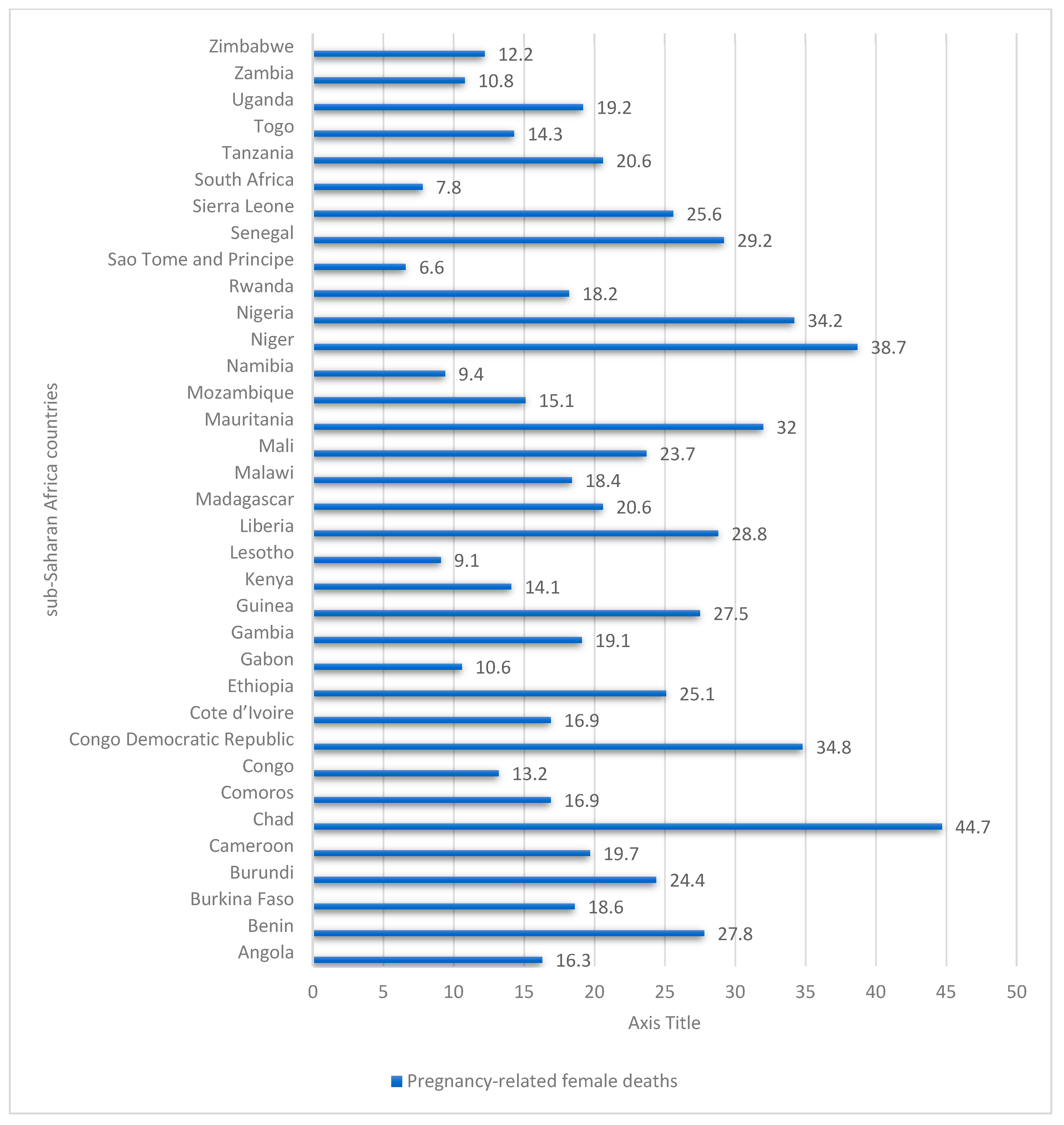
- Female deaths that are pregnancy-related: the percentage of all female adult deaths that are pregnancy-related, including those from accidents or violence during pregnancy, delivery, and the two months following delivery.
- Pregnancy-related mortality rate: this is expressed as the number of deaths from pregnancy in the seven years prior to the survey, per 1000 woman-years of exposure.
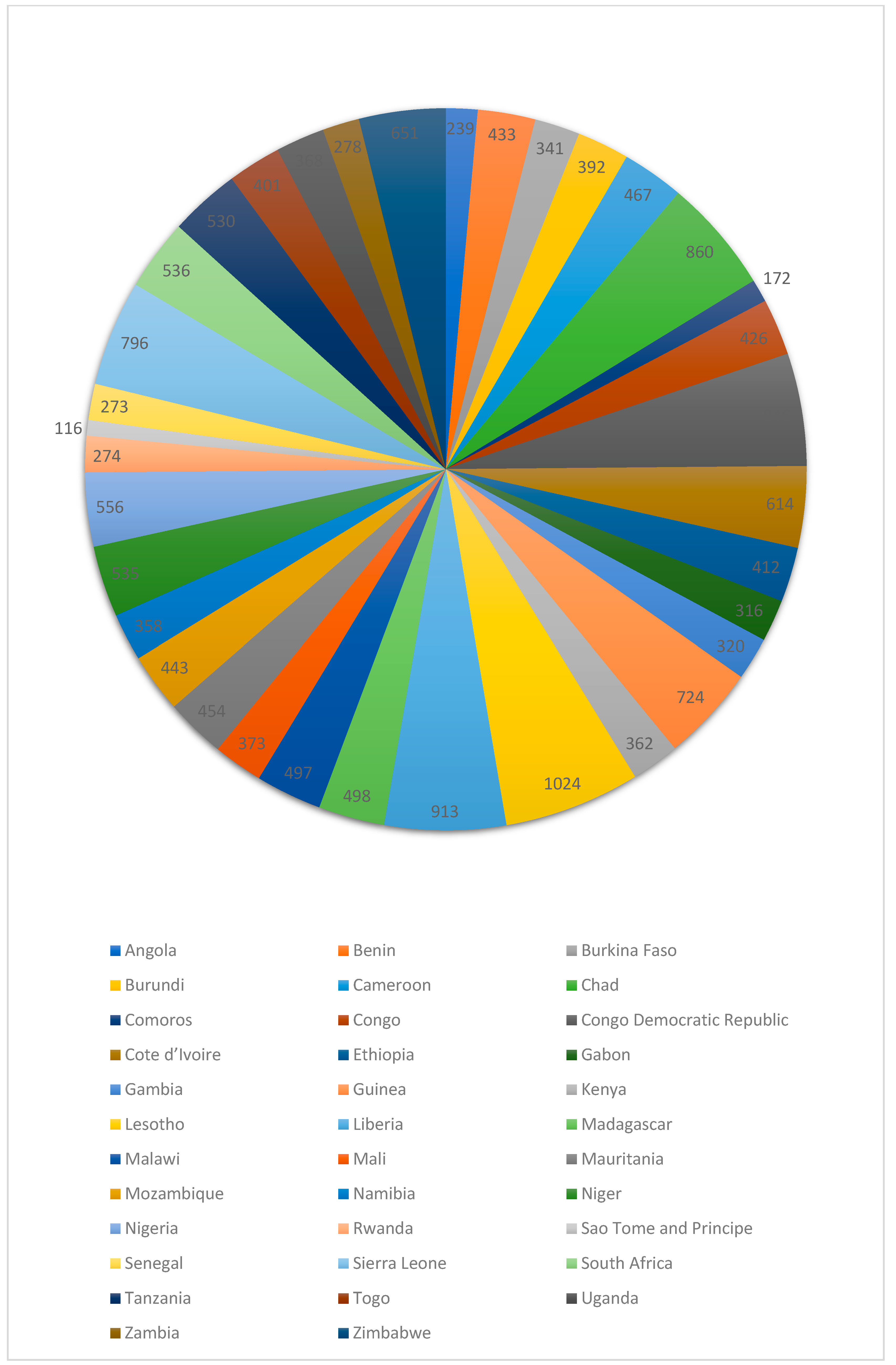
- Pregnancy-related mortality ratio: the pregnancy-related mortality ratio is calculated as the age-adjusted pregnancy-related mortality rate multiplied by 100 divided by the age-adjusted general fertility rate, and it is expressed as the number of pregnancies lost during the seven years prior to the survey per 100,000 live births.
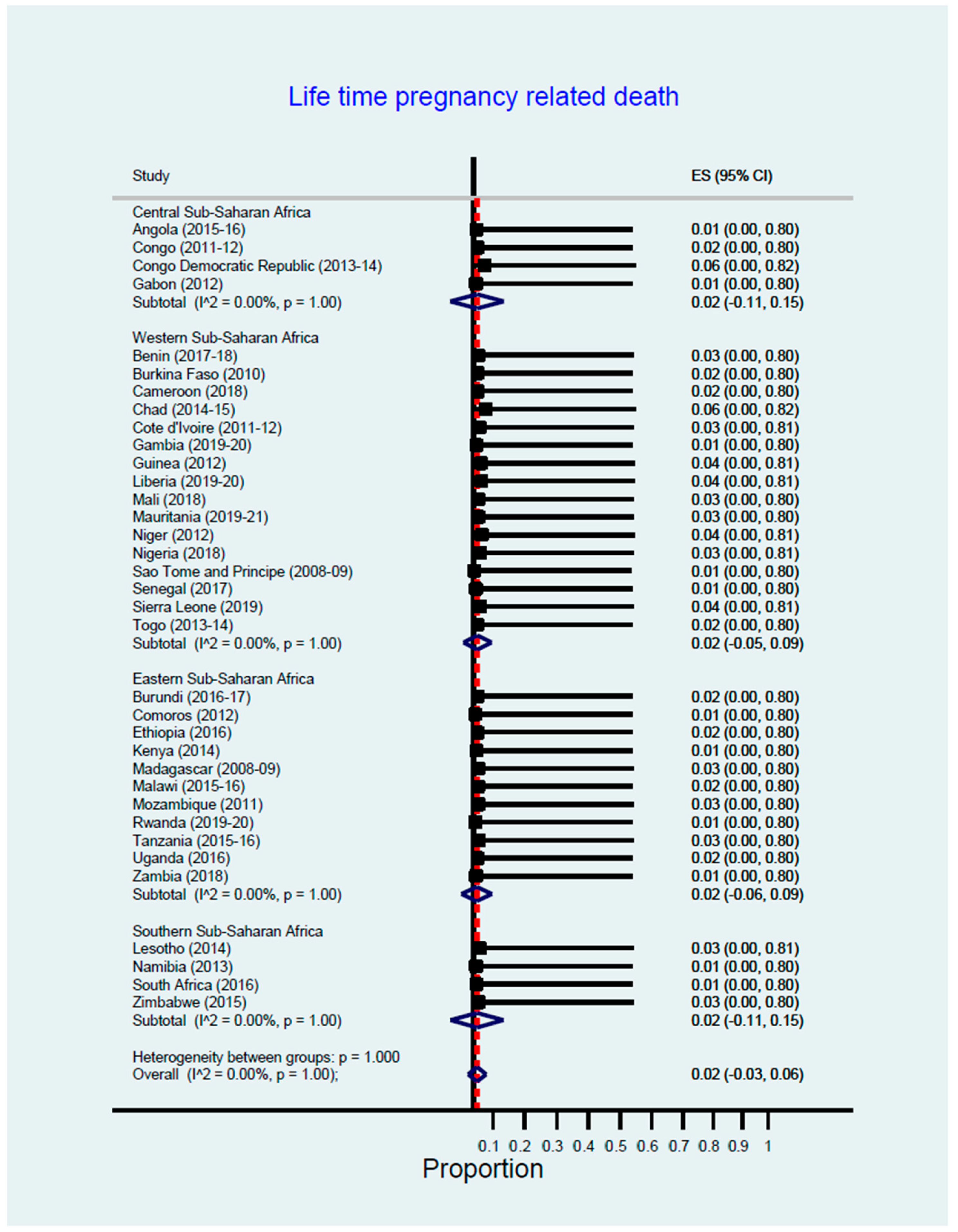
- Lifetime risk of pregnancy-related death: calculated as 1-(1-PRMR) TFR, where TFR is the total fertility rate for the seven years prior to the survey, is the lifetime risk of pregnancy-related death.
3.2. Explanatory Variable
3.3. Analytical Approach
3.4. Ethical Approval and Informed Consent
4. Results
5. Discussion
6. Strength and Limitation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maternal Mortality. Available online: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (accessed on 2 December 2022).
- UNICEF DATA. Maternal Mortality Rates and Statistics. Available online: https://data.unicef.org/topic/maternal-health/maternal-mortality/ (accessed on 2 December 2022).
- Merdad, L.; Ali, M.M. Timing of maternal death: Levels, trends, and ecological correlates using sibling data from 34 sub-Saharan African countries. PLoS ONE 2018, 13, e0189416. [Google Scholar] [CrossRef] [PubMed]
- Onambele, L.; Ortega-Leon, W.; Guillen-Aguinaga, S.; Forjaz, M.J.; Yoseph, A.; Guillen-Aguinaga, L.; Alas-Brun, R.; Arnedo-Pena, A.; Aguinaga-Ontoso, I.; Guillen-Grima, F. Maternal Mortality in Africa: Regional Trends (2000–2017). Int. J. Environ. Res. Public Health 2022, 19, 13146. [Google Scholar] [CrossRef] [PubMed]
- Musarandega, R.; Nyakura, M.; Machekano, R.; Pattinson, R.; Munjanja, S.P. Causes of maternal mortality in Sub-Saharan Africa: A systematic review of studies published from 2015 to 2020. J. Glob. Health 2021, 11, 04048. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Maternal Mortality Collaborators. Global, regional, and national levels of maternal mortality, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Lond. Engl. 2016, 388, 1775–1812. [Google Scholar] [CrossRef]
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.-B.; Daniels, J.; Gülmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob. Health 2014, 2, E323–E333. [Google Scholar] [CrossRef] [PubMed]
- Institutional Maternal and Perinatal Deaths: A Review of 40 Low and Middle Income Countries—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/28882128/ (accessed on 2 December 2022).
- Neal, S.; Mahendra, S.; Bose, K.; Camacho, A.V.; Mathai, M.; Nove, A.; Santana, F.; Matthews, Z. The causes of maternal mortality in adolescents in low and middle income countries: A systematic review of the literature. BMC Pregnancy Childbirth 2016, 16, 352. [Google Scholar] [CrossRef]
- Kumar, S.; Kumar, N.; Vivekadhish, S. Millennium development goals (MDGS) to sustainable development goals (SDGS): Addressing unfinished agenda and strengthening sustainable development and partnership. Indian J. Community Med. 2016, 41, 1. [Google Scholar] [CrossRef] [PubMed]
- Demographic and Health Surveys (DHS) Data. Available online: http://api.dhsprogram.com/rest/dhs/indicators?f=html (accessed on 5 January 2023).
- Owobi, O.U.; Okonji, O.C.; Nzoputam, C.I.; Ekholuenetale, M. Country-Level Variations in Overweight and Obesity among Reproductive-Aged Women in Sub-Saharan Countries. Women 2022, 2, 313–325. [Google Scholar] [CrossRef]
- Ekholuenetale, M.; Nzoputam, C.I.; Okonji, O.C. Sub-Regional Variations in Sexually Transmitted Infections Manifesting as Vaginitis among Reproductive-Aged Women in Sub-Saharan Countries. Venereology 2022, 1, 245–261. [Google Scholar] [CrossRef]
- Corsi, D.J.; Neuman, M.; Finlay, J.E.; Subramanian, S.V. Demographic and health surveys: A profile. Int. J. Epidemiol. 2012, 41, 1602–1613 . [Google Scholar] [CrossRef]
- Global Citizen. Why Maternal Mortality Is So High in Sub-Saharan Africa. In Global Citizen [Internet]. 2022. Available online: https://www.globalcitizen.org/en/content/maternal-mortality-sub-saharan-africa-causes/ (accessed on 5 January 2023).
- Okonofua, F.E.; Abejide, A.; Makanjuola, R.A. Maternal mortality in Ile-Ife, Nigeria: A study of risk factors. Stud. Fam. Plan. 1992, 23, 319–324. [Google Scholar] [CrossRef]
- Alkema, L.; Chou, D.; Hogan, D.; Zhang, S.; Moller, A.B.; Gemmill, A.; Fat, D.M.; Boerma, T.; Temmerman, M.; Mathers, C.; et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: A systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet 2016, 387, 462–474. [Google Scholar] [CrossRef] [PubMed]
- Diguisto, C.; Saucedo, M.; Kallianidis, A.; Bloemenkamp, K.; Bødker, B.; Buoncristiano, M.; Donati, S.; Gissler, M.; Johansen, M.; Knight, M.; et al. Maternal mortality in eight European countries with enhanced surveillance systems: Descriptive population based study. BMJ 2022, 379, e070621. [Google Scholar] [CrossRef] [PubMed]
- Abouchadi, S.; Zhang, W.-H.; De Brouwere, V. Underreporting of deaths in the maternal deaths surveillance system in one region of Morocco. PLoS ONE 2018, 13, e0188070. [Google Scholar] [CrossRef] [PubMed]
- Said, A.; Malqvist, M.; Pembe, A.B.; Massawe, S.; Hanson, C. Causes of maternal deaths and delays in care: Comparison between routine maternal death surveillance and response system and an obstetrician expert panel in Tanzania. BMC Health Serv. Res. 2020, 20, 614. [Google Scholar] [CrossRef] [PubMed]
- Horon, I.L. Underreporting of Maternal Deaths on Death Certificates and the Magnitude of the Problem of Maternal Mortality. Am. J. Public Health 2005, 95, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, J.L.; Gil, R.; Hernández, V.; Gil, A. Factors associated with maternal mortality in Sub-Saharan Africa: An ecological study. BMC Public Health 2009, 9, 462. [Google Scholar] [CrossRef] [PubMed]
- Filippi, V.; Chou, D.; Ronsmans, C.; Graham, W.; Say, L. Levels and Causes of Maternal Mortality and Morbidity. In Disease Control Priorities, 3rd ed.; Reproductive, Maternal, Newborn, and Child Health; The World Bank: Washington, DC, USA, 2016; Volume 2, pp. 51–70. [Google Scholar] [CrossRef]
- Batist, J. An intersectional analysis of maternal mortality in Sub-Saharan Africa: A human rights issue. J. Glob. Health 2019, 9, 010320. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Survey Year | Total Sample Size | Adult Female Mortality Rate | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 15–19 | 20–24 | 25–29 | 30–34 | 35–39 | 40–44 | 45–49 | Total | |||
| Angola | 2015–2016 | 14,379 | 1.99 | 2.48 | 2.86 | 3.87 | 4.13 | 5.63 | 2.41 | 3.04 |
| Benin | 2017–2018 | 15,928 | 2.45 | 2.23 | 2.32 | 4.02 | 3.82 | 3.9 | 4.71 | 3.06 |
| Burkina Faso | 2010 | 17,087 | 2.03 | 2.44 | 3.67 | 3.94 | 5.74 | 6.25 | 7.53 | 3.93 |
| Burundi | 2016–2017 | 17,269 | 1.92 | 1.77 | 2.46 | 3.27 | 4.25 | 6.54 | 7.4 | 3.24 |
| Cameroon | 2018 | 14,677 | 2.53 | 2.96 | 3.54 | 5.66 | 5.38 | 6.75 | 6.89 | 4.18 |
| Chad | 2014–2015 | 17,719 | 3.56 | 4.08 | 4.67 | 5.86 | 5.45 | 6.79 | 5.22 | 4.81 |
| Comoros | 2012 | 5329 | 0.53 | 1.09 | 1.43 | 2.08 | 2.08 | 3.72 | 2.68 | 1.58 |
| Congo | 2011–2012 | 10,819 | 2.22 | 3.07 | 4.44 | 7.05 | 6.6 | 11.36 | 10.2 | 5.36 |
| Congo Democratic Republic | 2013–2014 | 18,827 | 4.08 | 4.53 | 4.88 | 5.33 | 7.87 | 7.3 | 7.23 | 5.4 |
| Cote d’Ivoire | 2011–2012 | 10,060 | 2.86 | 3.75 | 4.13 | 8.62 | 8.87 | 11.87 | 11.46 | 6.15 |
| Ethiopia | 2016 | 15,683 | 2.22 | 2.23 | 2.32 | 3.68 | 2.2 | 3.85 | 4.57 | 2.74 |
| Gabon | 2012 | 8422 | 2.14 | 2.05 | 4.87 | 4.23 | 5.05 | 5.18 | 8.43 | 3.94 |
| Gambia | 2019–2020 | 11,865 | 0.93 | 1.55 | 2.24 | 3.27 | 3.57 | 6.27 | 6.25 | 2.72 |
| Guinea | 2012 | 9142 | 3.86 | 3.68 | 3.92 | 5.01 | 6.98 | 5.36 | 9.25 | 4.93 |
| Kenya | 2014 | 31,079 | 1.67 | 2.1 | 2.66 | 4.73 | 6.78 | 6.83 | 5 | 3.72 |
| Lesotho | 2014 | 6621 | 2.29 | 5.57 | 10.93 | 17.84 | 19.12 | 28.21 | 30.29 | 12.82 |
| Liberia | 2019–2020 | 8065 | 2.53 | 3.36 | 4.25 | 5.01 | 6 | 7.44 | 9.4 | 4.76 |
| Madagascar | 2008–2009 | 17,375 | 3.23 | 3.28 | 3.24 | 4.32 | 3.7 | 6.59 | 7.38 | 4.14 |
| Malawi | 2015–2016 | 24,562 | 1.7 | 3.29 | 4.38 | 5.62 | 6.56 | 9.41 | 9.66 | 4.77 |
| Mali | 2018 | 10,519 | 2.34 | 2.89 | 2.52 | 3.37 | 4.17 | 7.26 | 6.51 | 3.54 |
| Mauritania | 2019–2021 | 15,714 | 0.99 | 1.45 | 2.15 | 2.75 | 3.73 | 5.93 | 2.32 | 2.4 |
| Mozambique | 2011 | 13,745 | 2.38 | 4.78 | 6.4 | 7.07 | 7.45 | 5.44 | 10.71 | 5.71 |
| Namibia | 2013 | 10,018 | 1.56 | 2.29 | 4.71 | 6.74 | 7.71 | 6.47 | 6.44 | 4.53 |
| Niger | 2012 | 11,160 | 3.23 | 4.21 | 2.92 | 4.41 | 2.92 | 5.31 | 4.32 | 3.76 |
| Nigeria | 2018 | 41,821 | 1.59 | 2.39 | 2.52 | 3.25 | 4.01 | 5.35 | 5.86 | 3.18 |
| Rwanda | 2019–2020 | 14,634 | 0.82 | 1.21 | 1.32 | 2.09 | 2.51 | 2.36 | 5.06 | 1.88 |
| Sao Tome and Principe | 2008–2009 | 2615 | 1.18 | 2.1 | 1.51 | 2.65 | 3.21 | 4.32 | 6.45 | 2.59 |
| Senegal | 2017 | 16,787 | 0.79 | 0.89 | 1.06 | 2.12 | 1.98 | 2.85 | 2.45 | 1.5 |
| Sierra Leone | 2019 | 15,574 | 2.81 | 3.48 | 3.95 | 4.85 | 6.15 | 7.22 | 8.36 | 4.69 |
| South Africa | 2016 | 8514 | 1.02 | 3.65 | 4.48 | 9.82 | 9.13 | 11.39 | 8.32 | 6.34 |
| Tanzania | 2015–2016 | 13,266 | 1.27 | 2.32 | 2.78 | 4.67 | 6.35 | 9.67 | 10.82 | 4.37 |
| Togo | 2013–2014 | 9480 | 2.21 | 3.18 | 3.8 | 4.98 | 4.92 | 8.81 | 9.4 | 4.69 |
| Uganda | 2016 | 18,506 | 2.26 | 2.48 | 3.25 | 4.79 | 5 | 6.16 | 7.2 | 3.78 |
| Zambia | 2018 | 13,683 | 1.25 | 3.22 | 3.31 | 6.16 | 5.02 | 8.36 | 9.13 | 4.29 |
| Zimbabwe | 2015 | 9955 | 1.88 | 2.49 | 5.02 | 10.75 | 13.64 | 15.23 | 17.1 | 7.59 |
| Country | Female Deaths That Are Pregnancy-Related | |||||||
|---|---|---|---|---|---|---|---|---|
| 15–19 | 20–24 | 25–29 | 30–34 | 35–39 | 40–44 | 45–49 | Total | |
| Angola | 16.5 | 21.2 | 13.8 | 12.7 | 23.5 | 10.3 | 14.1 | 16.3 |
| Benin | 18.1 | 35 | 32.9 | 35.2 | 24.7 | 20.9 | 14.1 | 27.8 |
| Burkina Faso | 14.3 | 29 | 19.3 | 21 | 18.2 | 11.4 | 9 | 18.6 |
| Burundi | 8 | 23.8 | 41.6 | 36.6 | 27.1 | 17.2 | 1.1 | 24.4 |
| Cameroon | 16 | 25.1 | 19.3 | 27 | 15.5 | 18.6 | 2.4 | 19.7 |
| Chad | 50.8 | 45.4 | 55.2 | 45.2 | 37.1 | 32 | 15.2 | 44.7 |
| Comoros | 0 | 0 | 45.6 | 26.6 | 18.7 | 1 | 0 | 16.9 |
| Congo | 19.6 | 17.5 | 11.8 | 15.7 | 19.6 | 2.6 | 7.6 | 13.2 |
| Congo Democratic Republic | 29.2 | 45.7 | 38.6 | 30.1 | 35.8 | 34.9 | 11.4 | 34.8 |
| Cote d’Ivoire | 14.8 | 21.9 | 22.7 | 13.1 | 22 | 10 | 11.8 | 16.9 |
| Ethiopia | 17.4 | 28.7 | 29.3 | 30 | 24.4 | 20.3 | 13.7 | 25.1 |
| Gabon | 33.8 | 10.2 | 9.3 | 4.1 | 11.9 | 7 | 1.9 | 10.6 |
| Gambia | 8.6 | 21 | 26.5 | 27.1 | 19.2 | 15.4 | 0 | 19.1 |
| Guinea | 30.1 | 35.3 | 31.3 | 30.4 | 25.4 | 15.4 | 7.5 | 27.5 |
| Kenya | 6.8 | 21.8 | 27.4 | 13.7 | 12.8 | 7.3 | 4.5 | 14.1 |
| Lesotho | 25 | 14.4 | 15.5 | 6.2 | 10.9 | 0.5 | 4.3 | 9.1 |
| Liberia | 27.1 | 58.8 | 23.6 | 27.6 | 31.6 | 20.5 | 7.8 | 28.8 |
| Madagascar | 25.8 | 22.3 | 27.4 | 21.3 | 25.8 | 11 | 6.6 | 20.6 |
| Malawi | 16.2 | 21.2 | 26.4 | 23.6 | 15.8 | 9.8 | 2.6 | 18.4 |
| Mali | 16.6 | 23.5 | 28 | 28.6 | 33.7 | 18.4 | 6 | 23.7 |
| Mauritania | 27 | 23.1 | 39.3 | 26 | 45.7 | 23.9 | 38.3 | 32 |
| Mozambique | 24.2 | 21.7 | 17.5 | 9 | 13.4 | 8.5 | 8.8 | 15.1 |
| Namibia | 11.9 | 11.9 | 8.8 | 9.6 | 13.8 | 0.8 | 5.5 | 9.4 |
| Niger | 34.4 | 41.7 | 45.4 | 42.9 | 46.5 | 23.4 | 15.1 | 38.7 |
| Nigeria | 40.8 | 42.7 | 43.5 | 41.2 | 33 | 14.8 | 11.8 | 34.2 |
| Rwanda | 5.5 | 6.7 | 16.2 | 22.7 | 22.7 | 29 | 15.2 | 18.2 |
| Sao Tome and Principe | 0 | 0 | 7.1 | 12.9 | 3.3 | 20.6 | 0 | 6.6 |
| Senegal | 16.4 | 34.4 | 35.2 | 35.6 | 32.3 | 22.7 | 11.5 | 29.2 |
| Sierra Leone | 22.6 | 28.2 | 28.5 | 30.8 | 31.2 | 17.6 | 7.7 | 25.6 |
| South Africa | 0 | 9.8 | 13 | 4.7 | 8.3 | 10.7 | 1.3 | 7.8 |
| Tanzania | 21.9 | 28.8 | 35.2 | 12.8 | 19.8 | 21.3 | 10.4 | 20.6 |
| Togo | 17.8 | 25.1 | 20.5 | 11.1 | 14.4 | 9.1 | 1.3 | 14.3 |
| Uganda | 18.3 | 28.2 | 23.4 | 20 | 15.1 | 19.2 | 2.3 | 19.2 |
| Zambia | 3.5 | 19.9 | 17.2 | 10.3 | 5.4 | 3.8 | 11.2 | 10.8 |
| Zimbabwe | 20.2 | 31 | 16.2 | 10.7 | 9.7 | 10.6 | 4.5 | 12.2 |
| Pregnancy-Related Mortality Rate | Pregnancy-Related Mortality Ratio | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 15–19 | 20–24 | 25–29 | 30–34 | 35–39 | 40–44 | 45–49 | Total | ||
| Angola | 0.33 | 0.53 | 0.39 | 0.49 | 0.97 | 0.58 | 0.34 | 0.49 | 239 (CI: 164–313) |
| Benin | 0.44 | 0.78 | 0.76 | 1.42 | 0.94 | 0.81 | 0.66 | 0.81 | 433 (CI: 339–527) |
| Burkina Faso | 0.29 | 0.71 | 0.71 | 0.83 | 1.05 | 0.71 | 0.68 | 0.68 | 341 (CI: 275–406) |
| Burundi | 0.15 | 0.42 | 1.02 | 1.2 | 1.15 | 1.13 | 0.08 | 0.7 | 392 (CI: 312–472) |
| Cameroon | 0.4 | 0.74 | 0.68 | 1.53 | 0.83 | 1.25 | 0.16 | 0.78 | 467 (CI: 360–573) |
| Chad | 1.81 | 1.85 | 2.58 | 2.65 | 2.02 | 2.17 | 0.8 | 2.06 | 860 (CI: 728–993) |
| Comoros | 0 | 0 | 0.65 | 0.55 | 0.39 | 0.04 | 0 | 0.24 | 172 (CI: 60–284) |
| Congo | 0.44 | 0.54 | 0.52 | 1.11 | 1.29 | 0.29 | 0.78 | 0.69 | 426 (CI: 274–579) |
| Congo Democratic Republic | 1.19 | 2.07 | 1.88 | 1.61 | 2.82 | 2.55 | 0.82 | 1.83 | 846 (CI: 690–1003) |
| Cote d’Ivoire | 0.42 | 0.82 | 0.94 | 1.13 | 1.95 | 1.19 | 1.36 | 1 | 614 (CI: 445–783) |
| Ethiopia | 0.39 | 0.64 | 0.68 | 1.1 | 0.54 | 0.78 | 0.62 | 0.66 | 412 (CI: 273–551) |
| Gabon | 0.72 | 0.21 | 0.45 | 0.17 | 0.6 | 0.36 | 0.16 | 0.41 | 316 (CI: 178–454) |
| Gambia | 0.08 | 0.33 | 0.59 | 0.89 | 0.68 | 0.97 | 0 | 0.48 | 320 (CI: 231–409) |
| Guinea | 1.16 | 1.3 | 1.23 | 1.52 | 1.77 | 0.82 | 0.69 | 1.25 | 724 (CI: 531–916) |
| Kenya | 0.11 | 0.46 | 0.73 | 0.65 | 0.87 | 0.5 | 0.22 | 0.51 | 362 (CI: 254–471) |
| Lesotho | 0.57 | 0.8 | 1.7 | 1.11 | 2.09 | 0.15 | 1.31 | 1.07 | 1024 (CI: 731–1318) |
| Liberia | 0.69 | 1.98 | 1.01 | 1.38 | 1.89 | 1.52 | 0.74 | 1.31 | 913 (CI: 638–1189) |
| Madagascar | 0.83 | 0.73 | 0.89 | 0.92 | 0.96 | 0.72 | 0.49 | 0.81 | 498 (CI: 402–594) |
| Malawi | 0.28 | 0.7 | 1.16 | 1.33 | 1.03 | 0.92 | 0.25 | 0.8 | 497 (CI: 400–593) |
| Mali | 0.39 | 0.68 | 0.71 | 0.97 | 1.41 | 1.34 | 0.39 | 0.8 | 373 (CI: 288–458) |
| Mauritania | 0.27 | 0.34 | 0.84 | 0.72 | 1.71 | 1.41 | 0.89 | 0.76 | 454 (CI: 333–575) |
| Mozambique | 0.58 | 1.04 | 1.12 | 0.64 | 1 | 0.46 | 0.95 | 0.83 | 443 (CI: 328–559) |
| Namibia | 0.19 | 0.27 | 0.41 | 0.65 | 1.06 | 0.05 | 0.35 | 0.41 | 358 (CI: 222–495) |
| Niger | 1.11 | 1.76 | 1.33 | 1.89 | 1.36 | 1.24 | 0.65 | 1.41 | 535 (CI: 425–645) |
| Nigeria | 0.65 | 1.02 | 1.1 | 1.34 | 1.33 | 0.79 | 0.69 | 1 | 556 (CI: 484–629) |
| Rwanda | 0.05 | 0.08 | 0.21 | 0.47 | 0.57 | 0.68 | 0.77 | 0.34 | 274 (CI: 197–351) |
| Sao Tome and Principe | 0 | 0 | 0.11 | 0.34 | 0.11 | 0.89 | 0 | 0.18 | 116 (CI: 25–207) |
| Senegal | 0.13 | 0.31 | 0.37 | 0.76 | 0.64 | 0.65 | 0.28 | 0.42 | 273 (CI: 201–345) |
| Sierra Leone | 0.63 | 0.98 | 1.12 | 1.49 | 1.92 | 1.27 | 0.65 | 1.12 | 796 (CI: 632–960) |
| South Africa | 0 | 0.36 | 0.58 | 0.46 | 0.76 | 1.22 | 0.11 | 0.47 | 536 (CI: 270–802) |
| Tanzania | 0.28 | 0.67 | 0.98 | 0.6 | 1.26 | 2.06 | 1.13 | 0.87 | 530 (CI: 405–655) |
| Togo | 0.39 | 0.8 | 0.78 | 0.55 | 0.71 | 0.8 | 0.13 | 0.62 | 401 (CI: 290–512) |
| Uganda | 0.41 | 0.7 | 0.76 | 0.95 | 0.75 | 1.19 | 0.16 | 0.69 | 368 (CI: 301–434) |
| Zambia | 0.04 | 0.64 | 0.57 | 0.63 | 0.27 | 0.32 | 1.02 | 0.45 | 278 (CI: 182–375) |
| Zimbabwe | 0.38 | 0.77 | 0.81 | 1.15 | 1.32 | 1.62 | 0.77 | 0.9 | 651 (CI: 473–829) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okonji, O.C.; Nzoputam, C.I.; Ekholuenetale, M.; Okonji, E.F.; Wegbom, A.I.; Edet, C.K. Differentials in Maternal Mortality Pattern in Sub-Saharan Africa Countries: Evidence from Demographic and Health Survey Data. Women 2023, 3, 175-188. https://doi.org/10.3390/women3010014
Okonji OC, Nzoputam CI, Ekholuenetale M, Okonji EF, Wegbom AI, Edet CK. Differentials in Maternal Mortality Pattern in Sub-Saharan Africa Countries: Evidence from Demographic and Health Survey Data. Women. 2023; 3(1):175-188. https://doi.org/10.3390/women3010014
Chicago/Turabian StyleOkonji, Osaretin Christabel, Chimezie Igwegbe Nzoputam, Michael Ekholuenetale, Emeka Francis Okonji, Anthony Ike Wegbom, and Clement Kevin Edet. 2023. "Differentials in Maternal Mortality Pattern in Sub-Saharan Africa Countries: Evidence from Demographic and Health Survey Data" Women 3, no. 1: 175-188. https://doi.org/10.3390/women3010014
APA StyleOkonji, O. C., Nzoputam, C. I., Ekholuenetale, M., Okonji, E. F., Wegbom, A. I., & Edet, C. K. (2023). Differentials in Maternal Mortality Pattern in Sub-Saharan Africa Countries: Evidence from Demographic and Health Survey Data. Women, 3(1), 175-188. https://doi.org/10.3390/women3010014