Abstract
Slipped capital femoral epiphysis (SCFE) is the most common adolescent hip disorder in children 9–15 years old with an incidence that ranges from 0.33:100,000 to 24.58:100,000. Idiopathic SCFE is strongly associated with obesity, while atypical SCFE is associated with endocrinopathies, metabolic and renal disease, radiation therapy, and chemotherapy. In this review, we summarized the current data regarding the pathogenesis of SCFE and its association to obesity. In the last years, there have been increasing evidence regarding the implication of obesity in the pathogenesis of SCFE, but no definitive mechanism has been proven. The etiology is probably multifactorial, with both mechanical and metabolic factors contributing to the disease, with the later gaining more ground, especially in obese patients. Understanding what causes the disease will help paediatricians and orthopaedists develop more efficient strategies for treating patients and diminishing complication rates.
1. Introduction
Slipped capital femoral epiphysis (SCFE) is a common condition among adolescents, primarily affecting children between the ages of 9 and 15 years old [1,2].
It is defined as displacement of the proximal femoral epiphysis from the metaphysis through the proximal femoral growth plate. It is a condition that is often not detected early, because the primary clinical characteristic is subtle pain in the knee or thigh, that goes on for weeks or months, causing confusion among patients and clinicians alike. Delay in diagnosis is even more frequent when the primary complaint at presentation is knee pain, which can be misleading for physicians [3,4]. SCFE can be classified as stable or unstable, with the latter being more severe and preventing the patient from ambulating even with the aid of crutches [5]. No pathognomonic clinical sign exists, but limited internal rotation of the hip and passive hip flexion are the most common findings. Diagnosis is made with standard biplanar radiographic examination of the hips, where the supine anteroposterior pelvis and Lauenstein (frog) lateral view present the classical anterior displacement of the anterior femoral neck, with relative posterior displacement of the capital femoral epiphysis, while in the pre-slip, slight widening of the physis may be depicted [6].
The natural history of untreated SCFE seems to cause a low level of disability particularly in mild cases according to the reports of Orderberg et al. [7] and Carney and Weinstein et al. [8], but activity level and patient expectations may have changed since the early 20th century and operative treatment has been established as the gold standard [9]. The long-term sequelae of SCFE may lead to avascular necrosis of the femoral head, femoroacetabular impingement, permanent hip deformity, and the need for early hip arthroplasty due to degenerative arthritis [10]. The most common cause for an early total hip replacement in patients with SCFE is avascular necrosis of the femoral head, which occurs in 15–50% of patients with acute, unstable slips. Although the greatest risk to the femoral head may be avascular necrosis, we must not neglect that to the child, the greatest risk is undoubtedly the associated medical comorbidities and sequelae of obesity [9].
In addition to discussing the risk factors associated with obesity and SCFE, this study will also highlight the importance of early detection and proper management of the condition. Timely diagnosis and treatment can prevent long-term complications, such as avascular necrosis, hip deformity, and early hip arthroplasty. Furthermore, understanding the underlying mechanisms of SCFE can lead to the development of more effective prevention and treatment strategies. Overall, this study aims to provide a comprehensive overview of SCFE, with a focus on the relationship between obesity and the disease.
2. Epidemiology
The overall current incidence of SCFE ranges from 0.33 in 100,000 in Korean to 24.58 in 100,000 in African-American children 8–15 years and in the US-based population, it is 10.8/100,000 [11]. There is variation in the disease prevalence depending upon ethnicity, gender, season, geographical location, and place of residence [1,12,13]. In the US, the highest prevalence is seen in the Northeast regions while the lowest in the Midwest [2]. In the last century, a gradual decline in age of onset had been seen, but this trend has now stopped [11,14]. Currently, the average age of onset reported is 12.0 years for boys and 11.2 years for girls [15]. There are also variations regarding the male to female ratio, with reports from 1.1:1 in the Maori population, up to 4.1:1 in the Singapore population, but the difference has gradually leveled out with time [1,11,16]. Loder et al. [11] reported that the relative racial frequency (RRF) of SCFE relative to Caucasians is 5.6 for Polynesians, 3.9 for Africans, and 2.5 for Hispanics. The percentage is higher at 5.6 for Maori and at 4.2 for other Pacific Islanders. In Singapore, the RRFs, relative to Chinese, is 9.6 for Indo-Mediterraneans, 2.8 for Indo-Malay, and 3.0 for mixed Eurasians. The native Maori population is affected the most, while the Asian population demonstrates low incidence (Table 1). Epidemiologic studies suggest that obesity is prevalent among adolescents with SCFE, with >50% being over the 95th percentile weight for age and presenting with the condition in a younger age [11].

Table 1.
Epidemiologic studies on SCFE.
3. Slipped Capital Femoral Epiphysis and Obesity
Slipped capital femoral epiphysis has either idiopathic or atypical etiology [29]. Idiopathic SCFE is strongly associated with obesity, which consists almost 80% of the total population at risk [30], while atypical is associated with endocrinopathies, metabolic and renal disease, radiation therapy, and chemotherapy [31].
Most of the children presenting with SCFE are obese, with more than 50% of children being in the >95th percentile weight for the age [11]. A large cohort study that used data from health screening examinations at primary school entry (597,017 children 5–6 years old) in Scotland and a further screening examination at primary school exit (39,468 children 11–12 years old), linked to a nationwide hospital admissions database, from Perry et al. [32], found that children with the lowest BMI at 5 to 6 years old had an almost insignificant lifetime risk of SCFE, those with a normal BMI had an estimated lifetime risk of 1:2500, those overweight had an estimated risk of 1:1750, those with mild or moderate obesity had a risk of 1:650, and those with severe obesity had a lifetime risk of 1:450. For children 11–12 years old, which is the age where obesity has the strongest association with SCFE, the lifetime risk among those with severe obesity is 1:250. One of the most critical public health issues of the twenty-first century is childhood obesity. Rising obesity rates among children and adolescents aged 5 to 19 have been observed in practically all countries, even those where the issue was not very concerning 40 years ago. In the WHO European Region, one child out of three is overweight or obese [33]. According to WHO report of 9 June 2021 [34], the prevalence of overweight and obese children and adolescents aged 5–19 has risen dramatically, from just 4% in 1975 to just over 18% in 2016. The rise has occurred similarly among boys and girls: in 2016, 18% of girls and 19% of boys were overweight. In a retrospective study in the US that was conducted to investigate long-term patient-reported outcomes of a cohort of 64 patients with SCFE (91 affected hips) with a 20-year follow up, and to determine whether the slip angle was associated with poorer health outcomes, the self-reported health was poorer than the average population, with higher rates of diabetes, hypertension, and obesity observed [35]. In a case-control study of 51 patients treated for SCFE and 62 healthy adolescents without SCFE, mean HbA1c levels were significantly higher than in obese patients without the condition, but there were no differences in the lipid profile, pointing out that patients diagnosed with SCFE should be considered as potential future type 2 diabetes mellitus patients. As a result, follow-up after surgical treatment of SCFE patients should include not only orthopedic outcomes but evaluation of risk factors for diabetes mellitus as well [36]. Although association between childhood obesity and SCFE has not yet been definitively proven, the increase in its prevalence along with the increase in incidence of SCFE is alarming.
4. Pathogenesis
The pathogenesis of the disease is not yet thoroughly ascertained, with SCFE being most frequently the outcome of a multifactorial event [11]. Understanding SCFE’s pathogenesis precisely is crucial for both interpretation of the disease, the potential development of a rational therapeutic plan, as well as prevention strategies [37]. There are several etiological factors that can lead to SCFE, and which can act both separately or collectively. These include mechanical and anatomic factors [38,39], hormonal and endocrine factors [40,41], obesity [42,43], and immunological abnormalities [30].
Most cases of SCFE are idiopathic, presenting without any other underlying condition. However, a strong relation with childhood obesity has been demonstrated [19]. Obesity is recognized as a global health issue, particularly in Western industrialized nations [32,33,34], and is a well-established risk factor for SCFE. Three key elements in the pathophysiology of SCFE include an increase in body mass, the maintenance of the perichondrial ring, and high levels of activity [39]. In the presence of preexisting physeal pathology, the additional forces induced by obesity could result in a slip [43].
Obesity has been linked to leptin resistance, primarily by providing adequate satiety feedback and secondarily resulting in greater signaling at other sites of action [42]. This is achieved when the serum leptin levels exceed the normal ones in non-obese individuals. Leptin levels are elevated in children with obesity. As observed in SCFE, leptin has the potential to enhance the proliferative zone’s width. Leptin stimulates chondrocyte hypertrophy and proliferation; variations in leptin levels result in an extended physis, disrupted columnar structure, cellular apoptosis, and diminished expression and organization of the type-II and type-X collagen, normally observed throughout the hypertrophic zone [44]. Regarding the histologic similarities between SCFE-affected physes and hyperleptinemic physes, in addition to the connection between increased leptin and body mass index (BMI), we can suspect that leptin may be the cause of physeal pathology necessary for the emergence of SCFE [44,45]. In tissues obtained from biopsies in SCFE, alterations in the longitudinal orientation of the physeal cartilage cells, which are typically parallel to the axis of the bone, are observed. The columnar organization and the extracellular matrix composition of the physis in SCFE differ significantly histologically from those of a healthy physis (Figure 1). Although all the above changes are performed in sequence and in response, their role is still unknown. It remains a question as to whether they are of causal or adaptive reason. Additionally, some of these modifications can be present in endocrine or metabolic disorders [40].
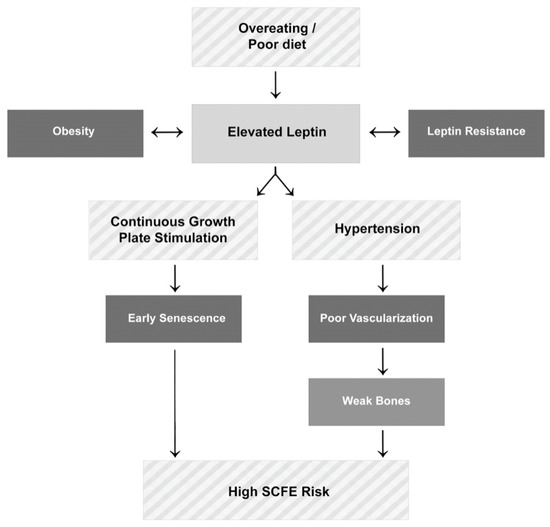
Figure 1.
The effect of leptin on the pathophysiology of slipped capital femoral epiphysis.
Obesity causes accelerated growth earlier in the prepubescent stage, advancing puberty in females and delaying it in males [46,47]. The positive effect of insulin and insulin like growth factor 1 (IGF-1) in the proliferation and hypertrophy of differentiated chondrocytes of the physis has been well demonstrated [48,49,50]. Wu et al. [51], using a mice model, demonstrated that mice fed with a high fat diet developed greater body and tibial growth and higher serum insulin levels. Montanez-Alvarez et al. [41], in a case-control study of 14 children with SCFE compared to 23 age and BMI matched obese children without the disease conducted in Mexico, found elevated serum insulin, triglycerides, and very low density lipoprotein levels in the first group. Hyperinsulinemia impairs normal apoptosis of chondrocytes, which is necessary in the transition from physis to bone, therefore contributing in the broadening and weakening of the physis [49,52]. In a histologic study of the proximal femoral growth plate of eight core biopsies of the proximal femoral growth plate during in situ epiphysiodesis in patients with SCFE in the pre-slipping stage in two cases and at the mild slipping stage (Southwick angle < 30°) in six cases, there were significant structural changes. Chondrocytes were smaller, elongated, and arranged in clusters rather than columns, with thinner collagen fibrils and impaired physeal architecture [53], events suggesting that there are probably hormonal and metabolic factors rather than mechanical that cause the physis to deteriorate before the slip occurs.
Patients with SCFE frequently have delayed sexual maturation, which could indicate a delay in physeal closure. This produces an extended period of weakness, resulting in a physis prone to the impacts of augmented load, mainly in the pre-existence of obesity. This interruption is implicated in the slip. Children with obesity are most commonly diagnosed with the above-mentioned condition [40].
It is fundamental to consider that atypical SCFE manifests with distinct clinical and radiological features, as well as different complications from idiopathic SCFE. Atypical SCFE is linked to endocrine abnormalities, neoplastic or metabolic disorders, including renal osteodystrophy, chemotherapy, or radiation therapy on the pelvic region [54].
Both biomechanical and biochemical alterations developing during puberty are generally established etiologies [55].
4.1. Endocrine Factors
Hypogonadal diseases, hypothyroidism, as well as growth hormone (GH) suppletion that constitute systemic or endocrine abnormalities deteriorate the physis. SCFE is prevalent among pediatric patients diagnosed with apparent endocrinopathies, which include hypopituitarism, hyperparathyroidism, and hypogonadal states but also hypo- and hyperthyroidism. Thyroid hormone via signaling of the Indian hedgehog/parathyroid hormone-related protein (IHH–PTHrH) pathway affects the physis both directly and indirectly [40].
Thyroid hormone facilitates growth, development, and maturation of the skeleton by stimulating chondrocyte proliferation, inducing differentiation of bone progenitor cells, mineralization, and angiogenesis. Moreover, it facilitates pituitary GH secretion and GH-dependent IGF-1 production in the bone, which both have regulatory effects on the activity of GH [56]. The epiphyseal plate becomes hypoplastic and endochondral and intramembranous ossification are delayed in children with thyroid hormone insufficiency. The growth hormone/insulin-like growth factor axis is rendered inactive by thyroid hormone deprivation. Recent animal studies have shown that hypothyroid swine displays much lower aggrecan and type X collagen gene expression, demonstrating the effect of hypothyroidism on the development plate [57]. Such modifications probably reduce the overall strength and resilience of the epiphysis, which may provide insight on the diseases of the human orthopedic growth plate. In patients with SCFE with atypical presentation, such as children younger than the age of 10 or older than 16 years old, those who have bilateral SCFE, or those whose height is less than 10% of the normal range for their age and sex, suggested thyroid function screening is suggested [58,59].
A rare pediatric condition, known as pseudohypoparathyroidism (PHP) type 1b, is marked by renal resistance to the parathyroid hormone (PTH), which results in biochemical hypoparathyroidism with skeletal sensitivity to PTH. Despite otherwise normal renal function, PHP is characterized by renal resistance to PTH, which leads to hypocalcemia and hyperphosphatemia and increased PTH concentrations. Since there is osseous sensitivity to PTH, bone resorption occurs [60].
In pediatric patients, long-lasting ailments provoke growth deficiency through altered mechanisms, which manifest on the GH/IGF-1 axis [61].
Physeal disorders mimic those developed in SCFE, mostly in young children with chronic renal failure that have higher risk of developing renal osteodystrophy. High and long-lasting concentrations of glucocorticoids decrease growth, directly and indirectly. Nevertheless, there is no clear evidence indicating the relation between glucocorticoids and SCFE [40].
In patients with malignancies, the survival rates have significantly improved, leading to the hypothesis of atypical SCFE as a late complication of radiotherapy and chemotherapy due to the systemic effects on the physis. Although physeal chondrocyte radiosensitivity, radiation’s indirect endocrine effects, and chemotherapeutic radiosensitization have all been proposed as potential reasons, the exact mechanisms are still unknown. The fact that the majority of studies to date have not particularly addressed the clinical and radiologic characteristics of atypical SCFE is likely related to the relatively small number of subjects. Chemotherapy as a systemic treatment for pediatric malignancies may be the cause of atypical SCFE associated with a secondary endocrine dysfunction. Up to date, there is lack of evidence about an immediate association between chemotherapy and SCFE [54].
4.2. Immunilogical/Biochemical Factors
In their study, Eisenstein and Rothschild [62] investigated the biochemical abnormalities associated with SCFE and chondrolysis. They found that patients with SCFE had elevated levels of serum immunoglobulins, particularly IgA, as well as an elevated C3 component of complement. Interestingly, IgA had the highest values despite other laboratory tests being normal. Additionally, urinary glycosaminoglycan levels were elevated and increased with the severity of the illness. The authors speculated that these findings could suggest either that slipping of the epiphysis generates an antigen that triggers an autoimmune response, or that slipping is a localized manifestation of a generalized process replicating a connective tissue disorder or an inflammatory state. They also noted that while no other biochemical abnormalities were detected in patients with chondrolysis, the IgM fraction was significantly increased. These preliminary findings suggest that SCFE may be associated with underlying immunological and connective tissue disorders. Furthermore, it is possible that a subset of patients with SCFE may be genetically predisposed to chondrolysis. However, further research is needed to confirm these hypotheses and to fully understand the underlying mechanisms of SCFE and its associated complications. Overall, the study by Eisenstein and Rothschild sheds light on the complex pathophysiology of SCFE and provides important insights into potential underlying mechanisms. Further studies are needed to confirm and expand upon these findings, which may ultimately lead to more effective prevention and treatment strategies for this condition.
4.3. Mechanical Factors
Mechanical factors are categorized as contributing factors in the pathogenesis of SCFE. Direct or indirect injuries are fairly uncommon, in most cases, mild and rarely of decisive importance [39]. The proximal femoral physis’ mechanical insufficiency is assumed to be part of the pathogenesis of SCFE. The slip can be caused either due to an abnormally high load across a normal physis or due to a physiological load across an abnormally weak physis, or a combination of both. Obesity, femoral and acetabular retroversion, the persistence of the perichondrial ring, epiphyseal tubercle height and location, and physeal cupping [63,64] are part of the mechanical factors contributing to the disease [39,65]. The accepted etiology postulates that as biomechanical forces increase, they eventually exceed the physis’ structural capacity, causing the epiphysis to slip or translate from its starting position, usually posteroinferiorly [44]. Many children during their growth expose their hip joints to high mechanical loads during both normal as well as strenuous sports activities [40]. Results indicate that during physical activity, the growth plate may undergo an abnormal escalation in tension when subjected to an impact loading. Even under physiological conditions, this could cause the plate to deteriorate and subsequently fracture [66]. Despite being obese and rapidly growing, the majority of adolescents with SCFE do not have hormonal metabolic or chronic disorders. However, it seems unlikely that mechanical overload of the proximal femur epiphysis caused, for instance, by excessive body weight alone, can result in a slip. The aforementioned theory is further supported by the results of Winston et al. [38]. In their research, they measured using computerized tomography, epiphyseal tubercule height, width, and volume, physeal diameter, cupping height, acetabular inclination and rotation, and metaphyseal bone density in 31 obese children and 31 age- and gender-matched children with normal weight. Their results indicate that obesity does not cause morphologic changes in the proximal femoral physis, but there is high metaphyseal metabolic activity, as demonstrated by lower bone mineral density in the metaphysis of obese children [38]. In a finite element 3-dimentional model of the adolescent hip, the combined effect of physeal thickness, physeal-diaphysis angle, body weight, physical activity, and the presence of the perichondrial ring were studied for their combined effect. Their results indicate that the most influential factors that contribute to the stresses along the physis are body mass, the presence of the perichondrial ring, and physical activity. In fact, the presence of the perichondrial ring decreased the stress along the physis by 2.53 MPa and high impact activity, such as jumping, had a double mean stress value than toe-off. Slopping angles between 49.9–51.9 had mean stress value 1.36 times greater than angles 41.9–47.9 [39], therefore indicating that increased obliquity is a stress riser of the physis. A detailed diagram of the factors contributing to the pathophysiology of SCFE is shown in Figure 2.
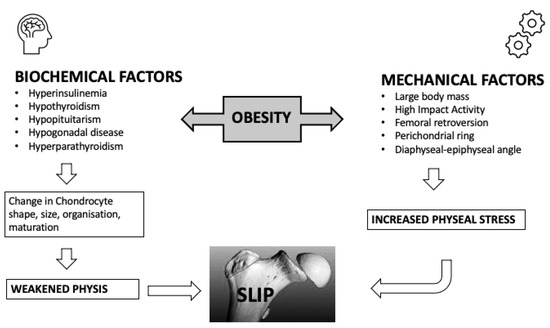
Figure 2.
Pathogenesis of slipped capital femoral epiphysis.
5. Summary
Although the exact mechanisms through which obesity predisposes adolescents to the disease are not yet fully understood, evidence linking obesity with idiopathic SCFE have been provided through observational studies [67,68], case series [69,70], mathematical models [39,71,72], and population-based epidemiologic cohorts [1,14,32], where a strong association has been demonstrated. Non-obese children presenting with the disease are more likely to suffer an atypical, unstable, and more severe slip [30]. For idiopathic cases, the lifetime risk for adolescents with severe obesity is 17 times higher than those with normal weight, who have almost negligible risk, as shown by Perry et al. [32]. The mechanisms through which obesity predisposes adolescents to the disease are based on metabolic and mechanistic theories, with no clear superiority of one over the other. On one hand, the excess adipose tissue of obese children causes earlier onset of the prepubertal period, delayed physeal closure, morphologic changes in the zones of the physis, and changes in the shape, size, alignment, and apoptosis of the physeal chondrocytes [46,47,49,50,51,52,53]. Elevated insulin levels observed in obese children contribute to the proliferation, hypertrophy, and delayed chondrocyte apoptosis, thus contributing to the proximal femoral growth plate widening and delayed ossification [51,52]. Other studies have suggested that obesity can lead to mechanical factors that increase stress on the proximal femoral physis [39,73,74]. Physeal thickness has been proposed as a contributing factor to the forces exerted across the proximal femoral physis, which is influenced by metabolic changes. As Castro et al. [39] showed, when physeal thickness exceeded 2.1 mm, there were significant changes in stress through the physis. In a retrospective study, the hip morphology of 31 obese and non-obese adolescents was documented using computerized tomography. Physeal diameter, tubercule height, width, and volume, cupping height, acetabular inclination and rotation, and bone density were measured. Obese children were found to have non-significant morphologic changes of the aforementioned parameters compared to non-obese children, with the exception of lower metaphyseal bone density [38]. On the other hand, another study demonstrated that children between 9–12 years old tend to have a more vertical proximal femoral orientation [73], which increases stress to the physis. The perichondrial ring, which is stronger and more important in early childhood, and the epiphyseal tubercle and metaphyseal fossa, are structures important to the stability of the capital epiphysis and resistance to shear forces. Damage to those elements may predispose the proximal femoral physis to failure under excess stress [39,65,74]. Children with increased body mass and high impact activities place their femurs in higher mechanical stress [39]. All the aforementioned factors, when combined, may lead to physeal fracture and a clinical slip. In the last years, there have been increasing evidence regarding the implication of obesity in the pathogenesis of SCFE, but no definitive mechanism has been proven. The etiology is probably multifactorial, with both mechanical and metabolic factors contributing to the disease, with the later gaining more ground, especially in obese patients.
Developing effective strategies for preventing, diagnosing, and managing SCFE is essential for improving the prognosis and reducing the morbidity and mortality associated with this condition. Given the established link between obesity and idiopathic SCFE, interventions that focus on reducing obesity may be a critical component of primary prevention efforts. Efforts should also be directed towards screening high-risk individuals, including overweight and obese children, for early detection and timely management of the disease. Treatment approaches for SCFE include surgical and non-surgical interventions, with the former being the preferred treatment option for severe slips. In addition, early diagnosis and treatment can help prevent complications, such as chondrolysis and avascular necrosis. Clinicians should also be aware of potential risk factors for the disease and provide appropriate counseling to patients and families regarding lifestyle modifications and weight management. Overall, a better understanding of the etiology of SCFE can lead to the development of more effective prevention and treatment strategies, ultimately improving the outcomes for children with this condition.
Author Contributions
Conceptualization, V.C. and G.K.; methodology, V.C.; investigation, V.C., E.P. and G.R.; resources, V.C., E.P. and G.R.; data curation, V.C. and G.K.; writing—original draft preparation, V.C., E.P., G.R. and G.K.; writing—review and editing, V.C. and G.K.; visualization, G.K.; supervision, V.C.; project administration, G.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors acknowledge the contribution of the Architect Myrto Bitsa in designing the Figures of this manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Herngren, B.; Stenmarker, M.; Vavruch, L.; Hagglund, G. Slipped Capital Femoral Epiphysis: A Population-Based Study. BMC Musculoskelet. Disord. 2017, 18, 304. [Google Scholar] [CrossRef]
- Lehmann, C.L.; Arons, R.R.; Loder, R.T.; Vitale, M.G. The Epidemiology of Slipped Capital Femoral Epiphysis: An Update. J. Pediatr. Orthop. 2006, 26, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Perry, D.C.; Metcalfe, D.; Costa, M.L.; Van Staa, T. A Nationwide Cohort Study of Slipped Capital Femoral Epiphysis. Arch. Dis. Child. 2017, 102, 1132–1136. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.S.; Bishop, J.A.; Weed, B.; Hresko, M.T.; Millis, M.B.; Kim, Y.J.; Kasser, J.R. Delay in Diagnosis of Slipped Capital Femoral Epiphysis. Pediatrics 2004, 113, e322–e325. [Google Scholar] [CrossRef] [PubMed]
- Loder, R.T.; Richards, B.S.; Shapiro, P.S.; Reznick, L.R.; Aronson, D.D. Acute Slipped Capital Femoral Epiphysis: The Importance of Physeal Stability. J. Bone Jt. Surg. Am. 1993, 75, 1134–1140. [Google Scholar] [CrossRef]
- Millis, M.B. SCFE: Clinical Aspects, Diagnosis, and Classification. J. Child. Orthop. 2017, 11, 93–98. [Google Scholar] [CrossRef]
- Ordeberg, G.; Hansson, L.I.; Sandström, S. Slipped Capital Femoral Epiphysis in Southern Sweden. Long-Term Result with No Treatment or Symptomatic Primary Treatment. Clin. Orthop. Relat. Res. 1984, 191, 95–104. [Google Scholar] [CrossRef]
- Carney, B.T.; Weinstein, S.L. Natural History of Untreated Chronic Slipped Capital Femoral Epiphysis. Clin. Orthop. Relat. Res. 1996, 322, 43–47. [Google Scholar] [CrossRef]
- Mathew, S.E.; Larson, A.N. Natural History of Slipped Capital Femoral Epiphysis. J. Pediatr. Orthop. 2019, 39, S23–S27. [Google Scholar] [CrossRef]
- Porter, M.; Borroff, M.; Gregg, P.; Howard, P.; MacGregor, A.; Tucker, K. National Joint Registry for England and Wales. 9th Annual Report; National Joint Registry for England and Wales: Hemel Hempstead, UK, 2012. [Google Scholar]
- Loder, R.T.; Skopelja, E.N. The Epidemiology and Demographics of Slipped Capital Femoral Epiphysis. ISRN Orthop. 2011, 2011, 486512. [Google Scholar] [CrossRef]
- Farrier, A.J.; Ihediwa, U.; Khan, S.; Kumar, A.; Gulati, V.; Uzoigwe, C.E.; Choudhury, M.Z. The Seasonality of Slipped Upper Femoral Epiphysis-Meta-Analysis: A Possible Association with Vitamin D. HIP Int. 2015, 25, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Loder, R.T.; Schneble, C.A. Seasonal Variation in Slipped Capital Femoral Epiphysis: New Findings Using a National Children’s Hospital Database. J. Pediatr. Orthop. 2019, 39, e44–e49. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, G.; Hansson, L.I.; Ordeberg, G. Epidemiology of Slipped Capital Femoral Epiphysis in Southern Sweden. Clin. Orthop. Relat. Res. 1984, 191, 82–94. [Google Scholar] [CrossRef]
- Aprato, A.; Conti, A.; Bertolo, F.M.A. Slipped Capital Femoral Epiphysis: Current Management Strategies. Orthop. Res. Rev. 2019, 11, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.-J.; Kagda, F.; Lam, K.S.; Hui, J.H.P.; Lim, K.B.L.; Mahadev, A.; Lee, E.H. Demographics and Clinical Presentation of Slipped Capital Femoral Epiphysis in Singapore: Comparing the East with the West. J. Pediatr. Orthop. B 2008, 17, 289–292. [Google Scholar] [CrossRef]
- Larson, A.N.; Yu, E.M.; Melton, L.J., 3rd; Peterson, H.A.; Stans, A.A. Incidence of Slipped Capital Femoral Epiphysis: A Population-Based Study. J. Pediatr. Orthop. B 2010, 19, 9–12. [Google Scholar] [CrossRef]
- Witbreuk, M.M.; van Royen, B.J.; Van Kemenade, F.J.; Witte, B.I.; van der Sluijs, J.A. Incidence and Gender Differences of Slipped Capital Femoral Epiphysis in the Netherlands from 1998-2010 Combined with a Review of the Literature on the Epidemiology of SCFE. J. Child. Orthop. 2013, 7, 99–105. [Google Scholar] [CrossRef]
- Murray, A.W.; Wilson, N.I.L. Changing Incidence of Slipped Capital Femoral Epiphysis: A Relationship with Obesity? J. Bone Jt. Surg. Br. 2008, 90, 92–94. [Google Scholar] [CrossRef]
- Benson, E.C.; Miller, M.; Bosch, P.; Szalay, E.A. A New Look at the Incidence of Slipped Capital Femoral Epiphysis in New Mexico. J. Pediatr. Orthop. 2008, 28, 529–533. [Google Scholar] [CrossRef]
- Song, K.-S.; Oh, C.-W.; Lee, H.-J.; Kim, S.-D. Epidemiology and Demographics of Slipped Capital Femoral Epiphysis in Korea: A Multicenter Study by the Korean Pediatric Orthopedic Society. J. Pediatr. Orthop. 2009, 29, 683–686. [Google Scholar] [CrossRef]
- Noguchi, Y.; Sakamaki, T.; Multicenter Sutdy Commitee of the Japanese Pediatric Orthopaedic Association. Epidemiology and Demographics of Slipped Capital Femoral Epiphysis in Japan: A Multicenter Study by the Japanese Paediatric Orthopaedic Association. J. Orthop. Sci. 2002, 7, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Ravinsky, R.; Rofaiel, J.; Escott, B.G.; Lim, Z.; Ravi, B.; Howard, A. Epidemiology of Slipped Capital Femoral Epiphysis in Ontario, Canada. J. Pediatr. Orthop. 2019, 39, e165–e167. [Google Scholar] [CrossRef]
- Phadnis, J.; Phillips, P.; Willoughby, R. The Epidemiologic Characteristics of Slipped Capital Femoral Epiphysis in Maori Children. J. Pediatr. Orthop. 2012, 32, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Fedorak, G.T.; Brough, A.K.; Miyamoto, R.H.; Raney, E.M. The Epidemiology of Slipped Capital Femoral Epiphysis in American Samoa. Hawaii. J. Med. Public Health 2018, 77, 215–219. [Google Scholar] [PubMed]
- Longo, U.G.; Papalia, R.; De Salvatore, S.; Ruzzini, L.; Candela, V.; Piergentili, I.; Oggiano, L.; Costici, P.F.; Denaro, V. Slipped Capital Femoral Epiphysis: An Epidemiological Nationwide Study in Italy from 2001 to 2015. BMC Musculoskelet. Disord. 2021, 22, 570. [Google Scholar] [CrossRef]
- Beharry, A.C.; Quan Soon, C.H.; Augustus, M.; Toby, D.; Thomas, D. Increasing Incidence of Slipped Capital Femoral Epiphysis in Trinidad and Tobago: A 50-Year Review. Trop. Doct. 2023, 53, 85–90. [Google Scholar] [CrossRef]
- Nguyen, A.R.; Ling, J.; Gomes, B.; Antoniou, G.; Sutherland, L.M.; Cundy, P.J. Slipped Capital Femoral Epiphysis: Rising Rates with Obesity and Aboriginality in South Australia. J. Bone Jt. Surg. Br. 2011, 93, 1416–1423. [Google Scholar] [CrossRef]
- Loder, R.T.; Greenfield, M.L. Clinical Characteristics of Children with Atypical and Idiopathic Slipped Capital Femoral Epiphysis: Description of the Age-Weight Test and Implications for Further Diagnostic Investigation. J. Pediatr. Orthop. 2001, 21, 481–487. [Google Scholar] [CrossRef]
- Obana, K.K.; Siddiqui, A.A.; Broom, A.M.; Barrett, K.; Andras, L.M.; Millis, M.B.; Goldstein, R.Y. Slipped Capital Femoral Epiphysis in Children without Obesity. J. Pediatr. 2020, 218, 192–197.e1. [Google Scholar] [CrossRef]
- Mann, D.C.; Weddington, J.; Richton, S. Hormonal Studies in Patients with Slipped Capital Femoral Epiphysis without Evidence of Endocrinopathy. J. Pediatr. Orthop. 1988, 8, 543–545. [Google Scholar] [CrossRef]
- Perry, D.C.; Metcalfe, D.; Lane, S.; Turner, S. Childhood Obesity and Slipped Capital Femoral Epiphysis. Pediatrics 2018, 142, e20181067. [Google Scholar] [CrossRef] [PubMed]
- Nittari, G.; Scuri, S.; Petrelli, F.; Pirillo, I.; di Luca, N.M.; Grappasonni, I. Fighting Obesity in Children from European World Health Organization Member States. Epidemiological Data, Medical-Social Aspects, and Prevention Programs. Clin. Ter. 2019, 170, e223–e230. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 10 January 2023).
- Escott, B.G.; De La Rocha, A.; Jo, C.-H.; Sucato, D.J.; Karol, L.A. Patient-Reported Health Outcomes After in Situ Percutaneous Fixation for Slipped Capital Femoral Epiphysis: An Average Twenty-Year Follow-up Study. J. Bone Jt. Surg. Am. 2015, 97, 1929–1934. [Google Scholar] [CrossRef] [PubMed]
- Ucpunar, H.; Camurcu, I.Y.; Duman, S.; Ucpunar, E.; Sofu, H.; Bayhan, A.I. Obesity-Related Metabolic and Endocrine Disorders Diagnosed during Postoperative Follow-up of Slipped Capital Femoral Epiphysis. Acta Orthop. 2018, 89, 314–319. [Google Scholar] [CrossRef]
- Carlos, C.; Magda, M. Slipped Capital Femoral Epiphysis: A Review for Pediatricians. Pediatr. Ann. 2018, 47, e377–e380. [Google Scholar] [CrossRef]
- Winston, T.W.; Landau, A.J.; Hosseinzadeh, P. Proximal Femoral Changes Related to Obesity: An Analysis of Slipped Capital Femoral Epiphysis Pathoanatomy. J. Pediatr. Orthop. B 2022, 31, 216–223. [Google Scholar] [CrossRef]
- Castro-Abril, H.A.; Galván, F.; Garzón-Alvarado, D.A. Geometrical and Mechanical Factors That Influence Slipped Capital Femoral Epiphysis: A Finite Element Study. J. Pediatr. Orthop. B 2015, 24, 418–424. [Google Scholar] [CrossRef]
- Witbreuk, M.; van Kemenade, F.J.; van der Sluijs, J.A.; Jansma, E.P.; Rotteveel, J.; van Royen, B.J. Slipped Capital Femoral Epiphysis and Its Association with Endocrine, Metabolic and Chronic Diseases: A Systematic Review of the Literature. J. Child. Orthop. 2013, 7, 213–223. [Google Scholar] [CrossRef]
- Montañez-Alvarez, M.; Flores-Navarro, H.H.; Cuevas-De Alba, C.; Arana-Hernández, E.I.; Ramírez-Ruiz, M. The Role of Hyperinsulinemia in Slipped Capital Femoral Epiphysis. J. Pediatr. Orthop. 2020, 40, 413–417. [Google Scholar] [CrossRef]
- Galbraith, R.T.; Gelberman, R.H.; Hajek, P.C.; Baker, L.A.; Sartoris, D.J.; Rab, G.T.; Cohen, M.S.; Griffin, P.P. Obesity and Decreased Femoral Anteversion in Adolescence. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 1987, 5, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Wabitsch, M.; Horn, M.; Esch, U.; Mayer, H.; Moss, A.; Günther, K.-P.; Nelitz, M. Silent Slipped Capital Femoral Epiphysis in Overweight and Obese Children and Adolescents. Eur. J. Pediatr. 2012, 171, 1461–1465. [Google Scholar] [CrossRef] [PubMed]
- Halverson, S.J.; Warhoover, T.; Mencio, G.A.; Lovejoy, S.A.; Martus, J.E.; Schoenecker, J.G. Leptin Elevation as a Risk Factor for Slipped Capital Femoral Epiphysis Independent of Obesity Status. J. Bone Jt. Surg. 2017, 99, 865–872. [Google Scholar] [CrossRef]
- Bhatia, N.N.; Pirpiris, M.; Otsuka, N.Y. Body Mass Index in Patients with Slipped Capital Femoral Epiphysis. J. Pediatr. Orthop. 2006, 26, 197–199. [Google Scholar] [CrossRef]
- Dunger, D.B.; Ahmed, M.L.; Ong, K.K. Effects of Obesity on Growth and Puberty. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 375–390. [Google Scholar] [CrossRef] [PubMed]
- Burt Solorzano, C.M.; McCartney, C.R. Obesity and the Pubertal Transition in Girls and Boys. Reproduction 2010, 140, 399–410. [Google Scholar] [CrossRef]
- Green, H.; Morikawa, M.; Nixon, T. A Dual Effector Theory of Growth-Hormone Action. Differentiation 1985, 29, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zhang, Y.; De Luca, F. The Effect of a High-Calorie Diet on Bone Growth Is Mediated by the Insulin Receptor. Bone 2019, 122, 166–175. [Google Scholar] [CrossRef]
- Zhang, F.; He, Q.; Tsang, W.P.; Garvey, W.T.; Chan, W.Y.; Wan, C. Insulin Exerts Direct, IGF-1 Independent Actions in Growth Plate Chondrocytes. Bone Res. 2014, 2, 14012. [Google Scholar] [CrossRef]
- Wu, S.; Aguilar, A.L.; Ostrow, V.; De Luca, F. Insulin Resistance Secondary to a High-Fat Diet Stimulates Longitudinal Bone Growth and Growth Plate Chondrogenesis in Mice. Endocrinology 2011, 152, 468–475. [Google Scholar] [CrossRef]
- Torres, E.S.; Andrade, C.V.; Fonseca, E.C.; Mello, M.A.; Duarte, M.E.L. Insulin Impairs the Maturation of Chondrocytes In Vitro. Braz. J. Med. Biol. Res. 2003, 36, 1185–1192. [Google Scholar] [CrossRef]
- Tresoldi, I.; Modesti, A.; Dragoni, M.; Potenza, V.; Ippolito, E. Histological, Histochemical and Ultrastructural Study of Slipped Capital Femoral Epiphysis. J. Child. Orthop. 2017, 11, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.H.; Ko, K.R.; Kim, J.H.; Shim, J.S. Clinical and Radiographic Characteristics of Atypical Slipped Capital Femoral Epiphysis. J. Pediatr. Orthop. 2019, 39, e742–e749. [Google Scholar] [CrossRef] [PubMed]
- Zelaya, R.; Zarka, A.; Byerly, D. Slipped Capital Femoral Epiphysis as a Presentation of Underlying Metabolic Disorders: Pseudohypoparathyroidism and Juvenile Hypothyroidism. Cureus 2021, 13, e13775. [Google Scholar] [CrossRef] [PubMed]
- Gutch, M.; Philip, R.; Philip, R.; Toms, A.; Saran, S.; Gupta, K.K. Skeletal Manifestations of Juvenile Hypothyroidism and the Impact of Treatment on Skeletal System. Indian J. Endocrinol. Metab. 2013, 17 (Suppl. 1), S181–S183. [Google Scholar] [CrossRef]
- Tank, J.C.; Weiner, D.S.; Jacquet, R.; Childs, D.; Ritzman, T.F.; Horne, W.I.; Steiner, R.; Morscher, M.A.; Landis, W.J. The Effects of Hypothyroidism on the Proximal Femoral Physis in Miniature Swine. J. Orthop. Res. 2013, 31, 1986–1991. [Google Scholar] [CrossRef]
- Moyer, J.; Jacks, L.; Hunter, J.D.; Chan, G. Slipped Capital Femoral Epiphysis and Associated Hypothyroidism. A Review of the Literature with Two Classic Case Examples. J. Pediatr. Endocrinol. Metab. 2016, 29, 427–434. [Google Scholar] [CrossRef]
- Kadowaki, S.; Hori, T.; Matsumoto, H.; Kanda, K.; Ozeki, M.; Shirakami, Y.; Kawamoto, N.; Ohnishi, H.; Fukao, T. Prepubertal Onset of Slipped Capital Femoral Epiphysis Associated with Hypothyroidism: A Case Report and Literature Review. BMC Endocr. Disord. 2017, 17, 59. [Google Scholar] [CrossRef]
- Agarwal, C.; Seigle, R.; Agarwal, S.; Bilezikian, J.P.; Hyman, J.E.; Oberfield, S.E. Pseudohypoparathyroidism: A Rare Cause of Bilateral Slipped Capital Femoral Epiphysis. J. Pediatr. 2006, 149, 406–408. [Google Scholar] [CrossRef]
- Jingushi, S.; Suenaga, E. Slipped Capital Femoral Epiphysis: Etiology and Treatment. J. Orthop. Sci. 2004, 9, 214–219. [Google Scholar] [CrossRef]
- Eisenstein, A.; Rothschild, S. Biochemical Abnormalities in Patients with Slipped Capital Femoral Epiphysis and Chondrolysis. J. Bone Jt. Surg. Am. 1976, 58, 459–467. [Google Scholar] [CrossRef]
- Liu, R.W.; Armstrong, D.G.; Levine, A.D.; Gilmore, A.; Thompson, G.H.; Cooperman, D.R. An Anatomic Study of the Epiphyseal Tubercle and Its Importance in the Pathogenesis of Slipped Capital Femoral Epiphysis. J. Bone Jt. Surg. Am. 2013, 95, e341–e348. [Google Scholar] [CrossRef] [PubMed]
- Kiapour, A.M.; Kiapour, A.; Maranho, D.A.; Kim, Y.-J.; Novais, E.N. Relative Contribution of Epiphyseal Tubercle and Peripheral Cupping to Capital Femoral Epiphysis Stability during Daily Activities. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2019, 37, 1571–1579. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.M.; Batterman, S.C.; Brighton, C.T. Shear Strength of the Human Femoral Capital Epiphyseal Plate. J. Bone Jt. Surg. Am. 1976, 58, 94–103. [Google Scholar] [CrossRef]
- Loder, R.T.; Gunderson, Z.J.; Sun, S.; Liu, R.W.; Novais, E.V. Slipped Capital Femoral Epiphysis Associated with Athletic Activity. Sport. Health 2022, 19417381221093044. [Google Scholar] [CrossRef]
- Manoff, E.M.; Banffy, M.B.; Winell, J.J. Relationship Between Body Mass Index and Slipped Capital Femoral Epiphysis. J. Pediatr. Orthop. 2005, 25, 744–746. [Google Scholar] [CrossRef] [PubMed]
- Poussa, M.; Schlenzka, D.; Yrjönen, T. Body Mass Index and Slipped Capital Femoral Epiphysis. J. Pediatr. Orthop. B 2003, 12, 369–371. [Google Scholar] [CrossRef]
- Azzopardi, T.; Sharma, S.; Bennet, G.C. Slipped Capital Femoral Epiphysis in Children Aged Less than 10 Years. J. Pediatr. Orthop. B 2010, 19, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Chatziravdeli, V.; Stefanou, M.; Pilichou, A.; Krallis, P.; Anastasopoulos, J. Early Onset Slipped Capital Femoral Epiphysis in Children under 10 Years Old. Surgical Treatment with Two Different Methods and Results. Hippokratia 2019, 23, 165–168. [Google Scholar]
- Fishkin, Z.; Armstrong, D.G.; Shah, H.; Patra, A.; Mihalko, W.M. Proximal Femoral Physis Shear in Slipped Capital Femoral Epiphysis—A Finite Element Study. J. Pediatr. Orthop. 2006, 26, 291–294. [Google Scholar] [CrossRef]
- Farzaneh, S.; Paseta, O.; Gómez-Benito, M.J. Multi-Scale Finite Element Model of Growth Plate Damage during the Development of Slipped Capital Femoral Epiphysis. Biomech. Model. Mechanobiol. 2015, 14, 371–385. [Google Scholar] [CrossRef]
- Mirkopulos, N.; Weiner, D.S.; Askew, M. The Evolving Slope of the Proximal Femoral Growth Plate Relationship to Slipped Capital Femoral Epiphysis. J. Pediatr. Orthop. 1988, 8, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Hosseinzadeh, S.; Novais, E.N.; Maranho, D.A.; Emami, S.A.; Portilla, G.; Kim, Y.-J.; Kiapour, A.M. Age- and Sex-Specific Morphologic Changes in the Metaphyseal Fossa Adjacent to Epiphyseal Tubercle in Children and Adolescents without Hip Disorders. J. Orthop. Res. 2020, 38, 2213–2219. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).