1. Introduction
Postoperative respiratory depression in patients undergoing anesthesia has risen to a renewed level of attention in recent years. In 2016, a national registry identified over 44,551 acute respiratory events across U.S. hospitals, with almost 40% resulting in mortality [
1]. The true incidence of opioid-induced respiratory depression is unknown. Still, it is believed to be higher than the reported values, between 0.3% and 21% of all post-surgical patients [
2]. In fact, Opioid-Induced Respiratory Depression events (OIRD) are associated with increased readmission (15.8% vs. 9.4% in patients without events), increased length of stay (5 additional days on average), and increased cost (
$10,000 on the average increase) [
3,
4]. Recent studies identified patients with one or more respiratory depression events had a more extended stay and higher hospital costs than those with no R.D. events [
5], Identifying those at risk for these events, such as those with OSA, and potentially mitigating this risk with low opioid anesthesia could improve outcomes associated with OIRD. A systematic review and meta-analysis showed an increased risk of OIRD in patients with pre-existing heart conditions, pulmonary disease, and OSA and had findings that those with OIRD received a higher dose of morphine equivalents [
6]. Respiratory events are challenging to observe and could be underreported without continuous monitoring, and non-critical, near-misses often go unnoticed.
In addition to the commonly used pulse oximetry, breath-by-breath capnography can detect respiratory depression before desaturation occurs, especially when supplemental oxygen is administered [
7]. Another study showed that continuous respiratory monitoring is much more effective at detecting respiratory depression than periodic vital checks [
8]. As these capnography devices become more cost-effective, they should be considered especially for high-risk populations, such as bariatric and obstructive sleep apnea (OSA) patients.
In a 2019 study, Khanna et al. [
2] suggested that hospitals could reduce the frequency and mortality of these respiratory depressive events using capnography to monitor respiration directly in patients at high risk. Thus, he introduced the PRODIGY scoring system to stratify an individual’s risk of experiencing respiratory depression. The risk factors in the PRODIGY scoring system are assigned different weights and include five patient characteristics: age, sex, previous opioid use, sleep-disordered breathing, and chronic heart failure. A value from 0 to 5 or from 0 to 8 for each factor is summed, yielding low risk (0 to 8), intermediate risk (9 to 15), or high risk (>15) for predicting respiratory adverse events.
We aimed to evaluate how PRODIGY scoring would predict the frequency of postoperative respiratory events in an at-risk population not previously studied—obese patients receiving bariatric surgery. Estimated incidence of OSA in bariatric surgery patients is as high as 70% [
9]. Due to the accepted strong correlations between obese patients and obstructive sleep apnea (OSA) as well as OSA and respiratory depression, we stratified our patients using OSA status and their PRODIGY score measured pre-surgery. We hypothesized that we would find more respiratory events (RE) in the OSA patient cohort and an increased incidence of RE in patients with higher PRODIGY scores. In addition, since OSA status was part of the PRODIGY score, we expected the data to reflect that OSA patients and patients in the high-risk PRODIGY category would have the most respiratory depressive events.
2. Methods
This study was IRB-approved by the University of South Florida IRB on 22 March 2021 with protocol number Pro00036836. Additionally, The study was recorded at the National Clinical Trials Registry with number NCT 03076047. The patient population included OSA and non-OSA patients studied using continuous surveillance of respiratory variables during postoperative recovery (PACU), after bariatric surgery (gastric bypass, gastric sleeve, and esophageal surgery), utilizing capnography and pulse oximetry (Capnostream 35, Medtronic Inc. (Dublin, Ireland) and Profox software (Coral Springs, FL, USA, 33076)). All patients were studied between May 2021 to April 2022. Inclusion criteria comprised patients between 18 and 80 years of age undergoing surgical gastric bypass, gastric sleeve, or esophageal surgery. Preoperative preparation included OSA evaluation for all patients, sleep studies for severe OSA grades, and evaluation of risk for respiratory depression (low, intermediate, or high) using the PRODIGY scoring.
The majority of patients studied who received gastric bypass or gastric sleeve surgery had been diagnosed with Obstructive Sleep Apnea (OSA) and was actively using a CPAP or nasal PAP during sleep. Patients with known OSA were required to comply with PAP therapy to qualify for surgery. PAP machine compliance was defined as >70% usage in the following categories: usage 5+ nights per week and use for 4+ hours a night; compliance maintenance was updated every 3 months in the preoperative period and again the week before surgery.
In addition, all patients received multimodal intraoperative non-opioid anesthesia—at our institution, low and no-opioid anesthesia is becoming the new standard for surgery. Despite the common usage of opioids, since our study builds upon the principles from Khanna [
2], we also applied the PRODIGY scoring system to all our study cohorts after data collection. We analyzed how the PRODIGY score stratifies bariatric OSA and non-OSA patients. They underwent bariatric surgery and esophageal hernia repairs with low-/no-opioid anesthesia as compared to stratification by OSA status alone.
Anesthesia management comprised Enoxaparin, oral gabapentin, acetaminophen and Decadron tablets (8 mg; 4 mg if diabetic), a scopolamine patch, and IV Famotidine 20 mg. Standard induction was with propofol/etomidate, lidocaine, paralytic agent, and oral intubation. Intraoperative opioid-sparing maintenance comprised dexmedetomidine 0.2–0.7 mcg/kg/hr, propofol 75–150 mcg/kg/min and ketamine 25 mg/hr for a max of 50 mg during the procedure. These medications were dosed based on the patient’s lean body weight. At emergence, patients received antiemetic agents: metoclopramide 10 mg, ondansetron 4 mg (if no Q.T. prolongation), and Benadryl 12.5–25 mg. Reversal agents consisted of Sugammadex for patients with BMI above 40 (2 mg/kg for 2 or more twitches via TOF, 4 mg/kg for <2 twitches via TOF). For patients with BMI below 40, we used neostigmine/glycopyrrolate. Toradol 15–30 mg provided further analgesia if not contraindicated. Postoperatively in the PACU, patients with an OSA diagnosis were placed on their home CPAP machine, or we provided a hospital machine with the same parameters. Postoperative narcotics were limited to fentanyl 12.5–25 mcg q 5 min for breakthrough pain with a max of 250 mcg, cyclobenzaprine 10 mg P.O. × 1 prn (decreased dose for the elderly), gabapentin 200 mg P.O. × 1 prn (decreased dose for renal dysfunction or the elderly), and magnesium chloride 128 mg P.O. × 1 prn (not for renal dysfunction).
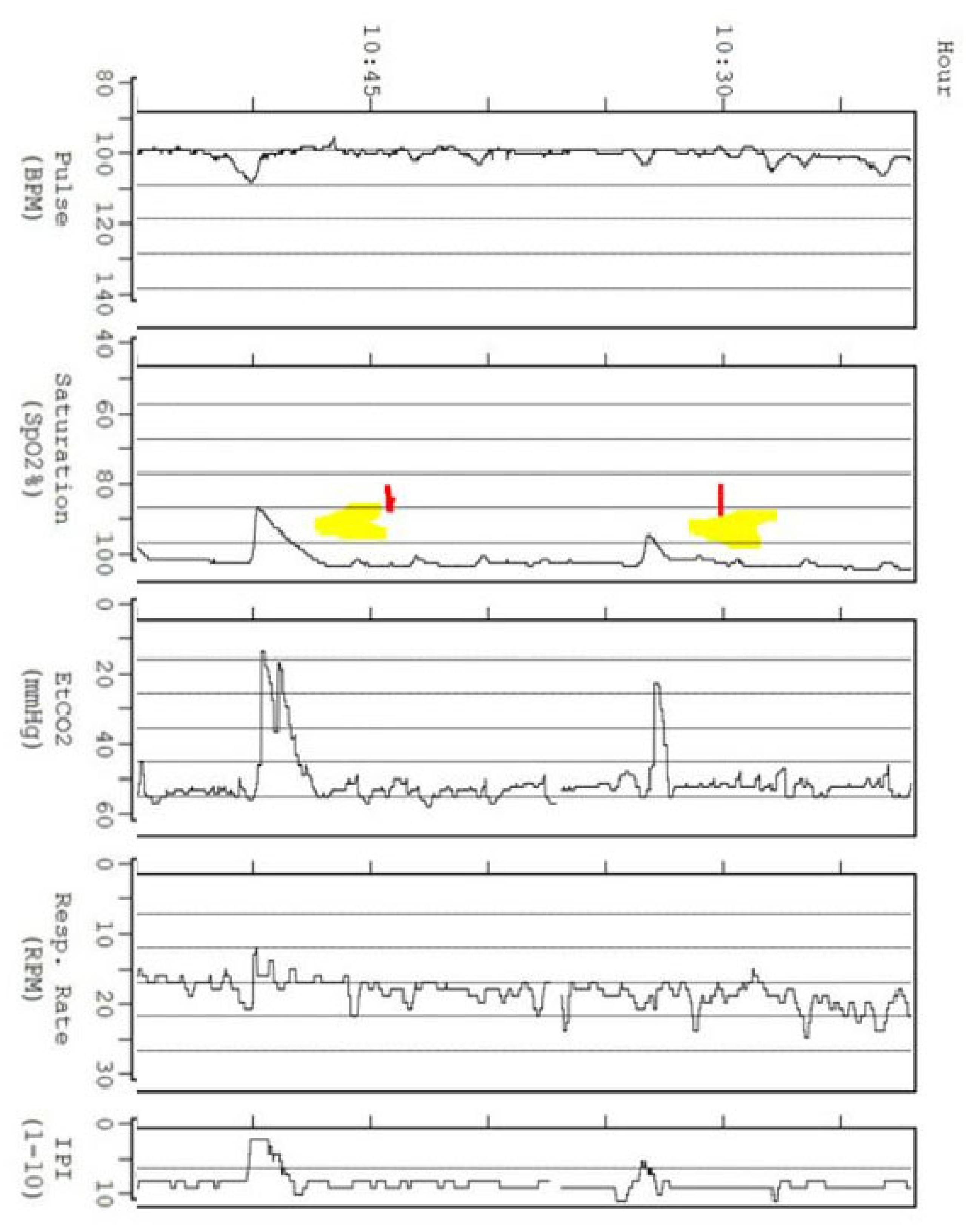
After surgery, all patients received continuous respiratory surveillance in PACU (average duration exceeding 140 min). Monitoring began in the PACU and continued through their transition to the general care floor. We used the same five events as described by Khanna [
2], but we shortened the duration for each event. Namely, we counted as an episode of respiratory depression any of the following: respiratory rate ≤5 breaths/min (bpm) for ≥20 s, oxygen saturation (Spo2) ≤85% for ≥20 s, end-tidal carbon dioxide (Etco2) ≤15 or ≥60 mm Hg for ≥20 s, apnea episode lasting >20 s, or any respiratory opioid-related adverse event [
2]. The events were measured by analysis of continuously recorded tracing of the respiratory variables, compiled by observers blinded to the patient attribution.
5. Discussion
A 2019 study by Chan et al. revealed that severe OSA patients were at a statistically significant elevation of risk for cardiovascular events (atrial fibrillation, stroke, thromboembolism, cardiac death, and congestive heart failure) within 30 days of surgery than non-OSA patients, 21.7% vs. 14.2% [
10]. A recent article analyzed OSA death and near miss registry data. The study found 76% of events occurred within 24 h of anesthesia, and 97% received opioids within 24 h of the event [
11]. The authors concluded that events resulting in death or brain damage were more likely to occur in patients who lacked respiratory monitoring, were not on supplemental oxygen, and had unwitnessed events [
11]. Yet another study, a meta-analysis of 20 prospective cohort studies encompassing 3756 patients, 2127 OSA patients and 1629 non-OSA patients, also recently arrived at similar conclusions. Data from the meta-analysis revealed OSA patients had almost double the risk of postoperative complications (Odds Ratio = 1.92, CI 95%
p < 0.001) [
12]. Patients across the 20 cohort studies had a 1.56 odds ratio (CI 95%,
p = 0.001) for cardiovascular events and a 1.91 odds ratio (CI 95%,
p < 0.001) for respiratory events when compared with non-OSA patients [
12]. Undiagnosed OSA patients have a higher risk of postoperative cardiovascular complications (2.20 [1.16 to 4.17],
p = 0.02) compared to diagnosed OSA patients (0.75 [0.43 to 1.28],
p = 0.29) [
13]. This emerging research emphasizes the need for additional precautions, diagnosis, and monitoring of this high-risk group in the postoperative period. Hence, we believed this population to be an excellent cohort for immediate postoperative capnography monitoring.
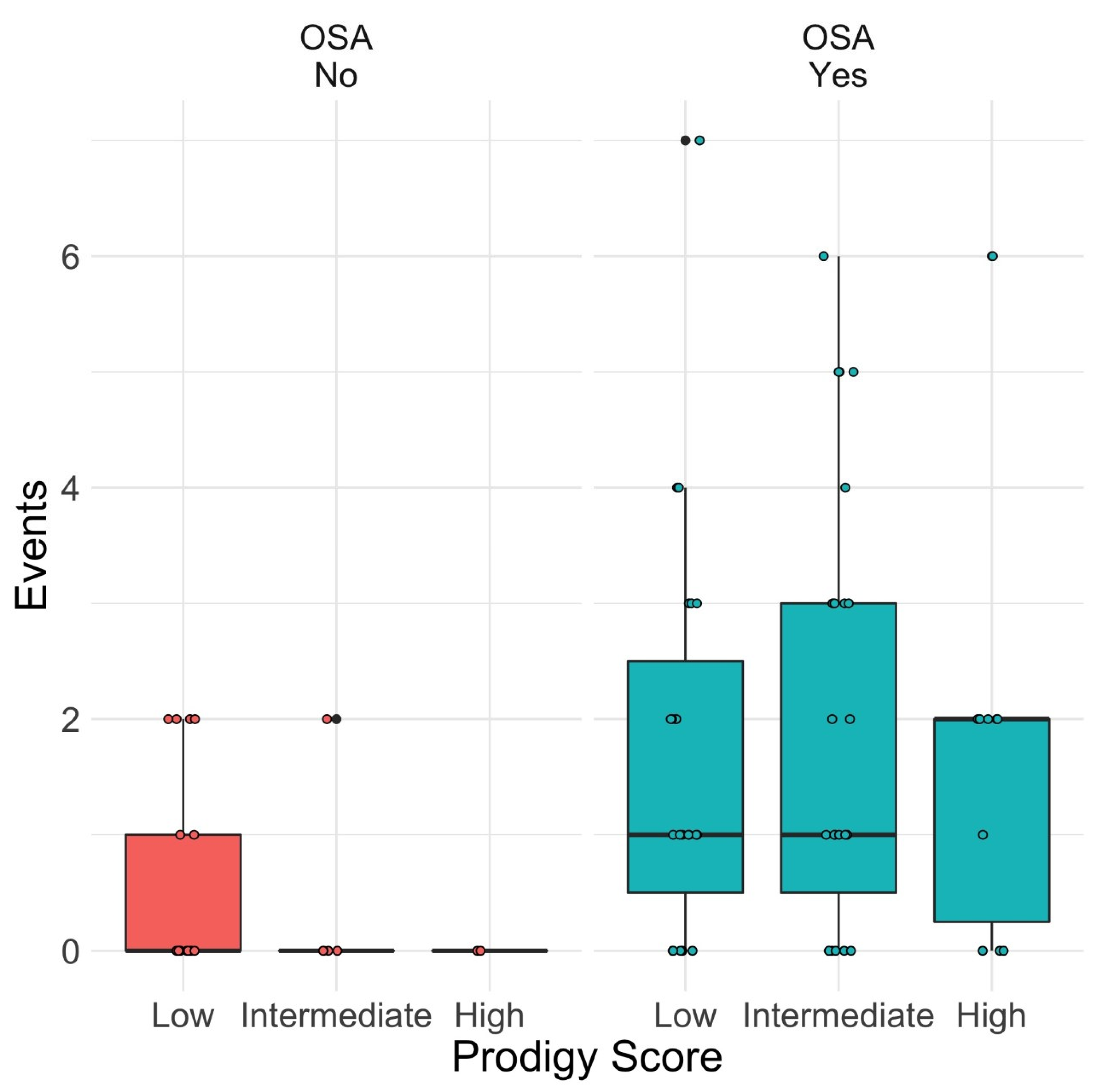
Our results support that OSA patients will manifest a significantly higher number of respiratory events than the non-OSA group. However, the RE frequency did not increase proportionally to a higher PRODIGY score in the OSA group, unlike Khanna’s [
2] description.
In observing patients early after surgery with capnography, no respiratory events occurred that required intervention to aid respiration for our patients. We suggest that the absence of events requiring intervention and the transient nature of the events observed, which differed from the events observed in Khanna’s study, could be attributed to several factors: preoperative patient optimization, head-up positioning, early CPAP utilization on admission to PACU, and especially the low peri- and postoperative narcotic utilization. In addition, in our study, the mean patient stay time in the hospital was less than 24 h post-surgery; most patients were discharged the day following their surgeries.
One of the differences from the previous group of studies was the observation period of postoperative monitoring. The survey from Weingarten et al. observed that a large portion of respiratory depressive events occurred in the hours following surgery and suggested, “the best practice would be the application of these monitors in the PACU.” [
14] Another study found that postoperative respiratory complications were more uncommon (1–2%) in patients without recurrent PACU events compared to patients with recurrent PACU events (11%) [
15]. These findings indicate the importance of capnography monitoring in the PACU period.
Another difference from previous reports was our use of low- or no-opioid anesthesia and low postoperative opioids for pain control. Prolonged recovery of bariatric surgery patients has a strong association with respiratory depression events and the use of opioid treatment. In a study of postoperative bariatric surgery patients, 38.9% had prolonged recovery (greater than 90 min in phase 1 recovery) with increased respiratory depression and opioid treatment [
16]. Seemingly, recovery times can be shortened by reducing opioid utilization. In the study by Khanna, the average patient with at least one OIRD received 15 milligrams of morphine equivalent (MMEs) on the general care floor, although MMEs intra-op and in the PACU are not mentioned [
2]. In our study, OSA patients were given an average of 4.8 MMEs intra-op, 8.2 MMEs in the PACU, and 10.7 MMEs on the general care floor, whereas non-OSA patients were given 9.0 MMEs intra-op, 9.8 MMEs in the PACU, and 11.9 MMEs on the general care floor. On average, OSA patients received 28.7% fewer opioids on the general care floor than in the PRODIGY study, and non-OSA received 20.7% less. A paper by Doug et al. demonstrated ventilatory chemosensitivity to opioids was an essential predictor of OIRD [
17]. These authors (Doug et al.) compared pre- and postoperative ventilatory chemosensitivity after patients received opioids and verified a reduced ventilatory response to hypoxia and CO
2, especially during sleep in the postoperative time [
17]. This factor could have contributed to the lack of respiratory events.
A possible reason for the lack of significant postoperative respiratory events (events requiring intervention or fitting Khanna’s original parameters of respiratory depression) may be that each patient underwent prolonged optimization before surgery. Most patients spent 6–12 months undergoing optimization for surgery, which consisted of weight loss, monitoring pulmonary function, and OSA evaluation. Patients were initially evaluated for OSA using the STOP-Bang Questionnaire, amongst other screening tools, which led to a possible referral to pulmonologists for a complete work-up, including polysomnography. OSA was screened for and treated before surgery with a personalized CPAP and monitored for usage and compliance. After completion of the surgery, OSA patients were immediately placed back onto CPAP machines upon arrival at the PACU.
Several studies have shown positive airway pressure after surgery improves respiratory functioning. For example, in 2013, Liao et al. examined how PAP usage postoperatively improves the apnea-hypopnea index (AHI) scores in patients with moderate and severe OSA. Their results were that patients who used PAP after surgery (
p = 87) had a decreased AHI score postoperatively (AHI 30.1 at baseline to 3.0,
p < 0.001), whereas OSA patients who did not receive PAP treatment after surgery had an increase from their baseline AHI of 30.4, to 31.9 (
p = 0.302) [
18]. In a more recent study, Zaremba et al. [
19] analyzed the usage of CPAP in bariatric patients after surgery. They also used the AHI to measure sleep-disordered breathing after surgery. They found that treatment with a CPAP decreased AHI (8/h vs. 25/h,
p < 0.001), reduced oxygen desaturations (5/h vs. 16/h,
p < 0.001), and increased mean oxygen saturation by 3% (
p = 0.003). A recent randomized crossover study by Sakaguchi et al. demonstrated the effectiveness of the combined application of high-flow nasal cannula and upper-body elevation to reduce OSA severity and nocturnal hypoxemia without using postoperative CPAP, which had a reduced patient acceptance [
20]. These factors may have contributed to the lack of respiratory depressive events and the transient nature of the events we observed.
Our study had several limitations. On average, patients were monitored with capnography only for two hours, beginning before discharge from the PACU, but patients were not monitored overnight. In addition, patients were not observed with capnography pre-operatively. Thus, patients did not have a baseline to determine whether abnormalities in breathing were pre-existing or worsened postoperatively. However, all monitored postoperative end-tidal PCO2 values ranged within acceptable values. The monitoring of the patients with capnography is also subject to artifact, depending on patient compliance and proper application of equipment. In adjudicating respiratory depressive episodes, subjectivity is present, which was minimized by observing patients in real-time. In addition, many of the events observed were transient, lasting only for 30–60 s before resolving spontaneously; none of the events required intervention.
Another limitation was the sample size of our study. Khanna’s original study had a population of 1335 patients who were monitored and whose data were collected. Our study was comprised of 80 patients monitored at our institution. Additionally, while we used the PRODIGY score to stratify our patients, this study diverged from the original PRODIGY methodology in decreasing respiratory depression duration requirements. In a complete absence of events lasting 3 min or greater, the durational requirements for which abnormal measurements were required to be classified as respiratory depressive events were reduced, in most cases, from 3 min or greater to 30 s. We did this to create quantifiable data which could be analyzed and compared. Finally, as mentioned in the methodology, this study monitored patients for over two hours, with capnography and pulse oximetry beginning in the PACU. This decision was based on the discussion in the paper by Driver et al., stating that earlier application of monitoring was optimal and could help to discover R.D. events earlier [
14]. In the original study by Khanna, capnography monitoring began several hours after their transfer to the general care floor and was continued for a median of 24 h [
2]. We believe that early capnography and detecting early events could be more helpful in predicting events on the general care floor.
In our study, the PRODIGY score was not predictive of OIRD. While a male sex and OSA status, elements of the PRODIGY study, correlated significantly with a more significant number of OIRD (
p = 0.01 and
p = 0.0003, respectively), other individual characteristics of the PRODIGY (such as age) and the PRODIGY score as a whole did not correlate with an increase in OIRD. As explained earlier, we attributed this to reduced intra- and postoperative opioids, early CPAP usage, and preoperative optimization of patients. In addition, we believe the same factors contributed to the self-resolving nature of the events we observed. Our decision to change the criteria from events lasting 3 min to events lasting only 20 s stemmed from our cohort’s brief, transient nature of respiratory depressive events; no patients monitored had respiratory depression lasting 3 min or greater. Finally, Khanna discusses how the PRODIGY score can reduce mortality, hospital stays, and costs; in our study, patients averaged less than 24 h from surgery before being discharged, and most patients were released home the following day [
2]. Based on the results of our study, we believe that the goals of reducing mortality, hospital costs, and respiratory depressive severity can be achieved through low- and no-opioid anesthesia and early CPAP usage. Using these factors can potentially mitigate risks for significant OIRD in patients deemed at greater risk via the PRODIGY score. However, additional data and more comprehensive monitoring are needed.







{kind=link}
{kind=link}