
Novel ML-Based Algorithm for Detecting Seizures from Single-Channel EEG


Abstract
1. Introduction
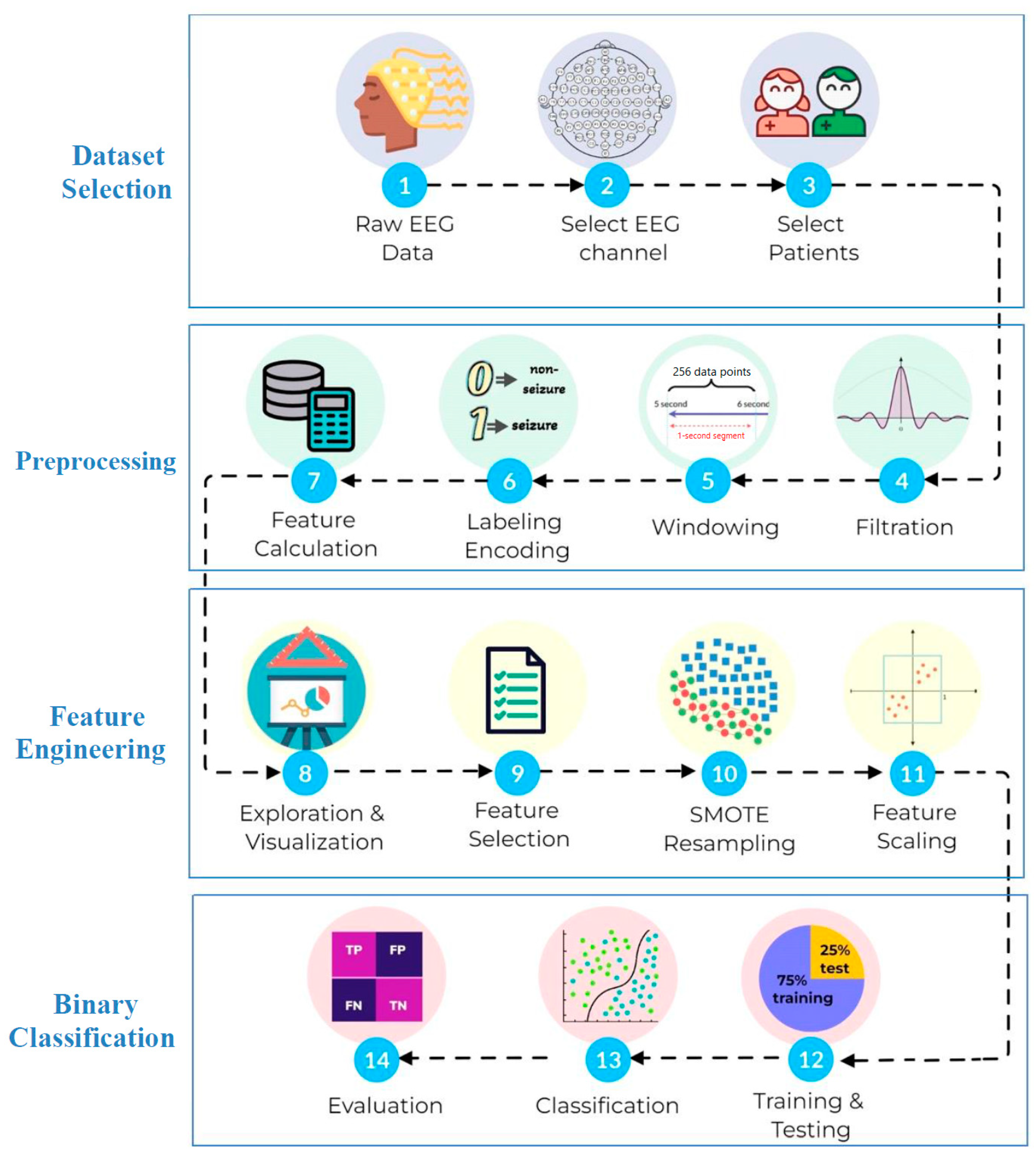
2. Materials and Methods
2.1. Dataset
2.2. Data Preprocessing
2.3. Classification
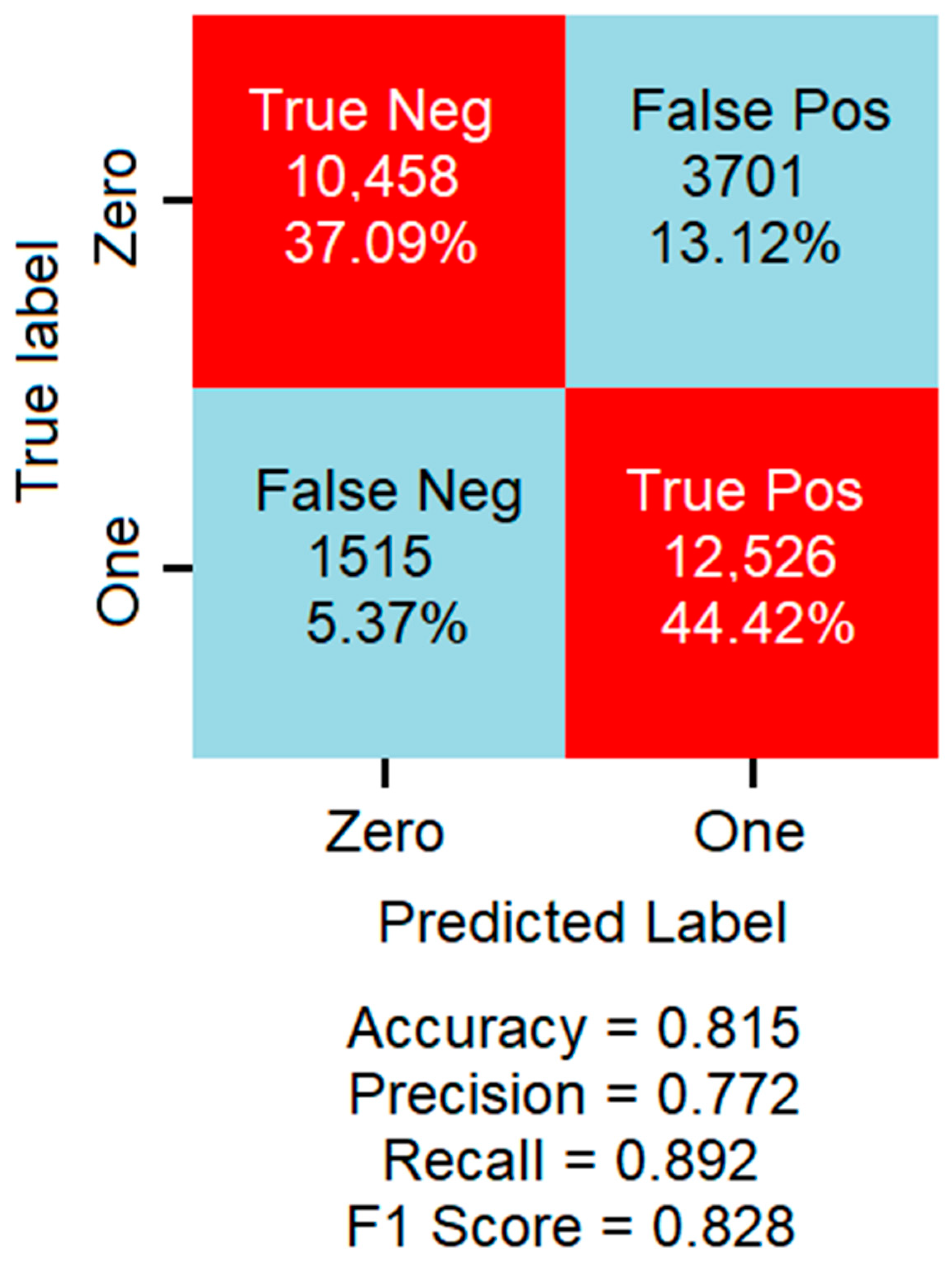
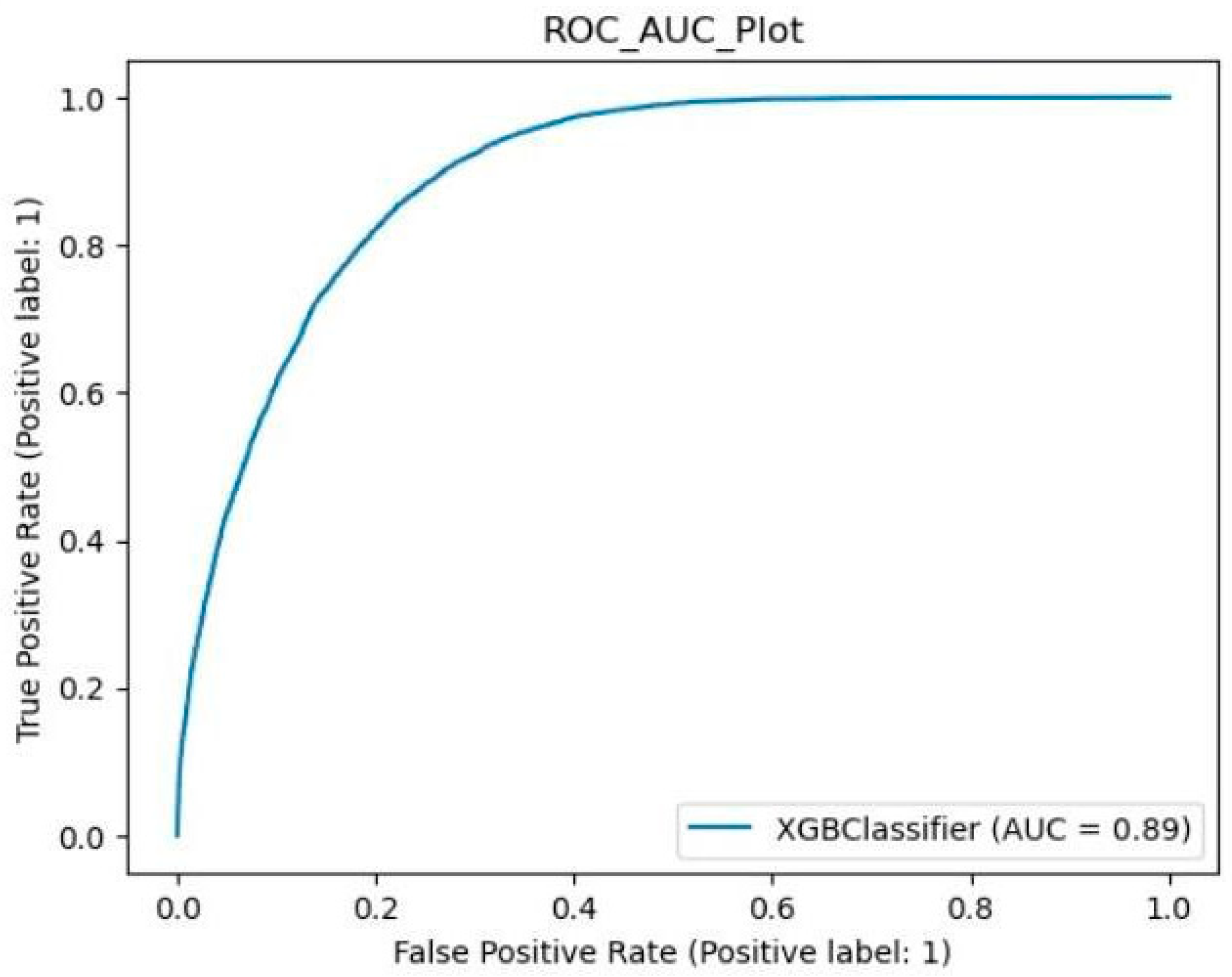
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Features Formulae
References
- Stafstrom, C.E.; Carmant, L. Seizures and epilepsy: An overview for neuroscientists. Cold Spring Harb. Perspect. Med. 2015, 5, a022426. [Google Scholar] [CrossRef]
- Kuzniecky, R.I. Neuroimaging of epilepsy: Therapeutic implications. NeuroRx 2005, 2, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Wyllie, E.; Cascino, G.D.; Gidal, B.E.; Goodkin, H.P. Wyllie’s Treatment of Epilepsy: Principles and Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- González, F.L.; Osorio, X.R.; Rein, A.G.N.; Martínez, M.C.; Fernández, J.S.; Haba, V.V.; Pedraza, A.D.; Cerdá, J. Drug-resistant epilepsy: Definition and treatment alternatives. Neurol. Engl. Ed. 2015, 30, 439–446. [Google Scholar] [CrossRef]
- Schmitt, B. Sleep and epilepsy syndromes. Neuropediatrics 2015, 46, 171–180. [Google Scholar] [CrossRef]
- Kostopoulos, G.K.; Koutroumanidis, M. Brain mechanisms linking epilepsy to sleep. In Reference Module in Neuroscience and Biobehavioral Psychology; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Elger, C.E.; Hoppe, C. Diagnostic challenges in epilepsy: Seizure under-reporting and seizure detection. Lancet Neurol. 2018, 17, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, C.; Poepel, A.; Elger, C.E. Epilepsy: Accuracy of patient seizure counts. Arch. Neurol. 2007, 64, 1595–1599. [Google Scholar] [CrossRef] [PubMed]
- Purnell, B.S.; Thijs, R.D.; Buchanan, G.F. Dead in the night: Sleep-wake and time-of-day influences on sudden unexpected death in epilepsy. Front. Neurol. 2018, 9, 1079. [Google Scholar] [CrossRef]
- Kloster, R.; Engelskjøn, T. Sudden unexpected death in epilepsy (SUDEP): A clinical perspective and a search for risk factors. J. Neurol. Neurosurg. Psychiatry 1999, 67, 439–444. [Google Scholar] [CrossRef]
- Ulate-Campos, A.; Coughlin, F.; Gaínza-Lein, M.; Fernández, I.S.; Pearl, P.; Loddenkemper, T. Automated seizure detection systems and their effectiveness for each type of seizure. Seizure 2016, 40, 88–101. [Google Scholar] [CrossRef]
- Smith, S.J.M. EEG in the diagnosis, classification, and management of patients with epilepsy. J. Neurol. Neurosurg. Psychiatry 2005, 76 (Suppl. S1), ii2–ii7. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Sperling, M.R. Normal awake, drowsy, and sleep EEG patterns that might be overinterpreted as abnormal. J. Clin. Neurophysiol. 2019, 36, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Maganti, R.K.; Rutecki, P. EEG and epilepsy monitoring. CONTINUUM Lifelong Learn. Neurol. 2013, 19, 598–622. [Google Scholar] [CrossRef] [PubMed]
- Maturana, M.I.; Meisel, C.; Dell, K.; Karoly, P.J.; D’souza, W.; Grayden, D.B.; Burkitt, A.N.; Jiruska, P.; Kudlacek, J.; Hlinka, J.; et al. Critical slowing down as a biomarker for seizure susceptibility. Nat. Commun. 2020, 11, 2172. [Google Scholar] [CrossRef] [PubMed]
- Jin, B.; Aung, T.; Geng, Y.; Wang, S. Epilepsy and its interaction with sleep and circadian rhythm. Front. Neurol. 2020, 11, 327. [Google Scholar] [CrossRef]
- Ramgopal, S.; Thome-Souza, S.; Jackson, M.; Kadish, N.E.; Fernández, I.S.; Klehm, J.; Bosl, W.; Reinsberger, C.; Schachter, S.; Loddenkemper, T. Seizure detection, seizure prediction, and closed-loop warning systems in epilepsy. Epilepsy Behav. 2014, 37, 291–307. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Thijs, R.D.; Gutter, T.; Ungureanu, C.; Cluitmans, P.; Van Dijk, J.; van Andel, J. Multimodal nocturnal seizure detection in a residential care setting: A long-term prospective trial. Neurology 2018, 91, e2010–e2019. [Google Scholar] [CrossRef] [PubMed]
- Duun-Henriksen, J.; Baud, M.; Richardson, M.P.; Cook, M.; Kouvas, G.; Heasman, J.M.; Friedman, D.; Peltola, J.; Zibrandtsen, I.C.; Kjaer, T.W. A new era in electroencephalographic monitoring? Subscalp devices for ultra–long-term recordings. Epilepsia 2020, 61, 1805–1817. [Google Scholar] [CrossRef]
- Schad, A.; Schindler, K.; Schelter, B.; Maiwald, T.; Brandt, A.; Timmer, J.; Schulze-Bonhage, A. Application of a multivariate seizure detection and prediction method to non-invasive and intracranial long-term EEG recordings. Clin. Neurophysiol. 2008, 119, 197–211. [Google Scholar] [CrossRef]
- Gu, Y.; Cleeren, E.; Dan, J.; Claes, K.; Van Paesschen, W.; Van Huffel, S.; Hunyadi, B. Comparison between scalp EEG and behind-the-ear EEG for development of a wearable seizure detection system for patients with focal epilepsy. Sensors 2017, 18, 29. [Google Scholar] [CrossRef]
- You, S.; Cho, B.H.; Yook, S.; Kim, J.Y.; Shon, Y.M.; Seo, D.W.; Kim, I.Y. Unsupervised automatic seizure detection for focal-onset seizures recorded with behind-the-ear EEG using an anomaly-detecting generative adversarial network. Comput. Methods Programs Biomed. 2020, 193, 105472. [Google Scholar] [CrossRef]
- Vandecasteele, K.; De Cooman, T.; Dan, J.; Cleeren, E.; Van Huffel, S.; Hunyadi, B.; Van Paesschen, W. Visual seizure annotation and automated seizure detection using behind-the-ear electroencephalographic channels. Epilepsia 2020, 61, 766–775. [Google Scholar] [CrossRef]
- Becker, T.; Vandecasteele, K.; Chatzichristos, C.; Van Paesschen, W.; Valkenborg, D.; Van Huffel, S.; De Vos, M. Classification with a deferral option and low-trust filtering for automated seizure detection. Sensors 2021, 21, 1046. [Google Scholar] [CrossRef]
- Paul, Y. Various epileptic seizure detection techniques using biomedical signals: A review. Brain Inform. 2018, 5, 6. [Google Scholar] [CrossRef]
- Wang, L.; Xue, W.; Li, Y.; Luo, M.; Huang, J.; Cui, W.; Huang, C. Automatic epileptic seizure detection in EEG signals using multi-domain feature extraction and nonlinear analysis. Entropy 2017, 19, 222. [Google Scholar] [CrossRef]
- Boonyakitanont, P.; Lek-Uthai, A.; Chomtho, K.; Songsiri, J. A review of feature extraction and performance evaluation in epileptic seizure detection using EEG. Biomed. Signal Process. Control 2019, 57, 101702. [Google Scholar] [CrossRef]
- Güler, N.F.; Übeyli, E.D.; Güler, I. Recurrent neural networks employing Lyapunov exponents for EEG signals classification. Expert Syst. Appl. 2005, 29, 506–514. [Google Scholar] [CrossRef]
- Peachap, A.B.; Tchiotsop, D. Epileptic seizures detection based on some new Laguerre polynomial wavelets, artificial neural networks and support vector machines. Inform. Med. Unlocked 2019, 16, 100209. [Google Scholar] [CrossRef]
- Andrzejak, R.G.; Lehnertz, K.; Mormann, F.; Rieke, C.; David, P.; Elger, C.E. Indications of nonlinear deterministic and finite-dimensional structures in time series of brain electrical activity: Dependence on recording region and brain state. Phys. Rev. E 2001, 64, 061907. [Google Scholar] [CrossRef] [PubMed]
- Acharya, U.R.; Oh, S.L.; Hagiwara, Y.; Tan, J.H.; Adeli, H. Deep convolutional neural network for the automated detection and diagnosis of seizure using EEG signals. Comput. Biol. Med. 2018, 100, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Nasehi, S.; Pourghassem, H. Patient-specific epileptic seizure onset detection algorithm based on spectral features and IPSONN classifier. In Proceedings of the 2013 International Conference on Communication Systems and Network Technologies (CSNT 2013), Gwalior, India, 6–8 April 2013; pp. 186–190. [Google Scholar]
- Satapathy, S.K.; Dehuri, S.; Jagadev, A.K. EEG signal classification using PSO trained RBF neural network for epilepsy identification. Inform. Med. Unlocked 2017, 6, 1–11. [Google Scholar] [CrossRef]
- Aleksander, I.; De Gregorio, M.; Galvao França, F.M.; Vieira Lima, P.M.; Morton, H. A brief introduction to weightless neural systems. In Proceedings of the ESANN—2009 Proceedings, European Symposium on Artificial Neural Networks-Advances in Computational Intelligence and Learning, Bruges, Belgium, 22–24 April 2009; pp. 299–305. [Google Scholar]
- De Aguiar, K.; França, F.M.; Barbosa, V.C.; Teixeira, C.A. Early detection of epilepsy seizures based on a weightless neural network. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 4470–4474. [Google Scholar]
- Ayodele, K.P.; Ikezogwo, W.O.; Komolafe, M.A.; Ogunbona, P. Supervised domain generalization for integration of disparate scalp EEG datasets for automatic epileptic seizure detection. Comput. Biol. Med. 2020, 120, 103757. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Ma, Y.; Chen, C.; Wang, Y. Classification of single-channel EEG signals for epileptic seizures detection based on hybrid features. Technol. Health Care 2018, 26, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Bergstrom, R.A.; Choi, J.H.; Manduca, A.; Shin, H.-S.; Worrell, G.A.; Howe, C.L. Automated identification of multiple seizure-related and interictal epileptiform event types in the EEG of mice. Sci. Rep. 2013, 3, 1483. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.H. Greedy function approximation: A gradient boosting machine. Ann. Stat. 2001, 29, 1189–1232. [Google Scholar] [CrossRef]
- Tianqi, C.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Ciurea, A.; Manoila, C.-P.; Tautan, A.-M.; Ionescu, B. Low latency automated epileptic seizure detection: Individualized vs. Global approaches. In Proceedings of the 2020 International Conference on e-Health and Bioengineering (EHB), Iasi, Romania, 29–30 October 2020; pp. 1–4. [Google Scholar]
- Wu, J.; Zhou, T.; Li, T. Detecting epileptic seizures in EEG signals with complementary ensemble empirical mode decomposition and extreme gradient boosting. Entropy 2020, 22, 140. [Google Scholar] [CrossRef] [PubMed]
- Long, J.-M.; Yan, Z.-F.; Shen, Y.-L.; Liu, W.-J.; Wei, Q.-Y. Detection of epilepsy using MFCC-based feature and XGBoost. In Proceedings of the 2018 11th International Congress on Image and Signal Processing, BioMedical Engineering and Informatics (CISP-BMEI), Beijing, China, 13–15 October 2018; pp. 1–4. [Google Scholar]
- Shoeb, A.H. Application of Machine Learning to Epileptic Seizure Onset Detection and Treatment. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2009. [Google Scholar]
- Krook-Magnuson, E.; Armstrong, C.; Oijala, M.; Soltesz, I. On-demand optogenetic control of spontaneous seizures in temporal lobe epilepsy. Nat. Commun. 2013, 4, 1376. [Google Scholar] [CrossRef] [PubMed]
- Sahani, M.; Rout, S.K.; Dash, P.K. FPGA implementation of epileptic seizure detection using semisupervised reduced deep convolutional neural network. Appl. Soft Comput. 2021, 110, 107639. [Google Scholar] [CrossRef]
- Zabihi, M.; Kiranyaz, S.; Rad, A.B.; Katsaggelos, A.K.; Gabbouj, M.; Ince, T. Analysis of high-dimensional phase space via poincaré section for patient-specific seizure detection. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 24, 386–398. [Google Scholar] [CrossRef]
- Sopic, D.; Aminifar, A.; Atienza, D. e-glass: A wearable system for real-time detection of epileptic seizures. In Proceedings of the 2018 IEEE International Symposium on Circuits and Systems (ISCAS), Florence, Italy, 27–30 May 2018; pp. 1–5. [Google Scholar]
- Wei, Z.; Zou, J.; Zhang, J.; Xu, J. Automatic epileptic EEG detection using convolutional neural network with improvements in time-domain. Biomed. Signal Process. Control 2019, 53, 101551. [Google Scholar] [CrossRef]
- Liang, W.; Pei, H.; Cai, Q.; Wang, Y. Scalp EEG epileptogenic zone recognition and localization based on long-term recurrent convolutional network. Neurocomputing 2019, 396, 569–576. [Google Scholar] [CrossRef]
- Hu, X.; Yuan, S.; Xu, F.; Leng, Y.; Yuan, K.; Yuan, Q. Scalp EEG classification using deep Bi-LSTM network for seizure detection. Comput. Biol. Med. 2020, 124, 103919. [Google Scholar] [CrossRef]
- Temkin, O. The Falling Sickness: A History of Epilepsy from the Greeks to the Beginnings of Modern Neurology; JHU Press: Baltimore, MD, USA, 1994. [Google Scholar]
- Ng, M.; Pavlova, M. Why are seizures rare in rapid eye movement sleep? Review of the frequency of seizures in different sleep stages. Epilepsy Res. Treat. 2013, 2013, 932790. [Google Scholar] [CrossRef] [PubMed]
- Gibbon, F.M.; Maccormac, E.; Gringras, P. Sleep and epilepsy: Unfortunate bedfellows. Arch. Dis. Child. 2019, 104, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Kotagal, P.; Yardi, N. The Relationship Between Sleep and Epilepsy. Semin. Pediatr. Neurol. 2008, 15, 42–49. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. | Patient | Gender | Age | Seizures (s) |
|---|---|---|---|---|
| 1 | chb-02 | M | 11 | 184 |
| 2 | chb-04 | M | 22 | 400 |
| 3 | chb-05 | F | 7 | 524 |
| 4 | chb-07 | F | 14.5 | 340 |
| 5 | chb-09 | F | 10 | 296 |
| 6 | chb-11 | F | 12 | 816 |
| 7 | chb-14 | F | 9 | 177 |
| 8 | chb-15 | M | 16 | 2012 |
| 9 | chb-16 | F | 7 | 77 |
| 10 | chb-17 | F | 12 | 296 |
| 11 | chb-19 | F | 19 | 239 |
| 12 | chb-20 | F | 6 | 302 |
| Reference | Channel Count | Window Length | Features (Input Shape) | Feature Domain | Classification | Sensitivity |
|---|---|---|---|---|---|---|
| Zabihi 2016 [47] | 23 | 1 s | 7 features | Non-Linear | LDA and NB | 88.27% |
| Sopic 2018 [48] | 2 | 4 s | 7 features | Nonlinear and Power | Random Forest | 93.80% |
| Wei 2019 [49] | 23 | 5 s | Waveform image (1280 × 23 × 1) | Time | CNN | 72.11% |
| Ayodele 2020 [36] | 8 | 5 s | 17 10-layer 16 × 16 raster arrays | Frequency | RNN | 71.45% |
| Liang 2020 [50] | 18 | 2 s | waveform image (100 × 227 × 1) | Time | LRCN | 84.00% |
| Hu 2020 [51] | 23 | 4 s | 10 features | Non-Linear | Bi-LSTM | 93.61% |
| Proposed Approach | 1 | 1 s | 3 features | Time | XGBoost | 89.21% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dweiri, Y.M.; Al-Omary, T.K. Novel ML-Based Algorithm for Detecting Seizures from Single-Channel EEG. NeuroSci 2024, 5, 59-70. https://doi.org/10.3390/neurosci5010004
Dweiri YM, Al-Omary TK. Novel ML-Based Algorithm for Detecting Seizures from Single-Channel EEG. NeuroSci. 2024; 5(1):59-70. https://doi.org/10.3390/neurosci5010004
Chicago/Turabian StyleDweiri, Yazan M., and Taqwa K. Al-Omary. 2024. "Novel ML-Based Algorithm for Detecting Seizures from Single-Channel EEG" NeuroSci 5, no. 1: 59-70. https://doi.org/10.3390/neurosci5010004
APA StyleDweiri, Y. M., & Al-Omary, T. K. (2024). Novel ML-Based Algorithm for Detecting Seizures from Single-Channel EEG. NeuroSci, 5(1), 59-70. https://doi.org/10.3390/neurosci5010004