
Vitamin D Deficiency in Orthopedic Patients in Different Latitudes—First Study Comparing German and Greek Populations

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maier, G.S.; Jakobs, P.; Roth, K.E.; Kurth, A.A.; Maus, U. Is there an epidemic vitamin D deficiency in German orthopaedic patients? Clin. Orthop. Relat. Res. 2013, 471, 3029–3035. [Google Scholar] [CrossRef] [PubMed]
- Grossman, D.C.; Curry, S.J.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; Krist, A.H.; et al. Vitamin D, Calcium, or Combined Supplementation for the Primary Prevention of Fractures in Community-Dwelling Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 319, 1592–1599. [Google Scholar] [PubMed]
- Zhao, J.-G.; Zeng, X.-T.; Wang, J.; Liu, L. Association Between Calcium or Vitamin D Supplementation and Fracture Incidence in Community-Dwelling Older Adults: A Systematic Review and Meta-analysis. JAMA 2017, 318, 2466–2482. [Google Scholar] [CrossRef] [PubMed]
- Wacker, M.; Holick, M.F. Vitamin D—Effects on skeletal and extraskeletal health and the need for supplementation. Nutrients 2013, 5, 111–148. [Google Scholar] [CrossRef] [PubMed]
- Goltzman, D. Functions of vitamin D in bone. Histochem. Cell Biol. 2018, 149, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Carrillo-Cruz, E.; Montero, I.; Perez-Simon, J.A. Vitamin D: Effect on Haematopoiesis and Immune System and Clinical Applications. Int. J. Mol. Sci. 2018, 19, 2663. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Zhu, X.; Gu, L.; Zhan, Y.; Chen, L.; Li, X. Association Between Vitamin D and Influenza: Meta-Analysis and Systematic Review of Randomized Controlled Trials. Front. Nutr. 2021, 8, 799709. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef]
- Entrenas Castillo, M.; Entrenas Costa, L.M.; Vaquero Barrios, J.M.; Alcalá Díaz, J.F.; López Miranda, J.; Bouillon, R.; Quesada Gomez, J.M. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef]
- Geng, C.; Shaikh, A.S.; Han, W.; Chen, D.; Guo, Y.; Jiang, P. Vitamin D and depression: Mechanisms, determination and application. Asia Pac. J. Clin. Nutr. 2019, 28, 689–694. [Google Scholar]
- Cosentino, N.; Campodonico, J.; Milazzo, V.; de Metrio, M.; Brambilla, M.; Camera, M.; Marenzi, G. Vitamin D and Cardiovascular Disease: Current Evidence and Future Perspectives. Nutrients 2021, 13, 3603. [Google Scholar] [CrossRef] [PubMed]
- Charoenngam, N.; Shirvani, A.; Holick, M.F. Vitamin D for skeletal and non-skeletal health: What we should know. J. Clin. Orthop. Trauma 2019, 10, 1082–1093. [Google Scholar] [CrossRef] [PubMed]
- de La Puente Yagüe, M.; Collado Yurrita, L.; Ciudad Cabañas, M.J.; Cuadrado Cenzual, M.A. Role of Vitamin D in Athletes and Their Performance: Current Concepts and New Trends. Nutrients 2020, 12, 579. [Google Scholar] [CrossRef] [PubMed]
- de Martinis, M.; Allegra, A.; Sirufo, M.M.; Tonacci, A.; Pioggia, G.; Raggiunti, M.; Ginaldi, L.; Gangemi, S. Vitamin D Deficiency, Osteoporosis and Effect on Autoimmune Diseases and Hematopoiesis: A Review. Int. J. Mol. Sci. 2021, 22, 8855. [Google Scholar] [CrossRef]
- Chevalley, T.; Brandi, M.L.; Cashman, K.D.; Cavalier, E.; Harvey, N.C.; Maggi, S.; Cooper, C.; Al-Daghri, N.; Bock, O.; Bruyère, O.; et al. Role of vitamin D supplementation in the management of musculoskeletal diseases: Update from an European Society of Clinical and Economical Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases [ESCEO] working group. Aging Clin. Exp. Res. 2022, 34, 2603–2623. [Google Scholar] [CrossRef]
- Giustina, A.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Lazaretti-Castro, M.; Lips, P.; Marcocci, C.; Bilezikian, J.P. Vitamin D in the older population: A consensus statement. Endocrine 2022, 79, 31–44. [Google Scholar] [CrossRef]
- Gallagher, J.C. Vitamin D and aging. Endocrinol. Metab. Clin. N. Am. 2013, 42, 319–332. [Google Scholar] [CrossRef]
- Caccamo, D.; Ricca, S.; Currò, M.; Ientile, R. Health Risks of Hypovitaminosis D: A Review of New Molecular Insights. Int. J. Mol. Sci. 2018, 19, 892. [Google Scholar] [CrossRef]
- Lamberg-Allardt, C. Vitamin D in foods and as supplements. Prog. Biophys. Mol. Biol. 2006, 92, 33–38. [Google Scholar] [CrossRef]
- Jungert, A.; Neuhäuser-Berthold, M. Dietary vitamin D intake is not associated with 25-hydroxyvitamin D3 or parathyroid hormone in elderly subjects, whereas the calcium-to-phosphate ratio affects parathyroid hormone. Nutr. Res. 2013, 33, 661–667. [Google Scholar] [CrossRef]
- Mithal, A.; Wahl, D.A.; Bonjour, J.-P.; Burckhardt, P.; Dawson-Hughes, B.; Eisman, J.A.; El-Hajj Fuleihan, G.; Josse, R.G.; Lips, P.; Morales-Torres, J. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int. 2009, 20, 1807–1820. [Google Scholar] [CrossRef]
- Glowacki, J.; Hurwitz, S.; Thornhill, T.S.; Kelly, M.; LeBoff, M.S. Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J. Bone Jt. Surg. 2003, 85, 2371–2377. [Google Scholar] [CrossRef]
- Foo, L.H.; Zhang, Q.; Zhu, K.; Ma, G.; Trube, A.; Greenfield, H.; Fraser, D.R. Relationship between vitamin D status, body composition and physical exercise of adolescent girls in Beijing. Osteoporos. Int. 2009, 20, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Hill, T.R.; Cotter, A.A.; Mitchell, S.; Boreham, C.A.; Dubitzky, W.; Murray, L.; Strain, J.J.; Flynn, A.; Robson, P.J.; Wallace, J.M.W.; et al. Vitamin D status and its determinants in adolescents from the Northern Ireland Young Hearts 2000 cohort. Br. J. Nutr. 2008, 99, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Hintzpeter, B.; Mensink, G.B.M.; Thierfelder, W.; Müller, M.J.; Scheidt-Nave, C. Vitamin D status and health correlates among German adults. Eur. J. Clin. Nutr. 2008, 62, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- Kechichian, E.; Ezzedine, K. Vitamin D and the Skin: An Update for Dermatologists. Am. J. Clin. Dermatol. 2018, 19, 223–235. [Google Scholar] [CrossRef]
- Smith, N.; Sievert, L.L.; Muttukrishna, S.; Begum, K.; Murphy, L.; Sharmeen, T.; Gunu, R.; Chowdhury, O.; Bentley, G.R. Mismatch: A comparative study of vitamin D status in British-Bangladeshi migrants. Evol. Med. Public Health 2021, 9, 164–173. [Google Scholar] [CrossRef]
- Schilling, S. Epidemic vitamin D deficiency among patients in an elderly care rehabilitation facility. Dtsch. Arztebl. Int. 2012, 109, 33–38. [Google Scholar] [CrossRef]
- Moon, A.S.; Boudreau, S.; Mussell, E.; He, J.K.; Brabston, E.W.; Ponce, B.A.; Momaya, A.M. Current concepts in vitamin D and orthopaedic surgery. Orthop. Traumatol. Surg. Res. OTSR 2019, 105, 375–382. [Google Scholar] [CrossRef]
- Jones, G. Interpreting vitamin D assay results: Proceed with caution. Clin. J. Am. Soc. Nephrol. CJASN 2015, 10, 331–334. [Google Scholar] [CrossRef]
- Hollis, B.W. Circulating 25-hydroxyvitamin D levels indicative of vitamin D sufficiency: Implications for establishing a new effective dietary intake recommendation for vitamin D. J. Nutr. 2005, 135, 317–322. [Google Scholar] [CrossRef]
- Grant, W.B.; Holick, M.F. Benefits and requirements of vitamin D for optimal health: A review. Altern. Med. Rev. J. Clin. Ther. 2005, 10, 94–111. [Google Scholar]
- Scharla, S.H. Prevalence of subclinical vitamin D deficiency in different European countries. Osteoporos. Int. 1998, 8 (Suppl. S2), S7–S12. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P.; Sitbon, J.; Dubory, A.; Auregan, J.C. Vitamin D history part III: The “modern times”-new questions for orthopaedic practice: Deficiency, cell therapy, osteomalacia, fractures, supplementation, infections. Int. Orthop. 2019, 43, 1755–1771. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, I.; Hiraiwa, H.; Ishizuka, S.; Kawai, R.; Hoshino, Y.; Kusaka, Y.; Tsukahara, T. Comparison of vitamin D sufficiency between indoor and outdoor elite male collegiate athletes. Nagoya J. Med. Sci. 2021, 83, 219–226. [Google Scholar]
- Priemel, M.; von Domarus, C.; Klatte, T.O.; Kessler, S.; Schlie, J.; Meier, S.; Proksch, N.; Pastor, F.; Netter, C.; Streichert, T.; et al. Bone mineralization defects and vitamin D deficiency: Histomorphometric analysis of iliac crest bone biopsies and circulating 25-hydroxyvitamin D in 675 patients. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2010, 25, 305–312. [Google Scholar] [CrossRef]
- Smith, J.M.; Cancienne, J.M.; Brockmeier, S.F.; Werner, B.C. Vitamin D deficiency and total shoulder arthroplasty complications. Shoulder Elb. 2021, 13, 99–105. [Google Scholar] [CrossRef]
- Jamal, A.B.; Hasan Khan, M.N.; Sadiq, M. Intertrochanteric Hip Fractures And Vitamin D Deficiency; A Significant Association. J. Ayub Med. Coll. Abbottabad JAMC 2021, 33, 257–261. [Google Scholar]
- Webb, A.R. Who, what, where and when-influences on cutaneous vitamin D synthesis. Prog. Biophys. Mol. Biol. 2006, 92, 17–25. [Google Scholar] [CrossRef]
- Sizar, O.; Khare, S.; Goyal, A.; Bansal, P.; Givler, A. StatPearls. In Vitamin D Deficiency; StatPearls Publishing LLC: Treasure Island, FL, USA, 2021. [Google Scholar]
- Rizzoli, R. Vitamin D supplementation: Upper limit for safety revisited? Aging Clin. Exp. Res. 2021, 33, 19–24. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Both Groups | Group Regensburg | Group Patras | |||
|---|---|---|---|---|---|
| 25-OH-D mean value (Sign.) | 25-OH-D mean value (Sign.) | ||||
| Patients (n) | 1000 | 500 | - | 500 | |
| Men (n) | 433 (43.3%) | 230 (46%) | 17.70 | 204 (40.7%) | 18.20 |
| Women (n) | 567 (56.7%) | 270 (54%) | 18.10 | 297 (59.3%) | 18.40 |
| Age (years) | 59 (SD ±± 18.2) | 60 (SD ±± 18.1) | - | 59 (SD ±± 18.2) | |
| Osteoporosis | 165 (16.5%) | 57 (11.4%) | 23.50 | 108 (21.6%) | 23.95 |
| Obesity (BMI) | 248 (24.8%) | 133 (26.7%) | 16.00 | 115 (23%) | 15.40 |
| Thyroid disease | 129 (12.9%) | 64 (12.8%) | 16 | 65 (13%) | 17.60 |
| Psychiatric diseases | 171 (17.1%) | 91 (18.2%) | 16.9 | 80 (16%) | 18.15 |
| Infectious diseases | 24 (2.4%) | 13 (2.6%) | 15.50 | 11 (2.2%) | 16.40 |
| Renal failure | 92 (9.2%) | 57 (11.4%) | 17.80 | 35 (7%) | 14.60 |
| Pulmonary disease | 85 (8.5%) | 48 (9.6%) | 18.50 | 37 (7.4%) | 17.30 |
| Cardiovascular disease | 238 (23.8%) | 133 (26.7%) | 17.50 | 105 (21%) | 17.30 |
| Diabetes | 146 (14.6%) | 87 (17.4%) | 16.50 | 59 (11.8%) | 14.30 |
| Hypertension | 456 (45.6%) | 253 (50.7%) | 16.80 | 203 (40.5%) | 17.10 |
| Carcinoma | 176 (17.6%) | 96 (9.2%) | 16.35 | 80 (16%) | 17.20 |
| Bone fracture | 81 (8.1%) | 46 (9.2%) | 18.85 | 35 (7%) | 18.50 |
| Supplement VitD | 132 (13.2%) | 51 (10.2%) | 24.50 | 81 (16.2%) | 23.50 |
| Spring | 198 (19.8%) | 92 (18.4%) | 20.64 | 106 (21.2%) | 20.39 |
| Summer | 206 (20.6%) | 85 (17%) | 21.89 | 121 (24.2%) | 20.8 |
| Autumn | 353 (35.5%) | 194 (38.8%) | 20.62 | 159 (31.8%) | 20.52 |
| Winter | 243 (24.3%) | 129 (25.8%) | 17.72 | 114 (20.8%) | 19.17 |
| I | |||||
|---|---|---|---|---|---|
| Age Group | Mean Value | SD | 95% Confidence Interval | Median | |
| Lower Limit | Upper Limit | ||||
| 30 years and younger | 19.40 | ±±8.26 | 16.89 | 21.91 | 18.60 |
| 31–50 years | 21.05 | ±±10.58 | 18.83 | 23.27 | 19.20 |
| 51–69 years | 19.55 | ±±9.84 | 18.09 | 21.02 | 18.00 |
| 70 years and older | 20.28 | ±±11.75 | 18.60 | 21.96 | 17.00 |
| II | |||||
| Age Group | Mean Value | SD | 95% Confidence Interval | Median | |
| Lower Limit | Upper Limit | ||||
| 30 years and younger | 20.56 | ±±8.8 | 17.80 | 23.33 | 17.65 |
| 31–50 years | 20.72 | ±±9.44 | 18.98 | 22.45 | 19.20 |
| 51–69 years | 21.07 | ±±10.44 | 19.47 | 22.66 | 18.70 |
| 70 years and older | 21.87 | ±±12.79 | 19.97 | 23.79 | 17.30 |
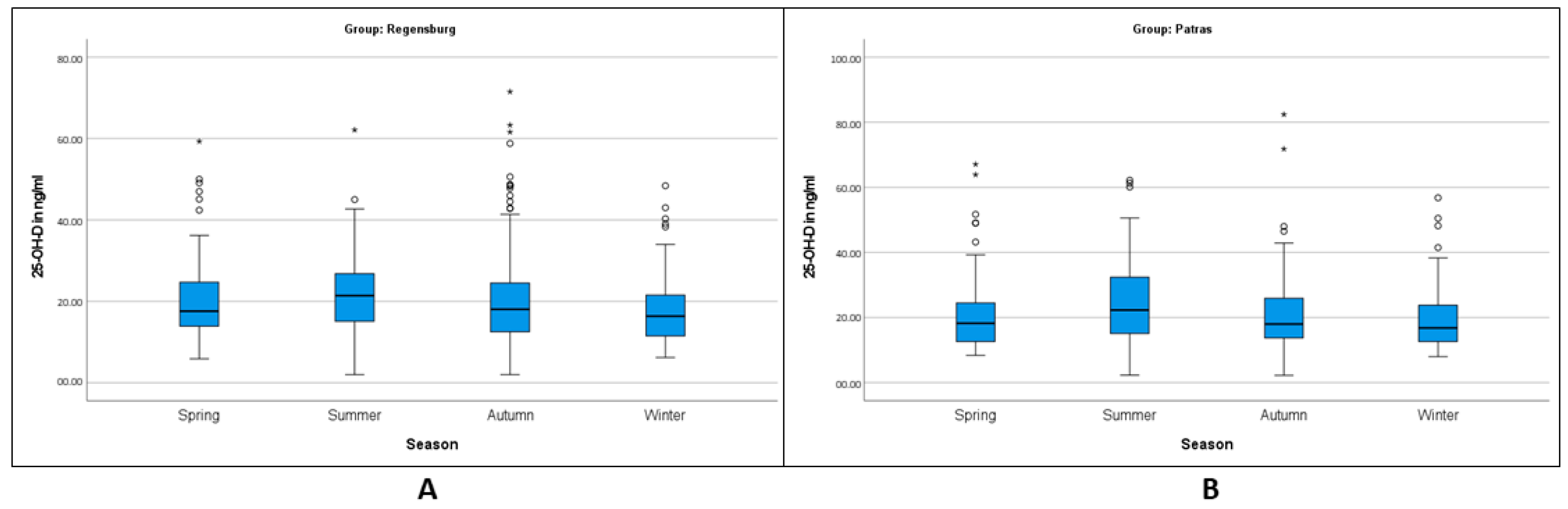
| I | |||||
|---|---|---|---|---|---|
| Season | Mean Value | SD | 95% Confidence Interval | Median | |
| Lower Limit | Upper Limit | ||||
| Spring | 20.65 | ±±10.38 | 18.50 | 22.80 | 17.60 |
| Summer | 21.89 | ±±10.42 | 19.63 | 24.14 | 21.40 |
| Autumn | 20.61 | ±±11.87 | 18.93 | 22.29 | 18.05 |
| Winter | 17.72 | ±±8.34 | 16.26 | 19.16 | 16.40 |
| II | |||||
| Season | Mean Value | SD | 95% Confidence Interval | Median | |
| Lower Limit | Upper Limit | ||||
| Spring | 20.39 | ±±10.95 | 18.28 | 22.50 | 18.25 |
| Summer | 24.80 | ±±12.25 | 22.59 | 27.00 | 22.30 |
| Autumn | 20.52 | ±±10.49 | 18.89 | 22.17 | 18.00 |
| Winter | 19.19 | ±±9.40 | 17.44 | 20.94 | 16.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamilos, A.; Matzaroglou, C.; Maier, G.S.; Zawy Alsofy, S.; Drees, P.; Kafchitsas, K. Vitamin D Deficiency in Orthopedic Patients in Different Latitudes—First Study Comparing German and Greek Populations. Osteology 2023, 3, 11-20. https://doi.org/10.3390/osteology3010002
Mamilos A, Matzaroglou C, Maier GS, Zawy Alsofy S, Drees P, Kafchitsas K. Vitamin D Deficiency in Orthopedic Patients in Different Latitudes—First Study Comparing German and Greek Populations. Osteology. 2023; 3(1):11-20. https://doi.org/10.3390/osteology3010002
Chicago/Turabian StyleMamilos, Andreas, Charalambos Matzaroglou, Gerrit S. Maier, Samer Zawy Alsofy, Philipp Drees, and Konstantinos Kafchitsas. 2023. "Vitamin D Deficiency in Orthopedic Patients in Different Latitudes—First Study Comparing German and Greek Populations" Osteology 3, no. 1: 11-20. https://doi.org/10.3390/osteology3010002
APA StyleMamilos, A., Matzaroglou, C., Maier, G. S., Zawy Alsofy, S., Drees, P., & Kafchitsas, K. (2023). Vitamin D Deficiency in Orthopedic Patients in Different Latitudes—First Study Comparing German and Greek Populations. Osteology, 3(1), 11-20. https://doi.org/10.3390/osteology3010002