Sedentary Behavior, Physical Activity, and Health of Workers in Chile According to the National Health Survey-2017




Abstract
1. Introduction
2. Materials and Methods
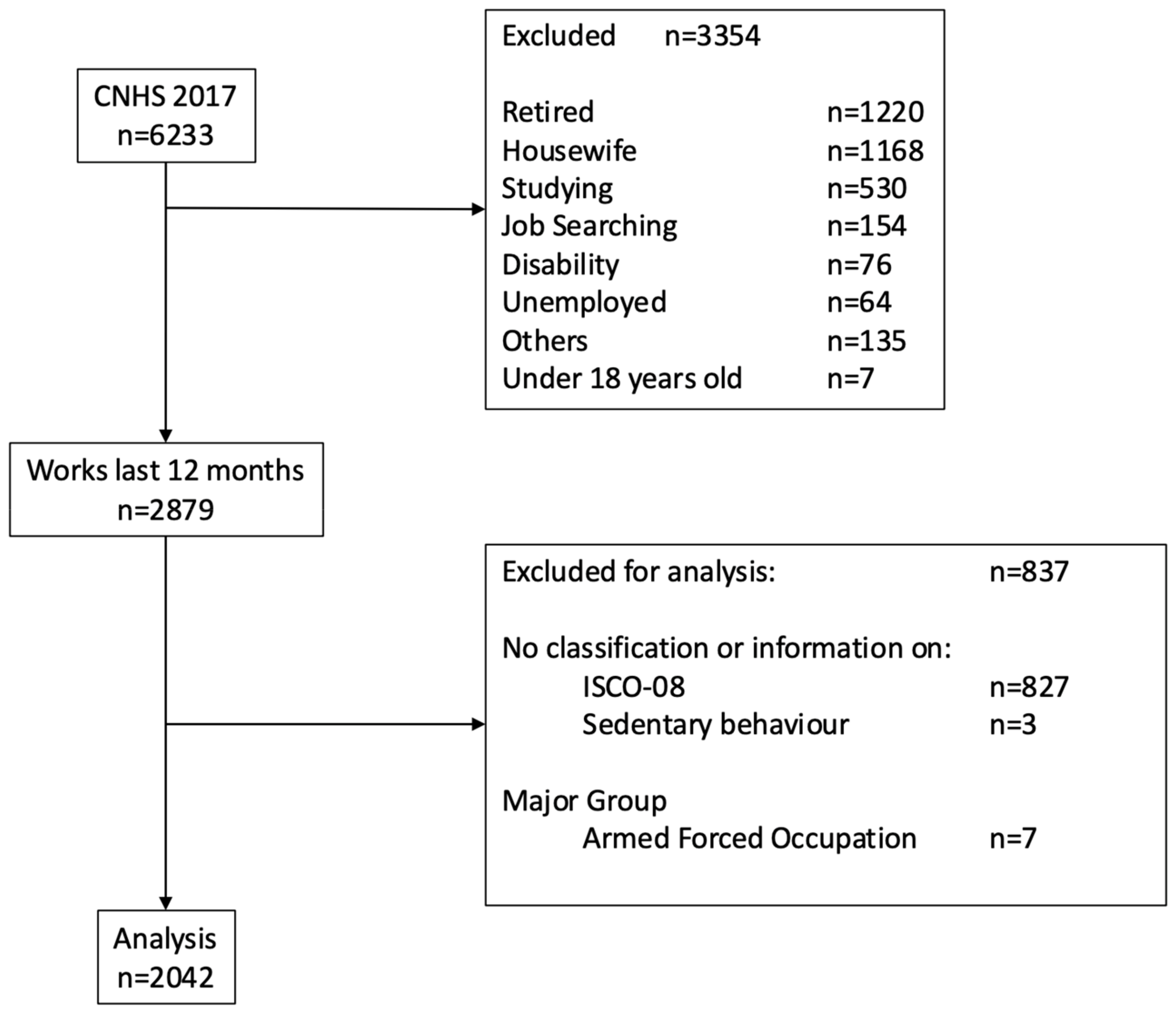
2.1. Study Design
2.2. Participants
2.3. Classification of Occupations
- Managers
- Professionals
- Technicians and associate professionals
- Clerical support workers
- Service and sales workers
- Skilled agricultural, forestry, and fishery workers
- Craft and related trades workers
- Plant and machine operators, and assemblers
- Elementary occupations
- Armed forces occupations
2.4. Measurements
- Frequency (days per week) of PA in each domain.
- Duration (minutes per day) of moderate and vigorous PA in each domain.
- Sufficiently active (≥600 MET-min/week).
- Insufficiently active (<600 MET-min/week).
2.5. Health Conditions
2.5.1. Musculoskeletal Symptoms (MKS)
2.5.2. Hypertension (HT)
2.5.3. Diabetes Mellitus (DM)
2.5.4. Metabolic Syndrome (MetS)
- Blood pressure ≥130/85 mmHg or treatment for hypertension.
- Triglycerides ≥150 mg/dL.
- Fasting glucose ≥100 mg/dL or treatment for diabetes.
- Waist circumference >80 cm (women) or >90 cm (men), following WHO standards.
- Low HDL cholesterol levels (<40 mg/dL for men, <50 mg/dL for women).
2.5.5. Cardiovascular Risk (CVR)
2.5.6. Overweight
2.6. Statistical Analysis
2.7. Ethics Approval
3. Results
3.1. Demographic Characteristics
3.2. Health Conditions
3.3. Sedentary Behavior and Physical Activity
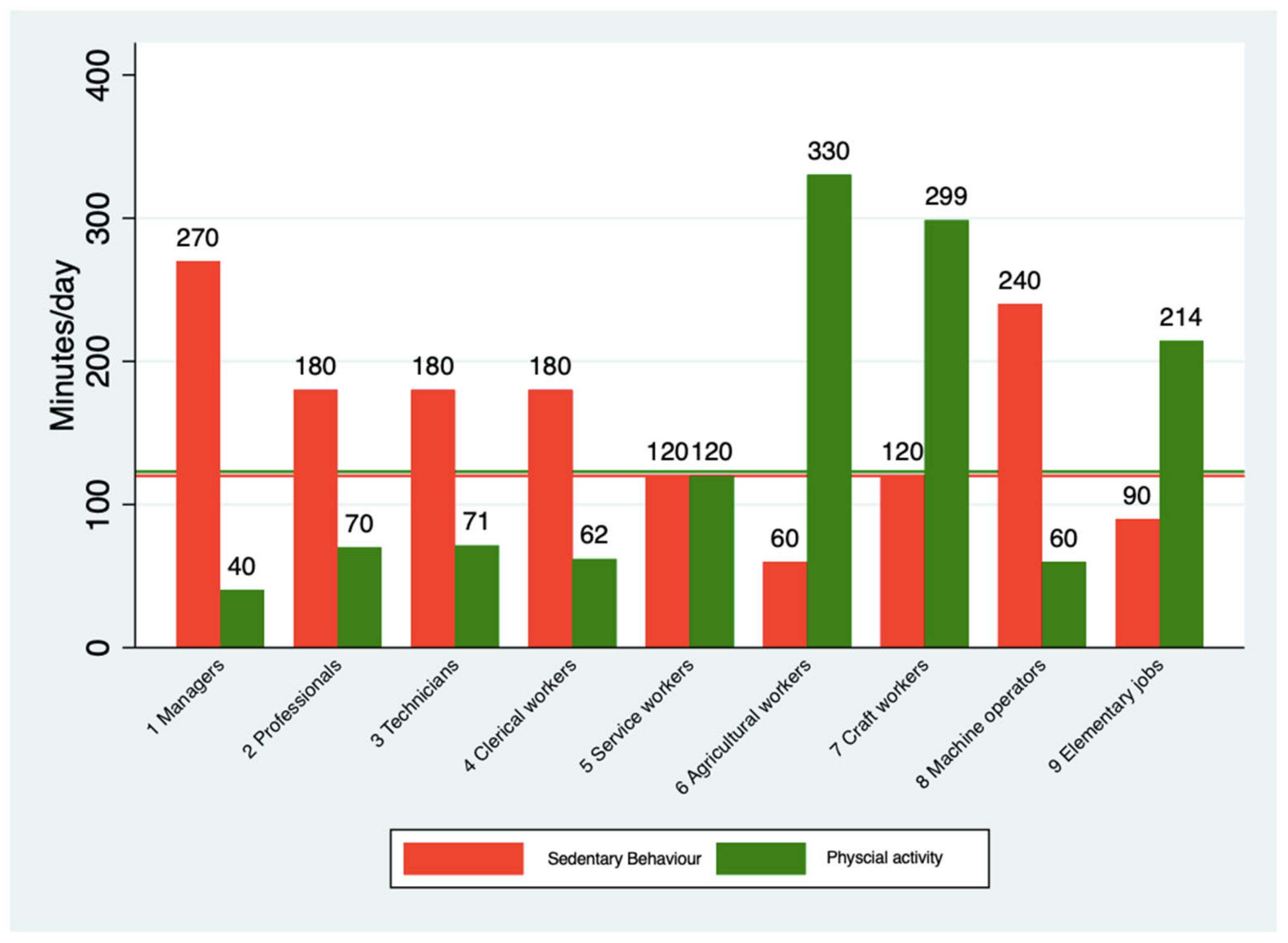
3.4. Major Occupational Group and Patterns of SB and PA
3.5. Association Between Health Outcomes and, SB and PA
4. Discussion
4.1. Comparison with Previous Studies
4.2. The Physical Activity Paradox
4.3. Practical and Theoretical Relevance
4.4. Strengths and Limitations
4.5. Future Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SB | Sedentary behavior |
| PA | Physical activity |
| CNHS-2017 | Chilean National Health Survey-2017 |
| ISCO-08 | International Standard Occupation Classification 08 |
| GPAQ | Global Physical Activity Questionnaire |
| WHO | World Health Organization |
| OR | Odds ratio |
| CI | Confidence interval |
| MOGs | Major occupational group |
| MSK | Musculoskeletal symptoms |
| HT | Hypertension |
| DM | Diabetes mellitus |
| MetS | Metabolic syndrome |
References
- Pronk, N.P. Implementing movement at the workplace: Approaches to increase physical activity and reduce sedentary behavior in the context of work. Prog. Cardiovasc. Dis. 2021, 64, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.; Prüss-Ustün, A.; Ivanov, I.; Mudgal, S.; Corvalán, C.; Bos, R.; Neira, M. Preventing Disease Through a Healthier and Safer Workplace; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; SBRN Terminology Consensus Project Participants. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef]
- Lee, H.; Lee, M. Correlates of Objectively Measured Sitting Time in South Korean Adults: 2014–2015 Korea National Health and Nutrition Examination Survey. Front. Public Health 2022, 10, 846542. [Google Scholar] [CrossRef]
- Koohsari, M.J.; Kaczynski, A.T.; Yasunaga, A.; Hanibuchi, T.; Nakaya, T.; McCormack, G.R.; Oka, K. Active workplace design: Current gaps and future pathways. Br. J. Sports Med. 2024, 58, 1157–1158. [Google Scholar] [CrossRef]
- Franco, M.; Ricceri, F. The physical activity paradox. Recent. Prog. Med. 2024, 115, 325–327. [Google Scholar]
- Holtermann, A.; Straker, L.; Lee, I.M.; Stamatakis, E.; van der Beek, A.J. Workplace physical activity promotion: Why so many failures and few successes? The need for new thinking. Br. J. Sports Med. 2020, 55, 650–651. [Google Scholar] [CrossRef]
- Casanova, F.; O’Loughlin, J.; Karageorgiou, V.; Beaumont, R.N.; Bowden, J.; Wood, A.R.; Tyrrell, J. Effects of physical activity and sedentary time on depression, anxiety and well-being: A bidirectional Mendelian randomisation study. BMC Med. 2023, 21, 501. [Google Scholar] [CrossRef]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef]
- Dempsey, P.C.; Biddle, S.J.H.; Buman, M.P.; Chastin, S.; Ekelund, U.; Friedenreich, C.M.; Katzmarzyk, P.T.; Leitzmann, M.F.; Stamatakis, E.; van der Ploeg, H.P.; et al. New global guidelines on sedentary behaviour and health for adults: Broadening the behavioural targets. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 151. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Brown, W.J.; Steene-Johannessen, J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.E.; Lee, I.-M. Do the associations of sedentary behaviour with cardiovascular disease mortality and cancer mortality differ by physical activity level? A systematic review and harmonised meta-analysis of data from 850 060 participants. Br. J. Sports Med. 2019, 53, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.-M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef]
- Aguilar-Farias, N.; Leppe Zamora, J. Is a single question of the Global Physical Activity Questionnaire (GPAQ) valid for measuring sedentary behaviour in the Chilean population? J. Sports Sci. 2017, 35, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Verdejo, R.; Suárez-Reyes, M. Physical inactivity versus sedentariness: Analysis of the chilean national health survey 2016–2017. Rev. Med. Chil. 2021, 149, 103–109. [Google Scholar] [CrossRef]
- Leppe, J.; Margozzini, P.; Villarroel, L.; Sarmiento, O.; Guthold, R.; Bull, F. Validity of the global physical activity questionnaire in the National Health Survey–Chile 2009–10. J. Sci. Med. Sport 2012, 15, S297. [Google Scholar] [CrossRef]
- Diaz-Martinez, X.; Steell, L.; Martinez, M.A.; Leiva, A.M.; Salas-Bravo, C.; Labrana, A.M.; Durán, E.; Cristi-Montero, C.; Livingstone, K.M.; Garrido-Méndez, A.; et al. Higher levels of self-reported sitting time is associated with higher risk of type 2 diabetes independent of physical activity in Chile. J. Public Health 2018, 40, 501–507. [Google Scholar] [CrossRef]
- Poblete-Valderrama, F.; Rivera, C.F.; Petermann-Rocha, F.; Leiva, A.M.; Martínez-Sanguinetti, M.A.; Troncoso, C.; Mardones, L.; Villagrán, M.; Nazar, G.; Ulloa, N.; et al. Physical activity and sedentary behaviours are associated with cognitive impairment in Chilean older adults. Rev. Med. Chil. 2019, 147, 1247–1255. [Google Scholar] [CrossRef]
- Steeves, J.A.; Tudor-Locke, C.; Murphy, R.A.; King, G.A.; Fitzhugh, E.C.; Bassett, D.R.; Van Domelen, D.; Schuna, J.M.; Harris, T.B. Daily Physical Activity by Occupational Classification in US Adults: NHANES 2005–2006. J. Phys. Act. Health 2018, 15, 900–911. [Google Scholar] [CrossRef]
- Sung, J.H.; Son, S.R.; Baek, S.H.; Kim, B.J. Association of occupation with the daily physical activity and sedentary behaviour of middle-aged workers in Korea: A cross-sectional study based on data from the Korea National Health and Nutrition Examination Survey. BMJ Open 2021, 11, e055729. [Google Scholar] [CrossRef]
- Pratt, M.; Varela, A.R.; Bauman, A. The Physical Activity Policy to Practice Disconnect. J. Phys. Act. Health 2023, 20, 461–464. [Google Scholar] [PubMed]
- Pratt, M.; Ramírez Varela, A.; Hallal, P.C. Celebrating 10 Years of the Global Observatory for Physical Activity-GoPA! J. Phys. Act. Health 2024, 21, 423–424. [Google Scholar] [CrossRef]
- Chile MdSd. Encuesta Nacional de Salud 2017. Chile. Available online: https://epi.minsal.cl/encuesta-ens-descargable/ (accessed on 17 March 2025).
- International Labour Office. International Standard Classification of Occupations 2008 (ISCO-08): Structure, Group Definitions and Correspondence Tables; International Labour Office: Geneva, Switzerland, 2012; Available online: https://public.ebookcentral.proquest.com/choice/publicfullrecord.aspx?p=991922 (accessed on 17 March 2025).
- Bull, F.C.; Maslin, T.S.; Armstrong, T. Global physical activity questionnaire (GPAQ): Nine country reliability and validity study. J. Phys. Act. Health 2009, 6, 790–804. [Google Scholar] [CrossRef] [PubMed]
- Bennett, K.; Cardiel, M.H.; Ferraz, M.B.; Riedemann, P.; Goldsmith, C.H.; Tugwell, P. Community screening for rheumatic disorder: Cross cultural adaptation and screening characteristics of the COPCORD Core Questionnaire in Brazil, Chile, and Mexico. The PANLAR-COPCORD Working Group. Pan American League of Associations for Rheumatology. Community Oriented Programme for the Control of Rheumatic Disease. J. Rheumatol. 1997, 24, 160–168. [Google Scholar] [PubMed]
- Mena-Iturriaga, M.J.; Mauri-Stecca, M.V.; Sizer, P.S.; Leppe, J. Quality of life in chronic musculoskeletal symptomatic Chilean population: Secondary analysis of National Health Survey 2009–2010. BMC Musculoskelet. Disord. 2020, 21, 262. [Google Scholar]
- Saidj, M.; Menai, M.; Charreire, H.; Weber, C.; Enaux, C.; Aadahl, M.; Kesse-Guyot, E.; Hercberg, S.; Simon, C.; Oppert, J.-M. Descriptive study of sedentary behaviours in 35,444 French working adults: Cross-sectional findings from the ACTI-Cités study. BMC Public Health 2015, 15, 379. [Google Scholar]
- Kitano, N.; Kai, Y.; Jindo, T.; Fujii, Y.; Tsunoda, K.; Arao, T. Association of domain-specific physical activity and sedentary behavior with cardiometabolic health among office workers. Scand. J. Med. Sci. Sports. 2022, 8, 1224–1235. [Google Scholar] [CrossRef]
- Shivakumar, M.; Welsh, V.; Bajpai, R.; Helliwell, T.; Mallen, C.; Robinson, M.; Shepherd, T. Musculoskeletal disorders and pain in agricultural workers in Low- and Middle-Income Countries: A systematic review and meta-analysis. Rheumatol. Int. 2024, 44, 235–247. [Google Scholar]
- Parry, S.P.; Coenen, P.; Shrestha, N.; O’Sullivan, P.B.; Maher, C.G.; Straker, L.M. Workplace interventions for increasing standing or walking for decreasing musculoskeletal symptoms in sedentary workers. Cochrane Database Syst. Rev. 2019, 2019, CD012487. [Google Scholar] [CrossRef]
- Holtermann, A.; Hansen, J.V.; Burr, H.; Søgaard, K.; Sjøgaard, G. The health paradox of occupational and leisure-time physical activity. Br. J. Sports Med. 2012, 46, 291–295. [Google Scholar] [CrossRef]
- Pronk, N. Physical activity paradox: Providing evidence-based guidance while closing research gaps. Br. J. Sports Med. 2024, 58, 932–933. [Google Scholar] [PubMed]
- Gupta, N.; Dencker-Larsen, S.; Lund Rasmussen, C.; McGregor, D.; Rasmussen, C.D.N.; Thorsen, S.V.; Jørgensen, M.B.; Chastin, S.; Holtermann, A. The physical activity paradox revisited: A prospective study on compositional accelerometer data and long-term sickness absence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 93. [Google Scholar]
- Govaerts, R.; Tassignon, B.; Ghillebert, J.; Serrien, B.; De Bock, S.; Ampe, T.; El Makrini, I.; Vanderborght, B.; Meeusen, R.; De Pauw, K. Prevalence and incidence of work-related musculoskeletal disorders in secondary industries of 21st century Europe: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2021, 22, 751. [Google Scholar] [CrossRef] [PubMed]
- Dogra, S.; Copeland, J.L.; Altenburg, T.M.; Heyland, D.K.; Owen, N.; Dunstan, D.W. Start with reducing sedentary behavior: A stepwise approach to physical activity counseling in clinical practice. Patient Educ. Couns. 2022, 105, 1353–1361. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.C.; Matthews, C.E.; Dashti, S.G.; Doherty, A.R.; Bergouignan, A.; van Roekel, E.H.; Dunstan, D.W.; Wareham, N.J.; Yates, T.E.; Wijndaele, K.; et al. Sedentary Behavior and Chronic Disease: Mechanisms and Future Directions. J. Phys. Act. Health 2020, 17, 52–61. [Google Scholar] [CrossRef]
- Zhou, L.; Deng, X.; Guo, K.; Hou, L.; Hui, X.; Wu, Y.; Xu, M.; Wang, Y.; Liang, S.; Yang, K.; et al. Effectiveness of Multicomponent Interventions in Office-Based Workers to Mitigate Occupational Sedentary Behavior: Systematic Review and Meta-Analysis. JMIR Public Health Surveill. 2023, 9, e44745. [Google Scholar]
- Taylor, W.C.; Williams, J.R.; Harris, L.E.; Shegog, R. Computer Prompt Software to Reduce Sedentary Behavior and Promote Physical Activity Among Desk-Based Workers: A Systematic Review. Hum. Factors 2021, 65, 891–908. [Google Scholar] [CrossRef]
- Azevedo, L.M.; Chiavegato, L.D.; Carvalho, C.R.F.; Braz, J.R.; Nunes Cabral, C.M.; Padula, R.S. Are blue-collar workers more physically active than white-collar at work? Arch. Environ. Occup. Health 2021, 76, 338–347. [Google Scholar] [CrossRef]
- Watanabe, K.; Kawakami, N. Effects of a Multi-Component Workplace Intervention Program with Environmental Changes on Physical Activity among Japanese White-Collar Employees: A Cluster-Randomized Controlled Trial. Int. J. Behav. Med. 2018, 25, 637–648. [Google Scholar]

{kind=link}
{kind=link}
| Total | Female | Male | p-Value | |
|---|---|---|---|---|
| n (%) | 2042 (100) | 1017 (49.8) | 1025 (50.2) | |
| Age (years) | 45 (33–56) | 44 (33–54) | 46 (33–57) | 0.015 |
| Age group | ||||
| 18–24 years | 139 (6.8) | 64 (6.3) | 75 (7.3) | 0.059 |
| 25–44 years | 880 (43.1) | 466 (45.8) | 414 (40.4) | |
| 45–64 years | 891 (43.6) | 430 (42.3) | 461 (45.0) | |
| ≥64 years | 132 (6.5) | 57 (5.6) | 75 (7.3) | |
| Residence area | ||||
| Urban | 1802 (88.2) | 894 (87.9) | 908 (88.6) | 0.63 |
| Education | ||||
| Low (<8 years) | 252 (12.4) | 121 (12.0) | 131 (12.9) | 0.049 |
| Medium (8–12 years) | 1161 (57.3) | 557 (55.2) | 604 (59.3) | |
| High (≥13 years) | 614 (30.3) | 331 (32.8) | 283 (27.8) | |
| Major Occupational Group | ||||
| 1. Managers | 74 (3.6) | 39 (3.8) | 35 (3.4) | <0.001 |
| 2. Professionals | 243 (11.9) | 151 (14.8) | 92 (9.0) | |
| 3. Technicians and associate professionals | 214 (10.5) | 102 (10.0) | 112 (10.9) | |
| 4. Clerical support workers | 97 (4.8) | 63 (6.2) | 34 (3.3) | |
| 5. Service and sales workers | 504 (24.7) | 333(32.7) | 171 (16.7) | |
| 6. Skilled agricultural, forestry, and fishery workers | 64 (3.1) | 20.(2.0) | 44 (4.3) | |
| 7. Craft and related trades workers | 309 (15.1) | 58 (5.7) | 251 (24.5) | |
| 8. Plant and machine operators, and assemblers | 200 (9.8) | 27 (2.7) | 173 (16.9) | |
| 9. Elementary occupations | 337 (16.5) | 224 (22.0) | 113 (11.0) | |
| Health conditions | ||||
| Overweight | 1416 (79.1) | 703 (77.9) | 713 (80.3) | 0.22 |
| Metabolic syndrome | 474 (41.5) | 217 (38.1) | 257 (45.0) | 0.017 |
| Musculoskeletal symptoms | 788 (38.6) | 462 (45.4) | 326 (31.8) | <0.001 |
| Hypertension | 527 (28.8) | 223 (24.2) | 304 (33.4) | <0.001 |
| Cardiovascular risk | 253 (22.2) | 131 (22.9) | 122 (21.4) | 0.028 |
| Diabetes | 220 (12.8) | 110 (12.7) | 110 (12.9) | 0.88 |
| Sedentary behavior P50 (P25–P75) | ||||
| Total (min/day) | 120 (60, 243) | 120 (60–240) | 120 (60–300) | 0.008 |
| Sedentary behavior (quartiles) | ||||
| <1 h | 364 (17.8) | 201 (19.8) | 163 (15.9) | 0.065 |
| 1–2 h | 403 (19.7) | 206 (20.3) | 197 (19.2) | |
| 2–4 h | 609 (29.8) | 299 (29.4) | 310 (30.2) | |
| >4 h | 666 (32.6) | 311 (30.6) | 355 (34.6) | |
| Physical activity P50 (P25–P75) | ||||
| Total (min/day) | 123 (23–381) | 86 (15–320) | 180 (34–443) | <0.001 |
| Work (min/day) | 0 (0–257) | 0 (0–214) | 23 (0–334) | <0.001 |
| Travel (min/day) | 20 (0–60) | 17 (0–51) | 26 (0–86) | <0.001 |
| Leisure (min/day) | 0 (0, 13) | 0 (0–0) | 0 (0–19) | <0.001 |
| Sufficiently active (WHO criteria) | 1408 (71.7) | 647 (66.4) | 761 (77.0) | <0.001 |
| Major Occupational Groups | SB-Total (min/day) | SB ≥ 4 (hours) | PA-Total (min/day) | PA-Travel (min/day) | PA-Work (min/day) | PA-Leisure (min/day) | Sufficiently Active |
|---|---|---|---|---|---|---|---|
| Total | 120 (60–243) | 32.6% | 123 (223–381) | 20 (0–60) | 0 (0–257) | 0 (0–13) | 71.7% |
| 1. Managers | 270 (120–480) | 59.5% | 40 (0–158) | 0 (0–37) | 0 (0–21) | 0 (0–17) | 56.9% |
| 2. Professionals | 180 (60–360) | 46.9% | 70 (17–250) | 17 (0–60) | 0 (0–86) | 0 (0–26) | 67.5% |
| 3. Technicians and associate professionals | 180 (90–363) | 47.2% | 71 (17–266) | 18 (0–60) | 0 (0–86) | 0 (0–26) | 66.0% |
| 4. Clerical support workers | 180 (60–420) | 47.4% | 62 (11–300) | 15 (0–60) | 0 (0–129) | 0 (0–17) | 57.6% |
| 5. Service and sales workers | 120 (60–240) | 27.6% | 120 (26–352) | 21 (0–79) | 0 (0–214) | 0 (0–0) | 70.4% |
| 6. Skilled agricultural, forestry, and fishery workers | 60 (30–180) | 15.6% | 330 (194–588) | 44 (4–240) | 189 (0–420) | 0 (0–0) | 87.3% |
| 7. Craft and related trades workers | 120 (60–180) | 20.4% | 299 (66–489) | 25 (0–60) | 206 (0–386) | 0 (0–17) | 86.3% |
| 8. Plant and machine operators, and assemblers | 240 (60–480) | 53.5% | 60 (0–408) | 0 (0–41) | 0 (0–310) | 0 (0–9) | 56.8% |
| 9. Elementary occupations | 90 (47–180) | 12.5% | 214 (39–424) | 25 (0–86) | 69 (0–309) | 0 (0–0) | 80.1% |
| Unadjusted Model (95%CI) | |||||
|---|---|---|---|---|---|
| Sedentary Behavior (Quartile) | Musculoskeletal Symptoms | Hypertension | Diabetes | Metabolic Syndrome | Cardiovascular Risk |
| <1 h (reference) | reference | reference | reference | reference | reference |
| 1–2 h | 1.34 (1.01–1.80) | 1.44 (1.04–2.00) | 0.92 (0.59–1.44) | 1.21 (0.83–1.78) | 1.15 (0.74–1.80) |
| 2–4 h | 1.26 (0.96–1.65) | 1.10 (0.81–1.49) | 0.73 (0.48–1.11) | 0.90 (0.63–1.28) | 0.90 (0.59–1.37) |
| >4 h | 1.28 (0.98–1.67) | 1.03 (0.76–1.39) | 0.89 (0.60–1.34) | 1.01 (0.71–1.43) | 0.91 (0.60–1.38) |
| Adjusted Model OR (95%CI) | |||||
| Sedentary Behavior (Quartile) | Musculoskeletal Symptoms | Hypertension | Diabetes | Metabolic Syndrome | Cardiovascular Risk |
| <1 h | reference | reference | reference | reference | reference |
| 1–2 h | 1.43 (1.06–1.94) | 1.67 (1.15–2.42) | 0.98 (0.61–1.55) | 1.27 (0.84–1.90) | 1.35 (0.83–2.21) |
| 2–4 h | 1.37 (1.04–1.82) | 1.31 (0.92–1.85) | 0.79 (0.51–1.22) | 0.97 (0.67–1.41) | 1.04 (0.66–1.66) |
| >4 h | 1.60 (1.20–2.13) | 1.52 (1.06–2.19) | 1.03 (0.66–1.60) | 1.19 (0.81–1.74) | 1.17 (0.73–1.87) |
| Major Occupational Groups | |||||
| 1. Managers | reference | reference | reference | reference | reference |
| 2. Professionals | 1.37 (0.76–2.47) | 0.97 (0.45–2.08) | 1.40 (0.49–4.06) | 0.97 (0.46–2.06) | 0.80 (0.31–2.08) |
| 3. Technicians | 1.61 (0.89–2.93) | 0.90 (0.42–1.93) | 1.84 (0.65–5.19) | 0.84 (0.39–1.78) | 0.73 (0.28–1.87) |
| 4. Clerical support workers | 1.76 (0.90–3.47) | 1.24 (0.52–2.98) | 1.36 (0.41–4.48) | 2.11 (0.89–5.02) | 1.19 (0.40–3.59) |
| 5. Service and sales workers | 1.65 (0.93–2.92) | 1.45 (0.71–2.98) | 1.19 (0.43–3.28) | 1.17 (0.58–2.34) | 0.85 (0.35–2.07) |
| 6. Agricultural workers | 2.26 (1.03–4.95) | 0.99 (0.37–2.66) | 1.57 (0.42–5.81) | 0.60 (0.23–1.57) | 0.60 (0.17–2.15) |
| 7. Craft and related trades | 2.01 (1.11–3.67) | 1.09 (0.52–2.30) | 0.82 (0.28–2.39) | 1.28 (0.62–2.63) | 0.48 (0.19–1.23) |
| 8. Machine operators | 2.00 (1.08–3.72) | 1.26 (0.59–2.71) | 1.77 (0.62–5.11) | 1.56 (0.73–3.33) | 1.03 (0.39–2.71) |
| 9. Elementary occupations | 1.87 (1.03–3.41) | 1.49 (0.71–3.15) | 1.26 (0.44–3.59) | 1.09 (0.53–2.26) | 0.77 (0.30–1.97) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leppe Zamora, J.; Leppe Zamora, M.; Roa-Alcaino, S.; Sarmiento, O.L. Sedentary Behavior, Physical Activity, and Health of Workers in Chile According to the National Health Survey-2017. Epidemiologia 2025, 6, 15. https://doi.org/10.3390/epidemiologia6010015
Leppe Zamora J, Leppe Zamora M, Roa-Alcaino S, Sarmiento OL. Sedentary Behavior, Physical Activity, and Health of Workers in Chile According to the National Health Survey-2017. Epidemiologia. 2025; 6(1):15. https://doi.org/10.3390/epidemiologia6010015
Chicago/Turabian StyleLeppe Zamora, Jaime, Marco Leppe Zamora, Sonia Roa-Alcaino, and Olga Lucía Sarmiento. 2025. "Sedentary Behavior, Physical Activity, and Health of Workers in Chile According to the National Health Survey-2017" Epidemiologia 6, no. 1: 15. https://doi.org/10.3390/epidemiologia6010015
APA StyleLeppe Zamora, J., Leppe Zamora, M., Roa-Alcaino, S., & Sarmiento, O. L. (2025). Sedentary Behavior, Physical Activity, and Health of Workers in Chile According to the National Health Survey-2017. Epidemiologia, 6(1), 15. https://doi.org/10.3390/epidemiologia6010015