
Post-COVID-19: Time to Change Our Way of Life for a Better Future


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Impact of Population Density on the Spread of COVID-19 in Cities and Municipal Areas
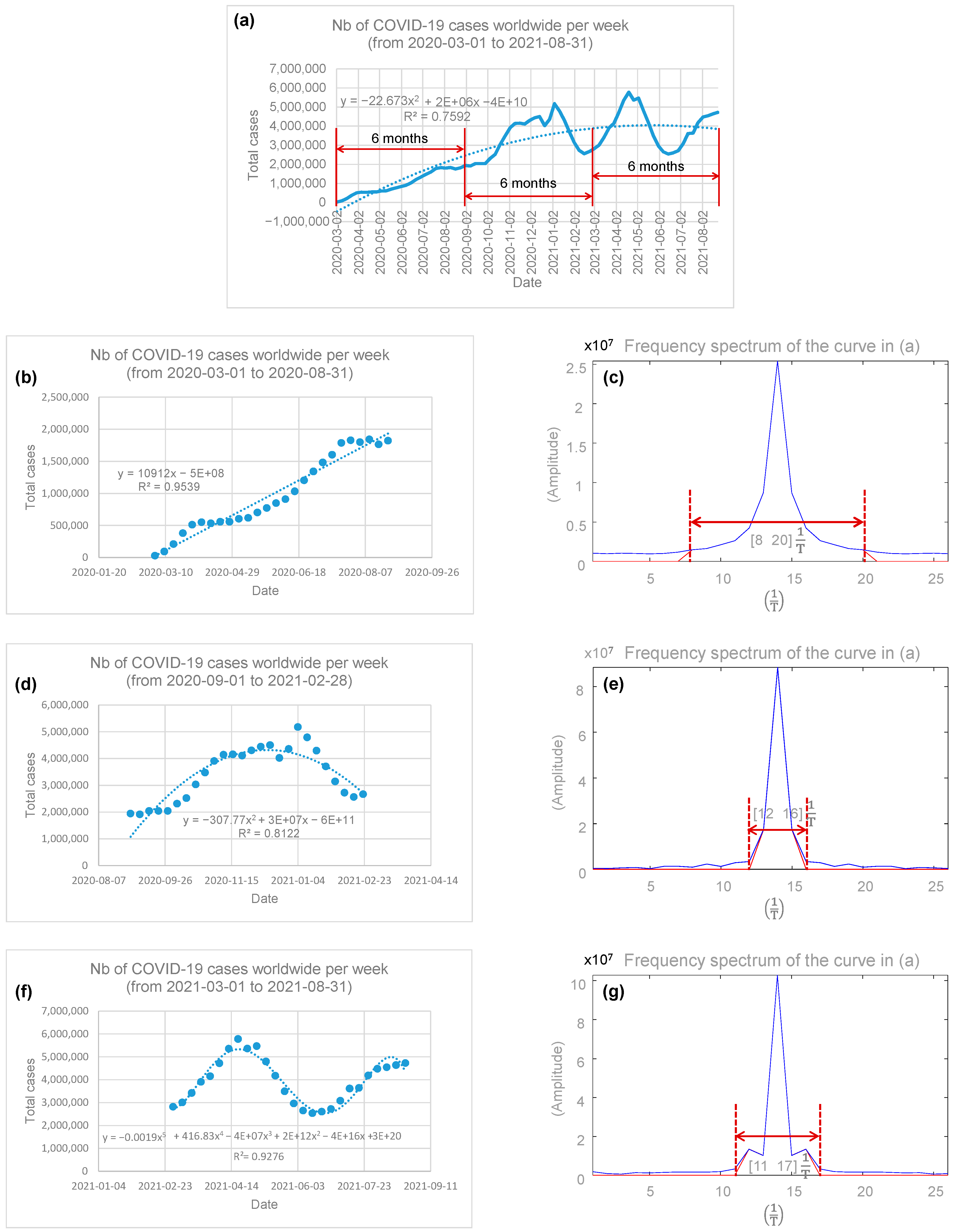
3.2. Spectral Analysis of the Temporal Evolution of COVID-19
- COVID-19 spread from 2 March 2020 to 31 August 2020
- 2.
- COVID-19 spread from 1 September 2020 to 28 February 2021
- 3.
- COVID-19 spread from 1 March 2021 to 31 August 2021
4. Discussion
4.1. COVID-19 Data Reliability
4.2. Spread of COVID-19 in G20 Countries
4.3. Impact of Population Density on the Spread of COVID-19
4.4. What Is Learned from the Spectral Analysis of COVID-19
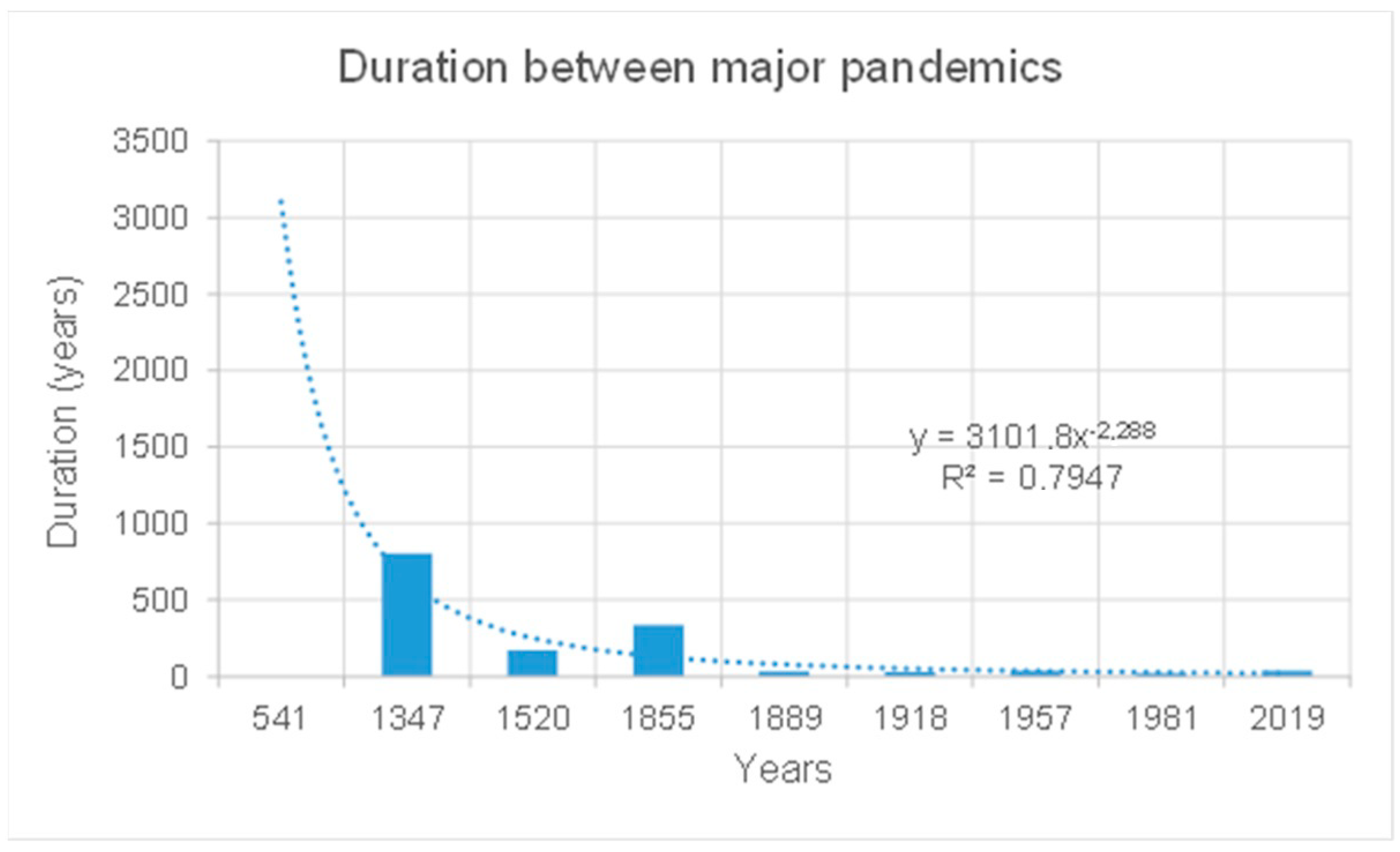
4.5. The Very Next Pandemic Could Be Closer Than Expected
4.6. Limitations of the Study
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Spiteri, G.; Fielding, J.; Diercke, M.; Campese, C.; Enouf, V.; Gaymard, A.; Bella, A.; Sognamiglio, P.; Moros, M.J.S.; Riutort, A.N.; et al. First cases of coronavirus disease 2019 (COVID-19) in the WHO European Region, 24 January to 21 February 2020. Eurosurveillance 2020, 25, 2000178. [Google Scholar] [CrossRef]
- Islam, M.A.; Kundu, S.; Alam, S.S.; Hossan, T.; Kamal, M.A.; Hassan, R. Prevalence and characteristics of fever in adult and paediatric patients with coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis of 17515 patients. PLoS ONE 2021, 16, e0249788. [Google Scholar] [CrossRef]
- Islam, M.A.; Alam, S.S.; Kundu, S.; Hossan, T.; Kamal, M.A.; Cavestro, C. Prevalence of Headache in Patients With Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of 14,275 Patients. Front. Neurol. 2020, 11, 562634. [Google Scholar] [CrossRef]
- Saniasiaya, J.; Islam, M.A.; Abdullah, B. Prevalence of Olfactory Dysfunction in Coronavirus Disease 2019 (COVID-19): A Meta-analysis of 27,492 Patients. Laryngoscope 2021, 131, 865–878. [Google Scholar] [CrossRef]
- Saniasiaya, J.; Islam, M.A.; Abdullah, B. Prevalence and Characteristics of Taste Disorders in Cases of COVID-19: A Meta-analysis of 29,349 Patients. Otolaryngol. Head Neck Surg. 2020, 165, 33–42. [Google Scholar] [CrossRef]
- Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19). Centers for Disease Control and Prevention. 30 June 2020. Available online: https://stacks.cdc.gov/view/cdc/89980 (accessed on 27 December 2021).
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nature Reviews. Microbiology 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Meyerowitz, E.A.; Richterman, A.; Gandhi, R.T.; Sax, P.E. Transmission of SARS-CoV-2: A review of viral, host, and environmental factors. Ann. Intern. Med. 2021, 174, 69–79. [Google Scholar] [CrossRef]
- Wang, C.C.; Prather, K.A.; Sznitman, J.; Jimenez, J.L.; Lakdawala, S.S.; Tufekci, Z.; Marr, L.C. Airborne transmission of respiratory viruses. Science 2021, 373, eabd9149. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Jimenez, J.L.; Prather, K.A.; Tufekci, Z.; Fisman, D.; Schooley, R. Ten scientific reasons in support of airborne transmission of SARS-CoV-2. Lancet 2021, 397, 1603–1605. [Google Scholar] [CrossRef]
- Wei, H.-Y.; Chang, C.-P.; Liu, M.-T.; Mu, J.-J.; Lin, Y.-J.; Dai, Y.-T.; Su, C.-P. Probable aerosol transmission of SARS-CoV-2 through floors and walls of quarantine hotel, Taiwan, 2021. Emerg. Infect. Dis. 2022, 28, 2374–2382. [Google Scholar] [CrossRef]
- Abdool Karim, S.S.; de Oliveira, T. New SARS-CoV-2 Variants—Clinical, Public Health, and Vaccine Implications. N. Engl. J. Medicine. Mass. Med. Soc. 2021, 384, 1866–1868, ISSN 0028-4793. [Google Scholar] [CrossRef]
- Mallapaty, S. COVID mink analysis shows mutations are not dangerous—Yet. Nature 2020, 587, 340–341. [Google Scholar] [CrossRef] [PubMed]
- Koyama, T.; Platt, D.; Parida, L. Variant analysis of SARS-CoV-2 genomes. Bull. World Health Organ. 2020, 98, 495–504. [Google Scholar] [CrossRef]
- Andersen, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The proximal origin of SARS-CoV-2. Nat. Med. 2020, 26, 450–452. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.; Wang, X.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.; Zhu, Y.; Li, B.; Huang, C.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.G.; Lin, T.; Wang, P. Mechanisms of SARS-CoV-2 Transmission and Pathogenesis. Trends Immunol. 2020, 41, 1100–1115. [Google Scholar] [CrossRef]
- Marik, P.E.; Iglesias, J.; Varon, J.; Kory, P. A scoping review of the pathophysiology of COVID-19. Int. J. Immunopathol. Pharmacol. 2021, 35, 20587384211048026. [Google Scholar] [CrossRef] [PubMed]
- Viana Martins, C.P.; Xavier, C.S.; Cobrado, L. Disinfection methods against SARS-CoV-2: A systematic review. J. Hosp. Infect. 2022, 119, 84–117, ISSN 1532-2939. [Google Scholar] [CrossRef]
- Boulos, L.; Curran, J.A.; Gallant, A.; Wong, H.; Johnson, C.; Delahunty-Pike, A.; Saxinger, L.; Chu, D.; Comeau, J.; Flynn, T.; et al. Effectiveness of face masks for reducing transmission of SARS-CoV-2: A rapid systematic review. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2023, 381, 2257. [Google Scholar] [CrossRef]
- Ju, J.T.; Boisvert, L.N.; Zuo, Y.Y. Face masks against COVID-19: Standards, efficacy, testing and decontamination methods. Adv. Colloid Interface Sci. 2021, 292, 102435. [Google Scholar] [CrossRef]
- Ataei, M.; Shirazi, F.M.; Nakhaee, S.; Abdollahi, M.; Mehrpour, O. Assessment of cloth masks ability to limit Covid-19 particles spread: A systematic review. Environ. Sci. Pollut. Res. Int. 2021, 29, 1645–1676. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.D.; Chi, W.Y.; Su, J.H.; Ferrall, L.; Hung, C.F.; Wu, T.C. Coronavirus vaccine development: From SARS and MERS to COVID-19. J. Biomed. Sci. 2020, 27, 104. [Google Scholar] [CrossRef] [PubMed]
- Subbarao, K. The success of SARS-CoV-2 vaccines and challenges ahead. Cell Host Microbe 2021, 29, 1111–1123. [Google Scholar] [CrossRef]
- Ye, Y.; Zhang, Q.; Wei, X.; Cao, Z.; Yuan, H.Y.; Zeng, D.D. Equitable access to COVID-19 vaccines makes a life-saving difference to all countries. Nat. Hum. Behav. 2022, 6, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.S.; Read, S.W.; Fauci, A.S. Therapy for Early COVID-19: A Critical Need. JAMA 2020, 324, 2149–2150. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Du, Z.; Zhu, F.; Cao, Z.; An, Y.; Gao, Y.; Jiang, B. Comorbidities and multi-organ injuries in the treatment of COVID-19. Lancet 2020, 395, e52. [Google Scholar] [CrossRef]
- Tao, K.; Tzou, P.L.; Nouhin, J.; Bonilla, H.; Jagannathan, P.; Shafer, R.W. SARS-CoV-2 Antiviral Therapy. Clin. Microbiol. Rev. 2021, 34, e0010921. [Google Scholar] [CrossRef]
- Martel, J.; Ko, Y.F.; Young, J.D.; Ojcius, D.M. Could nasal breathing help to mitigate the severity of COVID-19. Microbes Infect. 2020, 22, 168–171. [Google Scholar] [CrossRef]
- COVID-19 Coronavirus Pandemic. Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 3 January 2024).
- WHO COVID-19 Dashboard. World Health Organization. Available online: https://data.who.int/dashboards/covid19/ (accessed on 11 September 2021).
- Who Is Worldometers.info? Worldometer. Available online: https://www.worldometers.info/faq/ (accessed on 3 January 2024).
- Statista. Available online: https://www.statista.com/search/?p=1 (accessed on 3 January 2024).
- Wikipedia. Available online: https://en.wikipedia.org/wiki/ (accessed on 29 December 2023).
- La Banque Mondiale. Available online: https://donnees.banquemondiale.org/indicator/EN.POP.DNST (accessed on 10 September 2021).
- Available online: https://fr.wikipedia.org/wiki/Tableau_des_m%C3%A9dailles_des_Jeux_olympiques_d%27%C3%A9t%C3%A9_de_2020 (accessed on 27 December 2023).
- LePan, N. Visualizing the History of Pandemics. Visual Capitalist. March 2020. Available online: https://www.visualcapitalist.com/history-of-pandemics-deadliest/ (accessed on 10 September 2021).

{kind=link}
{kind=link}
| List of Top 30 Countries Ranked by Total Number of COVID-19 Cases as of September 2021 | ||||||
|---|---|---|---|---|---|---|
| Rank | Country | Total Cases | Total Deaths | Population | Area (km2) | Population Density |
| 1 | USA | 80,912,619 | 983,837 | 334,252,383 | 9,834,000 | 34 |
| 2 | India | 42,962,953 | 515,063 | 1,425,775,850 | 3,287,263 | 434 |
| 3 | Brazil | 29,033,052 | 651,988 | 215,089,085 | 8,510,000 | 25 |
| 4 | France | 23,011,998 | 139,243 | 65,515,351 | 551,695 | 119 |
| 5 | UK | 19,119,181 | 162,008 | 68,483,074 | 243,610 | 281 |
| 6 | Russia | 16,861,793 | 355,537 | 146,039,239 | 17,100,000 | 9 |
| 7 | Germany | 15,723,907 | 124,670 | 84,232,506 | 357,592 | 236 |
| 8 | Turkey | 14,326,217 | 95,379 | 85,858,254 | 783,562 | 110 |
| 9 | Italy | 12,991,055 | 155,782 | 60,312,960 | 302,073 | 200 |
| 10 | Spain | 11,100,428 | 100,431 | 46,785,101 | 506,030 | 92 |
| 11 | Argentina | 8,934,328 | 126,708 | 45,890,064 | 2,780,000 | 17 |
| 12 | Iran | 7,084,306 | 137,747 | 85,792,424 | 1,648,000 | 52 |
| 13 | Netherlands | 6,640,403 | 21,608 | 18,001,900 | 41,850 | 430 |
| 14 | Colombia | 6,070,616 | 139,037 | 51,790,765 | 1,141,748 | 45 |
| 15 | Poland | 5,734,042 | 112,535 | 37,777,204 | 322,575 | 117 |
| 16 | Indonesia | 5,723,858 | 149,918 | 278,365,371 | 1,905,000 | 146 |
| 17 | Mexico | 5,554,392 | 319,604 | 131,200,388 | 1,973,000 | 66 |
| 18 | Japan | 5,274,596 | 24,604 | 125,828,159 | 377,973 | 333 |
| 19 | Ukraine | 4,862,459 | 106,485 | 43,293,825 | 603,628 | 72 |
| 20 | Vietnam | 4,292,564 | 40,726 | 98,804,778 | 331,690 | 298 |
| 21 | S. Korea | 4,212,652 | 8796 | 51,343,064 | 100,210 | 512 |
| 22 | South Africa | 3,683,172 | 99,543 | 60,560,331 | 1,220,000 | 50 |
| 23 | Israel | 3,669,119 | 10,274 | 9,326,000 | 22,145 | 421 |
| 24 | Philippines | 3,666,672 | 56,879 | 112,022,278 | 300,439 | 373 |
| 25 | Czechia | 3,624,963 | 38,911 | 10,742,247 | 78,867 | 136 |
| 26 | Malaysia | 3,595,172 | 33,173 | 33,060,108 | 330,803 | 100 |
| 27 | Belgium | 3,586,292 | 30,259 | 11,674,074 | 30,688 | 380 |
| 28 | Peru | 3,524,504 | 210,995 | 33,740,598 | 1,285,215 | 26 |
| 29 | Australia | 3,344,617 | 5403 | 25,995,140 | 7,688,000 | 3 |
| 30 | Portugal | 3,322,134 | 21,182 | 10,146,927 | 92,152 | 110 |
| Total | 362,444,064 | 4,978,325 | 3,807,699,448 | |||
| Population Densities (PD: Inhabitants per Square Kilometer) of Cities and Municipalities among the Most Affected by COVID-19 | ||||||
|---|---|---|---|---|---|---|
| Cities or Municipalities | States | Countries | ||||
| Rank | Name | PD | Name | PD | Name | PD |
| 1 | Buenos Aires | 15,372 | Argentina | 17 | ||
| 2 | Cordoba | 2274 | ||||
| 1 | Sao Paulo | 8149 | Brazil | 25 | ||
| 5 | Rio de Janerio | 4836 | ||||
| 1 | Montréal-Nord | 7623 | Québec | 6 | Canada | 4 |
| 1 | Peel | 1283 | Ontario | 14 | ||
| 1 | Bogota | 4100 | Colombia | 42 | ||
| 2 | Prague | 2737 | Czechia | 136 | ||
| 2 | London | 5598 | England | 260 | ||
| 1 | Cologne | 2649 | Germany | 235 | ||
| 2 | Munich | 4988 | ||||
| 3 | Hanover | 2600 | ||||
| 1 | Tokyo | 6511 | Japan | 328 | ||
| 2 | Osaka | 5740 | ||||
| 1 | Putrajaya | 1387 | Malaysia | 99 | ||
| 1 | Mexico City | 6163 | Mexico | |||
| 1 | Utrecht | 3705 | Netherlands | 461 | ||
| 2 | Rotterdam | 2995 | ||||
| 1 | Quezon City | 17,666 | Philippines | 369 | ||
| 2 | Cavite | 2835 | ||||
| 3 | Laguna | 1725 | ||||
| 1 | Moscow | 10,900 | Russia | 8 | ||
| 2 | Saint-Petersburg | 3850 | ||||
| 1 | Gyeonggi | 1335 | South Korea | 531 | ||
| 2 | Seoul | 17,000 | ||||
| 3 | Busan | 4791 | ||||
| 1 | Kyiv city | 3531 | Ukraine | 71 | ||
| 1 | Los Angeles | 3206 | California | 98 | USA | 36 |
| 2 | San Diego | 1636 | ||||
| 1 | Brooklyn | 14,917 | New York | 166 | ||
| 2 | Queens | 8542 | ||||
| 3 | Manhattan | 28,154 | ||||
| 1 | Hanoi | 2398 | Vietnam | 290 | ||
| 2 | Ho Chi Minh City | 4481 | ||||
| 3 | Hi Phong | 1358 | ||||
| List of Some Major Pandemics in the Christian Era | ||||||
|---|---|---|---|---|---|---|
| Pandemic Name | Begin (y) | End (y) | Duration (ys) | Death Toll | Death Toll/y | Yr Diff |
| Plague of Justinian | 541 | 542 | 1 | 40,000,000 | 40,000,000 | --- |
| Black death (Bubonic Plague) | 1347 | 1351 | 4 | 200,000,000 | 50,000,000 | 806 |
| Smallpox | 1520 | 1520 | 1 | 56,000,000 | 56,000,000 | 173 |
| The Third Plague | 1855 | 1855 | 1 | 12,000,000 | 12,000,000 | 335 |
| Russian Flu | 1889 | 1890 | 1 | 1,000,000 | 1,000,000 | 34 |
| Spanish Flu | 1918 | 1919 | 1 | 45,000,000 | 45,000,000 | 29 |
| Asian Flu | 1957 | 1958 | 1 | 1,100,000 | 1,100,000 | 39 |
| HIV/AIDS | 1981 | 2022 * | 41 | 42,100,000 | 1,026,829 | 24 |
| COVID-19 | 2019 | 2023 * | 4 | 6,961,398 | 1,740,350 | 38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maurice, R.L. Post-COVID-19: Time to Change Our Way of Life for a Better Future. Epidemiologia 2024, 5, 211-220. https://doi.org/10.3390/epidemiologia5020015
Maurice RL. Post-COVID-19: Time to Change Our Way of Life for a Better Future. Epidemiologia. 2024; 5(2):211-220. https://doi.org/10.3390/epidemiologia5020015
Chicago/Turabian StyleMaurice, Roch Listz. 2024. "Post-COVID-19: Time to Change Our Way of Life for a Better Future" Epidemiologia 5, no. 2: 211-220. https://doi.org/10.3390/epidemiologia5020015
APA StyleMaurice, R. L. (2024). Post-COVID-19: Time to Change Our Way of Life for a Better Future. Epidemiologia, 5(2), 211-220. https://doi.org/10.3390/epidemiologia5020015