
First Successful Fertility Preservation Using Oocyte Vitrification in Patient with Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy

Abstract
1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| APECED | Autoimmune Poly-Endocrinopathy-Candidiasis-Ectodermal Dystrophy |
| APS-I | Autoimmune Polyglandular Syndrome Type I |
| AIRE gene | Autoimmune Regulator Gene |
| POI | Premature Ovarian Insufficiency |
| E2 | Estradiol |
| FSH | Follicle-Stimulating hormone |
| LH | Luteinizing Hormone |
| HRT | Hormone Replacement Therapy |
| GnRH | Gonadotropin-Releasing Hormone |
| hMG | Human Menopausal Gonadotropin |
| hCG | Human Chorionic Gonadotropin |
| PTA | Peripheral Tissue Antigen |
| MHC | Major Histocompatibility Complex |
| TCR | T Cell Receptor |
| cTEC | Cortical Thymic Epithelial Cell |
| mTEC | Medullary Thymic Epithelial Cell |
| P-TEFb | Positive Transcription Elongation Factor b |
| DNA-PK | DNA-Dependent Protein Kinase |
References
- Akirav, E.M.; Ruddle, N.H.; Herold, K.C. The Role of Aire in Human Autoimmune Disease. Nat. Rev. Endocrinol. 2011, 7, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Nagamine, K.; Peterson, P.; Scott, H.S.; Kudoh, J.; Minoshima, S.; Heino, M.; Krohn, K.J.; Lalioti, M.D.; Mullis, P.E.; Antonarakis, S.E.; et al. Positional Cloning of the Apeced Gene. Nat. Genet. 1997, 17, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Husebye, E.S.; Anderson, M.S.; Kämpe, O. Autoimmune Polyendocrine Syndromes. N. Engl. J. Med. 2018, 378, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
- Szeliga, A.; Calik-Ksepka, A.; Maciejewska-Jeske, M.; Grymowicz, M.; Smolarczyk, K.; Kostrzak, A.; Smolarczyk, R.; Rudnicka, E.; Meczekalski, B. Autoimmune Diseases in Patients with Premature Ovarian Insufficiency-Our Current State of Knowledge. Int. J. Mol. Sci. 2021, 22, 2594. [Google Scholar] [CrossRef]
- Komorowska, B. Autoimmune Premature Ovarian Failure. Prz. Menopauzalny 2016, 15, 210–214. [Google Scholar] [CrossRef]
- Saari, V.; Holopainen, E.; Mäkitie, O.; Laakso, S. Pubertal Development and Premature Ovarian Insufficiency in Patients with Apeced. Eur. J. Endocrinol. 2020, 183, 513–520. [Google Scholar] [CrossRef]
- Li, M.; Zhu, Y.; Wei, J.; Chen, L.; Chen, S.; Lai, D. The Global Prevalence of Premature Ovarian Insufficiency: A Systematic Review and Meta-Analysis. Climacteric 2023, 26, 95–102. [Google Scholar] [CrossRef]
- Perheentupa, J. Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy. J. Clin. Endocrinol. Metab. 2006, 91, 2843–2850. [Google Scholar] [CrossRef]
- Takaba, H.; Takayanagi, H. The Mechanisms of T Cell Selection in the Thymus. Trends Immunol. 2017, 38, 805–816. [Google Scholar] [CrossRef]
- Passos, G.A.; Speck-Hernandez, C.A.; Assis, A.F.; Mendes-da-Cruz, D.A. Update on Aire and Thymic Negative Selection. Immunology 2018, 153, 10–20. [Google Scholar] [CrossRef]
- Derbinski, J.; Gäbler, J.; Brors, B.; Tierling, S.; Jonnakuty, S.; Hergenhahn, M.; Peltonen, L.; Walter, J.; Kyewski, B. Promiscuous Gene Expression in Thymic Epithelial Cells Is Regulated at Multiple Levels. J. Exp. Med. 2005, 202, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Mathis, D.; Benoist, C. A Decade of Aire. Nat. Rev. Immunol. 2007, 7, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Stenson, P.D.; Mort, M.; Ball, E.V.; Chapman, M.; Evans, K.; Azevedo, L.; Hayden, M.; Heywood, S.; Millar, D.S.; Phillips, A.D.; et al. The Human Gene Mutation Database (Hgmd(®)): Optimizing Its Use in a Clinical Diagnostic or Research Setting. Hum. Genet. 2020, 139, 1197–1207. [Google Scholar] [CrossRef]
- Akiyama, T.; Shinzawa, M.; Qin, J.; Akiyama, N. Regulations of Gene Expression in Medullary Thymic Epithelial Cells Required for Preventing the Onset of Autoimmune Diseases. Front. Immunol. 2013, 4, 249. [Google Scholar] [CrossRef]
- Ucar, O.; Rattay, K. Promiscuous Gene Expression in the Thymus: A Matter of Epigenetics, Mirna, and More? Front. Immunol. 2015, 6, 93. [Google Scholar] [CrossRef]
- Skrabic, V.; Skrabic, I.; Skrabic, R.; Roje, B.; Simunovic, M. Clinical Characteristics in the Longitudinal Follow-up of Apeced Syndrome in Southern Croatia-Case Series. Genes 2022, 13, 558. [Google Scholar] [CrossRef]
- De Martino, L.; Capalbo, D.; Improda, N.; D’Elia, F.; Di Mase, R.; D’Assante, R.; D’Acunzo, I.; Pignata, C.; Salerno, M. APECED: A Paradigm of Complex Interactions between Genetic Background and Susceptibility Factors. Front. Immunol. 2013, 4, 331. [Google Scholar] [CrossRef]
- Capalbo, D.; Improda, N.; Esposito, A.; De Martino, L.; Barbieri, F.; Betterle, C.; Pignata, C.; Salerno, M. Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy from the Pediatric Perspective. J. Endocrinol. Investig. 2013, 36, 903–912. [Google Scholar]
- Garelli, S.; Dalla Costa, M.; Sabbadin, C.; Barollo, S.; Rubin, B.; Scarpa, R.; Masiero, S.; Fierabracci, A.; Bizzarri, C.; Crinò, A.; et al. Autoimmune Polyendocrine Syndrome Type 1: An Italian Survey on 158 Patients. J. Endocrinol. Investig. 2021, 44, 2493–2510. [Google Scholar] [CrossRef]
- De Vos, M.; Devroey, P.; Fauser, B.C. Primary Ovarian Insufficiency. Lancet 2010, 376, 911–921. [Google Scholar] [CrossRef]
- Saari, V.; Laakso, S.; Tiitinen, A.; Mäkitie, O.; Holopainen, E. Endocrine Disorders and Genital Infections Impair Gynecological Health in Apeced (APS-1). Front. Endocrinol. 2021, 12, 784195. [Google Scholar] [CrossRef] [PubMed]
- Laakso, S.; Holopainen, E.; Betterle, C.; Saari, V.; Vogt, E.; Schmitt, M.M.; Winer, K.K.; Kareva, M.; Sabbadin, C.; Husebye, E.S.; et al. Pregnancy Outcome in Women with Apeced (APS-1): A Multicenter Study on 43 Females with 83 Pregnancies. J. Clin. Endocrinol. Metab. 2022, 107, e528–e537. [Google Scholar] [CrossRef] [PubMed]
- Ahonen, P.; Myllärniemi, S.; Sipilä, I.; Perheentupa, J. Clinical Variation of Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy (Apeced) in a Series of 68 Patients. N. Engl. J. Med. 1990, 322, 1829–1836. [Google Scholar] [CrossRef]
- Reato, G.; Morlin, L.; Chen, S.; Furmaniak, J.; Smith, B.R.; Masiero, S.; Albergoni, M.P.; Cervato, S.; Zanchetta, R.; Betterle, C. Premature Ovarian Failure in Patients with Autoimmune Addison’s Disease: Clinical, Genetic, and Immunological Evaluation. J. Clin. Endocrinol. Metab. 2011, 96, e1255–e1261. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, M.; Bellacchio, E.; Dhamo, R.; Frasca, F.; Betterle, C.; Fierabracci, A. A Novel Homozygous Mutation of the Aire Gene in an Apeced Patient from Pakistan: Case Report and Review of the Literature. Front. Immunol. 2018, 9, 1835. [Google Scholar] [CrossRef]
- Alkhammash, S.; Saumet, J.; Genest, G. Infertility and Pregnancy in Patients with Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy: More Than Just Primary Ovarian Failure? Am. J. Reprod. Immunol. 2019, 82, e13169. [Google Scholar] [CrossRef]
- Alrufaidi, A.M.; Alnashery, M.M.; Alghanimi, A.A.; Elmansor, R.E.A.; Ghazy, R.M. An Uncommon Presentation of Autoimmune Polyglandular Syndrome Type 1 (APS-1)—A Case Report. Clin. Case Rep. 2024, 12, e9015. [Google Scholar] [CrossRef]
- Zheng, W.B.; Li, L.J.; Zhao, D.C.; Wang, O.; Jiang, Y.; Xia, W.B.; Li, M. A Novel Variant in Aire Causing a Rare, Non-Classical Autoimmune Polyendocrine Syndrome Type 1. Mol. Med. Rep. 2020, 22, 1285–1294. [Google Scholar] [CrossRef]
- Ruan, J.; Wang, X.; Jiang, X.; Chen, M. Acquired Pure Red Cell Aplasia and T Cell Large Granular Lymphocytic Leukaemia in Patients with Autoimmune Polyglandular Syndrome Type 1. BMC Med. Genom. 2021, 14, 22. [Google Scholar] [CrossRef]
- Ward, L.; Paquette, J.; Seidman, E.; Huot, C.; Alvarez, F.; Crock, P.; Delvin, E.; Kämpe, O.; Deal, C. Severe Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy in an Adolescent Girl with a Novel Aire Mutation: Response to Immunosuppressive Therapy. J. Clin. Endocrinol. Metab. 1999, 84, 844–852. [Google Scholar] [CrossRef]
- Fierabracci, A.; Lanzillotta, M.; Vorgučin, I.; Palma, A.; Katanić, D.; Betterle, C. Report of Two Siblings with Apeced in Serbia: Is There a Founder Effect of c.769C>T Aire Genotype? Ital. J. Pediatr. 2021, 47, 126. [Google Scholar] [CrossRef] [PubMed]
- Faddy, M.J.; Gosden, R.G.; Gougeon, A.; Richardson, S.J.; Nelson, J.F. Accelerated Disappearance of Ovarian Follicles in Mid-Life: Implications for Forecasting Menopause. Hum. Reprod. 1992, 7, 1342–1346. [Google Scholar] [CrossRef]
- Richardson, S.J.; Senikas, V.; Nelson, J.F. Follicular Depletion During the Menopausal Transition: Evidence for Accelerated Loss and Ultimate Exhaustion. J. Clin. Endocrinol. Metab. 1987, 65, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Borchers, J.; Pukkala, E.; Mäkitie, O.; Laakso, S. Patients with Apeced Have Increased Early Mortality Due to Endocrine Causes, Malignancies and Infections. J. Clin. Endocrinol. Metab. 2020, 105, e2207–e2213. [Google Scholar] [CrossRef] [PubMed]
- Goldman, K.N.; Kramer, Y.; Hodes-Wertz, B.; Noyes, N.; McCaffrey, C.; Grifo, J.A. Long-Term Cryopreservation of Human Oocytes Does Not Increase Embryonic Aneuploidy. Fertil. Steril. 2015, 103, 662–668. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
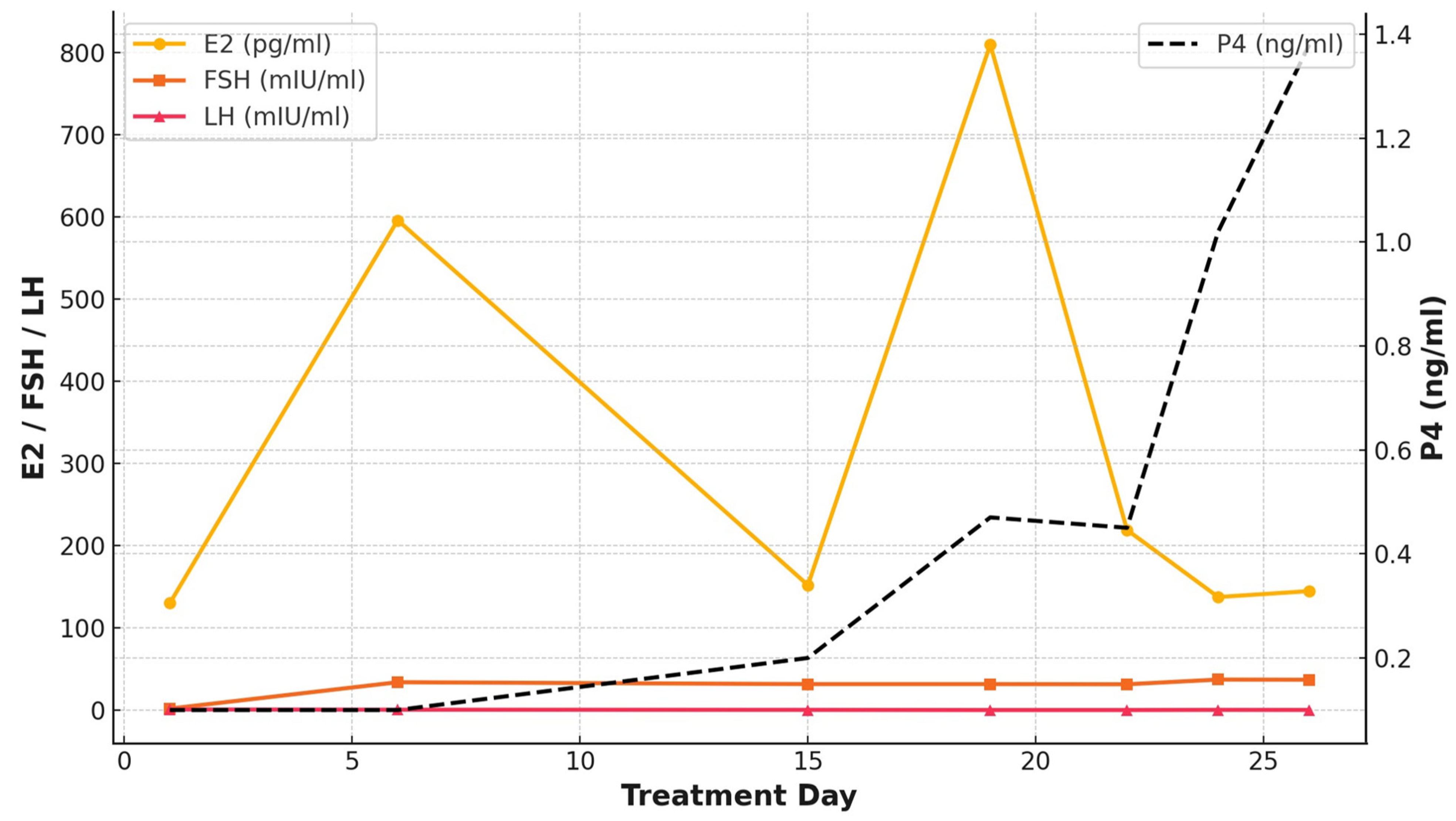
| Treatment Days | 1 | 6 | 15 | 19 | 22 | 24 | 26 | |
|---|---|---|---|---|---|---|---|---|
| Medications | Estradiol valerate (10 mg/1 A) | 1 | 1 | 1 | (-) | (-) | (-) | (-) |
| HMG (IU/day) | 300 | 300 | 300 | 375 | 375 | 375 | 375 | |
| hCG (IU) | 5000 | |||||||
| Conjugated estrogen tablet (0.625 mg/day) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Follicular diameter | Right ovary [mm × (follicle number)] | ND | 3(×3) | 10(×7) | 10(×10) | 12 <10(×10) | 16, 14, <10(×15) | 18, 12, 10, <10(×7) |
| Left ovary [mm × (follicle number)] | ND | 3(×4) | 9(×4) | 9(×7) | 10 <10(×6) | 11, 11, <10(×5) | 11, 11, <10(×5) | |
| Serum hormonal levels | E2 (pg/mL) | 130 | 596.1 | 151.9 | 810 | 219 | 137.5 | 144.7 |
| FSH (mIU/mL) | 1.9 | 34 | 31.7 | 31.7 | 31.5 | 37.2 | 37 | |
| LH (mIU/mL) | 0.9 | 0.6 | 0.4 | <0.2 | <0.2 | 0.4 | 0.3 | |
| P (ng/mL) | <0.1 | <0.1 | 0.2 | 0.47 | 0.45 | 1.02 | 1.38 |
| Cycle | COS Protocol | Follicular Diameter at hCG Trigger [mm × (Follicle Number)] | Number of Collected Oocytes (n) | Number of Mature Oocytes (n) |
|---|---|---|---|---|
| 1 | GnRH agonist Short + FSH/HMG | 18, 15, 15, 15, 14, 13, 12 | 7 | 6 |
| 2 | GnRH agonist Short + FSH/HMG | 16, 15, 12, 10, 10, <10(×7) | 3 | 2 |
| 3 | FSH/HMG alone | 18, 15, <10(×6) | 5 | 2 |
| 4 | FSH/HMG alone | 18, 12, 11, 11, 10, <10(×12) | 12 | 7 |
| Author (Year) | Study Design | Cohort Size (n) | AIRE Mutation | POI Prevalence (%) | POI Onset Age (Years) | AMH Level (ng/mL) | Presence of Ovarian Autoantibodies (%) |
| Ahonen et al. (1990) [23] | Retrospective study | 54 | N/A | 60% (41/54) | No details (range 13–30) | N/A | N/A |
| Reato et al. (2011) [24] | Retrospective study | 49 | N/A | 41% (20/49) | Median 24.1 (range 14–39) | N/A | POI: 84.6% (11/13) non-POI: 44% (11/25) (Data were available in 38 out of 49 patients.) |
| Saari et al. (2020) [6] | Longitudinal follow-up study | 40 | c.769C>T/c.769C>T (75%:30/40) c.769C>T/other (15%:6/40) c.769C>T/x (5%:2/40) Unknown (5%:2/40) | 70% (28/40) | Median 16.0 (range 11.3–36.5) | N/A | POI: 81% (22/27) non-POI: 30% (3/10) (Data were available in 37 out of 40 patients.) |
| Saari et al. (2021) [21] | Cross-sectional study | 19 | c.769C>T (p.Arg257Ter) (79%:15/19) c.932G>A (p.Cys311Tyr) (5.3%:1/19) c.967_979del13 (p.Leu323fs) (5.3%:1/19) c.137C>G (p.Thr46Arg) (5.3%:1/19) c.901G>A (p.Val301Met) (5.3%:1/19) | 84% (16/19) | Median 16.5 (range 11.3–36.5) | Undetectable AMH (<0.03): 79% (15/19), detectable AMH cases: 0.27, 0.04, and 0.89 (Data of one patient are not available in the literature.) | N/A |
| Garelli et al. (2021) [19] | Retrospective study | 103 | R139X (21.3%:58/272 *) R257X (11.8%:32/272) W78R (11.4%:31/272) C322fsX372 (8.8%:24/272) T16M (6.2%:17/272) R203X (4.0%:11/272) A21V (2.9%:8/272) Less frequent mutations 12.9%, very rare 9.6%, no mutations 11% | 50% (51/103) | Mean 22 ± 7.2 | N/A | POI: 85% (35/41) non-POI: 57% (24/42) (Data were available in 83 out of 103 patients.) |
| Laakso et al. (2022) [22] | Multinational retrospective study | 321 ** | c.769C>T, p.(Arg257Ter) 51% (22/43 ***) c.967_979del13, p.(Leu327fs) 21% (9/43) Other 16% (7/43) Unknown 12% (5/43) | 40% (17/43) | Median 28 (range 13–39) | N/A | N/A |
| Author (Year) | Pregnancy Outcomes | Pregnancy Method | Pregnancy Complications | Live Birth Rate | |||
| Ahonen et al. (1990) [23] | 2 pregnancies in 2 patients | N/A | N/A | N/A | |||
| Reato et al. (2011) [24] | N/A | N/A | N/A | N/A | |||
| Saari et al. (2020) [6] | POI: 8 pregnancies in 7 patients non-POI:7 pregnancies in 4 patients | POI: Spontaneous pregnancy 50% (4/8) Ovum donation 50% (4/8) non-POI: Spontaneous pregnancy 71% (5/7) Infertility treatment 29% (2/7) | POI: Spontaneous miscarriage 38% (3/8) (2 from spontaneous pregnancy, and 1 from ovum donation) Induced abortion 13% (1/8) non-POI: Induced abortion 29% (2/7) (2 from spontaneous pregnancy) | POI: 50% (4/8) (2 from spontaneous pregnancy, 2 from ovum donation) non-POI: 71% (5/7) (3 from spontaneous pregnancy, 2 from infertility treatment) | |||
| Saari et al. (2021) [21] | 10 pregnancies in 8 patients | Spontaneous pregnancy 50% (5/10) Ovum donation 50% (5/10) | N/A | N/A | |||
| Garelli et al. (2021) [19] | N/A | N/A | N/A | N/A | |||
| Laakso et al. (2022) [22] | POI: 7 pregnancies in 5 patients non-POI: 76 pregnancies in 38 patients | POI: Spontaneous pregnancy 29% (2/7) Ovum donation 71% (5/7) non-POI: Spontaneous pregnancy 96% (73/76) Infertility treatment 4% (3/76) | POI: Miscarriage 43% (3/7) non-POI: Miscarriage 14% (11/76) Stillbirths 3% (2/76) **** Preterm births 7% (5/76) Gestational diabetes mellitus 1% (1/76) Placental complications 4% (3/76) | POI: 57% (4/7) non-POI: 80% (56/76) | |||
| Author (Year) | AIRE Gene Mutation | Age of POI Onset (Years) | AMH Level (ng/mL) | Presence of Ovarian Autoantibodies | Pregnancy Status | Pregnancy Method | Pregnancy Complications | Live Birth |
|---|---|---|---|---|---|---|---|---|
| Ward et al. (1999) [30] | L93R | 13.6 | N/A | N/A | N/A | N/A | N/A | N/A |
| Pellegrino et al. (2018) [25] | c.396G>C (p.R132S), homozygous | 14.8 | N/A | Positive | N/A | N/A | N/A | N/A |
| Alkhammash et al. (2019) [26] | N/A | N/A | N/A | N/A | 1 | Ovum donation | Gestational diabetes Hypertension | N/A |
| Zheng et al. (2020) [28] | c.623G>T | 18 | N/A | N/A | N/A | N/A | N/A | N/A |
| Ruan et al. (2021) [29] | Heterozygous mutations c.371C>T and c.623G>T | 21 | N/A | N/A | N/A | N/A | N/A | N/A |
| Fierabracci et al. (2021) [31] | c.769C>T (R257X) | 16 | N/A | N/A | N/A | N/A | N/A | N/A |
| Alrufaidi et al. (2024) [27] | Homozygous pathogenic variants (No details) | 28 | N/A | Positive | N/A | N/A | N/A | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, Y.; Ishizuka, B.; Kawamura, K. First Successful Fertility Preservation Using Oocyte Vitrification in Patient with Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy. Endocrines 2025, 6, 31. https://doi.org/10.3390/endocrines6030031
Tanaka Y, Ishizuka B, Kawamura K. First Successful Fertility Preservation Using Oocyte Vitrification in Patient with Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy. Endocrines. 2025; 6(3):31. https://doi.org/10.3390/endocrines6030031
Chicago/Turabian StyleTanaka, Yuka, Bunpei Ishizuka, and Kazuhiro Kawamura. 2025. "First Successful Fertility Preservation Using Oocyte Vitrification in Patient with Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy" Endocrines 6, no. 3: 31. https://doi.org/10.3390/endocrines6030031
APA StyleTanaka, Y., Ishizuka, B., & Kawamura, K. (2025). First Successful Fertility Preservation Using Oocyte Vitrification in Patient with Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy. Endocrines, 6(3), 31. https://doi.org/10.3390/endocrines6030031