
Oncocytic Adenoma in a Pediatric Patient: A Case Report and Literature Review

 ,
,
Abstract
1. Introduction
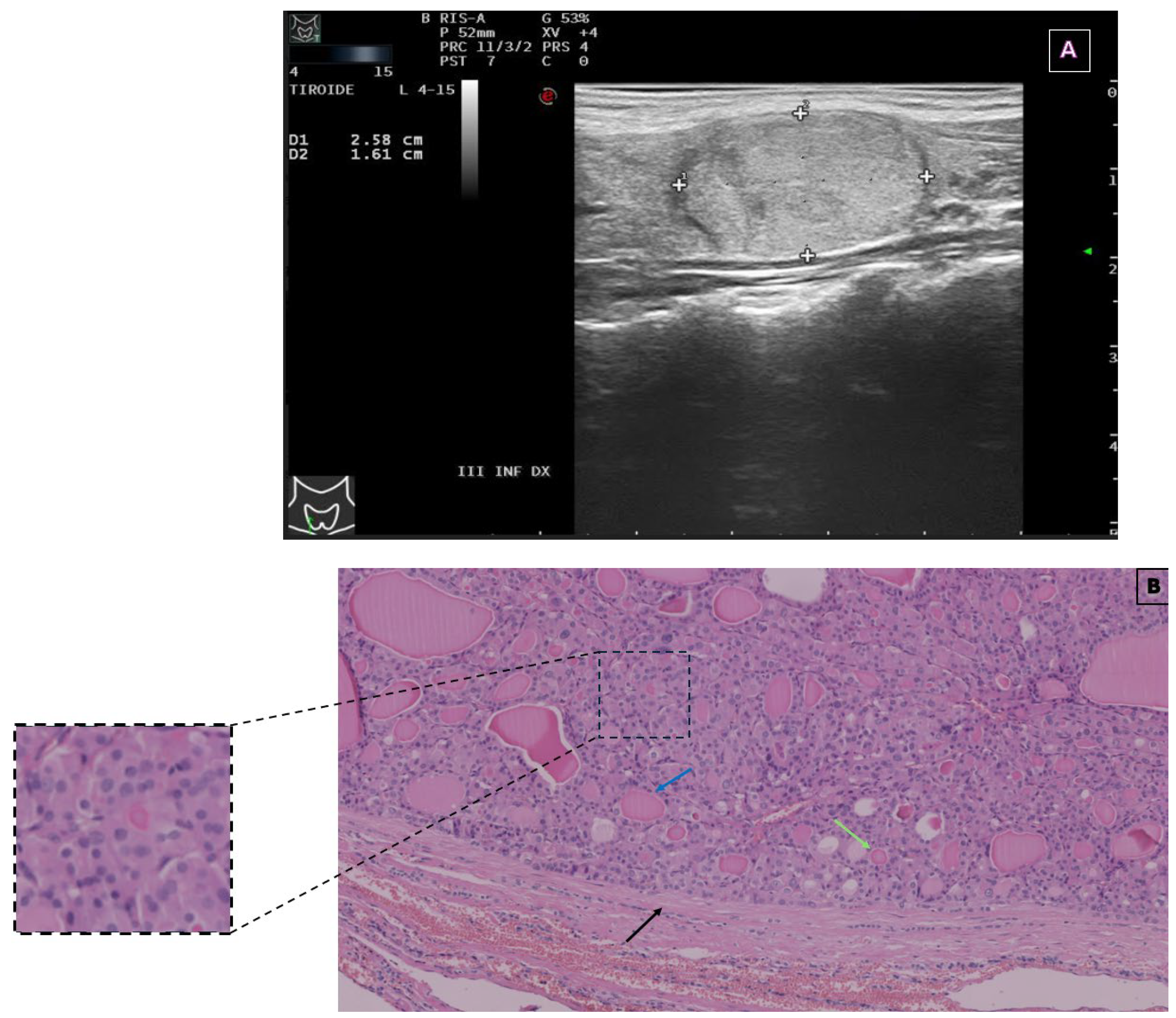
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EU-TIRADS | European Thyroid Imaging and Reporting Data System |
| FNA | Fine-needle aspiration |
| FT3 | Free tri-iodothyronine |
| FT4 | Free thyroxine |
| OA | Oncocytic adenoma |
| OC | Oncocytic carcinoma |
| SIAPEC | Italian Society of Anatomic Pathology and Diagnostic Cytopathology |
| TgAb | Anti-thyroglobulin antibodies |
| TPOAb | Thyroid peroxidase antibodies |
| TSH | Thyroid-stimulating hormone |
References
- Durante, C.; Hegedüs, L.; Czarniecka, A.; Paschke, R.; Russ, G.; Schmitt, F.; Soares, P.; Solymosi, T.; Papini, E. 2023 European Thyroid Association Clinical Practice Guidelines for Thyroid Nodule Management. Eur. Thyroid. J. 2023, 12, e230067. [Google Scholar] [CrossRef] [PubMed]
- Gharib, H.; Papini, E.; Paschke, R.; Duick, D.S.; Valcavi, R.; Hegedüs, L.; Vitti, P. AACE/AME/ETA Task Force on Thyroid Nodules; American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules: Executive Summary of Recommendations. Endocr. Pract. 2010, 16, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Suzuki, S.; Fukushima, T.; Midorikawa, S.; Shimura, H.; Matsuzuka, T.; Ishikawa, T.; Takahashi, H.; Ohtsuru, A.; Sakai, A.; et al. Comprehensive Survey Results of Childhood Thyroid Ultrasound Examinations in Fukushima in the First Four Years After the Fukushima Daiichi Nuclear Power Plant Accident. Thyroid 2016, 26, 843–851. [Google Scholar] [CrossRef]
- Rallison, M.L.; Dobyns, B.M.; Keating, F.R.; Rall, J.E.; Tyler, F.H. Thyroid Nodularity in Children. JAMA 1975, 233, 1069–1072. [Google Scholar] [CrossRef]
- Creo, A.; Alahdab, F.; Al Nofal, A.; Thomas, K.; Kolbe, A.; Pittock, S.T. Ultrasonography and the American Thyroid Association Ultrasound-Based Risk Stratification Tool: Utility in Pediatric and Adolescent Thyroid Nodules. Horm. Res. Paediatr. 2018, 90, 93–101. [Google Scholar] [CrossRef]
- Hanley, P.; Lord, K.; Bauer, A.J. Thyroid Disorders in Children and Adolescents: A Review. JAMA Pediatr. 2016, 170, 1008–1019. [Google Scholar] [CrossRef]
- Carlomagno, F.; Minnetti, M.; Angelini, F.; Pofi, R.; Sbardella, E.; Spaziani, M.; Aureli, A.; Anzuini, A.; Paparella, R.; Tarani, L.; et al. Altered Thyroid Feedback Loop in Klinefelter Syndrome: From Infancy Through the Transition to Adulthood. J. Clin. Endocrinol. Metab. 2023, 108, e1329–e1340. [Google Scholar] [CrossRef] [PubMed]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification of Thyroid Nodules in Adults: The EU-TIRADS. Eur. Thyroid J. 2017, 6, 225–237. [Google Scholar] [CrossRef]
- Francis, G.L.; Waguespack, S.G.; Bauer, A.J.; Angelos, P.; Benvenga, S.; Cerutti, J.M.; Dinauer, C.A.; Hamilton, J.; Hay, I.D.; Luster, M.; et al. Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Pediatric Thyroid Cancer. Thyroid 2015, 25, 716–759. [Google Scholar] [CrossRef]
- McFadden, D.G.; Sadow, P.M. Genetics, Diagnosis, and Management of Hürthle Cell Thyroid Neoplasms. Front. Endocrinol. 2021, 12, 696386. [Google Scholar] [CrossRef]
- Gopal, R.K.; Kübler, K.; Calvo, S.E.; Polak, P.; Livitz, D.; Rosebrock, D.; Sadow, P.M.; Campbell, B.; Donovan, S.E.; Amin, S.; et al. Widespread Chromosomal Losses and Mitochondrial DNA Alterations as Genetic Drivers in Hürthle Cell Carcinoma. Cancer Cell 2018, 34, 242–255.e5. [Google Scholar] [CrossRef]
- Wong, K.S.; Angell, T.E.; Barletta, J.A.; Krane, J.F. Hürthle Cell Lesions of the Thyroid: Progress Made and Challenges Remaining. Cancer Cytopathol. 2021, 129, 347–362. [Google Scholar] [CrossRef]
- Cibas, E.S.; Ali, S.Z. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2017, 27, 1341–1346. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.Z.; Baloch, Z.W.; Cochand-Priollet, B.; Schmitt, F.C.; Vielh, P.; VanderLaan, P.A. The 2023 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2023, 33, 1039–1044. [Google Scholar] [CrossRef] [PubMed]
- Grant, C.S. Operative and Postoperative Management of the Patient with Follicular and Hürthle Cell Carcinoma. Do They Differ? Surg. Clin. N. Am. 1995, 75, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Nardi, F.; Basolo, F.; Crescenzi, A.; Fadda, G.; Frasoldati, A.; Orlandi, F.; Palombini, L.; Papini, E.; Zini, M.; Pontecorvi, A.; et al. Italian Consensus for the Classification and Reporting of Thyroid Cytology. J. Endocrinol. Investig. 2014, 37, 593–599. [Google Scholar] [CrossRef]
- Corrias, A.; Mussa, A.; Baronio, F.; Arrigo, T.; Salerno, M.; Segni, M.; Vigone, M.C.; Gastaldi, R.; Zirilli, G.; Tuli, G.; et al. Diagnostic Features of Thyroid Nodules in Pediatrics. Arch. Pediatr. Adolesc. Med. 2010, 164, 714–719. [Google Scholar] [CrossRef]
- Gupta, A.; Ly, S.; Castroneves, L.A.; Frates, M.C.; Benson, C.B.; Feldman, H.A.; Wassner, A.J.; Smith, J.R.; Marqusee, E.; Alexander, E.K.; et al. A Standardized Assessment of Thyroid Nodules in Children Confirms Higher Cancer Prevalence Than in Adults. J. Clin. Endocrinol. Metab. 2013, 98, 3238–3245. [Google Scholar] [CrossRef]
- Green, O.; Keisling, M.; Kambalapalli, M.; McDaniel, J.; Boulanger, S.; Fornwalt, B.E.; Jeyakumar, A. Unusual Thyroid Mass in an Adolescent Patient. Ear Nose Throat J. 2022, 101, 654–656. [Google Scholar] [CrossRef]
- Kochummen, E.; Tong, S.; Umpaichitra, V.; Chin, V.L. A Unique Case of Bilateral Hürthle Cell Adenoma in an Adolescent. Horm. Res. Paediatr. 2017, 87, 136–142. [Google Scholar] [CrossRef]
- Bremer, A.A.; Feldman, B.J.; Iezza, G.; Clark, O.H.; Rosenthal, S.M. Report of a Hürthle Cell Neoplasm in a Peripubertal Girl. Thyroid 2007, 17, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Roggli, V.L.; Estrada, R.; Fechner, R.E. Thyroid Neoplasia Following Irradiation for Medulloblastoma: Report of Two Cases. Cancer 1979, 43, 2232–2238. [Google Scholar] [CrossRef] [PubMed]
- Nagamachi, Y.; Nakamura, T.; Yamada, T. Hürthle Cell Adenoma of the Thyroid in Identical Twins with 13 Year Follow-Up. Jpn. J. Surg. 1973, 3, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Doerfler, W.R.; Nikitski, A.V.; Morariu, E.M.; Ohori, N.P.; Chiosea, S.I.; Landau, M.S.; Nikiforova, M.N.; Nikiforov, Y.E.; Yip, L.; Manroa, P. Molecular Alterations in Hürthle Cell Nodules and Preoperative Cancer Risk. Endocr. Relat. Cancer 2021, 28, 301–309. [Google Scholar] [CrossRef]
- Goswami, P.; Patel, T.; Dave, R.; Singh, G.; Singh, A.; Kalonia, T. WHO 2022 Updates on Follicular Cell and C-Cell Derived Thyroid Neoplasm. J. Med. Life 2024, 17, 15–23. [Google Scholar] [CrossRef]
- Baloch, Z.W.; Asa, S.L.; Barletta, J.A.; Ghossein, R.A.; Juhlin, C.C.; Jung, C.K.; LiVolsi, V.A.; Papotti, M.G.; Sobrinho-Simões, M.; Tallini, G.; et al. Overview of the 2022 WHO Classification of Thyroid Neoplasms. Endocr. Pathol. 2022, 33, 27–63. [Google Scholar] [CrossRef]
- Caturegli, P.; Ruggere, C. Karl Hürthle! Now, Who Was He? Thyroid 2005, 15, 121–123. [Google Scholar] [CrossRef]
- Auger, M. Hürthle Cells in Fine-needle Aspirates of the Thyroid: A Review of Their Diagnostic Criteria and Significance. Cancer Cytopathol. 2014, 122, 241–249. [Google Scholar] [CrossRef]
- Asa, S.L. My Approach to Oncocytic Tumours of the Thyroid. J. Clin. Pathol. 2004, 57, 225–232. [Google Scholar] [CrossRef]
- Montone, K.T.; Baloch, Z.W.; LiVolsi, V.A. The Thyroid Hürthle (Oncocytic) Cell and Its Associated Pathologic Conditions: A Surgical Pathology and Cytopathology Review. Arch. Pathol. Lab. Med. 2008, 132, 1241–1250. [Google Scholar] [CrossRef]
- Elliott, D.D.; Pitman, M.B.; Bloom, L.; Faquin, W.C. Fine-Needle Aspiration Biopsy of Hurthle Cell Lesions of the Thyroid Gland: A Cytomorphologic Study of 139 Cases with Statistical Analysis. Cancer 2006, 108, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Okere, P.; Olusina, D.; Enyinnah, M. Hurthle Cell Tumor of the Thyroid Gland: Report of a Rare Case and Review of Literature. Niger. J. Clin. Pract. 2014, 17, 375–377. [Google Scholar] [CrossRef]
- Barnabei, A.; Ferretti, E.; Baldelli, R.; Procaccini, A.; Spriano, G.; Appetecchia, M. Hurthle Cell Tumours of the Thyroid. Personal Experience and Review of the Literature. ACTA Otorhinolaryngol. Ital. 2009, 29, 305–311. [Google Scholar] [PubMed]
- Zirilli, G.; Santucci, S.; Cuzzupè, C.; Corica, D.; Pitrolo, E.; Salzano, G. Peculiarities of Autoimmune Polyglandular Syndromes in Children and Adolescents. Acta Bio-Medica Atenei Parm. 2017, 88, 271–275. [Google Scholar]
- Zirilli, G.; Valenzise, M.; Dionigi, G.; Tuccari, G.; Romeo, C.; Campennì, A.; Corrias, A.; Tuli, G.; Ieni, A.; Pajno, G.B.; et al. Hurthle Cell Carcinoma in Childhood: A Retrospective Analysis of Five Cases and Review of Pediatric Literature. Pediatr. Blood Cancer 2020, 67, e28300. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Micangeli, G.; Menghi, M.; Profeta, G.; Paparella, R.; Tarani, F.; Petrella, C.; Barbato, C.; Minni, A.; Greco, A.; Ferraguti, G.; et al. Malignant and Benign Head and Neck Tumors of the Pediatric Age: A Narrative Review. Curr. Pediatr. Rev. 2024, 212, 118–132. [Google Scholar] [CrossRef]

{kind=link}
| Thyroid Function Test | Result | Reference Range |
|---|---|---|
| FT3 | 3.4 pg/mL | 2.3–4.2 |
| FT4 | 1.09 ng/dL | 0.8–1.6 |
| TSH | 1.81 mIU/mL | 0.4–3.5 |
| Calcitonin | <0.5 pg/mL | <6.4 |
| TPOAb | 30 U/mL | <60 |
| TgAb | <10 U/mL | <4.5 |
| Study | Age (Years)/Gender | Nodule Size | Presentation | FNA Cytology | Treatment | Outcome |
|---|---|---|---|---|---|---|
| Current case | 13/Female | 26 × 16 mm | Enlarging neck mass | Bethesda IV (follicular neoplasm with oncocytic features) | Hemithyroidectomy | No recurrence |
| Green et al., 2020 [19] | 18/Female | 5.9 × 4.4 × 3.7 cm | Incidentally identified neck mass, mild hyperthyroid symptoms | Rare clusters of cells with cytological atypia, negative for nuclear features of papillary carcinoma | Left hemithyroidectomy | No recurrence |
| Kochummen et al., 2017 [20] | 14/Female | Bilateral nodules (sizes not specified) | Enlarging thyroid nodules | Not specified | Sequential hemithyroidectomy | No recurrence |
| Bremer et al., 2007 [21] | 12/Female | 20 mm | Palpable thyroid nodule | Suspicious for follicular neoplasm | Hemithyroidectomy | No recurrence |
| Roggli et al., 1979 [22] 1 | 22/Female | Multiple nodules (largest: 4 cm) | Neck mass 18 years after medulloblastoma treatment | Not specified | Subtotal thyroidectomy (95%) | No recurrence (8.5-month follow-up) |
| Nagamachi et al., 1973 [23] | 12/Female (Twin 1) | Left lobe: single cystic tumor (~egg-sized); right lobe: three nodules (~10 mm each) | Enlarging cervical mass | Not specified | Local removal (First surgery), hemithyroidectomy (Second surgery) | No recurrence (13-year follow-up) |
| Nagamachi et al., 1973 [23] | 12/Female (Twin 2) | Left lobe: 1 cm nodule; right lobe: 3 cm cystic nodule | Enlarging cervical mass | Not specified | Local removal (First surgery), hemithyroidectomy (Second surgery) | No recurrence (13-year follow-up) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paparella, R.; Bellone, G.; Rizza, L.; Veccia, N.; Ricci, G.; Calvani, M.; Scommegna, S. Oncocytic Adenoma in a Pediatric Patient: A Case Report and Literature Review. Endocrines 2025, 6, 22. https://doi.org/10.3390/endocrines6020022
Paparella R, Bellone G, Rizza L, Veccia N, Ricci G, Calvani M, Scommegna S. Oncocytic Adenoma in a Pediatric Patient: A Case Report and Literature Review. Endocrines. 2025; 6(2):22. https://doi.org/10.3390/endocrines6020022
Chicago/Turabian StylePaparella, Roberto, Giulia Bellone, Laura Rizza, Norman Veccia, Gabriele Ricci, Mauro Calvani, and Salvatore Scommegna. 2025. "Oncocytic Adenoma in a Pediatric Patient: A Case Report and Literature Review" Endocrines 6, no. 2: 22. https://doi.org/10.3390/endocrines6020022
APA StylePaparella, R., Bellone, G., Rizza, L., Veccia, N., Ricci, G., Calvani, M., & Scommegna, S. (2025). Oncocytic Adenoma in a Pediatric Patient: A Case Report and Literature Review. Endocrines, 6(2), 22. https://doi.org/10.3390/endocrines6020022