
The Progression of Prediabetes to Type 2 Diabetes in Children and Adolescents in the United States: Current Challenges and Solutions

1
Division of Endocrinology, Department of Pediatrics, Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY 11549, USA
2
Children’s Diabetes Center, 1991 Marcus Avenue, Suite M100, Queens, NY 11042, USA
Endocrines 2022, 3(3), 545-551; https://doi.org/10.3390/endocrines3030045
Submission received: 20 July 2022
/
Revised: 19 August 2022
/
Accepted: 22 August 2022
/
Published: 1 September 2022
(This article belongs to the Section Obesity, Diabetes Mellitus and Metabolic Syndrome)
{kind=link}
{kind=link}
Abstract
:Prediabetes, the precursor of type 2 diabetes (T2D), is on the rise among children and adolescents in the United States. The natural history of prediabetes is poorly characterized in children compared to adults. The available data indicate a phenotype of an accelerated β-cell failure in youth with prediabetes. Data from randomized controlled trials showed no benefit on β-cell preservation or A1c in youth with prediabetes from therapeutic agents such as metformin and insulin. As a result, the American Diabetes Association recommends only lifestyle intervention, but not therapeutic agents, for the management of prediabetes in children and adolescents. These recommendations for lifestyle modification in youth, largely derived from data in adults, lack the precision necessary for efficacy in youth. However, a recent 4-year real-world study on youth reported that adherence to nutrition visits was associated with a 4-fold reduction in the likelihood of progressing from prediabetes to T2D. The finding that this reversal is associated with reduced insulin resistance (IR) and not with decreased body weight is novel and provides the foundation for trialing investigational products that may protect β-cells and reduce IR and/or body weight. This study provides the much-needed foundation for further exploration of the impact of lifestyle modification in conjunction with other approaches for the reversal of prediabetes in youth. The systematization of the protocol for medical nutrition therapy for the reversal of prediabetes in youth will ensure optimal and consistent results from adherent patients. This communication provides updates on the pathobiology of prediabetes in youth and a clear direction for efficacious studies in the field.
1. Introduction
There has been a sharp rise in the triad of childhood obesity, prediabetes, and overt type 2 diabetes (T2D) in children and adolescents in the United States [1,2,3,4]. The prevalence of prediabetes, the precursor of T2D, has risen significantly from 11.6% in 1999–2002 to 28.2% in 2015–2018 among US children and adolescents [5]. This sharp increase is on target to reach and exceed the current prevalence of prediabetes in adults of 34% [3,6]. This high prevalence translates to 96 million adults living with prediabetes in the United States [7].
Prediabetes has no confirmatory definition [1]. The American Diabetes Association (ADA) has designated any one of three criteria for the definition of prediabetes. These criteria are a hemoglobin A1c (HbA1c) level of 5.7% to 6.4%; impaired glucose tolerance (IGT), i.e., a 2 h postprandial glucose level of 140–199 mg/dL following 75 g of oral glucose intake; and impaired fasting glucose (IFG), i.e., a fasting plasma glucose level of 100–125 mg/dL [8]. Two nationwide studies have confirmed the suitability and specificity of HbA1c for defining prediabetes in children and adolescents [1,5]. The reported prevalence of prediabetes in studies could vary as a result of the parameters used for its definition [3,6].
This lack of a confirmatory definition for prediabetes contrasts with the established diagnostic criteria for the various types of diabetes mellitus, such as type 1 diabetes (T1D), type 2 diabetes (T2D), and other specific types of diabetes mellitus, such as the maturity-onset diabetes of the young (MODY). In these conditions, the diagnosis of diabetes mellitus is established using either a fasting blood glucose level of ≥126 mg/dL, a 2 h postprandial glucose level of ≥200 mg/dL following an oral glucose tolerance test, or a casual blood glucose level of ≥200 mg/dL with symptoms [8]. Additionally, a hemoglobin A1c level of ≥6.5% is now an acceptable marker for the diagnosis of T2D in children and adolescents [8].
The confirmation of a diagnosis of T1D requires the detection of diabetes-associated autoantibodies in serum [9], while the confirmation of a diagnosis of MODY requires the establishment of a strong family history of the disease and molecular genetic testing for associated mutations [10,11]. The establishment of the diagnosis of T2D is based on a strong family history of the disease, physical examination findings, a negative diabetes-associated autoantibody profile, and variable levels of insulin resistance (IR) [12].
Prediabetes is associated with accelerated β-cell loss in children and adolescents [13]. In adults, it is associated with severe health consequences, as reported by a Danish population study that found the highest risk for major adverse cardiovascular events and all-cause mortality in subjects with prediabetes [14]. A study [15] of 1.7 million adults in the US reported that after adjusting for confounders, prediabetes increased the odds for myocardial infarction by about 41% (MI, OR 1.41, 95% CI 1.35–1.47), as well as the risks for percutaneous coronary artery procedures (OR 1.45, 95% CI 1.37–1.53) and coronary artery bypass grafting (OR 1.95, 95% CI 1.77–2.16) [14].
Despite these severe health implications, prediabetes remains poorly characterized in children and adolescents, as the determinants of the natural history of prediabetes are poorly defined in this population [1,3]. Only a few clinical trials have been designed to investigate therapeutic approaches for prediabetes in children and adolescents [16] compared to adults. These trials are mostly of short duration with reported short-term outcomes, thus preventing translation to clinical care [16]. Therefore, the current recommendations for the management of prediabetes in children are derived from studies in adults [16].
This is problematic, as prediabetes has a more severe phenotype in children than in adults [2,17]. This phenomenon is demonstrated by several physiological processes [16], namely, (i) increased IR and an elevated insulinemic response to glucose infusion compared to adults [18], (ii) increased weight gain in youth with prediabetes who received metformin compared to weight loss in adults who received metformin [18] (iii) a worsening of β-cell function in children and adolescents compared to β-cell preservation in adults [13], and (iv) a longer prodromal phase of 5–10 years to progress from prediabetes to T2D in adults [17] versus only 2–3 years in youth [2]. Therefore, these age-related differences in β-cell dynamics, marked by the accelerated β-cell failure in children and adolescents with prediabetes who received metformin and/or insulin, suggest that newer agents or therapeutic modalities are needed to manage prediabetes in this population [13,16]. To address this knowledge gap, we recently conducted a 4-year study on the impact of adherence to medical nutrition therapy (MNT) on prediabetes. Its primary aim was to investigate the rate of progression from prediabetes to T2D in the first 4 years following the diagnosis of prediabetes, while the secondary aim was to determine the effect of adherence to MNT on the reversion from prediabetes to normoglycemia.
2. Lack of Consensus on the Approaches to the Management of Prediabetes in Children and Adolescents
There is a fundamental difference in the therapeutic recommendations for adults and youth with prediabetes based on the results of clinical trials in these two age groups. In children and adolescents, current trials have shown no consistent efficacy data to warrant the approval of therapeutic agents in this population. This was demonstrated by the multi-center, randomized clinical trial (RCT) called the Restoring Insulin Secretion (RISE) study [13]. This RCT simultaneously enrolled children and adults who had either impaired glucose tolerance (IGT) or were recently diagnosed with T2D and followed them for 15 months. The RCT found that metformin and glargine insulin had no beneficial effect on β-cell function in youth, in contrast to the significant beneficial effects of these agents in adults. The RISE study also found no sustained impact on the prevention of the progression to T2D following the withdrawal of metformin or insulin glargine in children and adolescents [13]. Thus, the RISE study [13] concluded that the accelerated β-cell loss in youth with prediabetes was not amenable to either metformin or insulin therapy. Further mechanistic studies showed that long-term metformin therapy could worsen the prognosis for prediabetes in youth, as it diffuses across the blood–brain barrier and augments appetite by stimulating orexigenic receptors in the hypothalamus [19]. The rest of the clinical studies in children and adolescents were of a short (≤6 month) duration [16] with limited outcomes. A review of these studies showed some evidence of improved insulin sensitivity from orlistat [20], metformin [21,22,23], and rosiglitazone [24]. An intensive lifestyle modification protocol improved the insulin sensitivity and 2 h postprandial glucose concentrations during an oral glucose tolerance test [25,26]. As a result of these poor efficacy data, the ADA does not recommend either metformin or insulin glargine as therapeutic agents for prediabetes in children and adolescents [16].
In contrast, some studies in adults have demonstrated a short-term effect of decreasing the rate of progression of prediabetes to T2D. These include the institution of intensive glycemic control using basal insulin [27], lifestyle modification [28], diet and exercise [29], weight loss, metformin [30], orlistat [31], thiazolidinediones [32], and gastric bypass [33]. In contrast, interventions with meglitinides [34], acarbose [35], and sulfonylureas [36] showed less efficacy on reversing the progression from prediabetes to T2D.
Given the failure of the therapeutic agents studied so far in clinical trials in youth to protect the β-cells and reverse the trajectory of prediabetes to T2D, it is prudent to study the impact of other less-studied agents, such as vitamin D, to determine the effects of their immunomodulatory properties on the reversion of prediabetes in children and adolescents. This paradigm is predicated on the results of a recent RCT by the author that reported evidence for β-cell protection by vitamin D [37]. Currently, there is a paucity of data on the impact of vitamin D supplementation on the natural history of prediabetes in youth. Most of the available studies on vitamin D were conducted on adults; some showed that vitamin D supplementation could reduce diabetes risk [38], while others did not [39]. A large meta-analysis [40] on vitamin D supplementation and prediabetes concluded that low 25(OH)D concentrations increased the risk for prediabetes, and that vitamin D supplementation improved impaired glucose tolerance in patients with prediabetes. A second meta-analysis [41] of subjects with prediabetes reported that vitamin D supplementation improved the fasting blood glucose, A1c, and fasting insulin concentration compared to controls. This meta-analysis suggested that long-term vitamin D supplementation could improve the markers of insulin activity, such as HOMA-IR and HOMA-B. A subgroup analysis from a meta-analysis that reported no beneficial effect of vitamin D on improving IR in prediabetes [42] found that vitamin D improved HOMA-IR among subjects with a 25(OH)D of ≥50 nmol/L. This subgroup analysis further showed that in patients with a baseline 25(OH)D of <50 nmol/L, vitamin D supplementation significantly reduced the 2 h oral glucose tolerance test plasma glucose, fasting plasma glucose, and HbA1c levels. However, the impact of vitamin D supplementation on the reversal of the progression of prediabetes to T2D has not been adequately studied in children and adolescents, either as a monotherapy or in conjunction with other therapeutic approaches.
3. New Data on the Efficacy of Medical Nutrition Therapy in Children and Adolescents with Prediabetes
In a recently published study [43], we provided evidence for the efficacy of adherence to MNT to reverse prediabetes in children and adolescents. Over the 4-year duration of the study, 14 (22.6%) of the 62 non-adherent subjects progressed to T2D, at a mean period of progression to T2D of 25.8 ± 12.6 months. In contrast, 4 (9.1%) of the 44 adherent subjects progressed to T2D, at a mean period of progression to T2D of 34.9 ± 11.8 months. Figure 1 shows that the hazard ratio for the progression from prediabetes to T2D for the non-adherent subjects compared to the adherent subjects was 3.88 (95% CI 1.26 to 11.98, p = 0.02) [43].
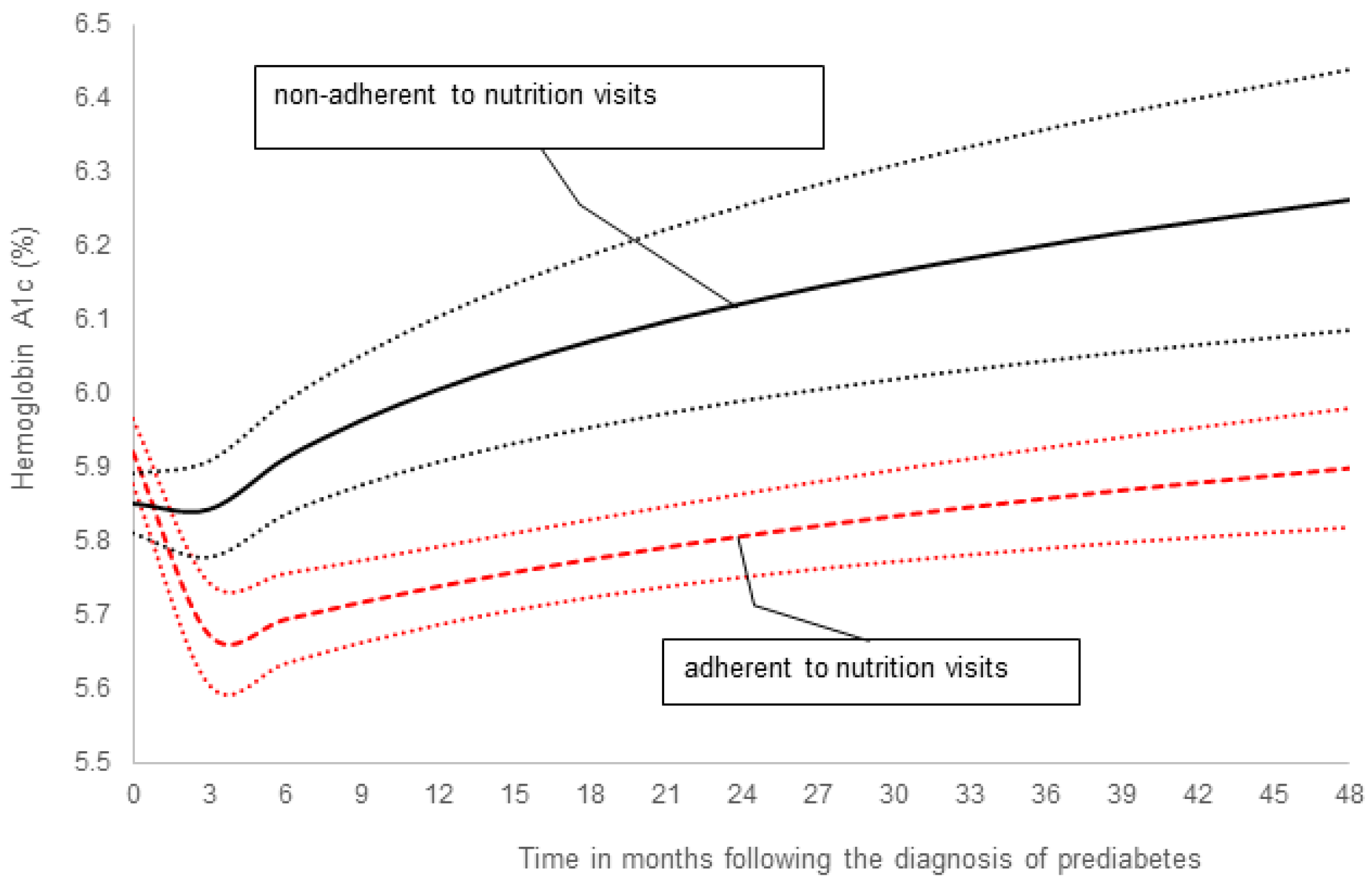
Figure 2 [43] shows a significant difference in the HbA1c trend between the two groups (p = 0.01) after adjusting for confounders.
The BMI z-scores were higher in the adherent group versus the non-adherent group (p = 0.003). There were no changes in the BMI z-score between the consecutive time points for both the adherent and non-adherent groups.
4. Discussion
The triad of the rising prevalence of prediabetes in US children and adolescents [5], the increased cardiovascular risk associated with prediabetes [14], and the dearth of data on therapeutic approaches for the management of prediabetes in children [16] represent a significant deficiency in healthcare delivery to US youth. Furthermore, the translation of data from adult studies for recommendations in children lacks the precision needed for optimal outcomes in children and adolescents. For example, although lifestyle modification is generally recommended, it is unclear if this recommendation is systematized to yield consistent benefits to the patients. However, the results of our recent study showing a strong benefit from adherence to structured MNT in children and adolescents provide the precision needed for optimal outcomes in this population, while serving as a foundation for further studies in this field. The finding that the reversion to normoglycemia was associated with reduced IR instead of a significant decrease in body weight is novel in the field of prediabetes and indicates that biochemical improvements could occur in the absence of phenotypic changes in body weight. This should be reassuring to patients and their families.
5. Conclusions and Future Directions
There is no approved therapeutic agent for prediabetes in youth. However, our recent study indicates that the systematization of the protocol for MNT could reverse the progression of prediabetes to T2D in children and adolescents and ensure optimal and consistent results from adherent patients. The demonstration of reduced IR, but no change in body weight, in these adherent subjects is novel and suggests that reducing IR might be central to reversing prediabetes in youth. This provides a mechanistic basis for the future trialing of investigational products that may protect the β-cells and reduce IR and/or body weight. This new direction will help reduce the rising prevalence of prediabetes in the US.
Funding
This study was funded in part by an investigator-initiated research grant, Grant ID: 5 R21 DK113353-03, to Benjamin U. Nwosu from NIDDK, NIH.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We thank Alan D. Rogol for his expert review of this manuscript.
Conflicts of Interest
The author has no conflict of interest.
References
- Wallace, A.S.; Wang, D.; Shin, J.-I.; Selvin, E. Screening and Diagnosis of Prediabetes and Diabetes in US Children and Adolescents. Pediatrics 2020, 146, e20200265. [Google Scholar] [CrossRef]
- Galderisi, A.; Giannini, C.; Weiss, R.; Kim, G.; Shabanova, V.; Santoro, N.; Pierpont, B.; Savoye, M.; Caprio, S. Trajectories of changes in glucose tolerance in a multiethnic cohort of obese youths: An observational prospective analysis. Lancet Child Adolesc. Health 2018, 2, 726–735. [Google Scholar] [CrossRef]
- Andes, L.J.; Cheng, Y.J.; Rolka, D.B.; Gregg, E.W.; Imperatore, G. Prevalence of Prediabetes Among Adolescents and Young Adults in the United States, 2005–2016. JAMA Pediatr. 2020, 174, e194498. [Google Scholar] [CrossRef]
- Cunningham, S.A.; Hardy, S.T.; Jones, R.; Ng, C.; Kramer, M.R.; Narayan, K.V. Changes in the Incidence of Childhood Obesity. Pediatrics 2022, 150, e2021053708. [Google Scholar] [CrossRef]
- Liu, J.; Li, Y.; Zhang, D.; Yi, S.S.; Liu, J. Trends in Prediabetes Among Youths in the US From 1999 Through 2018. JAMA Pediatr. 2022, 176, 608. [Google Scholar] [CrossRef]
- Tuso, P. Prediabetes and Lifestyle Modification: Time to Prevent a Preventable Disease. Perm. J. 2014, 18, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Report, National Diabetes Statistics Report Website, Centers for Disease Control and Prevention; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022. [Google Scholar]
- American Diabetes Association. Children and Adolescents: Standards of Medical Care in Diabetes. Diabetes Care 2020, 43, S163–S182. [Google Scholar] [CrossRef] [PubMed]
- DiMeglio, L.A.; Evans-Molina, C.; Oram, R.A. Type 1 diabetes. Lancet 2018, 391, 2449–2462. [Google Scholar] [CrossRef]
- Broome, D.T.; Pantalone, K.M.; Kashyap, S.R.; Philipson, L.H. Approach to the Patient with MODY-Monogenic Diabetes. J. Clin. Endocrinol. Metab. 2021, 106, 237–250. [Google Scholar] [CrossRef]
- Rubio-Cabezas, O.; Hattersley, A.T.; Njølstad, P.R.; Mlynarski, W.; Ellard, S.; White, N.; Chi, D.V.; Craig, M.E. ISPAD Clinical Practice Consensus Guidelines The diagnosis and management of monogenic diabetes in children and adolescents. Pediatr. Diabetes 2014, 15 (Suppl. S20), 47–64. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Khunti, K.; Davies, M.J. Type 2 diabetes. Lancet 2017, 389, 2239–2251. [Google Scholar] [CrossRef]
- RISE Consortium Investigators. Effects of Treatment of Impaired Glucose Tolerance or Recently Diagnosed Type 2 Diabetes With Metformin Alone or in Combination With Insulin Glargine on beta-Cell Function: Comparison of Responses In Youth And Adults. Diabetes 2019, 68, 1670–1680. [Google Scholar]
- Yahyavi, S.K.; Snorgaard, O.; Knop, F.K.; Schou, M.; Lee, C.; Selmer, C.; Gislason, G.; Torp-Pedersen, C.; Jensen, M.B.; Bonde, A.N. Prediabetes Defined by First Measured HbA1c Predicts Higher Cardiovascular Risk Compared With HbA1c in the Diabetes Range: A Cohort Study of Nationwide Registries. Diabetes Care 2021, 44, 2767–2774. [Google Scholar] [CrossRef]
- Thota, G. Prediabetes is a risk factor for myocardial infarction-a national inpatient sample study. In Proceedings of the Annual Endocrine Society Meeting, Atlanta, GA, USA, 12 June 2022. [Google Scholar]
- Magge, S.; Silverstein, J.; Elder, D.; Nadeau, K.; Hannon, T.S. Evaluation and Treatment of Prediabetes in Youth. J. Pediatr. 2020, 219, 11–22. [Google Scholar] [CrossRef]
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef]
- RISE Consortium Investigators. Impact of Insulin and Metformin Versus Metformin Alone on beta-Cell Function in Youth With Impaired Glucose Tolerance or Recently Diagnosed Type 2 Diabetes. Diabetes Care 2018, 41, 1717–1725. [Google Scholar] [CrossRef]
- Coughlan, K.A.; Valentine, R.J.; Ruderman, N.B.; Saha, A.K. AMPK activation: A therapeutic target for type 2 diabetes? Diabetes Metab. Syndr. Obes. Targets Ther. 2014, 7, 241–253. [Google Scholar]
- McDuffie, J.R.; Calis, K.; Uwaifo, G.; Sebring, N.; Fallon, E.; Frazer, T.; Hubbard, V.; Yanovski, J. Efficacy of Orlistat as an Adjunct to Behavioral Treatment in Overweight African American and Caucasian Adolescents with Obesity-related Co-morbid Conditions. J. Pediatr. Endocrinol. Metab. 2004, 17, 307–320. [Google Scholar] [CrossRef]
- Gomez-Diaz, R.; Talavera, J.O.; Pool, E.C.; Ortiz-Navarrete, V.; Solórzano-Santos, F.; Mondragon, R.; Valladares-Salgado, A.; Cruz, M.; Aguilar-Salinas, C.A.; Wacher, N.H. Metformin decreases plasma resistin concentrations in pediatric patients with impaired glucose tolerance: A placebo-controlled randomized clinical trial. Metabolism 2012, 61, 1247–1255. [Google Scholar] [CrossRef]
- Arslanian, S.A.; Lewy, V.; Danadian, K.; Saad, R. Metformin therapy in obese adolescents with polycystic ovary syndrome and impaired glucose tolerance: Amelioration of exaggerated adrenal response to adrenocorticotropin with reduction of insulinemia/insulin resistance. J. Clin. Endocrinol. Metab. 2002, 87, 1555–1559. [Google Scholar] [CrossRef]
- Kendall, D.; Vail, A.; Amin, R.; Barrett, T.; Dimitri, P.; Ivison, F.; Kibirige, M.; Mathew, V.; Matyka, K.; McGovern, A.; et al. Metformin in Obese Children and Adolescents: The MOCA Trial. J. Clin. Endocrinol. Metab. 2013, 98, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Cali, A.M.; Pierpont, B.M.; Taksali, S.E.; Allen, K.; Shaw, M.M.; Savoye, M.; Caprio, S. Rosiglitazone Improves Glucose Metabolism in Obese Adolescents With Impaired Glucose Tolerance: A Pilot Study. Obesity 2011, 19, 94–99. [Google Scholar] [CrossRef]
- Garnett, S.P.; Gow, M.; Ho, M.; Baur, L.A.; Noakes, M.; Woodhead, H.J.; Broderick, C.R.; Burrell, S.; Chisholm, K.; Halim, J.; et al. Optimal Macronutrient Content of the Diet for Adolescents With Prediabetes; RESIST a Randomised Control Trial. J. Clin. Endocrinol. Metab. 2013, 98, 2116–2125. [Google Scholar] [CrossRef] [PubMed]
- Savoye, M.; Caprio, S.; Dziura, J.; Camp, A.; Germain, G.; Summers, C.; Li, F.; Shaw, M.; Nowicka, P.; Kursawe, R.; et al. Reversal of Early Abnormalities in Glucose Metabolism in Obese Youth: Results of an Intensive Lifestyle Randomized Controlled Trial. Diabetes Care 2014, 37, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; Bosch, J.; Dagenais, G.R.; Díaz, R.; Jung, H.; Maggioni, A.P.; Pogue, J.; Probstfield, J.; Ramachandran, A.; Riddle, M.C.; et al. Basal insulin and cardiovascular and other outcomes in dysglycemia. N. Engl. J. Med. 2012, 367, 319–328. [Google Scholar] [CrossRef]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Prevention of Type 2 Diabetes Mellitus by Changes in Lifestyle among Subjects with Impaired Glucose Tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.-R.; Li, G.-W.; Hu, Y.-H.; Wang, J.-X.; Yang, W.-Y.; An, Z.-X.; Hu, Z.-X.; Lin, J.; Xiao, J.-Z.; Cao, H.-B.; et al. Effects of Diet and Exercise in Preventing NIDDM in People With Impaired Glucose Tolerance: The Da Qing IGT and Diabetes Study. Diabetes Care 1997, 20, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, A.; Snehalatha, C.; Mary, S.; Mukesh, B.; Bhaskar, A.D.; Vijay, V.; Indian Diabetes Prevention Programme (IDPP). The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Diabetologia 2006, 49, 289–297. [Google Scholar] [CrossRef]
- Torgerson, J.S.; Hauptman, J.; Boldrin, M.N.; Sjöström, L. XENical in the prevention of diabetes in obese subjects (XENDOS) study: A randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care 2004, 27, 155–161. [Google Scholar] [CrossRef]
- DREAM (Diabetes REduction Assessment with Ramipril and Rosiglitazone Medication) Trial Investigators. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: A randomised controlled trial. Lancet 2006, 368, 1096–1105. [Google Scholar] [CrossRef]
- Carlsson, L.M.; Peltonen, M.; Ahlin, S.; Anveden, C.; Bouchard, C.; Carlsson, B.; Jacobson, P.; Lönroth, H.; Maglio, C.; Näslund, I.; et al. Bariatric Surgery and Prevention of Type 2 Diabetes in Swedish Obese Subjects. N. Engl. J. Med. 2012, 367, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Holman, R.R.; Haffner, S.M.; McMurray, J.J.; Bethel, M.A.; Holzhauer, B.; Hua, T.A.; Belenkov, Y.; Boolell, M.; Buse, J.B.; Buckley, B.M.; et al. Effect of Nateglinide on the Incidence of Diabetes and Cardiovascular Events. N. Engl. J. Med. 2010, 362, 1463–1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiasson, J.-L.; Josse, R.G.; Gomis, R.; Hanefeld, M.; Karasik, A.; Laakso, M.; STOP-NIDDM Trail Research Group. Acarbose for prevention of type 2 diabetes mellitus: The STOP-NIDDM randomised trial. Lancet 2002, 359, 2072–2077. [Google Scholar] [CrossRef]
- Kahn, S.E.; Haffner, S.M.; Heise, M.A.; Herman, W.H.; Holman, R.R.; Jones, N.P.; Kravitz, B.G.; Lachin, J.M.; O’Neill, M.C.; Zinman, B.; et al. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N. Engl. J. Med. 2006, 355, 2427–2443. [Google Scholar] [CrossRef]
- Nwosu, B.U.; Parajuli, S.; Jasmin, G.; Fleshman, J.; Sharma, R.B.; Alonso, L.C.; Lee, A.F.; Barton, B.A. Ergocalciferol in New-onset Type 1 Diabetes: A Randomized Controlled Trial. J. Endocr. Soc. 2022, 6, bvab179. [Google Scholar] [CrossRef]
- Pittas, A.G.; Dawson-Hughes, B.; Sheehan, P.; Ware, J.H.; Knowler, W.C.; Aroda, V.R.; Brodsky, I.; Ceglia, L.; Chadha, C.; Chatterjee, R.; et al. Vitamin D Supplementation and Prevention of Type 2 Diabetes. N. Engl. J. Med. 2019, 381, 520–530. [Google Scholar] [CrossRef]
- Jorde, R.; Sollid, S.T.; Svartberg, J.; Schirmer, H.; Joakimsen, R.M.; Njølstad, I.; Fuskevåg, O.M.; Figenschau, Y.; Hutchinson, M.Y. Vitamin D 20 000 IU per Week for Five Years Does Not Prevent Progression From Prediabetes to Diabetes. J. Clin. Endocrinol. Metab. 2016, 101, 1647–1655. [Google Scholar] [CrossRef]
- Yu, L.; Zhai, Y.; Shen, S. Association between vitamin D and prediabetes: A PRISMA-compliant meta-analysis. Medicine 2020, 99, e19034. [Google Scholar] [CrossRef]
- Zhang, Y.; Xue, Y.; Zhang, D.; Liu, Y.; Xu, Z.; Gao, J.; Li, W.; Li, X. Effect of Vitamin D Supplementation on Glycemic Control in Prediabetes: A Meta-Analysis. Nutrients 2021, 13, 4464. [Google Scholar] [CrossRef]
- Poolsup, N.; Suksomboon, N.; Plordplong, N. Effect of vitamin D supplementation on insulin resistance and glycaemic control in prediabetes: A systematic review and meta-analysis. Diabet. Med. 2016, 33, 290–299. [Google Scholar] [CrossRef]
- Parajuli, S.; Jasmin, G.; Sirak, H.; Lee, A.F.; Nwosu, B.U. Prediabetes: Adherence to Nutrition Visits Decreases HbA1c in Children and Adolescents. Front. Endocrinol. 2022, 13, 916785. [Google Scholar] [CrossRef]
- Chiang, J.-K.; Lai, N.-S.; Chang, J.-K.; Koo, M. Predicting insulin resistance using the triglyceride-to-high-density lipoprotein cholesterol ratio in Taiwanese adults. Cardiovasc. Diabetol. 2011, 10, 93. [Google Scholar] [CrossRef] [Green Version]
- Rajappa, M.; Sridhar, M.G.; Balachander, J.; Sethuraman, K.R.; Rajendiran, K.S. Lipoprotein Ratios as Surrogate Markers for Insulin Resistance in South Indians with Normoglycemic Nondiabetic Acute Coronary Syndrome. ISRN Endocrinol. 2014, 2014, 981524. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Kaplan–Meier survival analysis of the progression from prediabetes to type 2 diabetes (T2D). The hazard ratio of progression from prediabetes to T2D for the non-adherent subjects compared to the adherent subjects was 3.88 (95% CL 1.26–11.98, p = 0.02) [43].
Figure 1.
Kaplan–Meier survival analysis of the progression from prediabetes to type 2 diabetes (T2D). The hazard ratio of progression from prediabetes to T2D for the non-adherent subjects compared to the adherent subjects was 3.88 (95% CL 1.26–11.98, p = 0.02) [43].
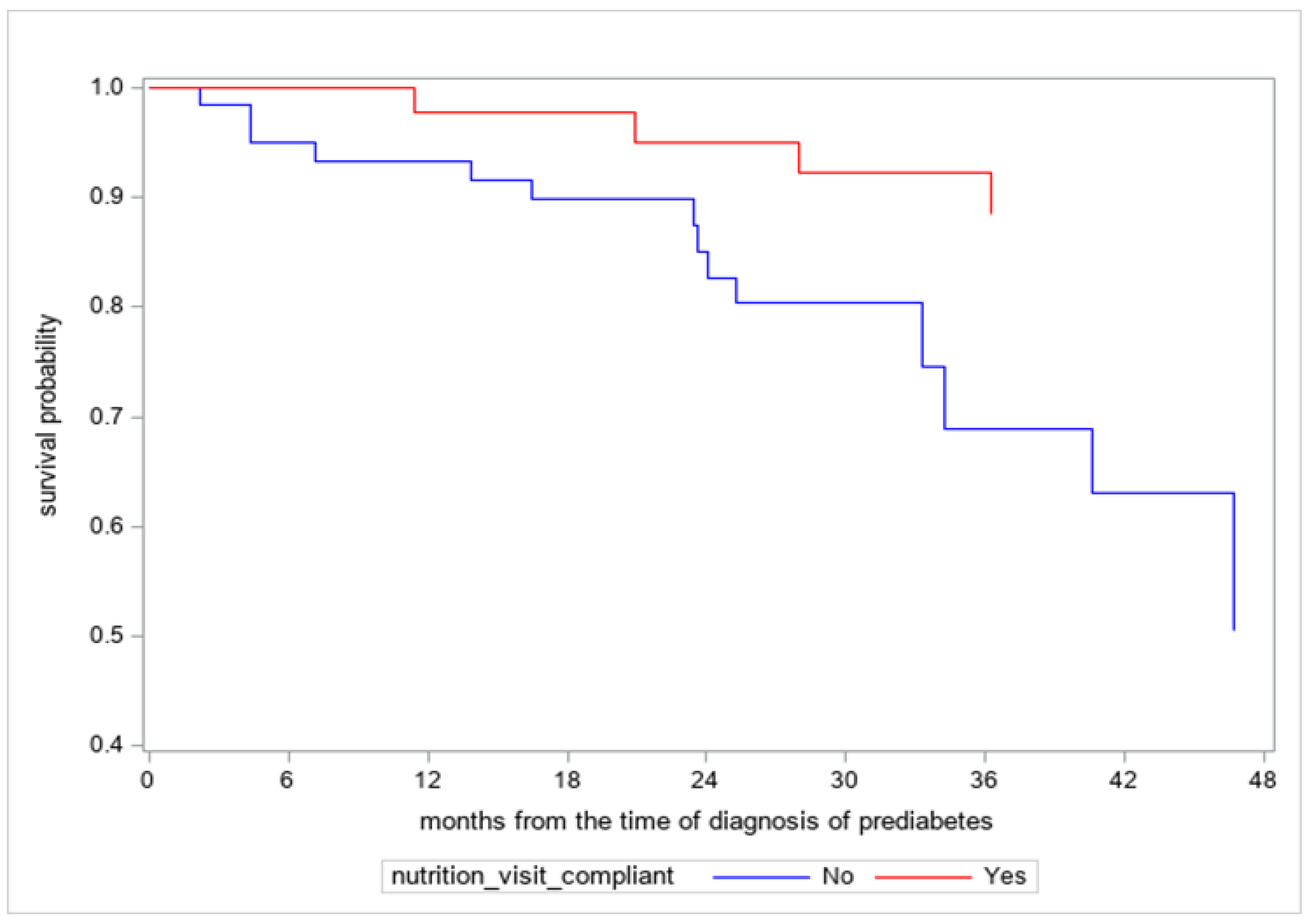
Figure 2.
A graphical representation of the comparison of trends in hemoglobin A1c between the adherent and non-adherent subjects. This shows that the difference in HbA1c trends between the two groups remained significant after adjusting for age, sex, race/ethnicity, metformin use, and BMI z-scores (p = 0.01) [43].
Figure 2.
A graphical representation of the comparison of trends in hemoglobin A1c between the adherent and non-adherent subjects. This shows that the difference in HbA1c trends between the two groups remained significant after adjusting for age, sex, race/ethnicity, metformin use, and BMI z-scores (p = 0.01) [43].
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Nwosu, B.U. The Progression of Prediabetes to Type 2 Diabetes in Children and Adolescents in the United States: Current Challenges and Solutions. Endocrines 2022, 3, 545-551. https://doi.org/10.3390/endocrines3030045
AMA Style
Nwosu BU. The Progression of Prediabetes to Type 2 Diabetes in Children and Adolescents in the United States: Current Challenges and Solutions. Endocrines. 2022; 3(3):545-551. https://doi.org/10.3390/endocrines3030045
Chicago/Turabian StyleNwosu, Benjamin Udoka. 2022. "The Progression of Prediabetes to Type 2 Diabetes in Children and Adolescents in the United States: Current Challenges and Solutions" Endocrines 3, no. 3: 545-551. https://doi.org/10.3390/endocrines3030045