Abstract
Combined heart-liver transplantation (CHLT) is a viable option for concurrent heart and liver failure, yet its indications are unclear. This preliminary study aimed to describe pre-transplant characteristics and outcomes of patients with liver fibrosis undergoing HT and CHLT, while exploring decompensated liver dysfunction following HT. A total of 52 patients (HT = 42; CHLT = 10) were included. In HT patients, F1 fibrosis was more common (52%), with 43% exhibiting F3 or F4 fibrosis. F4 fibrosis was predominant in the CHLT patients (80%). Post-hepatic portal hypertension was present in 62% of HT and 90% of CHLT patients. None progressed to liver decompensation (i.e., new ascites, variceal bleed, jaundice, hepatic hydrothorax, or hepatic encephalopathy) after HT. Over a median follow-up period of 3.7 [IQR 1.2–9.1] years, the two groups did not differ statistically in survival (p = 0.60). Altogether, HT and CHLT may have similar survival outcomes, and HT patients may not progress to decompensation postoperatively despite advanced fibrosis. Decompensated cirrhosis could serve as a factor for identifying CHLT candidates, but it is crucial to differentiate it from post-hepatic portal hypertension, which does not necessitate liver transplant. Further research is needed to determine selection criteria for CHLT, ensuring efficient utility of organs.
1. Introduction
The first-ever combined heart and liver transplantation (CHLT) was performed in 1984, treating a 6-year-old girl suffering from familial hypercholesterolemia and cardiovascular disease [1]. According to data from the Organ Procurement and Transplantation Network (OPTN), there have been 584 documented cases of CHLT from 1 January 1988 to 31 March 2024. Over the past two decades, this procedure has garnered widespread acceptance within the medical community, with 68 medical centers across the United States currently offering CHLT services [2]. Both the number of adults receiving CHLT and the number of centers performing the procedure have increased significantly [3]. While the range of conditions warranting CHLT are varied, they primarily encompass familial amyloid polyneuropathy, heart failure accompanied by cardiac cirrhosis, primary liver disease concurrent with end-stage cardiac issues, and familial hypercholesterolemia [4,5]. Remarkably, congenital heart disease has surpassed non-congenital heart conditions as the predominant indication for CHLT in the United States [4,5,6,7,8]. Restrictive and infiltrative cardiomyopathy was the most common until 2010, but in recent years, congenital heart disease has become the leading cause, accounting for 30.9% of CHLT cases compared to 16.5% in the previous decade [3].
Several studies have indicated that CHLT yields comparable graft and patient survival rates to isolated heart transplantation (HT) in carefully selected patients [2,5]. Within the transplant community, however, there is significant debate around determining which patients with heart failure and liver disease would benefit from CHLT compared to HT alone. Currently, there are few published protocols or guidelines for listing CHLT candidates [9,10,11]. Furthermore, CHLT raises ethical concerns about organ allocation, particularly regarding the principles of utility and equity. While CHLT offers life-saving treatment to individuals with complex medical conditions, allocating livers to CHLT candidates bypasses individuals awaiting liver-alone transplants. This highlights the need for transparent, fair, and evidence-based allocation policies that prioritize maximizing benefits for all transplant patients. Identifying the most suitable candidates for CHLT ensures fairness and justice in allocation [12]. This preliminary study aimed to describe pre-transplant characteristics and outcomes of patients with liver fibrosis undergoing HT and CHLT, while also exploring the incidence of decompensated hepatic dysfunction following HT.
2. Materials and Methods
2.1. Design
This retrospective cohort study compared pre-transplant characteristics and survival outcomes between 52 adult patients who underwent HT (42) and CHLT (10) at Cleveland Clinic Main Campus between 1 January 2009 and 30 August 2022. Recipients of other combined solid organ transplants were excluded from the analysis. The study was approved by Cleveland Clinic’s Institutional Review Board.
2.2. Outcomes
The primary outcome was survival after transplantation (i.e., the time from transplantation to death or last follow-up). The secondary outcome was new decompensation of underlying liver disease among the HT group, characterized by the occurrence of ascites, hepatic encephalopathy, variceal bleeding, hepatic hydrothorax, or jaundice after HT over the course of the study.
2.3. Variables
During chart review, pre-transplant characteristics including age, sex, transplant date, and age at transplantation were extracted. Etiology of heart failure (e.g., non-ischemic, ischemic, or congenital cardiomyopathies) and etiology of liver disease (e.g., primary liver disease or secondary to congestive hepatopathy from underlying heart failure) were extracted. Portal hypertension can occur as pre-hepatic, intra-hepatic, or post-hepatic. Cirrhosis is the primary cause of intra-hepatic portal hypertension, accounting for more than 90% of cases [13,14]. However, non-cirrhotic post-hepatic portal hypertension can develop in heart failure due to hemodynamic changes, resulting in increased preload and back pressure in the hepatic system. Prolonged hepatic congestion may eventually lead to congestive hepatopathy and liver cirrhosis [14]. In the cardiac patient population, portal hypertension typically manifests as post-hepatic or intra-hepatic. Post-hepatic portal hypertension is characterized by pervasive elevation of pressures throughout the cardiovascular system, affecting the portal system. Thus, its presence was defined as right atrial pressure of 8 mmHg or greater. Conversely, intra-hepatic portal hypertension exhibits a discernible gradient between the portal vein and the inferior vena cava. Its presence was defined as hepatic venous pressure gradient of 5 mmHg or greater.
Left ventricular ejection fraction from pre-operative echocardiograms was recorded. The degree of liver fibrosis was determined using the Batts–Ludwig scoring system (F0 to F4) from the last liver biopsy before transplantation. Pre-operative metabolic and liver function parameters were used to calculate the model for end-stage liver disease excluding INR (MELD-XI). MELD-XI is a modified version of the model for end-stage liver disease, excluding INR, used to assess liver disease severity and predict mortality risk. Scores range from 6 to 40, with higher scores indicating higher mortality risk.
2.4. Statistical Analysis
A survival analysis was conducted using Kaplan–Meier curves to visually inspect differences between HT and CHLT patients. Log-rank analysis was not performed because one of the groups had no events. Cox proportional hazards regression models were not conducted due to limitations imposed by the sample size.
3. Results
The mean age at transplant was 48 years in HT patients and 46 years in CHLT patients, and both patient groups were largely male (Table 1). Among HT patients, there were 23 cases (55%) of non-ischemic cardiomyopathy, 10 cases (24%) of congenital heart diseases, and 9 cases (21%) of ischemic cardiomyopathy; whereas there were 5 cases (50%) of non-ischemic cardiomyopathy, 4 cases (40%) of congenital heart diseases, and 1 case (10%) of ischemic cardiomyopathy among CHLT patients. Among HT patients, 9 (21%) were attributed to primary liver disease, 1 of which was due to transthyretin amyloidosis, and 33 (79%) were attributed to congestive hepatopathy. In contrast, among CHLT patients, there were 5 cases (50%) of primary liver disease, 1 of which was due to transthyretin amyloidosis, and 5 cases (50%) of congestive hepatopathy.

Table 1.
Baseline characteristics in combined heart–liver and isolated heart transplant.
F1 fibrosis was more prevalent in HT patients (52%), followed by F3 (26%), F4 (17%), and F2 (5%). F4 fibrosis was more common in CHLT patients (80%), followed by F2 (10%) and F3 (10%) (Table 1). Post-hepatic portal hypertension was present in 29 (62%) of HT patients and right atrial pressure measurements were not available in 1 (2%). There were no cases of intra-hepatic portal hypertension. In the CHLT group, post-hepatic portal hypertension was present in 9 (90%); right atrial pressure measurements were not available in 1 (10%). Preoperative left ventricular ejection fraction averaged 29% ± 20% for HT and 38% ± 14% for CHLT. Mean pre-transplant MELD-XI values were 11.2 ± 6.5 and 9.16 ± 5.0 for HT and CHLT patients, respectively.
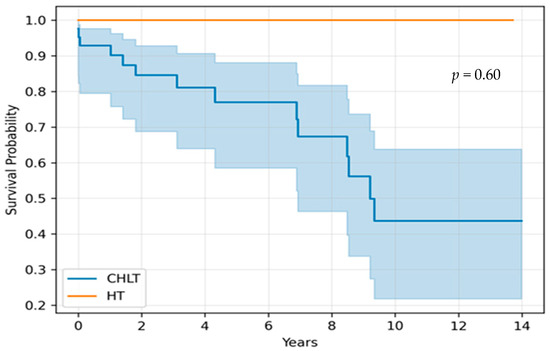
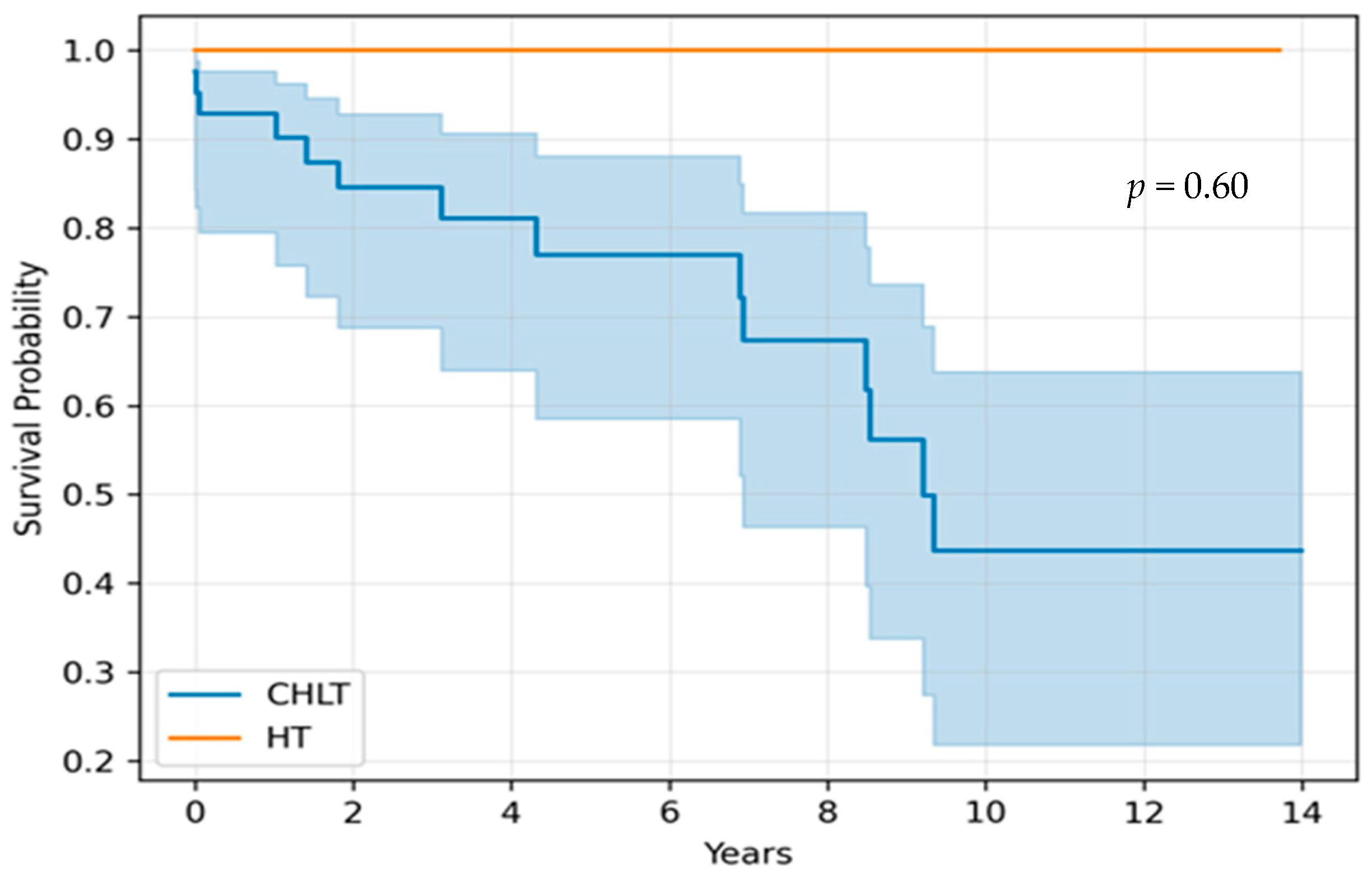
None of the HT patients experienced new decompensation of preexisting liver disease (i.e., ascites, hepatic encephalopathy, variceal bleeding, hepatic hydrothorax, or jaundice after HT). Over a median follow-up period of 3.7 years (interquartile range 1.2–9.1), the two groups did not differ statistically in survival (p = 0.60) (Figure 1). The primary cause of mortality among HT patients was graft dysfunction, followed by intraoperative complications. There were no deaths attributed to liver-related etiologies.
Figure 1.
Kaplan-Meier survival curve in combined heart-liver transplantation (chlt) and isolated heart transplantation (ht).
4. Discussion
Our study describes preliminary survival outcomes between HT and CHLT groups over a 3.7-year median follow-up period. The majority of CHLT patients had cirrhosis (F4) on biopsy and post-hepatic portal hypertension. Similarly, most patients in the HT group exhibited hepatic fibrosis, albeit of lesser severity, and post-hepatic portal hypertension. These patients underwent HT without concurrent liver transplantation and 67% achieved survival. However, the extended operative time and cold-ischemia time required for CHLT could present multiple risk factors for both patient and graft survival. A comprehensive evaluation of the procedure’s outcomes is still needed to determine if these results are generalizable to high-volume centers and to fully assess the overall outcomes. Furthermore, none of these HT patients at our center progressed to decompensation of their underlying liver disease after HT and there was no liver-related mortality. Due to the limited sample size and the lack of statistical power, a multivariate analysis comparing the HT and CHLT groups was not feasible. Nevertheless, we aim to present our institutional experience with CHLT, given the very limited number of such transplants performed annually.
A national survey of participating centers revealed significant variability in listing practices for CHLT, with many centers lacking established protocols. Fifty percent of the centers considered cirrhosis on liver biopsy as an indication for CHLT, while 33% believed that F3 hepatic fibrosis alone warranted CHLT [9]. The current consensus statement recommends CHLT for biopsy-proven fibrosis of any stage with clinical evidence of portal hypertension, or biopsy-proven cirrhosis regardless of portal hypertension [12]. Interestingly, our preliminary findings may suggest the feasibility of considering isolated heart transplantation in select patients presenting with liver fibrosis on biopsy or post-hepatic portal hypertension. While HT and CHLT are not directly comparable in terms of fibrosis grade, it is notable that 43% of HT patients had F3 or F4, with most experiencing post-hepatic portal hypertension. None of the patients with F3 or F4 fibrosis progressed to liver decompensation postoperatively following HT. This observation leads us to speculate that F3 or F4 may not invariably necessitate CHLT. However, future studies incorporating multivariate analysis based on fibrosis grade are needed to substantiate this hypothesis.
Additionally, it is important to recognize that signs and symptoms of portal hypertension may be attributed to non-cirrhotic, post-hepatic portal hypertension, for which a liver transplant is not necessary. This crucial distinction has significant ethical implications since allocating livers to patients who do not require transplantation can mean bypassing those in urgent need. Liver elastography, which measures liver stiffness through non-invasive imaging techniques, may be used to indicate increased stiffness, potentially reflecting hepatic congestion. Although initially developed for liver fibrosis assessment, studying the utility of liver stiffness measurements in heart failure patients could be valuable [15,16].
Over the past few years alone, the number of CHLT procedures has exceeded that of the preceding two decades combined, yet to date, no guidelines on CHLT evaluation and listing practices have been developed [2,3,9]. This is particularly significant because of ethical concerns surrounding organ allocation, as CHLT affects the deceased donor liver transplant waitlist by bypassing individuals awaiting isolated liver transplants [17]. Therefore, recognizing the evolving landscape of CHLT and establishing clear indications for patient selection will be essential to ensure positive outcomes moving forward.
There are several limitations and strengths of our study. The retrospective, single center design may limit generalizability of findings. Additional constraints were posed by missing data, reflective of variability in clinical practice. The lack of events in one group made it difficult to perform statistical analyses like the log-rank test, and the study was underpowered for Cox proportional hazard regression modeling. To address this, we used descriptive statistics and Kaplan–Meier curves to assess trends between groups. Additionally, HT and CHLT are not directly comparable, and the small number of patients precludes subgroup analysis based on fibrosis grade. Notwithstanding, due to the small number of procedures performed annually, our data provide a single center experience from a very large transplant center; and our data provide novel insights into the potential safety of HT among patients with compensated liver dysfunction.
5. Conclusions
In closing, we describe preliminarily outcomes after HT and CHLT, and note that patients with F3 or F4 liver fibrosis did not progress to decompensation after HT. Clinical manifestations of decompensated cirrhosis could serve as a factor for identifying patients who may derive benefit from CHLT. However, it is crucial to differentiate intra-hepatic from post-hepatic portal hypertension, as their presentation is often similar, yet post-hepatic portal hypertension does not necessitate liver transplantation. Further research is needed to empirically guide and establish selection criteria for HT vs. CHLT and to ensure efficient utility of limited organs and optimal outcomes. Currently, CHLT practices are based on retrospective models and subsequent investigations (e.g., prospective multicenter registries) hold promise in facilitating the development of evidence-based guidelines for CHLT.
Author Contributions
Conceptualization, R.M. and J.M.E.; methodology, R.M. and O.T.S.; formal analysis, R.M. and A.F.; investigation, R.M., A.F., O.T.S. and J.M.E.; data curation, R.M.; data interpretation, R.M., A.F., O.T.S. and J.M.E.; writing—original draft preparation, R.M., O.T.S. and J.M.E.; writing—review and editing, R.M., O.T.S., A.F. and J.M.E.; supervision, O.T.S. and J.M.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Cleveland Clinic (approval code #23-588, 14 June 2023).
Informed Consent Statement
Informed consent for participation was not required due to the retrospective nature of the study, as approved by the Institutional Review Board of the Cleveland Clinic.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to IRB restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HT | isolated heart transplant |
| CHLT | combined heart-liver transplantation |
| OPTN | Organ Procurement and Transplantation Network |
| MELD-XI | model for end-stage liver disease excluding INR |
References
- Starzl, T.E.; Bahnson, H.T.; Hardesty, R.L.; Iwatsuki, S.; Gartner, J.C.; Bilheimer, D.W.; Shaw, B.W.; Griffith, B.P.; Zitelli, B.J.; Malatack, J.J.; et al. Heart-Liver Transplantation in a Patient with Familial Hypercholesterolaemia. Lancet 1984, 323, 1382–1383. [Google Scholar] [CrossRef] [PubMed]
- Organ Procurement & Transplantation Network. OPTN. Available online: https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/ (accessed on 11 June 2024).
- Alexopoulos, S.P.; Wu, W.K.; Ziogas, I.A.; Matsuoka, L.K.; Rauf, M.A.; Izzy, M.; Perri, R.; Schlendorf, K.H.; Menachem, J.N.; Shah, A.S. Adult Combined Heart-Liver Transplantation: The United States Experience. Transpl. Int. 2022, 35, 10036. [Google Scholar] [CrossRef] [PubMed]
- Tracy, K.M.; Matsuoka, L.K.; Alexopoulos, S.P. Update on Combined Heart and Liver Transplantation: Evolving Patient Selection, Improving Outcomes, and Outstanding Questions. Curr. Opin. Organ Transplant. 2023, 28, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.S.A.; Challapalli, J.; Maynes, E.J.; Weber, M.P.; Choi, J.H.; O’Malley, T.J.; Entwistle, J.W.; Morris, R.J.; Samuels, L.E.; Massey, H.T.; et al. Indications and Outcomes of Combined Heart-Liver Transplant: A Systematic Review and Met-Analysis. Transplant. Rev. 2020, 34, 100517. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.; Mclean, R.C.; Hoteit, M.A.; Olthoff, K.M. Combined Heart and Liver Transplant: Indication, Patient Selection, and Allocation Policy. Clin. Liver Dis. 2019, 13, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Lebray, P.; Varnous, S. Combined Heart and Liver Transplantation: State of Knowledge and Outlooks. Clin. Res. Hepatol. Gastroenterol. 2019, 43, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Gong, T.; Hall, S. Considerations and Experience Driving Expansion of Combined Heart-Liver Transplantation. Curr. Opin. Organ Transplant. 2020, 25, 496–500. [Google Scholar] [CrossRef] [PubMed]
- Shingina, A.; Chadha, R.; Lim, N.; Pillai, A.; Vodkin, I.; Montenovo, M.; Heller, T.; Yardeni, D.; Ganger, D. Combined Heart-Liver Transplantation Practices Survey in North America: Evaluation and Organ Listing Practices. Liver Transplant. 2023, 29, 591–597. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, B.A.; Fuller, S.; Gleason, L.P.; Hornsby, N.; Wald, J.; Krok, K.; Shaked, A.; Goldberg, L.R.; Pochettino, A.; Olthoff, K.M.; et al. Single-Center Outcomes of Combined Heart and Liver Transplantation in the Failing Fontan. Clin. Transplant. 2017, 31, e12892. [Google Scholar] [CrossRef] [PubMed]
- Reardon, L.C.; Lin, J.P.; VanArsdell, G.S.; Kaldas, F.M.; Lluri, G.; Tan, W.; Whalen, K.M.; Cruz, D.; Nsair, A.; Deng, M.C.; et al. Orthotopic Heart and Combined Heart Liver Transplantation: The Ultimate Treatment Option for Failing Fontan Physiology. Curr. Transplant. Rep. 2021, 8, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Kobashigawa, J.; VanWagner, L.B.; Hall, S.; Emamaullee, J.; Entwistle, J.W.; Ganger, D.; Gebel, H.; Jeevanandam, V.; Kaldas, F.; Kilic, A.; et al. Summary of a Consensus Conference on Heart-Liver Transplantation. Am. J. Transplant. 2024, 24, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Al-Busafi, S.A.; McNabb-Baltar, J.; Farag, A.; Hilzenrat, N. Clinical Manifestations of Portal Hypertension. Int. J. Hepatol. 2012, 2012, 203794. [Google Scholar] [CrossRef] [PubMed]
- Ziccardi, M.R.; Pendela, V.S.; Singhal, M. Cardiac Cirrhosis. In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2023. [Google Scholar]
- Barr, R.G.; Ferraioli, G.; Palmeri, M.L.; Goodman, Z.D.; Garcia-Tsao, G.; Rubin, J.; Garra, B.; Myers, R.P.; Wilson, S.R.; Rubens, D.; et al. Elastography Assessment of Liver Fibrosis: Society of Radiologists in Ultrasound Consensus Conference Statement. Ultrasound Q. 2016, 32, 94–107. [Google Scholar] [CrossRef]
- Dhillon, J.K.; Fong, M.W.; Fong, T.L. Use of Liver Stiffness Measurements in Acute Decompensated Heart Failure: New Applications of a Non-Invasive Technique. ESC Heart Fail. 2022, 9, 2800–2807. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.S.; Wall, A.; Teuteberg, J. Ethical Decision-Making in Simultaneous Heart-Liver Transplantation. Curr. Opin. Organ Transplant. 2020, 25, 519–525. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).