
Comparison of Benefits and Risks Associated with Anti-T-Lymphocyte Globulin (ATLG) Serotherapy in Methotrexate (MTX)- versus Mycophenolate Mofetil (MMF)-Based Hematopoietic Stem Cell Transplantation

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Patients and Treatment
2.2. Definitions and Grading
3. Results
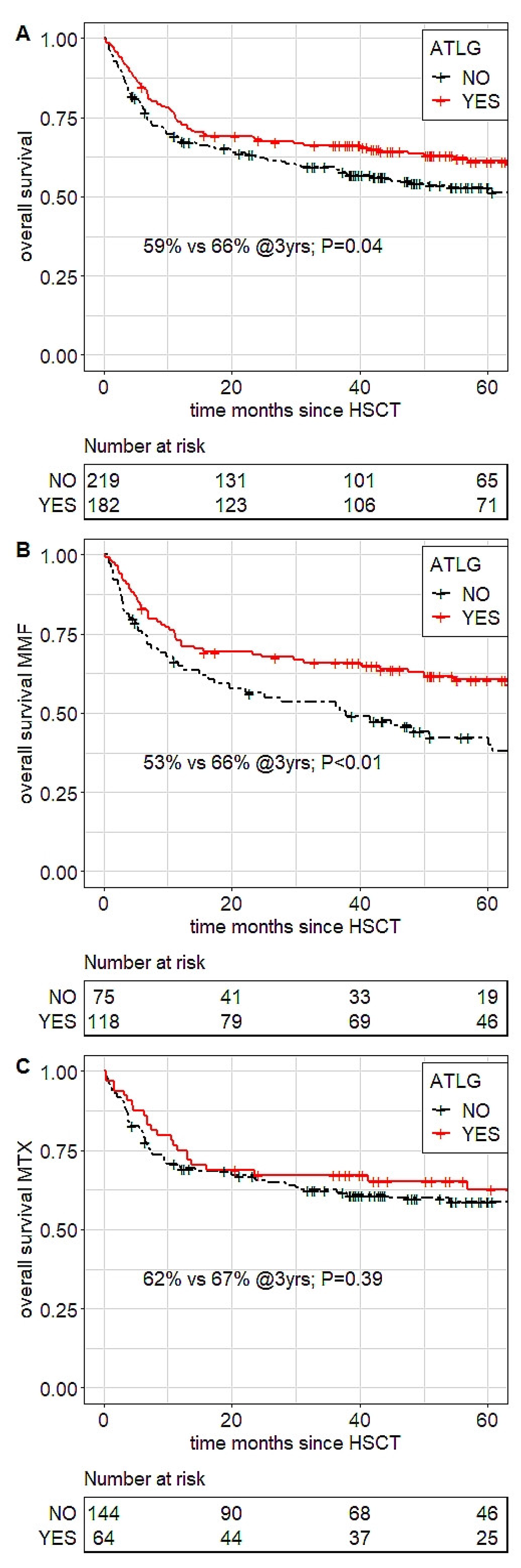
3.1. Overall Survival by ATLG in the MMF versus MTX Setting
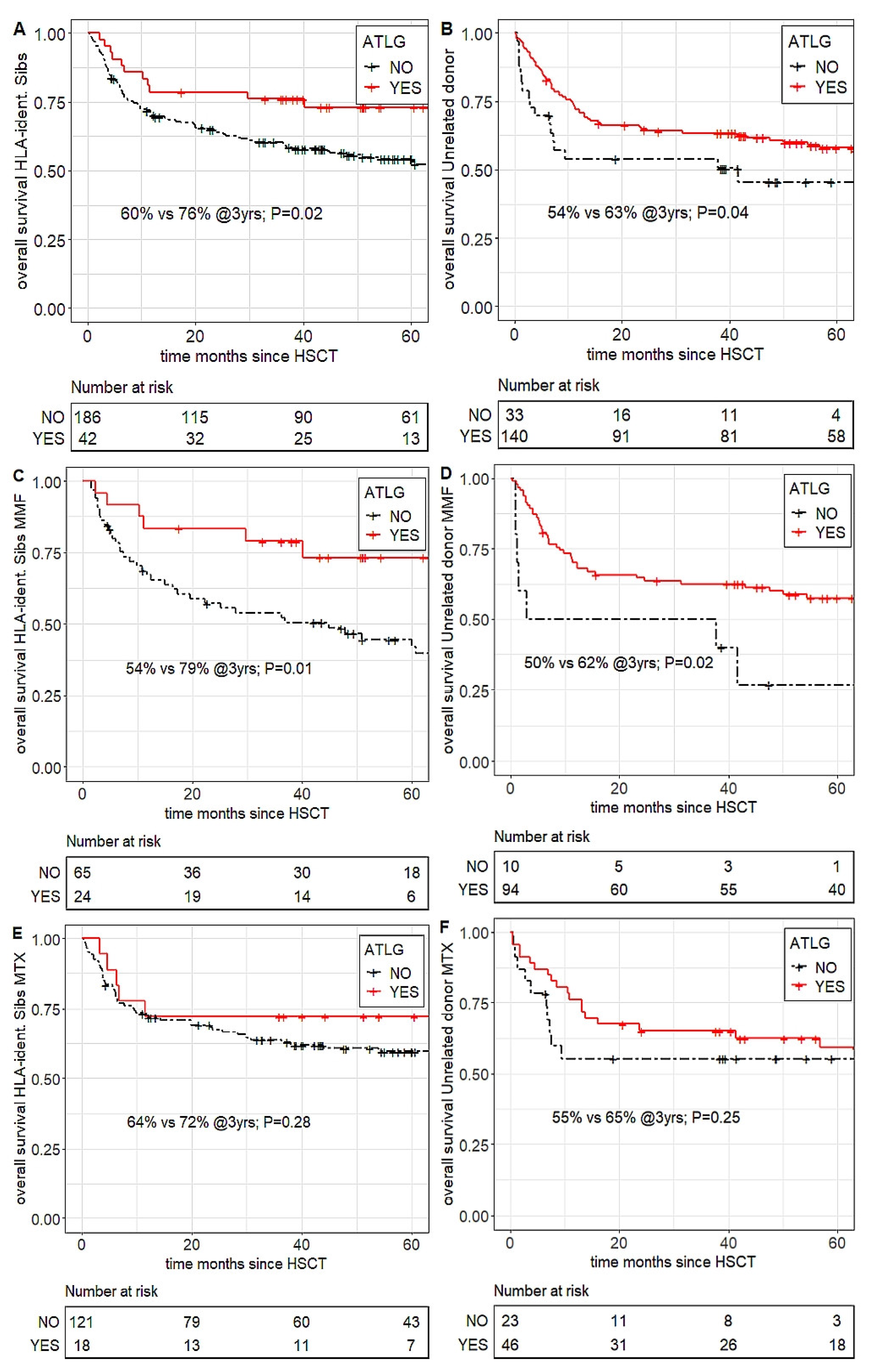
3.2. Overall Survival—Sibling Transplants
3.3. Overall Survival—Unrelated Transplants
Impact of ATLG on OS in MTX- versus MMF-Based HSCT by Conditioning Intensity
3.4. Impact of ATLG on OS in MTX- versus MMF-Based HSCT by Recipient Age
3.5. ATLG-Associated OS Benefit Following MMF-Based HSCT Is Independent of Disease Risk
3.6. ATLG-Associated OS Benefit Following MMF-Based HSCT Has Emerged in the More Recent Transplant Era
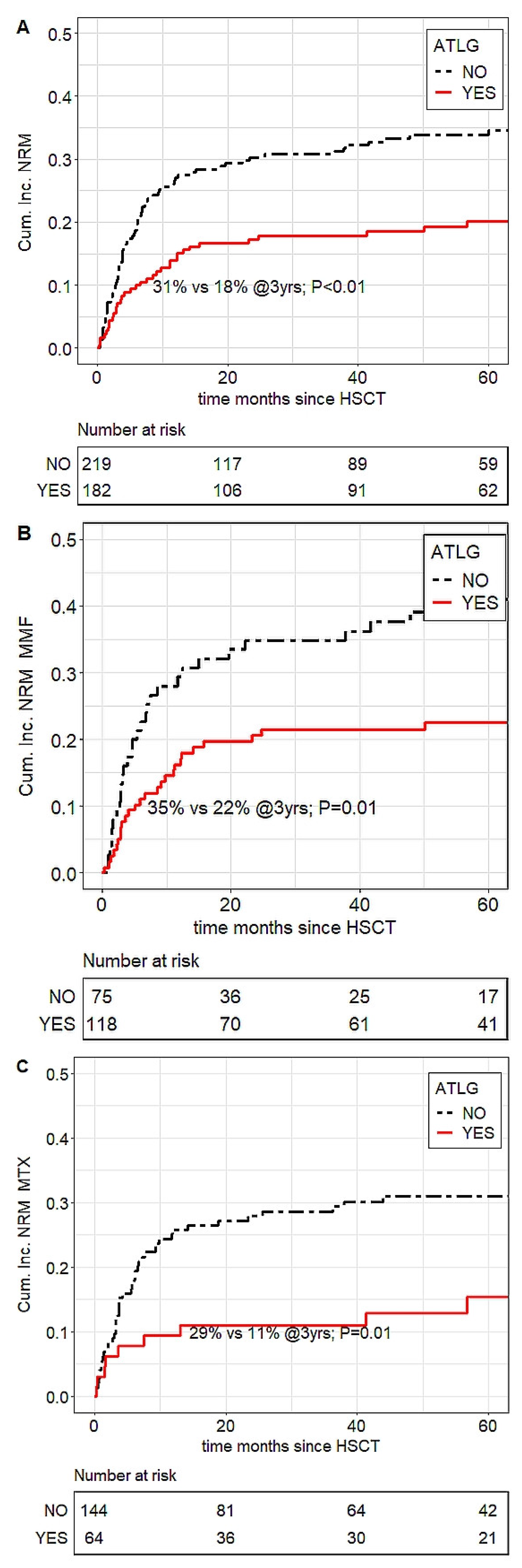
3.7. Non-Relapse Mortality (NRM) by ATLG in MMF- versus MTX-Based HSCT
3.8. Acute GVHD Grade III–IV by ATLG in MMF- versus MTX-Based HSCT
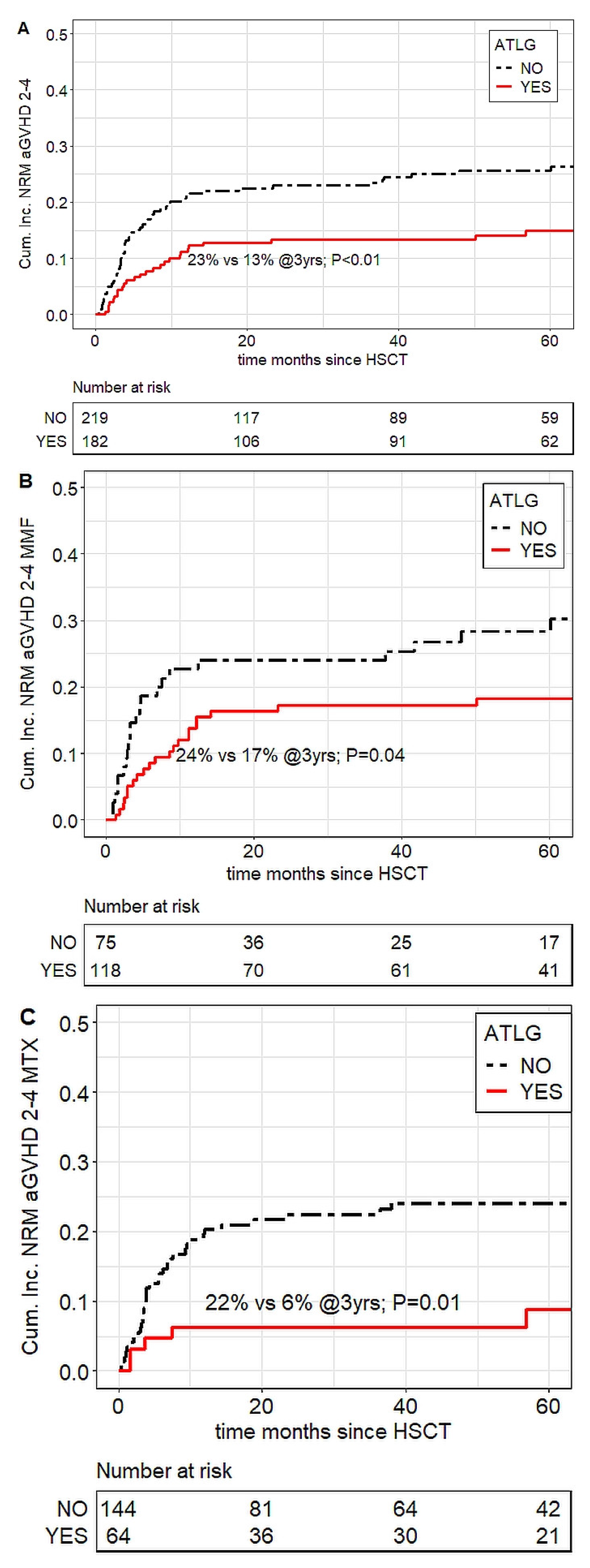
3.9. aGVHD-Associated Mortality
3.10. Chronic GVHD, Moderate/Severe
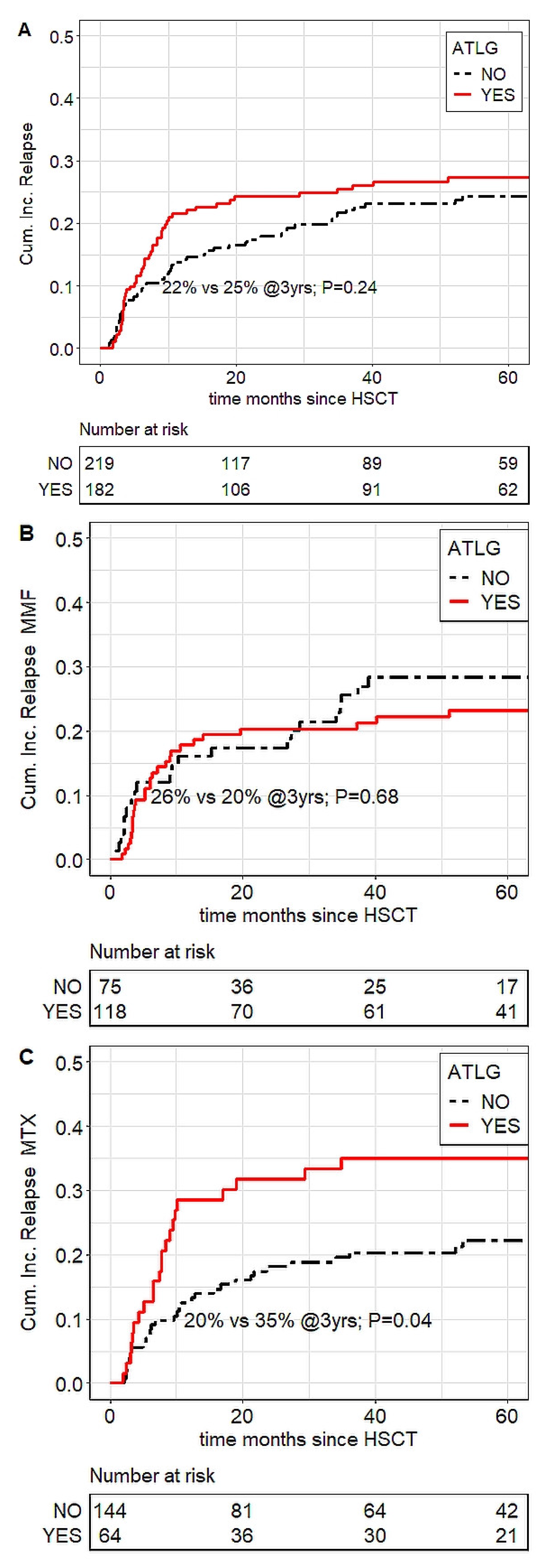
3.11. Relapse
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| aGVHD | acute GVHD |
| ALL | acute lymphocytic leukemia |
| AML | acute myeloid leukemia |
| ATG | Antithymocyte globulin |
| ATLG | anti-human T-lymphocyte globulin |
| BPDCN | blastic plasmacytoid dendritic cell neoplasm |
| cGVHD | chronic GVHD |
| CNI | calcineurin inhibitor |
| CsA | cyclosporin A |
| G-CSF | granulocyte-colony stimulating factor |
| GVHD | graft-versus-host disease |
| HR | hazard ratio |
| HSCT | allogeneic hematopoietic stem cell transplantation |
| MAC | myeloablative |
| MDS | myelodysplastic syndromes |
| MMF | mycophenolate mofetil |
| MPD | myeloproliferative disorder |
| MPN | myeloproliferative neoplasia |
| MPS | myeloproliferative syndromes |
| MTX | methotrexate |
| NMA | non-myeloablative |
| NRM | non-relapse mortality |
| OS | overall survival |
References
- Finke, J.; Bethge, W.A.; Schmoor, C.; Ottinger, H.D.; Stelljes, M.; Zander, A.R.; Volin, L.; Ruutu, T.; Heim, D.A.; Schwerdtfeger, R.; et al. Standard graft-versus-host disease prophylaxis with or without anti-T-cell globulin in haematopoietic cell transplantation from matched unrelated donors: A randomised, open-label, multicentre phase 3 trial. Lancet Oncol. 2009, 10, 855–864. [Google Scholar] [CrossRef] [PubMed]
- Soiffer, R.J.; Kim, H.T.; McGuirk, J.; Horwitz, M.E.; Johnston, L.; Patnaik, M.M.; Rybka, W.; Artz, A.; Porter, D.L.; Shea, T.C.; et al. Prospective, Randomized, Double-Blind, Phase III Clinical Trial of Anti–T-Lymphocyte Globulin to Assess Impact on Chronic Graft-Versus-Host Disease–Free Survival in Patients Undergoing HLA-Matched Unrelated Myeloablative Hematopoietic Cell Transplantation. J. Clin. Oncol. 2017, 35, 4003–4011. [Google Scholar] [CrossRef] [PubMed]
- Kröger, N.; Solano, C.; Wolschke, C.; Bandini, G.; Patriarca, F.; Pini, M.; Nagler, A.; Selleri, C.; Risitano, A.; Messina, G.; et al. Antilymphocyte Globulin for Prevention of Chronic Graft-versus-Host Disease. N. Engl. J. Med. 2016, 374, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Bacigalupo, A.; Lamparelli, T.; Bruzzi, P.; Guidi, S.; Alessandrino, P.E.; Di Bartolomeo, P.; Oneto, R.; Bruno, B.; Barbanti, M.; Sacchi, N.; et al. Antithymocyte globulin for graft-versus-host disease prophylaxis in transplants from unrelated donors: 2 randomized studies from Gruppo Italiano Trapianti Midollo Osseo (GITMO). Blood 2001, 98, 2942–2947. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-J.; Wu, D.-P.; Lai, Y.-R.; Liu, Q.-F.; Sun, Y.-Q.; Hu, J.; Hu, Y.; Zhou, J.-F.; Li, J.; Wang, S.-Q.; et al. Antithymocyte Globulin for Matched Sibling Donor Transplantation in Patients with Hematologic Malignancies: A Multicenter, Open-Label, Randomized Controlled Study. J. Clin. Oncol. 2020, 38, 3367–3376. [Google Scholar] [CrossRef]
- Walker, I.; Panzarella, T.; Couban, S.; Couture, F.; Devins, G.; Elemary, M.; Gallagher, G.; Kerr, H.; Kuruvilla, J.; Lee, S.J.; et al. Pretreatment with anti-thymocyte globulin versus no anti-thymocyte globulin in patients with haematological malignancies undergoing haemopoietic cell transplantation from unrelated donors: A randomised, controlled, open-label, phase 3, multicentre trial. Lancet Oncol. 2016, 17, 164–173. [Google Scholar] [CrossRef]
- Duléry, R.; Mohty, M.; Duhamel, A.; Robin, M.; Beguin, Y.; Michallet, M.; Vigouroux, S.; Lioure, B.; Garnier, A.; El Cheikh, J.; et al. Antithymocyte Globulin before Allogeneic Stem Cell Transplantation for Progressive Myelodysplastic Syndrome: A Study from the French Society of Bone Marrow Transplantation and Cellular Therapy. Biol. Blood Marrow Transplant. 2014, 20, 646–654. [Google Scholar] [CrossRef]
- Clausen, J.; Böhm, A.; Straßl, I.; Stiefel, O.; Buxhofer-Ausch, V.; Machherndl-Spandl, S.; König, J.; Schmidt, S.; Steitzer, H.; Danzer, M.; et al. HLA-C KIR-Ligands Determine the Impact of Anti-Thymocyte Globulin (ATG) on Graft versus Host and Graft versus Leukemia Effects Following Hematopoietic Stem Cell Transplantation. Biomedicines 2017, 5, 13. [Google Scholar] [CrossRef]
- Wolschke, C.; Zabelina, T.; Ayuk, F.; Alchalby, H.; Berger, J.; Klyuchnikov, E.E.; Pein, U.-M.; Schumacher, S.; Amtsfeld, G.; Adjallé, R.; et al. Effective prevention of GVHD using in vivo T-cell depletion with anti-lymphocyte globulin in HLA-identical or -mismatched sibling peripheral blood stem cell transplantation. Bone Marrow Transplant. 2014, 49, 126–130. [Google Scholar] [CrossRef]
- Baron, F.; Labopin, M.; Blaise, D.; Corral, L.L.; Vigouroux, S.; Craddock, C.; Attal, M.; Jindra, P.; Goker, H.; Socie, G.; et al. Impact of in vivo T-cell depletion on outcome of AML patients in first CR given peripheral blood stem cells and reduced-intensity conditioning allo-SCT from a HLA-identical sibling donor: A report from the Acute Leukemia Working Party of the European group for Blood and Marrow Transplantation. Bone Marrow Transplant. 2014, 49, 389–396. [Google Scholar] [CrossRef]
- Devillier, R.; Fürst, S.; El-Cheikh, J.; Castagna, L.; Harbi, S.; Granata, A.; Crocchiolo, R.; Oudin, C.; Mohty, B.; Bouabdallah, R.; et al. Antithymocyte Globulin in Reduced-Intensity Conditioning Regimen Allows a High Disease-Free Survival Exempt of Long-Term Chronic Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2014, 20, 370–374. [Google Scholar] [CrossRef]
- Crocchiolo, R.; Esterni, B.; Castagna, L.; Fürst, S.; El-Cheikh, J.; DeVillier, R.; Granata, A.; Oudin, C.; Calmels, B.; Chabannon, C.; et al. Two days of antithymocyte globulin are associated with a reduced incidence of acute and chronic graft-versus-host disease in reduced-intensity conditioning transplantation for hematologic diseases. Cancer 2013, 119, 986–992. [Google Scholar] [CrossRef]
- DeVillier, R.; Labopin, M.; Chevallier, P.; LeDoux, M.-P.; Socié, G.; Huynh, A.; Bourhis, J.-H.; Cahn, J.-Y.; Roth-Guepin, G.; Mufti, G.; et al. Impact of antithymocyte globulin doses in reduced intensity conditioning before allogeneic transplantation from matched sibling donor for patients with acute myeloid leukemia: A report from the acute leukemia working party of European group of Bone Marrow Transplantation. Bone Marrow Transplant. 2018, 53, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Ram, R.; Yeshurun, M.; Vidal, L.; Shpilberg, O.; Gafter-Gvili, A. Mycophenolate mofetil vs. methotrexate for the prevention of graft-versus-host-disease—Systematic review and meta-analysis. Leuk. Res. 2014, 38, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Perkins, J.; Field, T.; Kim, J.; Kharfan-Dabaja, M.A.; Fernandez, H.; Ayala, E.; Perez, L.; Xu, M.; Alsina, M.; Ochoa, L.; et al. A Randomized Phase II Trial Comparing Tacrolimus and Mycophenolate Mofetil to Tacrolimus and Methotrexate for Acute Graft-versus-Host Disease Prophylaxis. Biol. Blood Marrow Transplant. 2010, 16, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Eapen, M.; Logan, B.R.; Horowitz, M.M.; Zhong, X.; Perales, M.-A.; Lee, S.J.; Rocha, V.; Soiffer, R.J.; Champlin, R.E. Bone Marrow or Peripheral Blood for Reduced-Intensity Conditioning Unrelated Donor Transplantation. J. Clin. Oncol. 2015, 33, 364–369. [Google Scholar] [CrossRef]
- Al-Kadhimi, Z.; Gul, Z.; Chen, W.; Smith, D.; Abidi, M.; Deol, A.; Ayash, L.; Lum, L.; Waller, E.K.; Ratanatharathorn, V.; et al. High Incidence of Severe Acute Graft-Versus-Host Disease with Tacrolimus and Mycophenolate Mofetil in a Large Cohort of Related and Unrelated Allogeneic Transplantation Patients. Biol. Blood Marrow Transplant. 2014, 20, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar] [PubMed]
- Filipovich, A.H.; Weisdorf, D.; Pavletic, S.; Socie, G.; Wingard, J.R.; Lee, S.J.; Martin, P.; Chien, J.; Przepiorka, D.; Couriel, D.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. Diagnosis and Staging Working Group Report. Biol. Blood Marrow Transplant. 2005, 11, 945–956. [Google Scholar] [CrossRef]
- Giralt, S.; Ballen, K.; Rizzo, D.; Bacigalupo, A.; Horowitz, M.; Pasquini, M.; Sandmaier, B. Reduced-Intensity Conditioning Regimen Workshop: Defining the Dose Spectrum. Report of a Workshop Convened by the Center for International Blood and Marrow Transplant Research. Biol. Blood Marrow Transplant. 2009, 15, 367–369. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000; ISBN 0-387-98784-3. [Google Scholar]
- Gerds, T.A.; Kattan, M.W. Medical Risk Prediction Models: With Ties to Machine Learning, 1st ed.; Chapman and Hall/CRC: Abingdon, UK, 2021. [Google Scholar] [CrossRef]
- Gray, B. _cmprsk: Subdistribution Analysis of Competing Risks_. R package version 2.2-11. 2022. Available online: https://CRAN.R-project.org/package=cmprsk (accessed on 23 January 2023).
- Wilke, C. _cowplot: Streamlined Plot Theme and Plot Annotations for 'ggplot2'_. R package version 1.1.1. 2020. Available online: https://CRAN.R-project.org/package=cowplot (accessed on 23 January 2023).
- Kassambara, A.; Kosinski, M.; Biecek, P. _survminer: Drawing Survival Curves using 'ggplot2'_. R package version 0.4.9. 2021. Available online: https://CRAN.R-project.org/package=survminer (accessed on 23 January 2023).
- Harrison, E.; Drake, T.; Ots, R. _finalfit: Quickly Create Elegant Regression Results Tables and Plots when Modelling_. R package version 1.0.5. 2022. Available online: https://CRAN.R-project.org/package=finalfit (accessed on 23 January 2023).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis (Use R!), 2nd ed.; Springer: Cham, Switzerland, 2016; p. 276. ISBN 978-3-319-24277-4. [Google Scholar]
- Chhabra, S.; Liu, Y.; Hemmer, M.T.; Costa, L.; Pidala, J.A.; Couriel, D.R.; Alousi, A.M.; Majhail, N.S.; Stuart, R.K.; Kim, D.; et al. Comparative Analysis of Calcineurin Inhibitor–Based Methotrexate and Mycophenolate Mofetil–Containing Regimens for Prevention of Graft-versus-Host Disease after Reduced-Intensity Conditioning Allogeneic Transplantation. Biol. Blood Marrow Transplant. 2019, 25, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Sandmaier, B.M.; Kornblit, B.; Storer, B.E.; Olesen, G.; Maris, M.B.; Langston, A.A.; Gutman, J.A.; Petersen, S.L.; Chauncey, T.R.; Bethge, W.A.; et al. Addition of sirolimus to standard cyclosporine plus mycophenolate mofetil-based graft-versus-host disease prophylaxis for patients after unrelated non-myeloablative haemopoietic stem cell transplantation: A multicentre, randomised, phase 3 trial. Lancet Haematol. 2019, 6, e409–e418. [Google Scholar] [CrossRef] [PubMed]
- Paviglianiti, A.; Labopin, M.; Blaise, D.; Socié, G.; Bulabois, C.E.; Lioure, B.; Ceballos, P.; Blau, I.W.; Guillerm, G.; Maertens, J.; et al. Comparison of mycophenolate mofetil and calcineurin inhibitor versus calcineurin inhibitor-based graft-versus-host-disease prophylaxis for matched unrelated donor transplant in acute myeloid leukemia. A study from the ALWP of the EBMT. Bone Marrow Transplant. 2021, 56, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Soiffer, R.J.; LeRademacher, J.; Ho, V.; Kan, F.; Artz, A.; Champlin, R.E.; Devine, S.; Isola, L.; Lazarus, H.M.; Marks, D.I.; et al. Impact of immune modulation with anti–T-cell antibodies on the outcome of reduced-intensity allogeneic hematopoietic stem cell transplantation for hematologic malignancies. Blood 2011, 117, 6963–6970. [Google Scholar] [CrossRef]
- Admiraal, R.; Nierkens, S.; de Witte, M.A.; Petersen, E.J.; Fleurke, G.-J.; Verrest, L.; Belitser, S.V.; Bredius, R.G.M.; Raymakers, R.A.P.; Knibbe, C.A.J.; et al. Association between anti-thymocyte globulin exposure and survival outcomes in adult unrelated haemopoietic cell transplantation: A retrospective, pharmacodynamic cohort analysis. Lancet Haematol. 2017, 4, e183–e191. [Google Scholar] [CrossRef]
- Kennedy, V.E.; Chen, H.; Savani, B.N.; Greer, J.; Kassim, A.A.; Engelhardt, B.G.; Goodman, S.; Sengsayadeth, S.; Chinratanalab, W.; Jagasia, M. Optimizing Antithymocyte Globulin Dosing for Unrelated Donor Allogeneic Hematopoietic Cell Transplantation Based on Recipient Absolute Lymphocyte Count. Biol. Blood Marrow Transplant. 2018, 24, 150–155. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients and Transplant Details | All | CNI/MMF | CNI/MTX | p-Value |
|---|---|---|---|---|
| Total number of transplants (n) | 401 | 193 | 208 | |
| Recipient age at Tx years (median/range) | 48.6 (17.0–73.0) | 53.25 (18.0–73.0) | 42.75 (17.0–69.0) | <0.001 |
| Diagnosis (%) | ||||
| AML | 192 (47.9%) | 86 (44.6%) | 106 (51.0%) | |
| MDS, MPN, and MDS-MPN overlap syndromes | 82 (20.4%) | 41 (21.2%) | 41 (19.7%) | |
| ALL | 72 (18.0%) | 35 (18.1%) | 37 (17.8%) | |
| Lymphoma, Myeloma, BPDCN | 45 (11.2%) | 25 (13.0%) | 20 (9.6%) | |
| Non-malignant | 10 (2.4%) | 6 (3.1%) | 4 (1.9%) | 0.69 |
| Disease stage (%) | ||||
| Early | 211 (52.6%) | 86 (44.6%) | 125 (60.1%) | |
| Intermediate | 190 (47.4%) | 107 (55.4%) | 83 (39.9%) | 0.002 |
| Median year of HSCT (median/range) | 2010 (1996–2018) | 2011 (1999–2018) | 2007 (1996–2018) | |
| Median follow-up of survivors years (median/range) | 5.4 (0.4–20.7) | 65.3 (4.5–189.0) | 64.2 (4.4–248.5) | 0.72 |
| Conditioning (%) | ||||
| myeloablative (full intensity MAC or RTC) | 248 (61.8%) | 70 (36.3%) | 178 (85.6%) | |
| reduced intensity (RIC or NMA) | 153 (38.2%) | 123 (63.7%) | 30 (14.4%) | <0.001 |
| Donor (%) | ||||
| matched sibling | 228 (56.9%) | 89 (46.1%) | 139 (66.8%) | |
| unrelated (9/10 or 10/10 matched) | 173 (43.1%) | 104 (53.9%) | 69 (33.2%) | <0.001 |
| Graft source (%) | ||||
| G-CSF mobilized peripheral blood | 401 (100%) | 193 (100.0%) | 208 (100.0%) | |
| Anti-T cell Serotherapy (%) | ||||
| Yes (ATLG) | 182 (45.4%) | 118 (61.1%) | 64 (30.8%) | |
| No | 219 (54.6%) | 75 (38.9%) | 144 (69.2%) | <0.001 |
| ATLG dose in mg/kg (median/range) | 35 (15–60) | 30 (15–60) | 35 (15–60) | 0.08 |
| Donor/Recipient sex matching (%) | ||||
| female donor to male recipient | 94 (23.4%) | 43 (22.3%) | 51 (24.5%) | |
| Other | 307 (76.6%) | 150 (77.7%) | 157 (75.5%) | 0.64 |
| Endpoint/Cohort | Hazard Ratio */ Sub-Hazard Ratio | p Value |
|---|---|---|
| Overall Mortality * | ||
| Overall | 0.53 | 0.002 |
| MMF | 0.49 | 0.001 |
| MTX | 0.87 | 0.56 |
| Non-Relapse Mortality | ||
| Overall | 0.29 | <0.001 |
| MMF | 0.23 | <0.001 |
| MTX | 0.29 | <0.001 |
| aGVHD 3–4 | ||
| Overall | 0.51 | 0.004 |
| MMF | 0.38 | 0.006 |
| MTX | 0.58 | 0.11 |
| aGVHD-associated mortality | ||
| Overall | 0.29 | <0.001 |
| MMF | 0.22 | <0.001 |
| MTX | 0.3 | 0.01 |
| cGVHD moderate/severe | ||
| Overall | 0.38 | <0.001 |
| MMF | 0.46 | 0.02 |
| MTX | 0.29 | <0.001 |
| Relapse | ||
| Overall | 1.87 | 0.01 |
| MMF | 1.78 | 0.1 |
| MTX | 2.4 | 0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikoloudis, A.; Strassl, I.; Binder, M.; Stiefel, O.; Wipplinger, D.; Milanov, R.; Aichinger, C.; Kaynak, E.; Machherndl-Spandl, S.; Buxhofer-Ausch, V.; et al. Comparison of Benefits and Risks Associated with Anti-T-Lymphocyte Globulin (ATLG) Serotherapy in Methotrexate (MTX)- versus Mycophenolate Mofetil (MMF)-Based Hematopoietic Stem Cell Transplantation. Transplantology 2023, 4, 22-37. https://doi.org/10.3390/transplantology4010005
Nikoloudis A, Strassl I, Binder M, Stiefel O, Wipplinger D, Milanov R, Aichinger C, Kaynak E, Machherndl-Spandl S, Buxhofer-Ausch V, et al. Comparison of Benefits and Risks Associated with Anti-T-Lymphocyte Globulin (ATLG) Serotherapy in Methotrexate (MTX)- versus Mycophenolate Mofetil (MMF)-Based Hematopoietic Stem Cell Transplantation. Transplantology. 2023; 4(1):22-37. https://doi.org/10.3390/transplantology4010005
Chicago/Turabian StyleNikoloudis, Alexander, Irene Strassl, Michaela Binder, Olga Stiefel, Dagmar Wipplinger, Robert Milanov, Christoph Aichinger, Emine Kaynak, Sigrid Machherndl-Spandl, Veronika Buxhofer-Ausch, and et al. 2023. "Comparison of Benefits and Risks Associated with Anti-T-Lymphocyte Globulin (ATLG) Serotherapy in Methotrexate (MTX)- versus Mycophenolate Mofetil (MMF)-Based Hematopoietic Stem Cell Transplantation" Transplantology 4, no. 1: 22-37. https://doi.org/10.3390/transplantology4010005
APA StyleNikoloudis, A., Strassl, I., Binder, M., Stiefel, O., Wipplinger, D., Milanov, R., Aichinger, C., Kaynak, E., Machherndl-Spandl, S., Buxhofer-Ausch, V., Böhm, A., Petzer, A., Weltermann, A., Wolf, D., Nachbaur, D., & Clausen, J. (2023). Comparison of Benefits and Risks Associated with Anti-T-Lymphocyte Globulin (ATLG) Serotherapy in Methotrexate (MTX)- versus Mycophenolate Mofetil (MMF)-Based Hematopoietic Stem Cell Transplantation. Transplantology, 4(1), 22-37. https://doi.org/10.3390/transplantology4010005