
Outcomes of Neonates Exposed to Buprenorphine versus Methadone in Utero: A Systematic Review and Meta-Analysis of Safety in the Fetus and Neonate


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
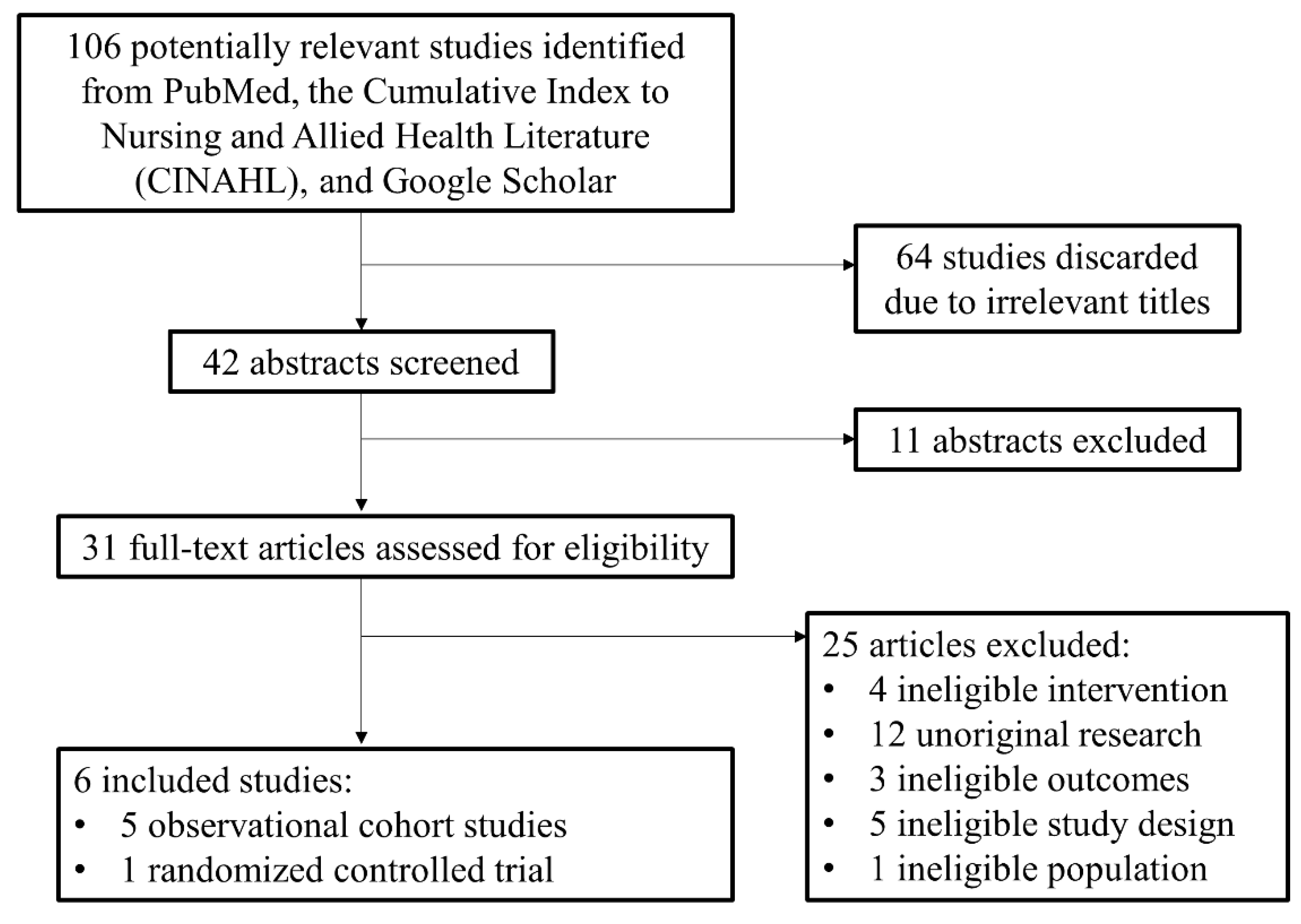
2.2. Study Selection
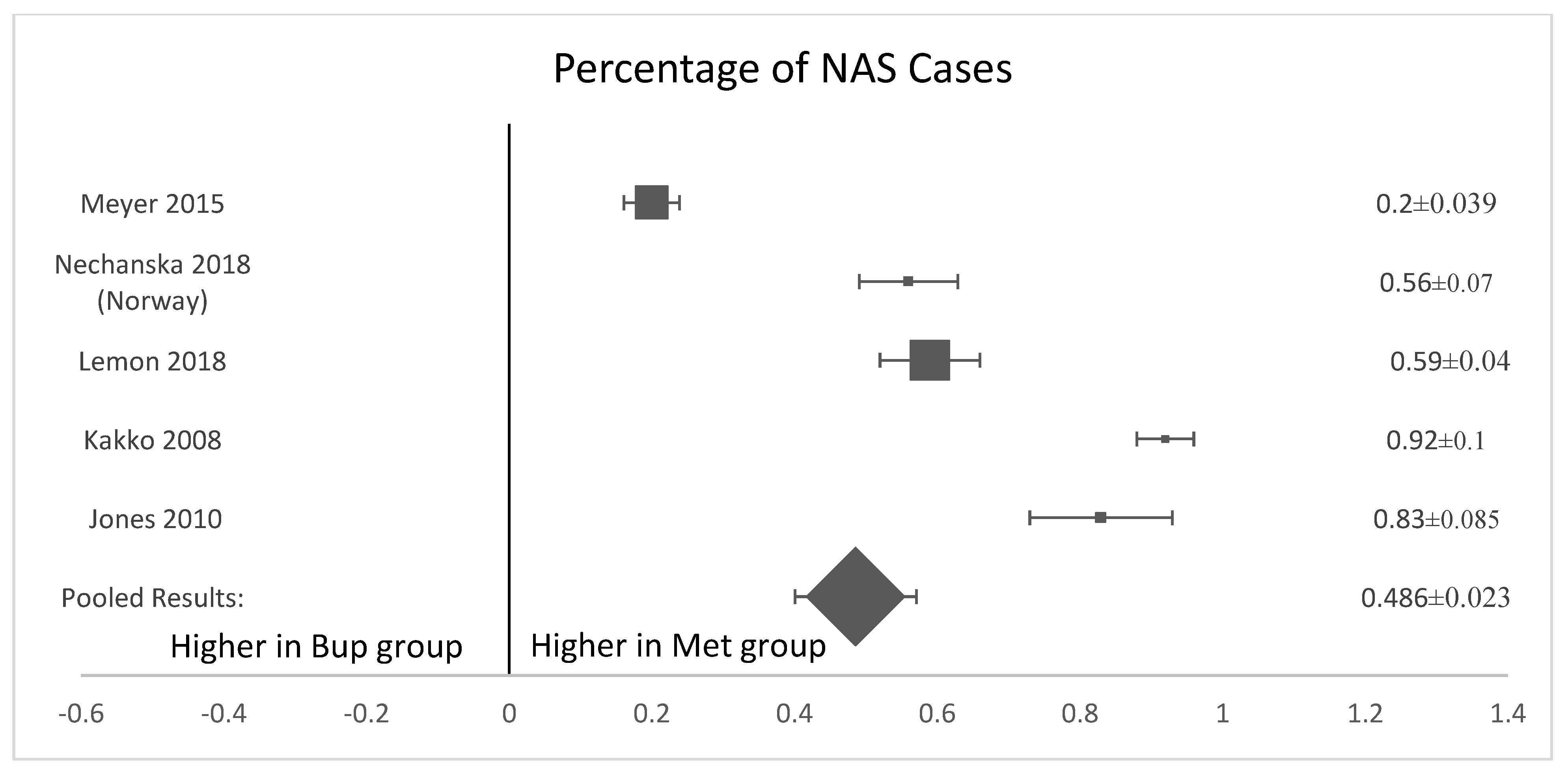
2.3. Statistical Analysis
3. Results
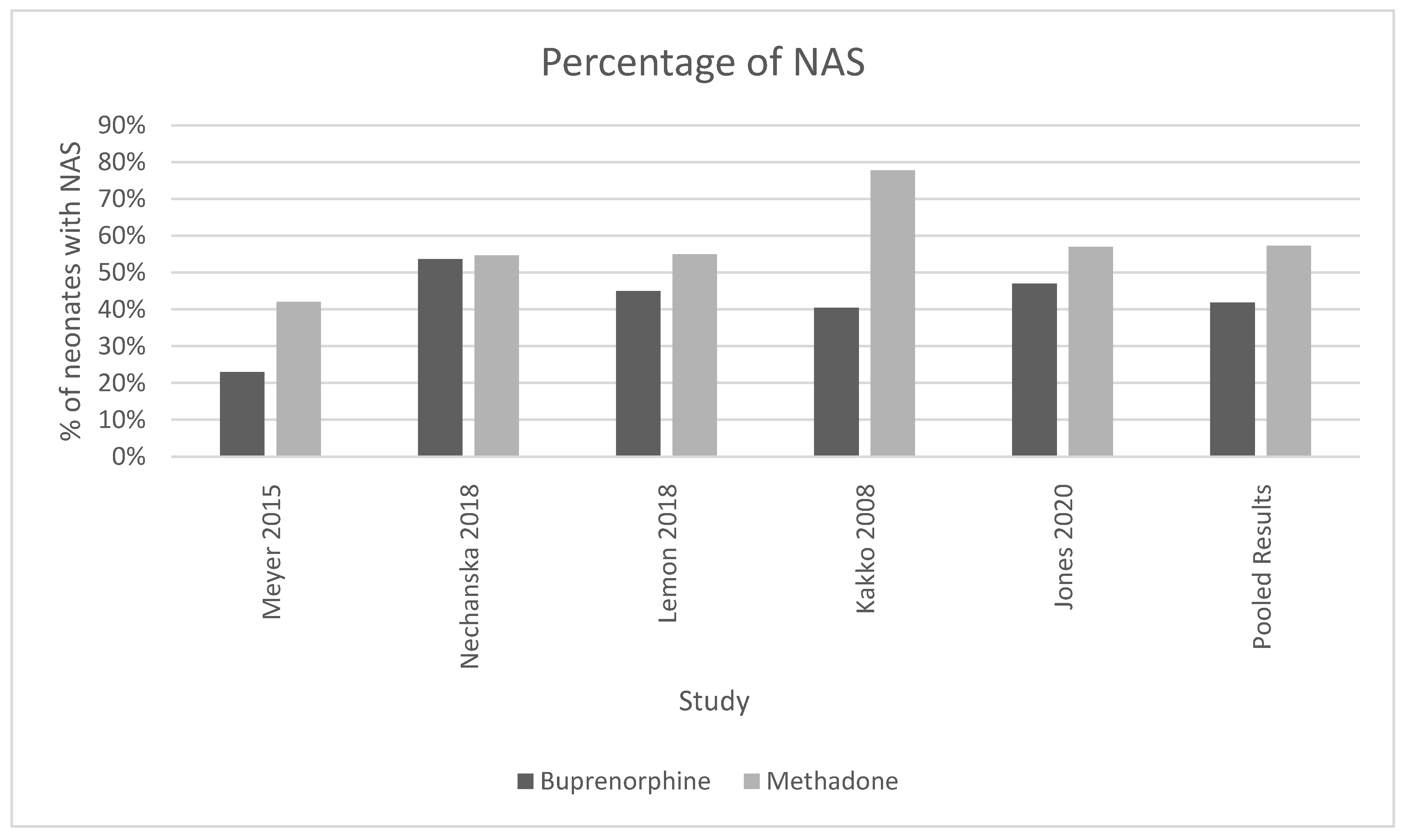
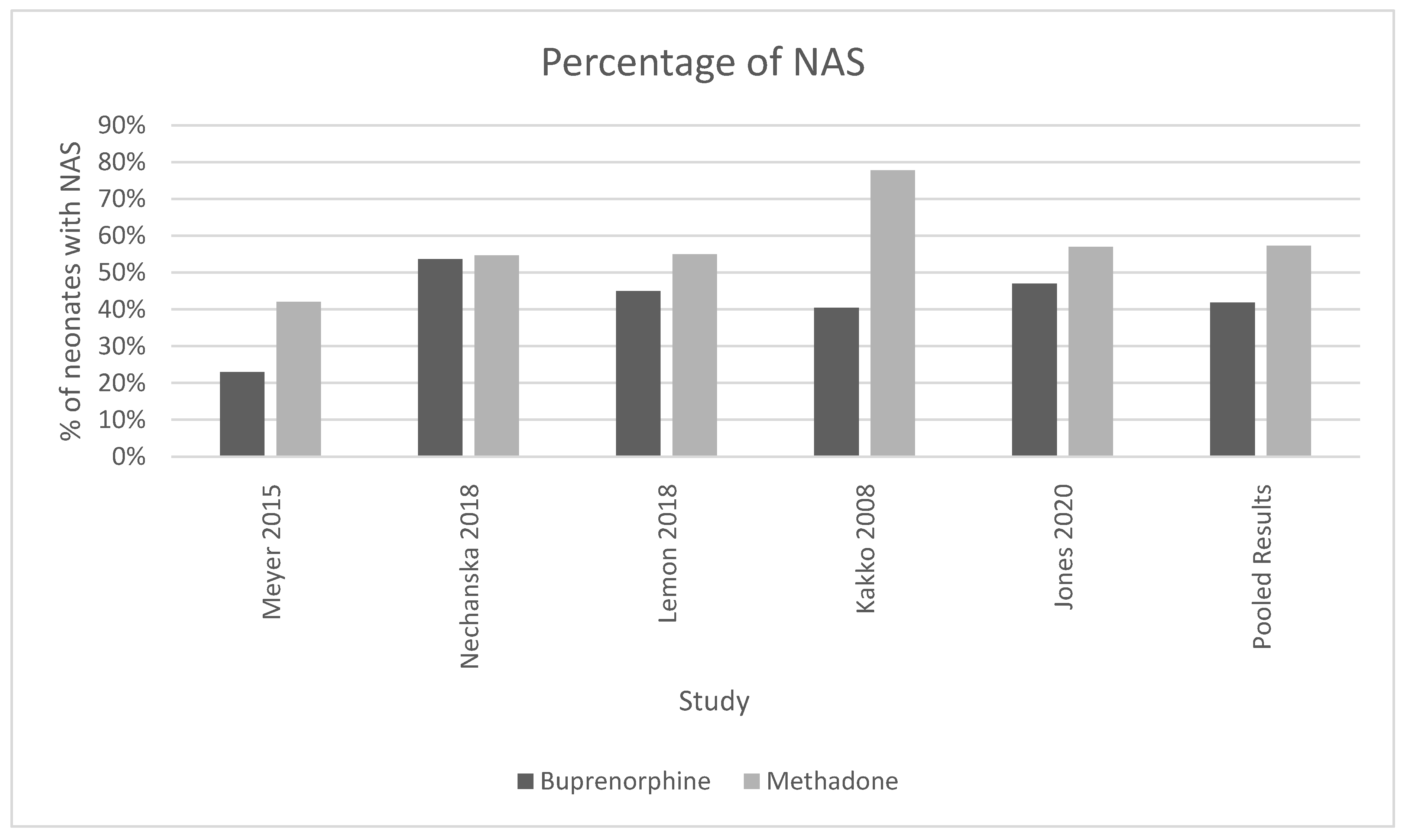
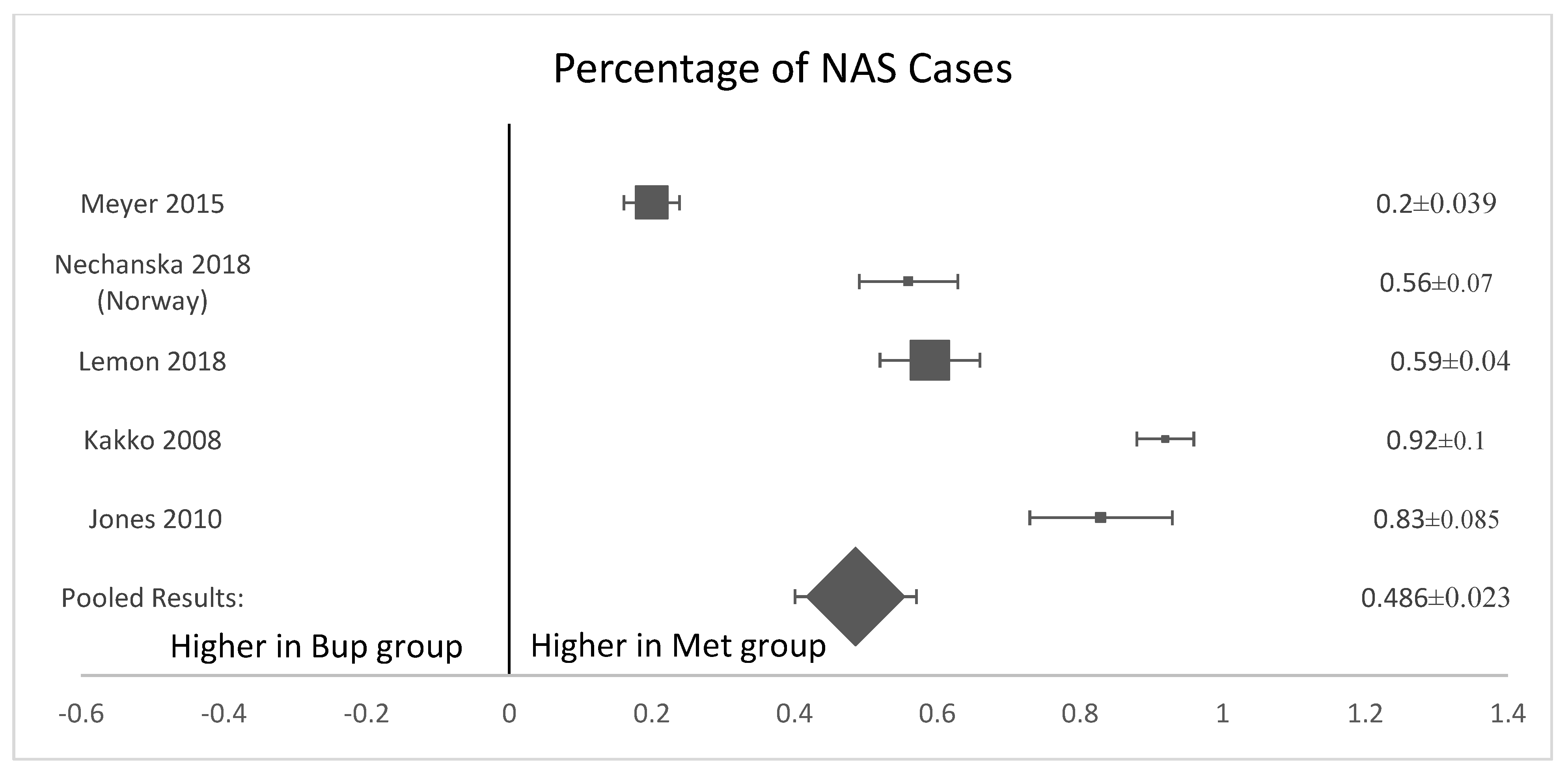
3.1. Presence of Neonatal Abstinence Syndrome
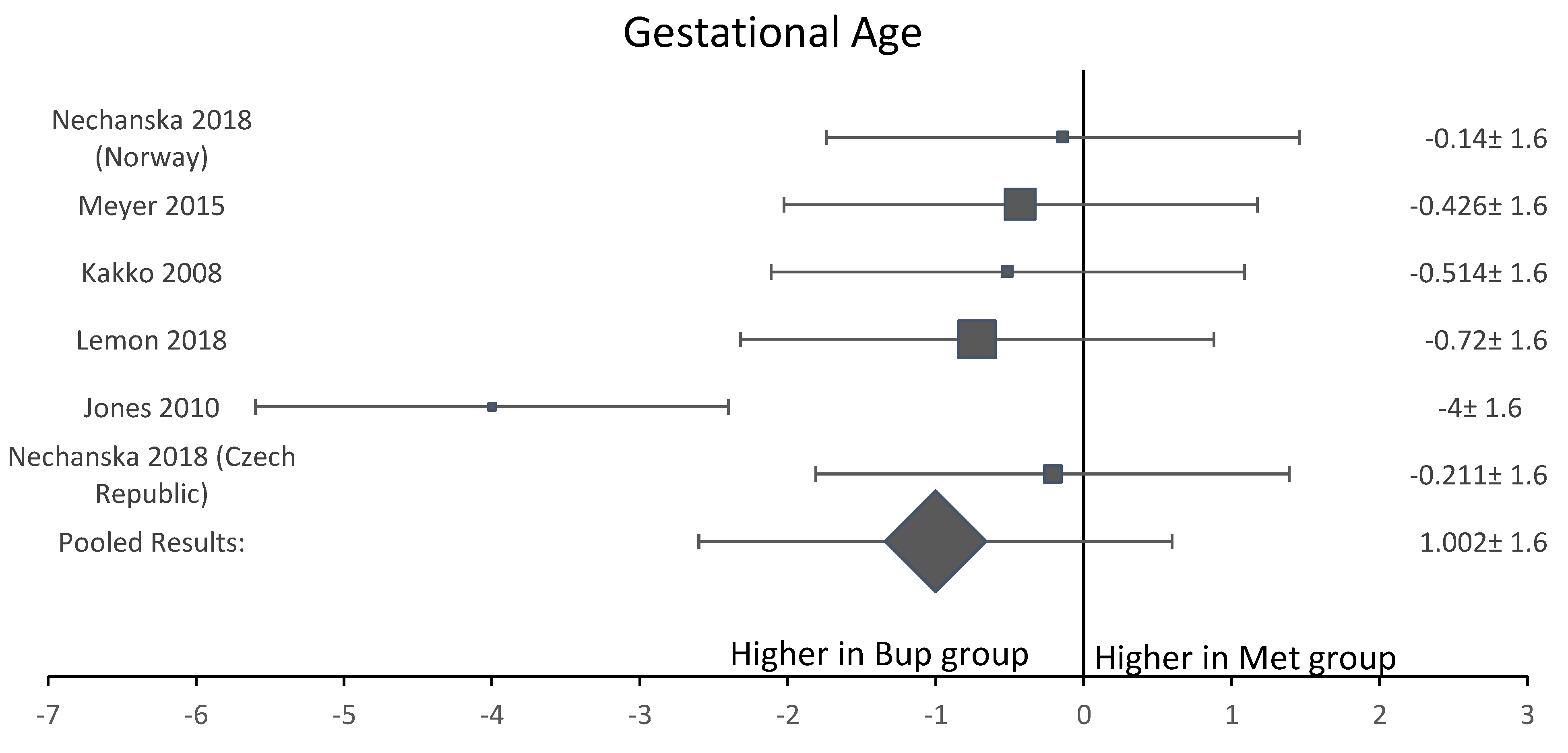
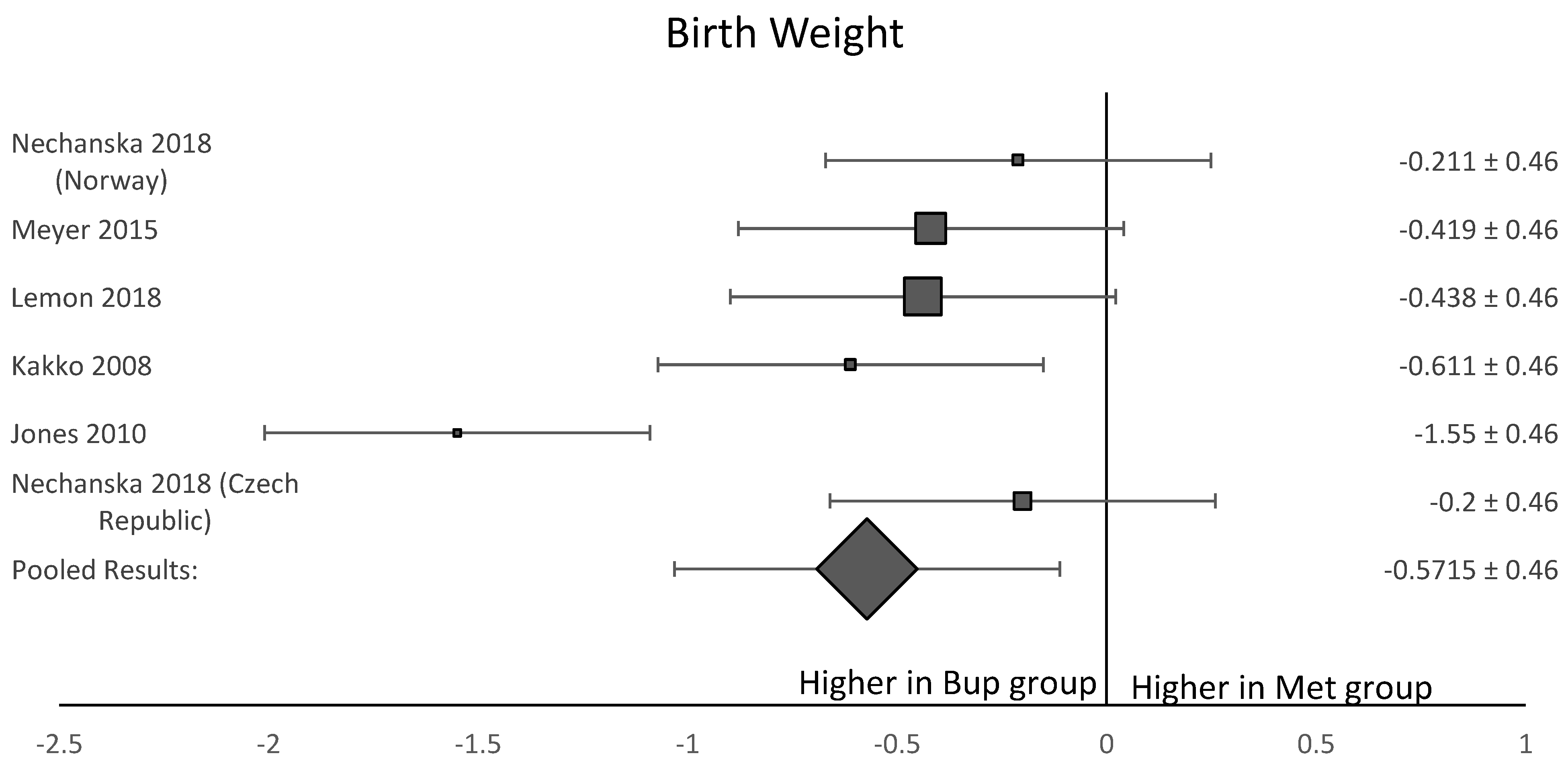
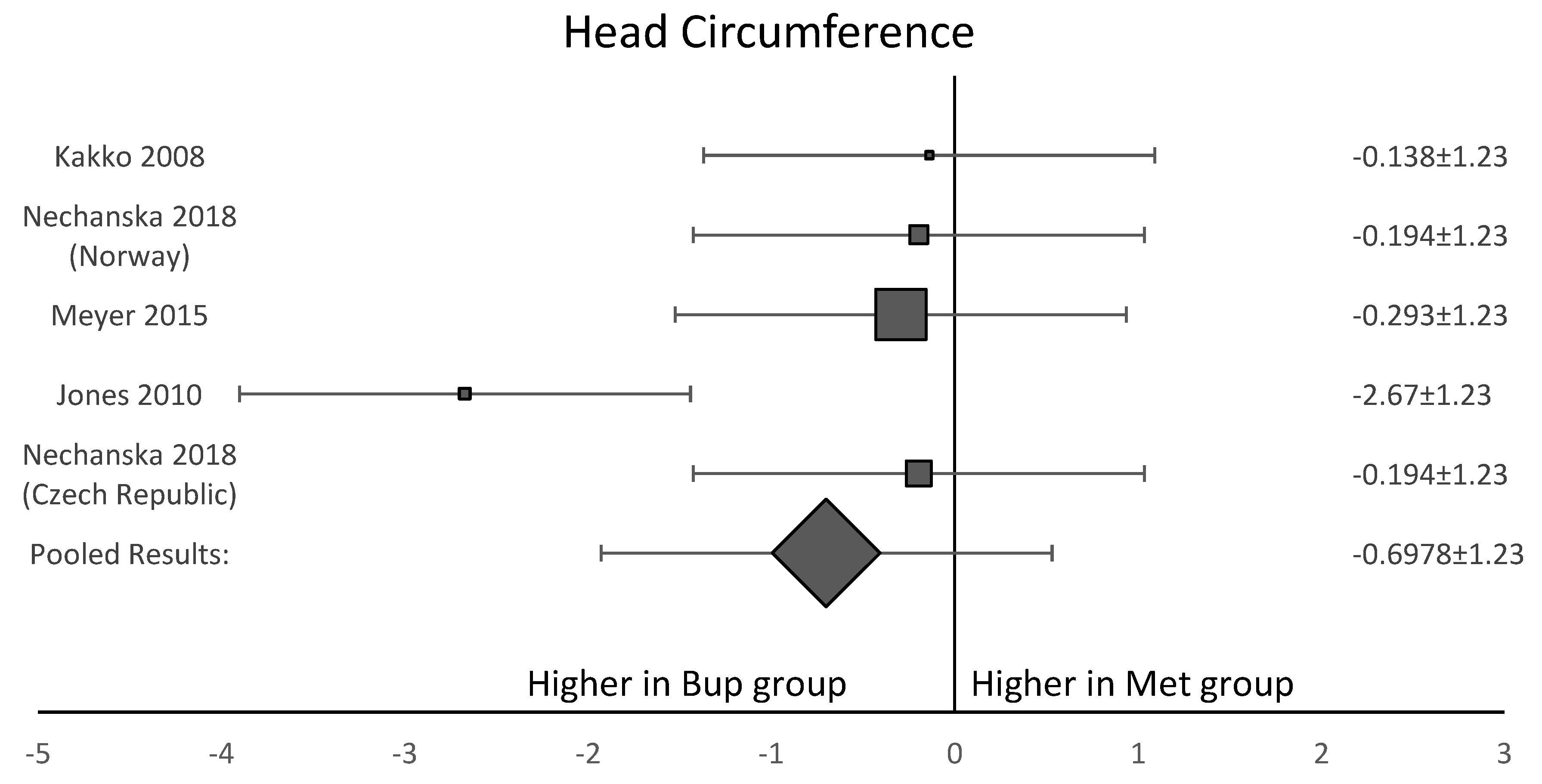
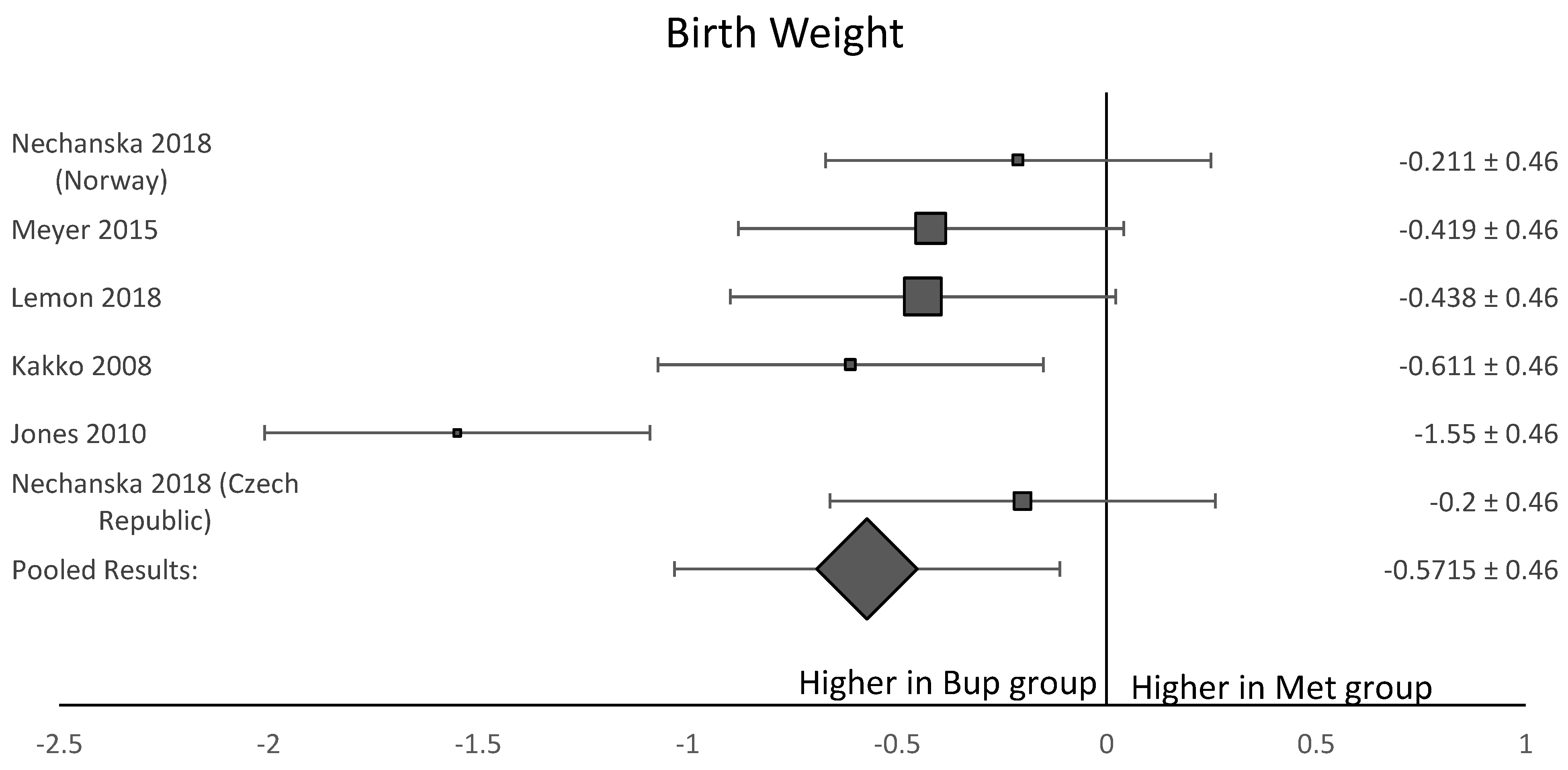
3.2. Birth and Growth Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mullins, N.; Galvin, S.; Ramage, M.; Gannon, M.; Lorenz, K.; Sager, B.; Coulson, C.C. Buprenorphine and Naloxone Versus Buprenorphine for Opioid Use Disorder in Pregnancy: A Cohort Study. J. Addict. Med. 2019, 14, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Clinical Guidance for Treating Pregnant and Parenting Women with Opioid Use Disorder and Their Infants ii Clinical Guidance for Treating Pregnant and Parenting Women with Opioid Use Disorder and Their Infants. Available online: http://store.samhsa.gov (accessed on 28 February 2020).
- Patrick, S.W.; Schumacher, R.E.; Benneyworth, B.D.; Krans, E.E.; McAllister, J.M.; Davis, M.M. Neonatal Abstinence Syndrome and Associated Health Care Expenditures. JAMA 2012, 307, 1934–1940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ACOG. Opioid Use and Opioid Use Disorder in Pregnancy. Available online: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2017/08/opioid-use-and-opioid-use-disorder-in-pregnancy (accessed on 19 July 2021).
- Laslo, J.; Brunner, J.-M.; Burns, D.; Butler, E.; Cunningham, A.; Killpack, R.; Pyeritz, C.; Rinard, K.; Childers, J.; Horzempa, J. An overview of available drugs for management of opioid abuse during pregnancy. Matern. Health Neonatol. Perinatol. 2017, 3, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institutes of Health. How Do Medications toTreat Opioid Use Disorder Work?|National Institute on Drug Abuse (NIDA). National Institute on Drug Abuse Research Reports. Available online: https://www.drugabuse.gov/publications/research-reports/medications-to-treat-opioid-addiction/how-do-medications-to-treat-opioid-addiction-work (accessed on 28 February 2020).
- Wilder, C.M.; Winhusen, T. Pharmacological Management of Opioid Use Disorder in Pregnant Women. CNS Drugs 2015, 29, 625–636. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.E.; Kaltenbach, K.; Heil, S.H.; Stine, S.M.; Coyle, M.G.; Arria, A.M.; O’Grady, K.E.; Selby, P.; Martin, P.R.; Fischer, G. Neonatal Abstinence Syndrome After Methadone or Buprenorphine Exposure. N. Engl. J. Med. 2010, 363, 2320–2331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PRISMA: Transparent Reporting of Systematic Reviews and Meta-Analyses. 2021. Available online: http://www.prisma-statement.org/ (accessed on 31 January 2020).
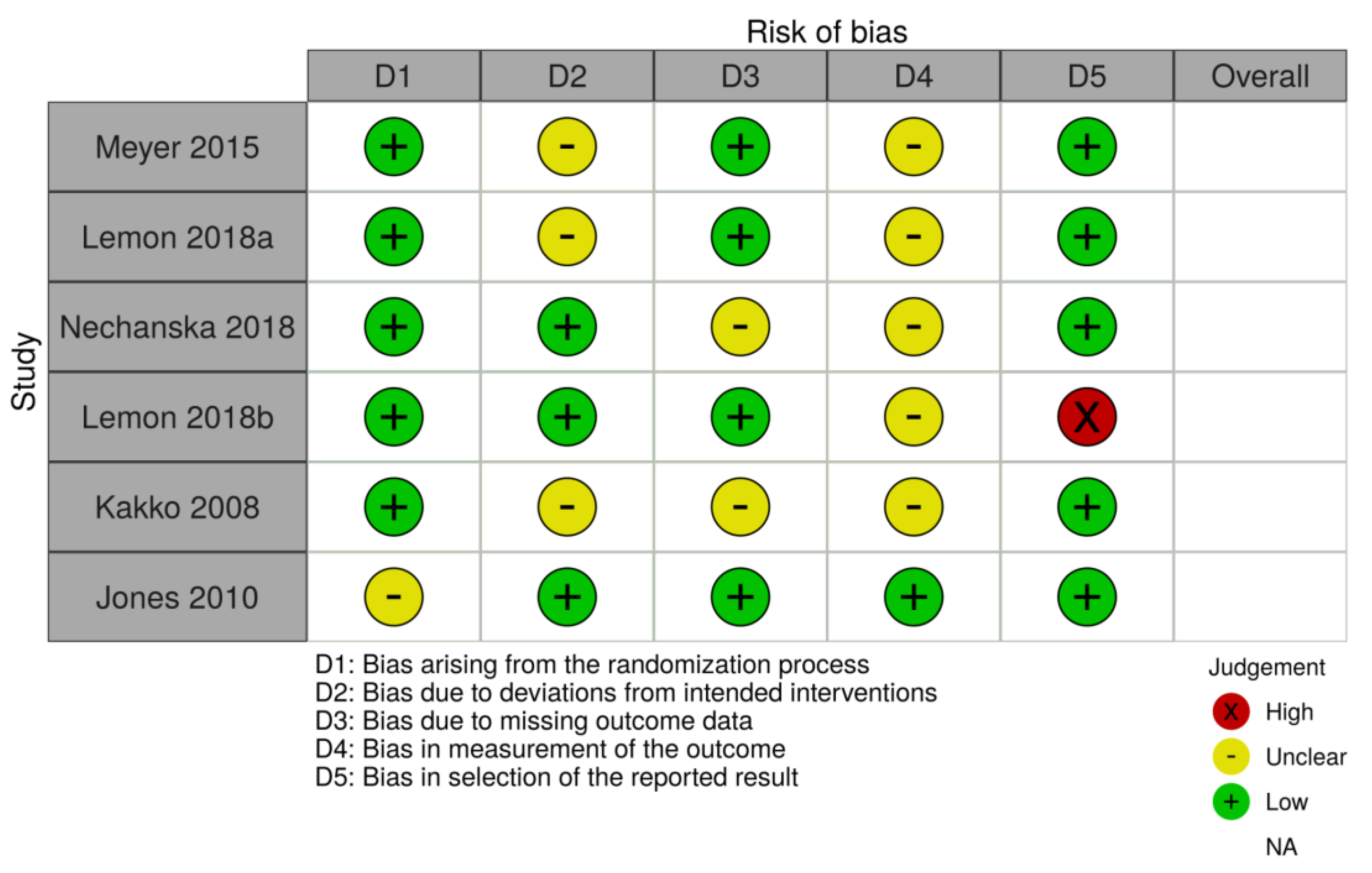
- Sterne, J.A.C.; Savović, J.; Page, M.; Elbers, R.G.; Blencowe, N.; Boutron, I.; Cates, C.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakko, J.; Heilig, M.; Sarman, I. Buprenorphine and methadone treatment of opiate dependence during pregnancy: Comparison of fetal growth and neonatal outcomes in two consecutive case series. Drug Alcohol Depend. 2008, 96, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Meyer, M.C.; Johnston, A.M.; Crocker, A.M.; Heil, S.H. Methadone and Buprenorphine for Opioid Dependence during Pregnancy. J. Addict. Med. 2015, 9, 81–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemon, L.S.; Caritis, S.N.; Venkataramanan, R.; Platt, R.W.; Bodnar, L.M. Methadone Versus Buprenorphine for Opioid Use Dependence and Risk of Neonatal Abstinence Syndrome. Epidemiology 2018, 29, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Lemon, L.S.; Naimi, A.; Caritis, S.N.; Platt, R.W.; Venkataramanan, R.; Bodnar, L.M. The Role of Preterm Birth in the Association between Opioid Maintenance Therapy and Neonatal Abstinence Syndrome. Paediatr. Périnat. Epidemiol. 2018, 32, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Nechanská, B.; Mravcik, V.; Skurtveit, S.; Lund, I.O.; Gabrhelik, R.; Engeland, A.; Handal, M. Neonatal outcomes after fetal exposure to methadone and buprenorphine: National registry studies from the Czech Republic and Norway. Addiction 2018, 113, 1286–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, T.H.; Griffin, B.L.; Stone, R.H.; Vest, K.M.; Todd, T.J. Methadone, Buprenorphine, and Naltrexone for the Treatment of Opioid Use Disorder in Pregnant Women. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 824–839. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Groups | Methods | Gestational Age OAT Initiated (Weeks) | EGA at Delivery (Mean, Weeks) | Outcome |
|---|---|---|---|---|---|
| Kakko et al. 2008 [11] | Methadone (n = 36), buprenorphine (n = 47) | OCS | N/A | Methadone: 38.6 ± 1.5 Buprenorphine: 39.5 ± 2.0 |
|
| Jones et al. 2010 [8] | Methadone (n = 73), buprenorphine (n = 58) | RCT | Methadone: 18.7 ± 0.8 Buprenorphine: 18.7 ± 0.7 | Methadone: 37.9 ± 0.3 Buprenorphine: 39.1 ± 0.3 |
|
| Meyer et al. 2015 [12] | Methadone (n = 248), buprenorphine (n = 361) | OCS | Methadone: 18.9 ± 19.1 Buprenorphine: 15.9 ± 8.1 | Methadone: 38.2 ± 2.5 Buprenorphine: 39.2 ± 2.2 |
|
| Lemon et al. 2018a [13] | Methadone (n = 407), buprenorphine (n = 309) | OCS | N/A | Methadone: 37.4 ± 2.9 Buprenorphine: 38.5 ± 2.5 |
|
| Lemon et al. 2018b [14] | Methadone (n = 407), buprenorphine (n = 309) | OCS | N/A | N/A |
|
| Nechanská et al. 2018 [15] | Cohort 1: Methadone (n=152), buprenorphine (n=152) Cohort 2: Methadone (n = 99), buprenorphine (n = 97) | OCS | N/A | Cohort 1: Methadone 38.3 ± 2.6 Buprenorphine 38.5 ± 2.7 Cohort 2: Methadone: 38.9 ± 1.9 Buprenorphine: 39.2 ± 2.4 |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christianson, H.L.; Sabry, A.A.; Sous, J.E.G.; Adams, J.H.; Hoppe, K.K.; Antony, K.M. Outcomes of Neonates Exposed to Buprenorphine versus Methadone in Utero: A Systematic Review and Meta-Analysis of Safety in the Fetus and Neonate. Reprod. Med. 2021, 2, 185-194. https://doi.org/10.3390/reprodmed2040019
Christianson HL, Sabry AA, Sous JEG, Adams JH, Hoppe KK, Antony KM. Outcomes of Neonates Exposed to Buprenorphine versus Methadone in Utero: A Systematic Review and Meta-Analysis of Safety in the Fetus and Neonate. Reproductive Medicine. 2021; 2(4):185-194. https://doi.org/10.3390/reprodmed2040019
Chicago/Turabian StyleChristianson, Hannah L., Alea A. Sabry, Jinan E. G. Sous, Jacquelyn H. Adams, Kara K. Hoppe, and Kathleen M. Antony. 2021. "Outcomes of Neonates Exposed to Buprenorphine versus Methadone in Utero: A Systematic Review and Meta-Analysis of Safety in the Fetus and Neonate" Reproductive Medicine 2, no. 4: 185-194. https://doi.org/10.3390/reprodmed2040019
APA StyleChristianson, H. L., Sabry, A. A., Sous, J. E. G., Adams, J. H., Hoppe, K. K., & Antony, K. M. (2021). Outcomes of Neonates Exposed to Buprenorphine versus Methadone in Utero: A Systematic Review and Meta-Analysis of Safety in the Fetus and Neonate. Reproductive Medicine, 2(4), 185-194. https://doi.org/10.3390/reprodmed2040019