
Occupational Physical Activity and Fitness in Predicting Cardiovascular Mortality among European Cohorts of Middle-Aged Men: A 60-Year Follow-Up in the Seven Countries Study

 ,
,  , and
, and
Abstract
1. Introduction
2. Material and Methods
2.1. Population and Measurements
2.2. Statistical Analysis
3. Results
3.1. Baseline Variables and Death Rates
3.2. OPA and Fitscore versus Indicators of Fitness
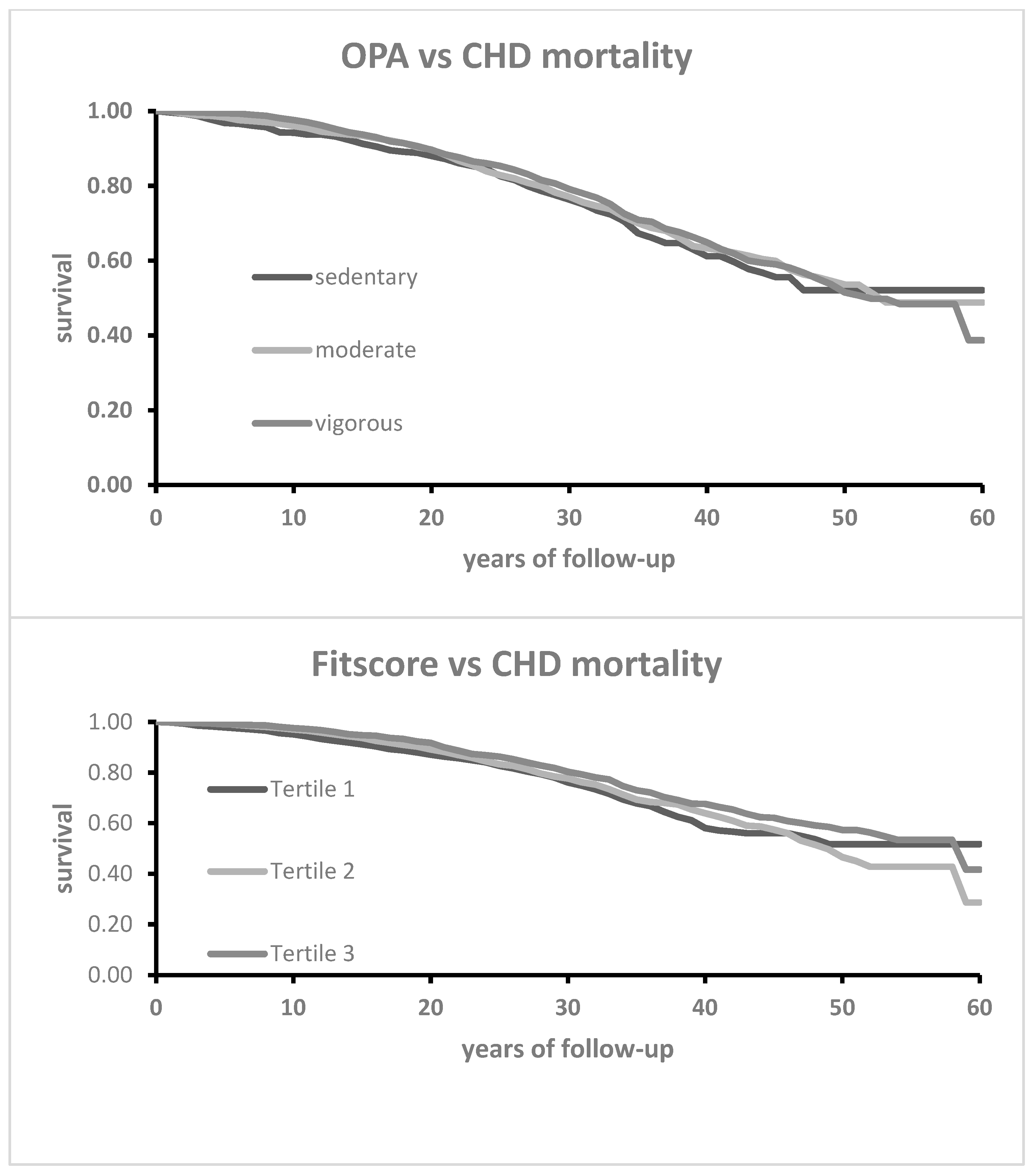
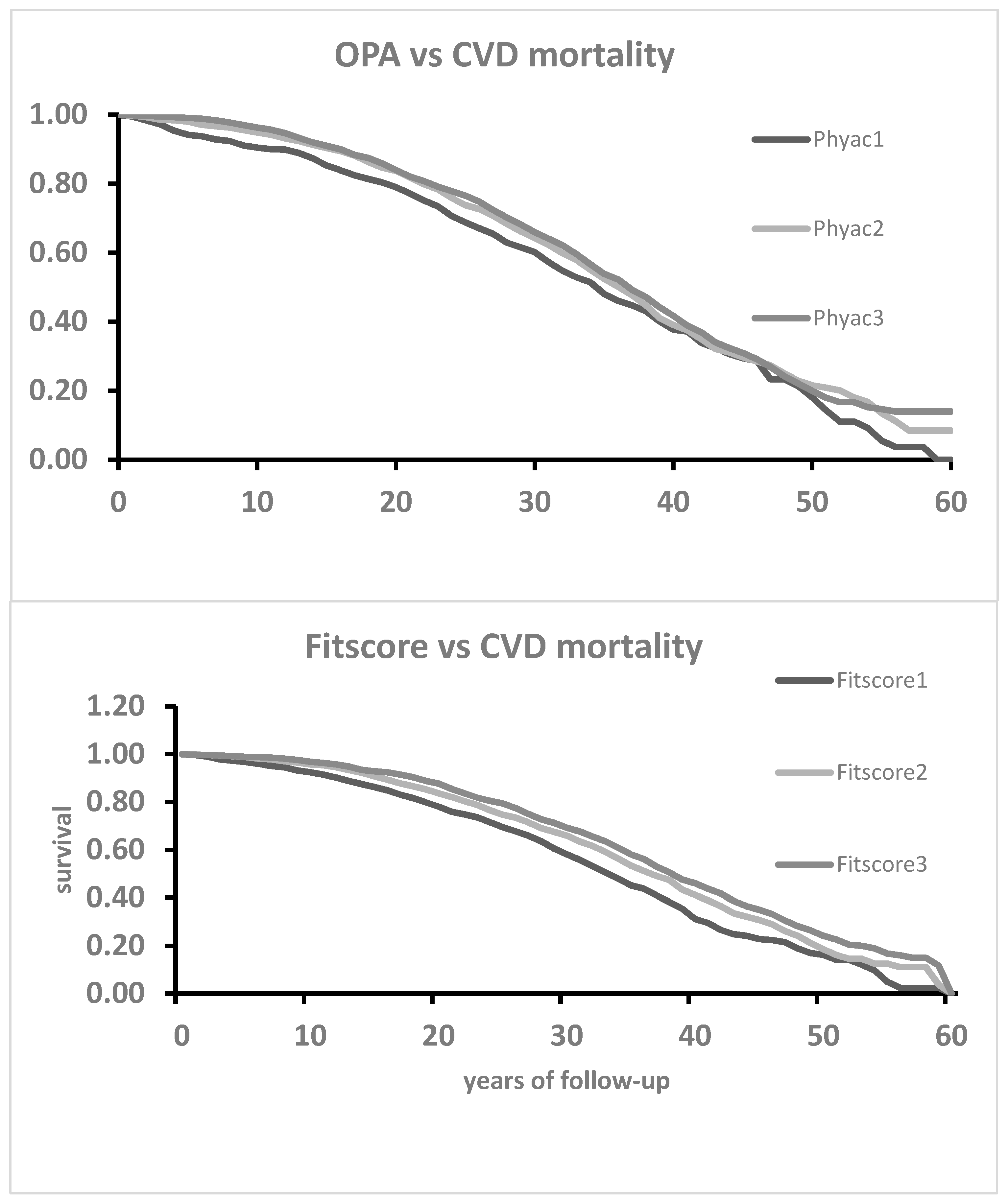
3.3. Prediction of 60-Year Mortality from CHD, HDUE, Stroke and CVD by OPA and Fitscore
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Powell, K.E.; Paffenbarger, R.S., Jr. Workshop on Epidemiologic and Public Health Aspects of Physical Activity and Exercise: A summary. Public. Health Rep. 1985, 100, 118–126. [Google Scholar]
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Menotti, A.; Keys, A.; Kromhout, D.; Nissinen, A.; Blackburn, H.; Fidanza, F.; Giampaoli, S.; Karvonen, M.; Pekkanen, J.; Punsar, S. All-cause mortality and its determinants in middle-aged men in Finland, the Netherlands and Italy in a 25-year follow-up. J. Epidemiol. Commun. Health 1991, 45, 125–130. [Google Scholar] [CrossRef]
- Menotti, A.; Puddu, P.E.; Tolonen, H.; Kafatos, A. Age at death in cohorts of middle-aged men followed-up until nearly extinction: The European Areas of the Seven Countries Study. Ann. Med. 2018, 50, 620–633. [Google Scholar] [CrossRef]
- Puddu, P.E.; Menotti, A.; Jacobs, D.R., Jr.; Adachi, H.; Kafatos, A.; Tolonen, H. Cardiovascular risk factors predict age at death in 60-year follow-up of the Seven Countries Study. Aging Clin. Exp. Res. 2023, 35, 193–202. [Google Scholar] [CrossRef]
- Sandvik, L.; Erikssen, J.; Thaulow, E.; Erikssen, G.; Mundal, R.; Rodahl, K. Physical fitness as a predictor of mortality among healthy, middle-aged Norwegian men. N. Engl. J. Med. 1993, 328, 533–537. [Google Scholar] [CrossRef]
- Blair, S.N.; Kampert, J.B.; Kohl, H.W., 3rd; Barlow, C.E.; Macera, C.A.; Paffenbarger, R.S.; Gibbons, L.W. Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA 1996, 276, 205–210. [Google Scholar] [CrossRef]
- Villeneuve, P.J.; Morrison, H.I.; Craig, C.L.; Schaubel, D.E. Physical activity, physical fitness, and risk of dying. Epidemiology 1998, 9, 626–631. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Bassett, D.R., Jr.; Strath, S.J.; Swartz, A.M.; O’Brien, W.L.; Thompson, R.W.; Jones, D.A.; Macera, C.A.; Kimsey, C.D. Comparison of three methods for measuring the time spent in physical activity. Med. Sci. Sports Exerc. 2000, 32 (Suppl. S9), S457–S464. [Google Scholar] [CrossRef]
- Macera, C.A.; Ham, S.A.; Jones, D.A.; Kimsey, C.D.; Ainsworth, B.E.; Neff, L.J. Limitations on the use of a single screening question to measure sedentary behavior. Am. J. Public Health 2001, 91, 2010–2012. [Google Scholar] [CrossRef]
- Cheng, Y.J.; Macera, C.A.; Addy, C.L.; Sy, F.S.; Wieland, D.; Blair, S.N. Effects of physical activity on exercise tests and respiratory function. Br. J. Sports Med. 2003, 37, 521–528. [Google Scholar] [CrossRef]
- Myers, J.; Kaykha, A.; George, S.; Abella, J.; Zaheer, N.; Lear, S.; Yamazaki, T.; Froelicher, V. Fitness versus physical activity patterns in predicting mortality in men. Am. J. Med. 2004, 117, 912–918. [Google Scholar] [CrossRef]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef]
- De Fina, L.F.; Haskell, W.L.; Willis, B.L.; Barlow, C.E.; Finley, C.E.; Levine, B.D.; Cooper, K.H. Physical activity versus cardiorespiratory fitness: Two (partly) distinct components of cardiovascular health? Prog. Cardiovasc. Dis. 2015, 57, 324–329. [Google Scholar] [CrossRef]
- Myers, J.; McAuley, P.; Lavie, C.J.; Despres, J.P.; Arena, R.; Kokkinos, P. Physical activity and cardiorespiratory fitness as major markers of cardiovascular risk: Their independent and interwoven importance to health status. Prog. Cardiovasc. Dis. 2015, 57, 306–314. [Google Scholar] [CrossRef]
- Davidson, T.; Vainshelboim, B.; Kokkinos, P.; Myers, J.; Ross, R. Cardiorespiratory fitness versus physical activity as predictors of all-cause mortality in men. Am. Heart J. 2018, 196, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Menotti, A.; Puddu, P.E.; Geleijnse, J.M.; Kafatos, A.; Tolonen, H. Physical activity and physical fitness in prediction of all-cuse mortality and age at death in European extinct cohorts of middle-aged men followef for 60 years. Eur. J. Prev. Cardiol. 2024. online ahead of print. [Google Scholar] [CrossRef]
- Keys, A.; Aravanis, C.; Blackburn, H.W.; Van Buchem, F.S.; Buzina, R.; Djordjević, B.D.; Dontas, A.S.; Fidanza, F.; Karvonen, M.J.; Kimura, N.; et al. Epidemiological studies related to coronary heart disease: Characteristics of men aged 40-59 in seven countries. Acta Med. Scand. 1967, 460, 1–392. [Google Scholar] [CrossRef]
- Kromhout, D.; Menotti, A.; Blackburn, H. Prevention of coronary heart disease. In Diet, Lifestyle and Risk Factors in the Seven Countries Study; Kluwer Public: Norwell, MA, USA; Dordrecht, NL, USA, 2022; pp. 1–267. [Google Scholar]
- Rose, G.; Blackburn, H. Cardiovascular Survey Methods; World Health Organization: Geneva, Switzerland, 1968; pp. 1–188. [Google Scholar]
- Hemsfield, S.B.; MacManus, C.; Smith, J.; Stevens, V.; Nixon, D.W. Anthropometric measurement of muscle mass: Revised equations for calculating bone-free arm muscle area. Am. J. Clin. Nutr. 1982, 36, 680–690. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.T.; Keys, A. Cholesterol in serum and lipoprotein fractions: Its measurement and stability. Clin. Chem. 1956, 2, 145–159. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Diseases and Causes of Death, 8th Revision; World Health Organization: Geneva, Switzerland, 1965; ICD-8. [Google Scholar]
- Menotti, A.; Puddu, P.E. Heart Diseases of uncertain etiology: Epidemiological observations compared with clinical experience. Med. Res. Arch. 2022, 10, 9. [Google Scholar]
- Puddu, P.E.; Menotti, A. Heart disease of uncertain etiology: A new definition of heart failure for epidemiological studies. J. Cardiovasc. Dev. Dis. 2023, 10, 132. [Google Scholar] [CrossRef]
- Lopez-Jaramillo, P.; Lopez-Lopez, J.P.; Tole, M.C.; Cohen, D.D. Increasing muscular strength to improve cardiometabolic risk factors. Clin. Investig. Arterioscler. 2023, 35, 144–154. [Google Scholar]
- Puddu, P.E.; Menotti, A.; Tolonen, H.; Nedeljkovic, S.; Kafatos, A. Determinants of 40-year all-cause mortality in the European cohorts of the Seven Countries Study. Eur. J. Epidemiol. 2011, 26, 595–608. [Google Scholar] [CrossRef]
- Palatini, P.; Parati, G.; Virdis, A.; Reboldi, G.; Masi, S.; Mengozzi, A.; Casiglia, E.; Tikhonoff, V.; Cicero, A.F.G.; Ungar, A.; et al. High heart rate amplifies the risk of cardiovascular mortality associated with elevated uric acid. Eur. J. Prev. Cardiol. 2023, 30, 2047–2048. [Google Scholar] [CrossRef]
- Delgado-Betancourt, V.; Chinda, K.; Mesirca, P.; Barrère, C.; Covinhes, A.; Gallot, L.; Vincent, A.; Bidaud, I.; Kumphune, S.; Nargeot, J.; et al. Heart rate reduction after genetic ablation of L-type Cav1.3 channels induces cardioprotection against ischemia-reperfusion injury. Front. Cardiovasc. Med. 2023, 10, 1134503. [Google Scholar] [CrossRef]
- Weinmayr, G.; Schulz, H.; Klenk, J.; Denkinger, M.; Duran-Tauleria, E.; Koenig, W.; Dallmeier, D.; Rothenbacher, D.; Böhm, B.; Geiger, H.; et al. Association of lung function with overall mortality is independent of inflammatory, cardiac, and functional biomarkers in older adults: The ActiFE-study. Sci. Rep. 2020, 10, 11862. [Google Scholar] [CrossRef]
- Costanzo, S.; Magnacca, S.; Bonaccio, M.; Di Castelnuovo, A.; Piraino, A.; Cerletti, C.; de Gaetano, G.; Donati, M.B.; Iacoviello, L. Reduced pulmonary function, low-grade inflammation and increased risk of total and cardiovascular mortality in a general adult population: Prospective results from the Moli-sani study. Respir. Med. 2021, 184, 106441. [Google Scholar] [CrossRef]
- Puddu, P.E.; Menotti, A.; Kromhout, D.; Kafatos, A.; Tolonen, H. Chronic bronchitis in the 50-year follow-up of the European cohorts of the Seven Countries Study: Prevalence, mortality and association with cardiovascular diseases. Respir. Med. 2021, 181, 106385. [Google Scholar] [CrossRef]
- Cillekens, B.; Huysmans, M.A.; Holtermann, A.; van Mechelen, W.; Straker, L.; Krause, N.; van der Beek, A.J.; Coenen, P. Physical activity at work may not be health enhancing. A systematic review with meta-analysis on the association between occupational physical activity and cardiovascular disease mortality covering 23 studies with 655892 participants. Scand. J. Work. Environ. Health 2022, 48, 86–98. [Google Scholar] [CrossRef]
- Löllgen, H.; Böckenhoff, A.; Knapp, G. Physical activity and all-cause mortality: An updated meta-analysis with different intensity categories. Int. J. Sports Med. 2009, 30, 313–324. [Google Scholar] [CrossRef]
- Bonekamp, N.E.; Visseren, F.L.J.; Ruigrok, Y.; Cramer, M.J.M.; de Borst, G.J.; May, A.M.; Koopal, C. Leisure-time and occupational physical activity and health outcomes in cardiovascular disease. Heart 2023, 109, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Quinn, T.D.; Lane, A.; Gabrie, K.P.; Sternfeld, B.; Jacobs, D.R.; Smith, P.; Gibbs, B.B. Associations between occupational physical activity and left ventricular structure and function over 25 years in CARDIA. Eur. J. Prev. Cardiol. 2024, 31, 425–433. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Finland | The Netherlands | Italy | Greece | Total | p of Chi Squared | |
|---|---|---|---|---|---|---|
| N | 1677 | 878 | 1712 | 1215 | 5482 | |
| 60-year CHD death rate per 1000 | 352 (12) | 267 (15) | 164 (9) | 132 (10) | 232 (6) | <0.0001 |
| 60-year HDUE death rate per 1000 | 61 (6) | 65 (8) | 120 (8) | 137 (10) | 97 (4) | <0.0001 |
| 60-year stroke death rate per 1000 | 101 (7) | 84 (9) | 131 (8) | 164 (14) | 122 (4) | <0.0001 |
| 60-year CVD death rate per 1000 | 513 (12) | 416 (17) | 416 (12) | 436 (14) | 450 (7) | <0.0001 |
| Arm Circumference mm | Heart Rate Beats/min | Vital Capacity L/m2 | Fitscore Arbitrary Units | |
|---|---|---|---|---|
| Physical activity Low N = 764 | 256.5 (24.6) | 73.7 (14.4) | 1.44 (0.24) | −0.50 (1.05) |
| Physical activity Intermediate N = 1617 | 263.9 (22.6) | 70.7 (13.2) | 1.49 (0.22) | −0.12 (0.92) |
| Physical activity High N = 3100 | 263.1 (21.6) | 66.8 (12.3) | 1.59 (0.24) | 0.18 (0.97) |
| ANOVA | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| Fitscore low N = 1827 | 244.8 (17.8) | 71.2 (14.2) | 1.34 (0.19) | |
| Fitscore intermediate N = 1828 | 262.8 (15.5) | 68.6 (12.9) | 1.53 (0.16) | |
| Fitscore high N = 1827 | 279.6 (18.8) | 67.0 (11.8) | 1.73 (0.20) | |
| ANOVA | <0.0001 | <0.0001 | <0.0001 |
| Coefficient | p Value | Hazard Ratio | 95% CI | |
|---|---|---|---|---|
| CHD mortality | ||||
| OPA low | Reference | --- | --- | --- |
| OPA intermediate | −0.0736 | 0.4221 | 0.93 | 0.78 1.11 |
| OPA high | −0.0895 | 0.2999 | 0.91 | 0.77 1.08 |
| Fitscore low | Reference | --- | --- | --- |
| Fitscore intermediate | −0.0889 | 0.2030 | 0.91 | 0.80 1.05 |
| Fitscore high | −0.2545 | 0.0004 | 0.78 | 0.67 0.89 |
| HDUE mortality | ||||
| OPA low | Reference | --- | --- | --- |
| OPA intermediate | −0.2409 | 0.0824 | 0.79 | 0.60 1.03 |
| OPA high | −0.1791 | 0.1631 | 0.84 | 0.65 1.07 |
| Fitscore low | Reference | --- | --- | --- |
| Fitscore intermediate | −0.3646 | 0.0009 | 0.69 | 0.56 0.86 |
| Fitscore high | −0.4839 | <0.0001 | 0.61 | 0.50 0.76 |
| Stroke mortality | ||||
| OPA low | Reference | --- | --- | --- |
| OPA intermediate | −0.1424 | 0.2473 | 0.87 | 0.69 1.10 |
| OPA high | −0.1458 | 0.2070 | 0.86 | 0.68 1.08 |
| Fitscore low | Reference | --- | --- | --- |
| Fitscore intermediate | −0.4324 | <0.0001 | 0.65 | 0.54 0.78 |
| Fitscore high | −0.5491 | <0.0001 | 0.58 | 0.48 0.70 |
| CVD mortality | ||||
| OPA low | Reference | --- | --- | --- |
| OPA intermediate | −0.1280 | 0.0487 | 0.88 | 0.77 0.99 |
| OPA high | −0.1240 | 0.0416 | 0.88 | 0.78 0.99 |
| Fitscore low | Reference | --- | --- | --- |
| Fitscore intermediate | −0.2419 | <0.0001 | 0.79 | 0.71 0.87 |
| Fitscore high | −0.3878 | <0.0001 | 0.68 | 0.61 0.75 |
| CHD Mortality | |||||
|---|---|---|---|---|---|
| Variable | Coefficient | p Value | Delta | Hazard Ratio | 95% CI |
| Age | 0.0658 | <0.0001 | 5 | 1.39 | 1.31 1.47 |
| Body mass index | 0.0101 | 0.3029 | 3.5 | 1.04 | 0.97 1.11 |
| Cigarettes | 0.0204 | <0.0001 | 10 | 1.23 | 1.16 1.29 |
| Systolic blood pressure | 0.0151 | <0.0001 | 20 | 1.35 | 1.28 1.43 |
| Serum cholesterol | 0.0043 | <0.0001 | 50 | 1.24 | 1.17 1.31 |
| OPA low | reference | --- | --- | --- | --- |
| OPA intermediate | −0.0218 | 0.8145 | 1 | 0.98 | 0.82 1.17 |
| OPA high | −0.1638 | 0.0810 | 1 | 0.85 | 0.71 1.02 |
| Fitscore low | reference | --- | --- | --- | --- |
| Fitscore intermediate | −0.1374 | 0.0597 | 1 | 0.87 | 0.76 1.01 |
| Fiscore high | −0.2055 | 0.0127 | 1 | 0.81 | 0.69 0.96 |
| The Netherlands | −0.4345 | <0.0001 | 1 | 0.65 | 0.54 0.77 |
| Italy | −0.6441 | <0.0001 | 1 | 0.53 | 0.45 0.62 |
| Greece | −1.1755 | <0.0001 | 1 | 0.31 | 0.26 0.37 |
| Finland | reference | ||||
| HDUE Mortality | |||||
|---|---|---|---|---|---|
| Variable | Coefficient | p Value | Delta | Hazard Ratio | 95% CI |
| Age | 0.1436 | <0.0001 | 5 | 2.05 | 1.86 2.26 |
| Body mass index | 0.0300 | 0.0469 | 3.5 | 1.11 | 1.00 1.23 |
| Cigarettes | 0.0186 | <0.0001 | 10 | 1.20 | 1.11 1.31 |
| Systolic blood pressure | 0.0113 | <0.0001 | 20 | 1.25 | 1.14 1.38 |
| Serum cholesterol | 0.0002 | 0.8289 | 50 | 1.01 | 0.91 1.12 |
| OPA low | reference | --- | --- | --- | --- |
| OPA intermediate | −0.2413 | 0.0862 | 1 | 0.79 | 0.60 1.03 |
| OPA high | −0.2954 | 0.0319 | 1 | 0.74 | 0.57 0.97 |
| Fitscore low | reference | --- | --- | --- | --- |
| Fitscore intermediate | −0.2319 | 0.0411 | 1 | 0.79 | 0.63 0.99 |
| Fiscore high | −0.3280 | 0.0116 | 1 | 0.72 | 0.56 0.93 |
| The Netherlands | −0.2287 | 0.0116 | 1 | 0.80 | 0.56 1.13 |
| Italy | 0.4602 | 0.0011 | 1 | 1.58 | 1.20 2.09 |
| Greece | 0.1673 | 0.2384 | 1 | 1.18 | 0.90 1.56 |
| Finland | reference | --- | --- | --- | --- |
| Stroke Mortality | |||||
|---|---|---|---|---|---|
| Variable | Coefficient | p Value | Delta | Hazard Ratio | 95% CI |
| Age | 0.1139 | <0.0001 | 5 | 1.77 | 1.63 1.92 |
| Body mass index | 0.0010 | 0.9395 | 3.5 | 1.00 | 0.92 1.09 |
| Cigarettes | 0.0002 | 0.9631 | 10 | 1.00 | 0.92 1.09 |
| Systolic blood pressure | 0.0154 | <0.0001 | 20 | 1.36 | 1.26 1.47 |
| Serum cholesterol | 0.0003 | 0.7353 | 50 | 1.02 | 0.93 1.11 |
| OPA low | reference | --- | --- | --- | --- |
| OPA intermediate | −0.1389 | 0.2656 | 1 | 0.87 | 0.68 1.11 |
| OPA high | −0.3106 | 0.0121 | 1 | 0.73 | 0.57 0.93 |
| Fitscore low | reference | --- | --- | --- | --- |
| Fitscore intermediate | −0.2801 | 0.0047 | 1 | 0.76 | 0.62 0.92 |
| Fiscore high | −0.3171 | 0.0053 | 1 | 0.73 | 0.58 0.91 |
| The Netherlands | −0.5080 | 0.0009 | 1 | 0.60 | 0.45 0.81 |
| Italy | 0.1316 | 0.2705 | 1 | 1.14 | 0.90 1.44 |
| Greece | −0.0306 | 0.7960 | 1 | 0.97 | 0.77 1.22 |
| Finland | reference | --- | --- | --- | --- |
| CVD mortality | |||||
|---|---|---|---|---|---|
| Variable | Coefficient | p Value | Delta | Hazard Ratio | 95% CI |
| Age | 0.0944 | <0.0001 | 5 | 1.60 | 0.54 1.67 |
| Body mass index | 0.0105 | 0.1350 | 3.5 | 1.04 | 0.99 1.09 |
| Cigarettes | 0.0149 | <0.0001 | 10 | 1.16 | 1.11 1.21 |
| Systolic blood pressure | 0.0144 | <0.0001 | 20 | 1.33 | 1.28 1.39 |
| Serum cholesterol | 0.0026 | <0.0001 | 50 | 1.14 | 1.09 1.19 |
| OPA low | reference | --- | --- | --- | --- |
| OPA intermediate | −0.1011 | 0.1240 | 1 | 0.90 | 0.79 1.03 |
| OPA high | −0.2262 | 0.0006 | 1 | 0.80 | 0.70 0.91 |
| Fitscore low | reference | --- | --- | --- | --- |
| Fitscore intermediate | −0.1983 | 0.0001 | 1 | 0.82 | 0.74 0.91 |
| Fiscore high | −0.2603 | <0.0001 | 1 | 0.77 | 0.69 0.87 |
| The Netherlands | −0.4353 | <0.0001 | 1 | 0.65 | 0.56 0.74 |
| Italy | −0.2206 | 0.0002 | 1 | 0.80 | 0.71 0.90 |
| Greece | −0.5435 | <0.0001 | 1 | 0.58 | 0.51 0.66 |
| Finland | reference | --- | --- | --- | --- |
| End-Point and Time Period | N | Arm Circumference mm | Heart Rate Beats/min | Vital Capacity L/m2 |
|---|---|---|---|---|
| CHD 0–30 | 896 | 260.7 (21.6) | 70.0 (13.3) | 1.55 (0.23) |
| CHD 31–60 | 374 | 264.5 (22.0) | 66.5 (11.6) | 1.58 (0.23) |
| p of t test | 0.0046 | <0.0001 | 0.0343 | |
| HDUE 0–30 | 223 | 261.9 (23.9) | 68.8 (14.1) | 1.47 (0.27) |
| HDUE 31–60 | 308 | 267.0 (20.6) | 65.7 (12.2) | 1.57 (0.24) |
| p | 0.0088 | 0.0070 | <0.0001 | |
| Stroke 0–30 | 415 | 262.0 (22.6) | 69.9 (13.3) | 1.50 (0.23) |
| Stroke 31–60 | 252 | 265.5 (21.2) | 69.3 (13.0) | 1.57 (0.24) |
| p of t test | 0.0476 | 0.5691 | 0.0002 | |
| CVD 0–30 | 1534 | 261.2 (22.2) | 69.8 (13.4) | 1.52 (0.24) |
| CVD 31–60 | 934 | 265.6 (21.3) | 67.0 (12.2) | 1.58 (0.24) |
| p of t test | <0.0001 | <0.0001 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puddu, P.E.; Kafatos, A.; Tolonen, H.; Geleijnse, J.M.; Menotti, A. Occupational Physical Activity and Fitness in Predicting Cardiovascular Mortality among European Cohorts of Middle-Aged Men: A 60-Year Follow-Up in the Seven Countries Study. Hearts 2024, 5, 259-274. https://doi.org/10.3390/hearts5030019
Puddu PE, Kafatos A, Tolonen H, Geleijnse JM, Menotti A. Occupational Physical Activity and Fitness in Predicting Cardiovascular Mortality among European Cohorts of Middle-Aged Men: A 60-Year Follow-Up in the Seven Countries Study. Hearts. 2024; 5(3):259-274. https://doi.org/10.3390/hearts5030019
Chicago/Turabian StylePuddu, Paolo Emilio, Anthony Kafatos, Hanna Tolonen, Johanna M. Geleijnse, and Alessandro Menotti. 2024. "Occupational Physical Activity and Fitness in Predicting Cardiovascular Mortality among European Cohorts of Middle-Aged Men: A 60-Year Follow-Up in the Seven Countries Study" Hearts 5, no. 3: 259-274. https://doi.org/10.3390/hearts5030019
APA StylePuddu, P. E., Kafatos, A., Tolonen, H., Geleijnse, J. M., & Menotti, A. (2024). Occupational Physical Activity and Fitness in Predicting Cardiovascular Mortality among European Cohorts of Middle-Aged Men: A 60-Year Follow-Up in the Seven Countries Study. Hearts, 5(3), 259-274. https://doi.org/10.3390/hearts5030019