Abstract
Although sinus problems have long been recognized as the most common respiratory symptoms associated with agricultural work, there is a scarcity of recent studies and/or reliable estimates as to the true prevalence or risk factors of sinus problems related to farming. The aim of this study was to determine the prevalence of sinus problems in farming and non-farming rural populations and further investigate the association of individual (for example life-style, occupational), contextual (e.g., environmental), and important covariates (e.g., age, sex) with sinus problems. A large-scale cross-sectional study was conducted in farm and non-farm residents of rural Saskatchewan, Canada. A logistic regression model based on a generalized estimating equations approach were fitted to investigate the risk factors of sinus problems. Sinus problems were reported by 2755 (34.0%) of the 8101 subjects. Farm residents were more likely to spend their first year of life on farm compared with non-farm residents, and indicated a significantly lower risk of sinus problems. Meanwhile, occupational exposure to solvent and mold were associated with an increased risk of sinus problems. Some health conditions such as allergy and stomach acidity/reflux, family history, and female sex were also related to a higher risk of sinus problems. Farm residents had a significantly lower risk of sinus problems than non-farm residents, likely due to the exposure to farm specific environments in their early life.
1. Introduction
Sinus problems including rhinitis and sinusitis are among the most common medical conditions, which can significantly decrease quality of life, aggravate comorbid conditions such as asthma, and require significant direct medical expenditures [1,2,3,4,5]. They also create even greater indirect costs to society by causing lost work and schooldays and reduced workplace productivity and school learning [2,3]. Based on the National Population Health Survey data from 1998 to 1999, the prevalence of self-reported doctor diagnosed chronic rhinosinusitis was 5.2% with 95% confidence interval (4.8–5.7%) [6].
Sinus problems have long been recognized as common respiratory symptoms associated with agricultural work, however, there is a scarcity of recent studies and/or reliable estimates as to the true prevalence or risk factors of sinus problems related to farming [3,7,8]. It has been reported that breeding and handling of livestock, dairy production, swine barn exposures, and grain farming increased nasal inflammation and symptoms [3,7]. Exposure to pesticides has also been associated with many respiratory symptoms including sinus problems [3,9]. On the other hand, several studies have identified some of the exposures associated with a farming lifestyle that contributed to the reduced risk of rhinitis, asthma, and allergic diseases in farm children (i.e., contact with livestock; contact with animal feed such as hay, grain, straw, and silage; and the consumption of unprocessed cow’s milk) [1,4,5,10,11,12,13,14,15]. The reduced risk in farm children has been attributed to higher endotoxin levels and more diverse exposures to microbial components in the farm environment [1,4,10,11,12,15]. This so-called “hygiene hypothesis” has a theoretical basis that the type and level of stimulation from the microbial environment may influence the postnatal differentiation of T-helper lymphocytes [1,4,5,10,11,13,14], and it supports the lifelong protective effect of farm exposures in early childhood against the development of allergies [11,15]. Some studies, however, failed to identify this protective effect [16] and the others reported that some farming and poor hygiene exposures were associated with an increase in the prevalence of rhinitis in schoolchildren [16,17]. There is no evidence which can fully explain this heterogeneity of the effects, although some possible backgrounds were suggested such as type or quantity of exposure, allergic/non-allergic, and early-onset/late-onset outcome [7,15,16,17,18]. There are many potential causative factors of sinus problems, and they sometimes modify the effects of each other. This may contribute to difficulty in reliably identifying risk factors of sinus problems in clinical settings.
The aim of this study was to determine the prevalence of sinus problems in farming and non-farming rural populations and further investigate the association of individual (for example life-style, occupational), contextual (e.g., environmental), and important covariates (e.g., age, sex) with sinus problems. The interactive effects between risk factors on sinus problems were investigated simultaneously to explain accurately the associations among these risk factors and sinus problems.
2. Materials and Methods
2.1. Baseline Survey
The Saskatchewan Rural Health Study (SRHS) design is a prospective cohort study being conducted in two phases: baseline and follow-up. Details of the baseline study are given elsewhere [19]. In brief, 39 rural municipalities (RMs) of the 298 RMs in Saskatchewan and 16 of the 145 towns (population ranging from 500 to 5000) in Saskatchewan were selected to participate in the study. These RMs and towns were selected at random from four quadrants of the province (southeast, southwest, northeast, and northwest). Councils of 32 out of 39 RMs (82.1%) and 15 out of 16 towns (93.8%) agreed to participate on behalf of their residents and supplied mailing addresses. Dillman’s method was utilized to recruit study participants [20]. The study population comprised 8261 individuals (males and females, 18 years of age or older) from 4624 households living in 32 rural municipalities and 15 towns in the study area.
2.2. Variables
Information on the variables described below was collected by self-administered, mailed questionnaires based on the Population Health Framework [21,22]. Some measures of lifestyle factors, occupational exposures, and socio-economic status used in our questionnaire were adopted from previous research studies that had validated these measures [22,23,24]. The SRHS was conducted with the understanding and the voluntary consent of the participants upon return of the questionnaire. The study was approved by the Biomedical Research Ethics Board (Bio# 09-56) of the University of Saskatchewan, Canada.
2.2.1. Primary Outcome
The primary outcome of interest was sinus problems based on a “yes or no” answer to the question “Has a doctor ever said you had sinus trouble ever in your life: yes or no?”.
In our survey, when we asked the question about sinus trouble, we captured the information either on sinusitis (including acute/chronic sinusitis) or rhinitis (including allergic or non-allergic rhinitis) or a combination of both. Sinusitis is an inflammation or swelling of the tissue lining the sinuses, while rhinitis is an inflammation of the nasal mucous membranes. Rhinosinusitis refers to inflammation of the nasal cavities and sinuses [25]. The symptoms of rhinitis and sinusitis overlap, and sinusitis rarely occurs in the absence of rhinitis [2].
2.2.2. Contextual Factors
The contextual factors associated with sinus problems of interest in this study were environmental factors including residence location, indoor/outdoor environment, and socioeconomic status. Designation of residence in a rural dwelling was further classified as living on farm or non-farm based on the question “Where is your home located?” with options: “farm, in town, acreage”. A non-farm category was created by combining town and acreage. This categorization was necessary because farming exposures can be unique compared to non-farming exposures among rural residents. Indoor environment was assessed by response to questions about smoking inside the house, filtered heating systems, dampness, indoor mold, any pets in home, and pesticides applied inside the residence. The outdoor environment was assessed using information about indoor (barn) intensive livestock operation (building), feedlot or corrals, balestack or bales, grain bins, and sewage pond or manure lagoon located near the home. Main drinking water source was also investigated. Socioeconomic status was assessed using household income adequacy, which was a derived variable with four categories based on various combinations of total household income and the number of people living in the household according to the Statistics Canada definition [26].
2.2.3. Individual Factors
The individual factors considered to be associated with sinus problems were: (i) lifestyle or behavior-related factors with an expected impact on health including smoking and alcohol consumption; (ii) early life exposures; (iii) occupational history and its exposures; (iv) co-morbid conditions; and (v) family history of lung disease. Early life exposures were assessed by the response to the questions regarding ever having lived on a farm, lived on a farm during first year of life, mother smoking in pregnancy, breastfed as a child and its term (for ≥6 month or not), and birth weight (<2500 g, 2500–3999 g or ≥4000 g) according to the national reports [27,28]. Information about occupational history was collected (job title; business, industry or service; total number of years at job). Based on the most frequent responses (i.e., farmers, farm managers, farm supervisors, specialized livestock workers and general farm workers) to occupational history questions, a variable farm worker was derived. An association of farm worker was investigated as a possible risk factor of sinus problems. Information on the following occupational exposures was collected: grain dust, mine dust, asbestos dust, wood dust, other dust (specify), livestock, smoke from stubble burning, diesel fumes, welding fumes, solvent fumes, oil/gas-well fumes, herbicides (to kill plants), fungicides (to treat grain), insecticides (to kill insects), molds, radiation, other (specify). As the co-morbid conditions, allergic conditions, ear infection in the past year, stomach acidity or reflux in past year, usual cough, usual phlegm, ever wheeze, ever asthma, ever hay fever, and chronic diseases (diabetes, heart disease, heart attack, arteriosclerosis, hypertension, cystic fibrosis, tuberculosis, stroke, cancer, other (specify)) were included in the analyses. In the present study, the number of chronic diseases (categorized as: ≥2 diseases, 1 disease, or 0 (no disease)) and not each individual disease, seemed appropriate for the analyses because of a very low prevalence of some chronic conditions such as cystic fibrosis (0.1%) or tuberculosis (0.4%). Information about a family history of lung disease was based on biological family member (father, mother, brother/sister) ever having had lung trouble (asthma, emphysema and chronic bronchitis).
2.2.4. Covariates
Information was obtained on covariates of importance such as age, sex, body mass index, and educational attainment. Body mass index (BMI) was derived from self-reported weight and height of the respondent and used to determine normal (<25 kg/m2), overweight (≥25 kg/m2, <30 kg/m2), or obese (≥30 kg/m2).
2.3. Statistical Analysis
Statistical analysis was completed using SPSS version 24.0 statistical software (IBM SPSS 24.0 Statistics for Windows, IBM Corp., Armonk, NY, USA). Prevalence was presented as observed/total and percentage. Chi-square tests were used to determine the association of prevalence of sinus problems and location of residence. A logistic regression model using generalized estimating equations to account for the within-subject (household—considered as level 2) dependencies that occur in the analysis due to multiple individuals (considered as level 1) from the same household was used in the analysis. Based on bi-variable analysis, variables with p < 0.20 became candidates for a multivariable model. All variables that were statistically significant (p < 0.05), important contextual factors (i.e., location of home and region), sex, and age were retained in the final multivariable model. A parsimonious model was selected based on the Quasilikelihood function under the Independence model criteria goodness-of-fit statistic [29,30]. The strength of associations is presented by odds ratios and their 95% confidence intervals.
3. Results
Of the 8261 participants, 160 were excluded because of missing data for sinus problems and/or location of home, leaving 8101 (98.1%) subjects for the analysis. The mean age of population was 55.8 ± 15.7 years (range 18–101 years). There were approximately equal proportions of males (49.2%) and females (50.8%) in this study. Although there were fewer farm residents (42.1%) than non-farm residents (57.9%), the difference was accounted for in the multivariable analyses. Farm residents were more likely to spend their first year of life on a farm compared with non-farm residents (79.4% vs. 59.6%, p < 0.001). Sinus problems were reported by 2755 (34.0%) of the 8101 subjects (Table 1). The prevalence of sinus problems among farm residents was lower than that among non-farm residents (32.3% vs. 35.2%, p = 0.006), especially southwest (33.3% vs. 39.7%, p = 0.015) and northwest of Saskatchewan (30.5% vs. 35.3%, p = 0.013).

Table 1.
Prevalence of sinus problems stratified by geographic location and farm/non-farm residence.
The bi-variable relationships between the contextual factors, individual factors, or covariates and sinus problems are shown in Table 2, Table 3 and Table 4. Univariate logistic regression analyses, adjusted for repeated households, showed that the diagnosis of sinus problems was associated with the following contextual factors, individual factors, and covariates: household income adequacy; region of Saskatchewan (quadrant); location of home (farm/non-farm); dampness in past year; mold inside (mildew odor or musty smell); any pets in the past year; application of insecticides inside the house in the past year; sewage pond or manure lagoon located near home; water source; smoking; alcohol consumption; early life exposures (ever lived on a farm, lived on a farm during first year of life, mother smoking in pregnancy, birth weight, breastfed as a child, breastfed for 6 months or longer); occupational history in farm; adult farming exposure years; occupational exposures (grain dust, asbestos dust, welding fumes, solvents, insecticides, mold, or radiation); health conditions (house dust allergy, cat allergy, dog allergy, grass allergy, pollen allergy, mold allergy, ear infection in past year, stomach acidity, or reflux in past year, usual cough, usual phlegm, ever wheeze, ever asthma, ever hay fever, number of chronic diseases); family histories (father lung disease, mother lung disease, brother/sister lung disease); sex, age, body mass index (BMI) and education.
Table 2.
Bivariable analysis of an association between contextual factors and sinus problems.
Table 3.
Bivariable analysis of the association between individual factors and sinus problems.
Table 4.
Bivariable analysis of the association between individual factors and sinus problems.
The multivariable logistic regression analysis adjusted for covariates and households is presented in Table 5. The contextual factor farm location was significantly associated with decreased risk of sinus problems, while sewage pond located near home was associated with increased risk of sinus problems. Past smoker, low birth weight, occupational exposures to solvents or molds, some health conditions (house dust allergy, pollen allergy, mold allergy, ear infection in past year, stomach acidity or reflux in past year, ever wheeze, and ever hay fever), family histories (father lung disease, mother lung disease, brother/sister lung disease), female sex, and higher educational status were also identified as the significant determinants positively associated with sinus problems.
Table 5.
Multivariable analysis of the dependency of sinus problems on contextual factors, individual factors, and covariates.
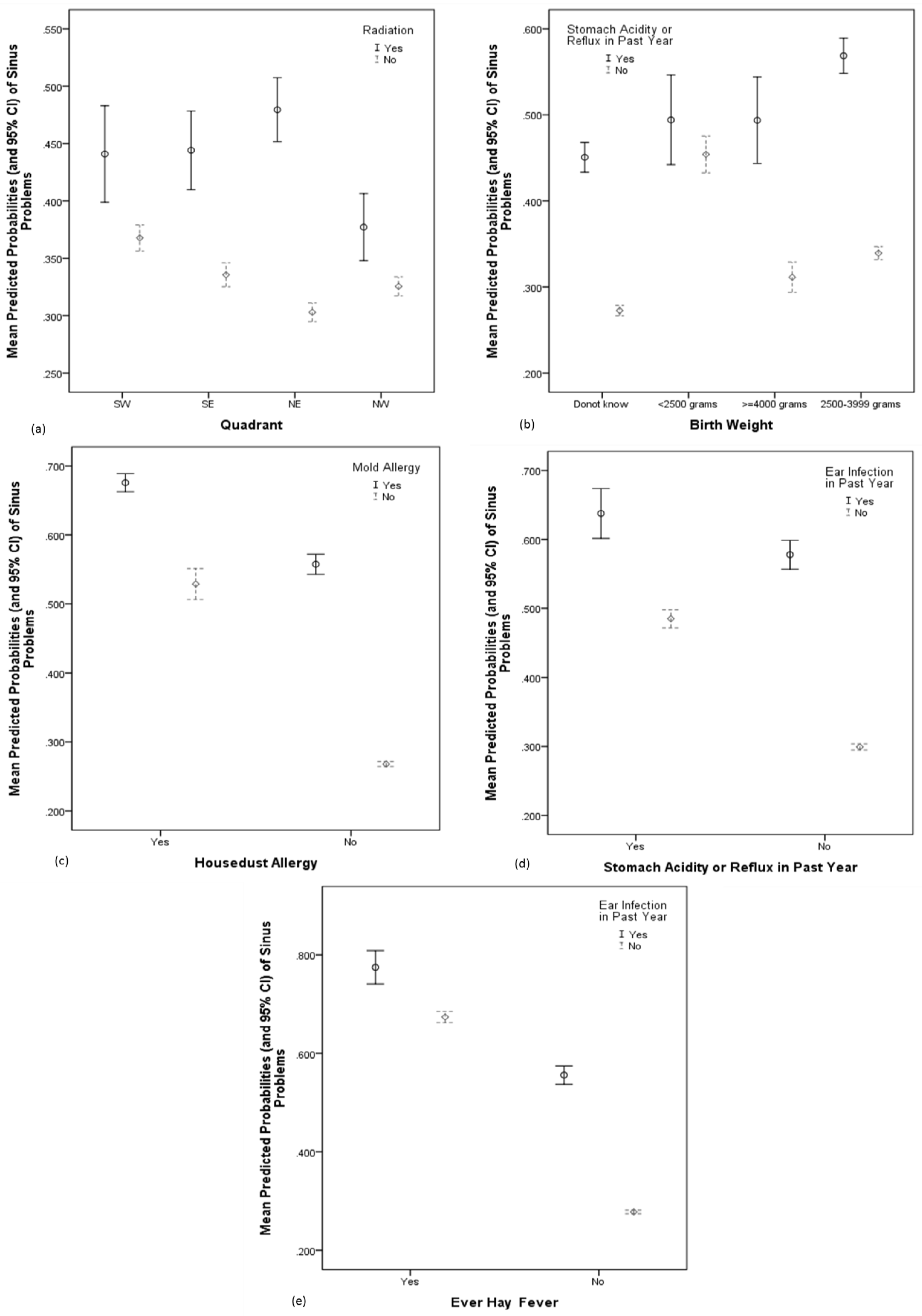
In this final model, five statistically significant interactions were observed (Table 5 and Figure 1). Radiation was a significant risk for sinus problems in all quadrant of Saskatchewan (Figure 1a). The association between birth weight and sinus problems completely differed depending on whether participants were with or without stomach acidity/reflux (Figure 1b). Among subjects without stomach acidity/reflux, lower birth weight indicated an increased risk compared with normal birth weight. In those with stomach acidity/reflux, however, lower birth weight was associated with decreased risk of sinus problems. Mold allergy was related to greater risk of sinus problems in subjects with and without house dust allergy (Figure 1c). Although the effect seemed to be blunted in the former, subjects who had both of these allergies were at a considerably higher risk. A similar tendency was observed in the interaction between stomach acidity/reflux and ear infection and in that between hay fever and ear infection as shown in Figure 1d,e, respectively.
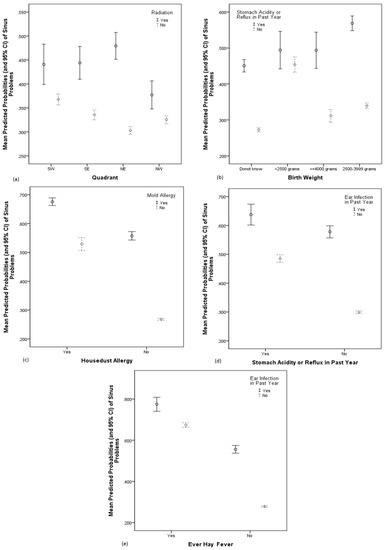
Figure 1.
Mean predicted probabilities of sinus problems, illustrating the interactive associations among risk factors.
4. Discussion
In this large-scale cross-sectional study, we found living on a farm to be associated with a lower risk of sinus problems, whereas some other environmental and occupational exposures, health conditions such as allergy and stomach acidity/reflux, family history of lung disease, and female sex were associated with a higher risk of sinus problems. We also revealed some significant interactive effects between these factors on sinus problems, which have a reasonable physiological or pathological basis. We discuss below the factors associated with sinus problems systematically.
4.1. Environmental Factors
The present study indicated an inverse relationship between farm living and the prevalence of sinus problems. On the other hand, living near a sewage pond or manure lagoon was significantly associated with the prevalence of sinus problems even after multivariable adjustment. Dampness, indoor mold, any pets in home, and pesticides applied inside residence were not included in the multivariable model, whereas they were indicated to be risks of sinus problems in bivariable analyses.
Lower risk of allergic rhinitis in farm specific conditions has been reported by many previous studies [1,4,13,15]. It has been postulated that exposure to endotoxin might promote a skewing of the type I helper T cells (Th1)/type 2 helper T cells (Th2) balance toward non-allergic Th1 responses [1,4], thus protecting against allergies. The immune deviation into either Th1 or Th2 polarization is suggested to be established already at 5 years of age [4]. It is also well known that pregnancy and early life represent a biological window of opportunity for shaping subsequent immune reactivity [5,14]. The timing of exposure seems to be crucial and determines the exposure’s beneficial or detrimental effects [5,7,10,12,14,16]. In the present study, farm residents were more likely to spend their first year of life on farm compared with non-farm residents. On the basis of this information, a high proportion of farm residents who had been exposed to farm specific conditions in their early life might experience the protective effect of living on a farm, via allergic sensitization and shaping subsequent immune responses.
Another possible explanation of the inverse association between living on a farm and sinus problems could relate to selective migration of less healthy residents from rural to urban areas. The subjects or their families may have stopped farming because of symptoms related to exposure. We could not rule out such a “healthy farmer effect” because of lack of information, although the proportion of the subjects who lived on a farm during their first year but not at the time of investigation were not different between subjects with and without sinus problems (47.6% vs. 50.0% in subjects who spent their early life on a farm, p = 0.100).
We could not find any previous studies showing the direct associations between sewage pond or manure lagoon located near home and the prevalence of sinus problems. In the present study, the subjects who lived near a sewage pond were more likely to report dampness (22.8% vs. 17.0%, p < 0.001) and/or indoor mildew odor (20.9% vs. 14.7%, p < 0.001), which both have been reported as risks of a variety of adverse respiratory health conditions including sinus problems [31,32]. Though these factors were not included in the multivariable model, there seems to be a need for more research to investigate whether or not these factors increase the risk of sinus problems.
4.2. Lifestyle
In the present study, compared to non-smokers, ex-smokers were significantly at a greater risk of sinus problems. Cigarette smoking can cause mucosal hyper-responsiveness, resulting in sinus symptoms and intensification of allergic reactions [2]. Adverse respiratory symptoms might make smokers quit smoking and contribute to the higher risk of ex-smokers.
4.3. Early Life Exposure
In a bivariable analysis, we observed that ever lived on a farm and lived on a farm during the first year of life were negatively associated with the prevalence of sinus problems, which supports the evidence of the hygiene hypothesis [4,10,11,12,15]. If the mother smoked during pregnancy, it was significantly associated with the increased risk of sinus problems, however, this variable was not significant at p < 0.05 in the multivariable analysis. In the final model, we found that low birth weight was associated with an increased risk of sinus problems, however, previous studies have reported conflicting results [33].
4.4. Occupational History and Exposures
A significant association was observed between occupational history related to farm work, adult farming exposure years, grain dust, asbestos dust, welding fumes, solvents, insecticides, mold or radiation, and sinus problems in bivariable analyses. Among them, solvents and mold were indicated to be risk factors by the multivariable analysis. Though there is limited information regarding the association between solvent and sinus problems, chemical exposures to paints, epoxies, and resins are known to produce nasal irritation [3]. Slager et al. reported that maintenance activities such as painting and repairing engines were significant predictors of rhinitis [3]. Mold is well known as one of the most common aeroallergens implicated in persistent allergic rhinitis [1,2], and this is consistent with the risk of mold allergy in this study. Although some previous studies reported that specific pesticides such as malathion and glyphosate might contribute to rhinitis in farmers [3,7], any variables regarding pesticides (i.e., insecticides, fungicides, and herbicides) were not retained in the final multivariable model in the current analysis. In the present study, an interactive effect was observed between radiation and quadrant on sinus problems, indicating that an occupational exposure associated with radiation was a significant risk for sinus problems in all quadrants. Some studies reported the post-radiotherapy rhinosinusitis in nasopharyngeal carcinoma patients [34], while there was no report showing the association between sinus problems and environmental or occupational exposure to radiation.
4.5. Health Conditions
House dust allergy, pollen allergy, mold allergy, ear infection, stomach acidity/reflux, wheeze, and hay fever were identified to be risk factors of sinus problems by multivariable analysis. Furthermore, some of these factors closely interacted with each other (i.e., house dust allergy and mold allergy, hay fever and ear infection, and stomach acidity/reflux and ear infection), with location of home (living on a farm and house dust allergy), and with birth weight (birth weight and stomach acidity/reflux).
The coexistence of gastro-esophageal reflux disease (GERD) and various respiratory disorders such as chronic rhinosinusitis or ear infection are reported by several past studies, although a causal link between them has so far not been sufficiently documented [35,36,37,38]. There are few studies showing the association between birth weight and stomach acidity/reflux. A national cohort study of more than 600,000 infants born in Sweden reported that preterm birth is associated with an increased risk of gastric acid-related disorders [39]. Another study using the same population suggested that preterm birth is also associated with a decreased risk of allergic rhinitis, in accordance with other previous studies [33]. However, the influence of stomach acidity/reflux was not considered in these previous studies, and there is no study in which the interactive effect between reflux and birth weight on sinus problems was investigated. In the present study, the association between birth weight and sinus problems completely differed depending on whether subjects were with or without stomach acidity/reflux; lower birth weight represented an increased risk in the subjects without reflux but a decreased risk in the subjects with reflux compared with normal birth weight. To our best knowledge, this is the first study reporting the interactive effect between birth weight and stomach acidity/reflux on the prevalence of sinus problems. Further studies are needed to confirm this finding.
4.6. Family History
In our study, there was no information on family history of sinus problems, however, the information on family history of lung disease (i.e., asthma, chronic bronchitis, and emphysema) was available. Hence, the association between family history of lung disease and sinus problems were investigated. Father, mother, and brother/sister lung disease were all significantly associated with the prevalence of sinus problems. Family history of asthma or allergic diseases have been reported to be a significant predictive factor of their children’s status by many previous studies [1,4,5,10,11,18,40].
4.7. Other Risk Factors (Female Sex and Educational Status)
In the present study, female sex and higher educational status were significantly associated with an increased risk of sinus problems. Female sex has been indicated to be a risk factor of rhinitis, whereas the associations seemed to differ by atopic status and/or population age [4,5,18]. Matheson et al. showed that in subjects who were atopic in adult life, the incidence of rhinitis was higher in boys, but this higher incidence reversed in adult life when women had a higher risk than men; and in subjects without atopy in adult life, females had a consistently increased risk of rhinitis compared with males throughout life [5]. Hormonal factors are a possible explanation for these sex differences [5,41]. The higher risk of sinus problems in females in this study is consistent with the previous studies, because we investigated the incidence of every sinus problem in adult population.
On the other hand, the association between educational status and sinus problems is controversial. Tokunaga et al. reported that higher educational attainment indicated a higher risk of allergic rhinitis [42], whereas some studies have shown the inverse associations [3,40,43]. Educational status, however, seemed to reflect various other socioeconomic, environmental, and occupational factors, rather than to be an independent risk factor itself.
4.8. Limitation and Strengths of This Study
Our study had some limitations that are pertinent to all questionnaire-based cross-sectional studies. The questionnaire-derived information could result in recall bias, misclassification, and underestimation of the prevalence of sinus problems and its association with the factors. There was also the lack of data on the intensity and age of initial exposures to the factors as well as no objective measurements of allergy status such as skin prick positivity or serum Immunoglobulin E (IgE) levels. Therefore, it was not possible to distinguish between allergic and non-allergic sinus problems. The information was collected on sinus trouble but not separately as rhinitis, chronic rhinitis/sinusitis, nasal disorders, or sinus disorders.
The major strength of this study is the large sample size and extensive information which has been obtained on contextual and individual factors and important covariates via self-administered mail-out questionnaires. Because the population studied live in widespread locations in the four quadrants of the province, representing a wide range of geographical areas in Saskatchewan, a mail questionnaire survey seemed to be the best option. Other authors have discussed this issue and they have concluded that with the increasing cost of interviewing, a mail questionnaire surveys in widely spread geographical areas was the best [20,44].
5. Conclusions
In the present study, farm residents had a significantly lower risk of sinus problems than non-farm residents, likely due to exposure to farm specific environments in their early life. Some occupational exposures (solvents and mold) related to farm work, however, exactly associated with an increased risk of sinus problems. The timing and type of the farm exposures are likely responsible for determining the development of non-allergic sinus problems or protection against allergy. We also reported the interactive effect between birth weight and stomach acidity/reflux on the prevalence of sinus problems for the first time. Lower birth weight represented an increased risk in the subjects without reflux but a decreased risk in the subjects with reflux compared with normal birth weight. Further studies are needed to confirm this finding. Our findings provided further insights into the prevalence and determinants of sinus problems in the rural population.
Acknowledgments
This study was funded by a grant from the Canadian Institutes of Health Research “Saskatchewan Rural Health Study”, Canadian Institutes of Health Research MOP-187209-POP-CCAA-11829, approved by the Biomedical Research Ethics Board (Bio# 09-56) of the University of Saskatchewan, Canada. The Saskatchewan Rural Health Study (SRHS) Team consists of: James Dosman (Designated Principal Investigator, University of Saskatchewan, Saskatoon, SK, Canada); Punam Pahwa (Co-principal Investigator, University of Saskatchewan, Saskatoon, SK, Canada); John Gordon (Co-principal Investigator, University of Saskatchewan, Saskatoon, SK, Canada); Yue Chen (University of Ottawa, Ottawa, ON, Canada); Roland Dyck (University of Saskatchewan, Saskatoon, SK, Canada); Louise Hagel (Project Manager, University of Saskatchewan, Saskatoon, SK, Canada); Bonnie Janzen (University of Saskatchewan, Saskatoon, SK, Canada); Chandima Karunanayake (University of Saskatchewan, Saskatoon, SK, Canada); Shelley Kirychuk (University of Saskatchewan, Saskatoon, SK, Canada); Niels Koehncke (University of Saskatchewan, Saskatoon, SK, Canada); Joshua Lawson (University of Saskatchewan, Saskatoon, SK, Canada); William Pickett (Queen’s University, Kingston, ON, Canada); Roger Pitblado (Professor Emeritus, Laurentian University, Sudbury, ON, Canada); Donna Rennie (University of Saskatchewan, Saskatoon, SK, Canada); Ambikaipakan Senthilselvan, (University of Alberta, Edmonton, AB, Canada). We are grateful for the contributions of the rural municipality administrators and the community leaders of the towns included in the study who facilitated access to the study populations and to all of the participants who donated their time to complete and return the survey.
Author Contributions
A.K.-M. authored most of the paper, carried out the statistical analysis, reviewed the literature, reviewed the citations, and created the abstract and manuscript. J.A.D. and P.P. are the co-principal investigators of the SRHS. C.P.K., D.C.R., J.A.L., S.K., R.F.D., N.K., A.S., J.A.D., and P.P. contributed to grant writing, development of study design, questionnaire development, and study coordination. C.P.K., D.C.R., J.A.L., S.K., R.F.D., N.K., A.S., J.A.D., and P.P. provided input into the writing of the manuscript and edited the manuscript. C.P.K. managed the database. The Saskatchewan Rural Health Study Team members contributed during the grant writing and questionnaires development and with conducting the survey. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflict of interest. The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
References
- Wang, D.Y. Risk factors of allergic rhinitis: Genetic or environmental? Ther. Clin. Risk Manag. 2005, 1, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Dykewicz, M.S.; Hamilos, D.L. Rhinitis and sinusitis. J. Allergy Clin. Immunol. 2010, 125, S103–S115. [Google Scholar] [CrossRef] [PubMed]
- Slager, R.E.; Simpson, S.L.; LeVan, T.D.; Poole, J.A.; Sandler, D.P.; Hoppin, J.A. Rhinitis associated with pesticide use among private pesticide applicators in the agricultural health study. J. Toxicol. Environ. Health A 2010, 73, 1382–1393. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.; Ekerljung, L.; Lötvall, J.; Pullerits, T.; Wennergren, G.; Rönmark, E.; Torén, K. Growing up on a farm leads to lifelong protection against allergic rhinitis. Allergy 2010, 65, 1397–1403. [Google Scholar] [CrossRef] [PubMed]
- Matheson, M.C.; Dharmage, S.C.; Abramson, M.J.; Walters, E.H.; Sunyer, J.; de Marco, R.; Leynaert, B.; Heinrich, J.; Jarvis, D.; Norbäck, D.; et al. Early-life risk factors and incidence of rhinitis: Results from the European Community Respiratory Health Study—An international population-based cohort study. J. Allergy Clin. Immunol. 2011, 128, 816–823. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, K.I.; McNally, J.D.; Massoud, E. The health and resource utilization of Canadians with chronic rhinosinusitis. Laryngoscope 2009, 119, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Poole, J.A. Farming-associated environmental exposures and effect on atopic diseases. Ann. Allergy Asthma Immunol. 2012, 109, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Sundaresan, A.S.; Hirsch, A.G.; Storm, M.; Tan, B.K.; Kennedy, T.L.; Greene, J.S.; Kern, R.C.; Schwartz, B.S. Occupational and environmental risk factors for chronic rhinosinusitis: A systematic review. Int. Forum Allergy Rhinol. 2015, 5, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- Demos, K.; Sazakli, E.; Jelastopulu, E.; Charokopos, N.; Ellul, J.; Leotsinidis, M. Does farming have an effect on health status? A comparison study in West Greece. Int. J. Environ. Res. Public Health 2013, 10, 776–792. [Google Scholar] [CrossRef] [PubMed]
- Riedler, J.; Braun-Fahrlander, C.; Eder, W.; Schreuer, M.; Waser, M.; Maisch, S.; Carr, D.; Schierl, R.; Nowak, D.; von Mutius, E.; et al. Exposure to farming in early life and development of asthma and allergy: A cross-sectional survey. Lancet 2001, 358, 1129–1133. [Google Scholar] [CrossRef]
- Leynaert, B.; Neukirch, C.; Jarvis, D.; Chinn, S.; Burney, P.; Neukirch, F.; European Community Respiratory Health Survey. Does living on a farm during childhood protect against asthma, allergic rhinitis, and atopy in adulthood? Am. J. Respir. Crit. Care Med. 2001, 164, 1829–1834. [Google Scholar] [CrossRef] [PubMed]
- Braun-Fahrlander, C.; Riedler, J.; Herz, U.; Eder, W.; Waser, M.; Grize, L.; Maisch, S.; Carr, D.; Gerlach, F.; Bufe, A.; et al. Environmental exposure to endotoxin and its relation to asthma in school-age children. N. Engl. J. Med. 2002, 347, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Waser, M.; Michels, K.B.; Bieli, C.; Flöistrup, H.; Pershagen, G.; von Mutius, E.; Ege, M.; Riedler, J.; Schram-Bijkerk, D.; Brunekreef, B.; et al. Inverse association of farm milk consumption with asthma and allergy in rural and suburban populations across Europe. Clin. Exp. Allergy 2007, 37, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Von Mutius, E.; Vercelli, D. Farm living: Effects on childhood asthma and allergy. Nat. Rev. Immunol. 2010, 10, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Smit, L.A.; Hooiveld, M.; van der Sman-de Beer, F.; Opstal-van Winden, A.W.; Beekhuizen, J.; Wouters, I.M.; Yzermans, C.J.; Heederik, D. Air pollution from livestock farms, and asthma, allergic rhinitis and COPD among neighbouring residents. Occup. Environ. Med. 2014, 71, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Brunekreef, B.; Von Mutius, E.; Wong, G.K.; Odhiambo, J.A.; Clayton, T.O.; ISAAC Phase Three Study Group. Early life exposure to farm animals and symptoms of asthma, rhinoconjunctivitis and eczema: An ISAAC Phase Three Study. Int. J. Epidemiol. 2012, 41, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.J.; Vaca, M.; Rodriguez, A.; Chico, M.E.; Santos, D.N.; Rodrigues, L.C.; Barreto, M.L. Hygiene, atopy and wheeze-eczema-rhinitis symptoms in schoolchildren from urban and rural Ecuador. Thorax 2014, 69, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Matheson, M.C.; Walters, E.H.; Simpson, J.A.; Wharton, C.L.; Ponsonby, A.L.; Johns, D.P.; Jenkins, M.A.; Giles, G.G.; Hopper, J.L.; Abramson, M.J.; et al. Relevance of the hygiene hypothesis to early vs. late onset allergic rhinitis. Clin. Exp. Allergy 2009, 39, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Pahwa, P.; Karunanayake, C.P.; Hagel, L.; Janzen, B.; Pickett, W.; Rennie, D.; Senthilselvan, A.; Lawson, J.; Kirychuk, S.; Dosman, J. The Saskatchewan rural health study: An application of a population health framework to understand respiratory health outcomes. BMC Res. Notes 2012, 5, 400. [Google Scholar] [CrossRef] [PubMed]
- Dillman, D.A. Mail and Internet Surveys: The Tailored Design Method; John Wiley: Hoboken, NJ, USA, 2007. [Google Scholar]
- Pickett, W.; Day, L.; Hagel, L.; Brison, R.J.; Marlenga, B.; Pahwa, P.; Koehncke, N.; Crowe, T.; Phyllis Snodgrass, P.; Dosman, J. The Saskatchewan Farm Injury Cohort: Rationale and methodology. Public Health Rep. 2008, 123, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Strategies for Population Health: Investing in the Health of Canadians; Health Canada: Ottawa, ON, Canada, 1994. Available online: http://publications.gc.ca/collections/Collection/H88-3-30-2001/pdfs/other/strat_e.pdf (accessed on 1 December 2017).
- Statistics Canada. Statistical Report on the Health of Canadians; Statistics Canada: Ottawa, ON, Canada, 1999. Available online: http://www.statcan.gc.ca/pub/82-570-x/4227734-eng.pdf (accessed on 1 December 2017).
- Health Canada. Toward a Healthy Future: Second Report on the Health of Canadians; Health Canada: Ottawa, ON, Canada, 1999. Available online: http://publications.gc.ca/collections/Collection/H39-468-1999E.pdf (accessed on 1 December 2017).
- Desrosiers, M.; Evans, G.A.; Keith, P.K.; Wright, E.D.; Kaplan, A.; Bouchard, J.; Ciavarella, A.; Doyle, P.W.; Javer, A.R.; Leith, E.S.; et al. Canadian clinical practice guidelines for acute and chronic rhinosinusitis. Allergy Asthma Clin. Immunol. 2011, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. National Population Health Survey Household Component: Documentation for the Derived Variables and the Constant Longitudinal Variables; Statistics Canada: Ottawa, ON, Canada. Available online: http://www23.statcan.gc.ca/imdb-bmdi/pub/document/3225_D10_T9_V3-eng.pdf (accessed on 1 December 2017).
- Human Resources and Skills Development Canada, the Public Health Agency of Canada and Indian and Northern Affairs Canada. The Well-Being of Canada’s Young Children: Government of Canada Report; Government of Canada: Ottawa, ON, Canada, 2011. Available online: http://www.dpe-agje-ecd-elcc.ca/eng/ecd/well-being/sp_1027_04_12_eng.pdf (accessed on 1 December 2017).
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.; Curtin, S.C.; Mathews, T.J. Births: Final Data for 2012; National Vital Statistics Reports; National Center for Health Statistics: Hyattsville, MD, USA, 2013; Volume 62. Available online: https://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_09.pdf (accessed on 1 December 2017).
- Pan, W. Akaike’s information criterion in generalized estimating equations. Biometrics 2001, 57, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Hardin, J.W.; Hilbe, J.M. Generalized Estimating Equations; Chapman & Hall/CRC: Boca Raton, FL, USA, 2003. [Google Scholar]
- Fisk, W.J.; Eliseeva, E.A.; Mendell, M.J. Association of residential dampness and mold with respiratory tract infections and bronchitis: A meta-analysis. Environ. Health 2010, 9, 72. [Google Scholar] [CrossRef] [PubMed]
- Thrasher, J.D.; Gray, M.R.; Kilburn, K.H.; Dennis, D.P.; Yu, A. A water-damaged home and health of occupants: A case study. J. Environ. Public Health 2012, 2012, 312836. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Sundquist, K.; Sundquist, J.; Winkleby, M.A. Gestational age at birth and risk of allergic rhinitis in young adulthood. J. Allergy Clin. Immunol. 2011, 127, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.Y.; Tang, A.Z. Bacteriology of postradiotherapy chronic rhinosinusitis in nasopharyngeal carcinoma patients and chronic rhinosinusitis. Eur. Arch. Otorhinolaryngol. 2009, 266, 1403–1407. [Google Scholar] [CrossRef] [PubMed]
- Miura, M.S.; Mascaro, M.; Rosenfeld, R.M. Association between otitis media and gastroesophageal reflux: A systematic review. Otolaryngol. Head Neck Surg. 2012, 146, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Sone, M.; Kato, T.; Nakashima, T. Current concepts of otitis media in adults as a reflux-related disease. Otol. Neurotol. 2013, 34, 1013–1017. [Google Scholar] [CrossRef] [PubMed]
- Katle, E.J.; Hatlebakk, J.G.; Steinsvag, S. Gastroesophageal reflux and rhinosinusitis. Curr. Allergy Asthma Rep. 2013, 13, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Bohnhorst, I.; Jawad, S.; Lange, B.; Kjeldsen, J.; Hansen, J.M.; Kjeldsen, A.D. Prevalence of chronic rhinosinusitis in a population of patients with gastroesophageal reflux disease. Am. J. Rhinol. Allergy 2015, 29, e70–e74. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Winkleby, M.A.; Sundquist, J.; Sundquist, K. Gestational age at birth and risk of gastric acid-related disorders in young adulthood. Ann. Epidemiol. 2012, 22, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Shpakou, A.; Brozek, G.; Stryzhak, A.; Neviartovich, T.; Zejda, J. Allergic diseases and respiratory symptoms in urban and rural children in Grodno Region (Belarus). Pediatr. Allergy Immunol. 2012, 23, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Govaere, E.; Van Gysel, D.; Massa, G.; Verhamme, K.M.; Doli, E.; De Baets, F. The influence of age and gender on sensitization to aero-allergens. Pediatr. Allergy Immunol. 2007, 18, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, T.; Ninomiya, T.; Osawa, Y.; Imoto, Y.; Ito, Y.; Takabayashi, T.; Narita, N.; Kijima, A.; Murota, H.; Katayama, I.; et al. Factors associated with the development and remission of allergic diseases in an epidemiological survey of high school students in Japan. Am. J. Rhinol. Allergy 2015, 29, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Kilty, S.J.; McDonald, J.T.; Johnson, S.; Al-Mutairi, D. Socioeconomic status: A disease modifier of chronic rhinosinusitis? Rhinology 2011, 49, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Hox, J.J.; De Leeuw, E.D. A comparison of nonresponse in mail, telephone, and face-to-face surveys. Qual. Quant. 1994, 28, 329–344. Available online: https://link.springer.com/article/10.1007/BF01097014 (accessed on 3 December 2017). [CrossRef]
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).