
Feasibility of Mindfulness for Burn Survivors and Parents of Children with Burns


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Participants
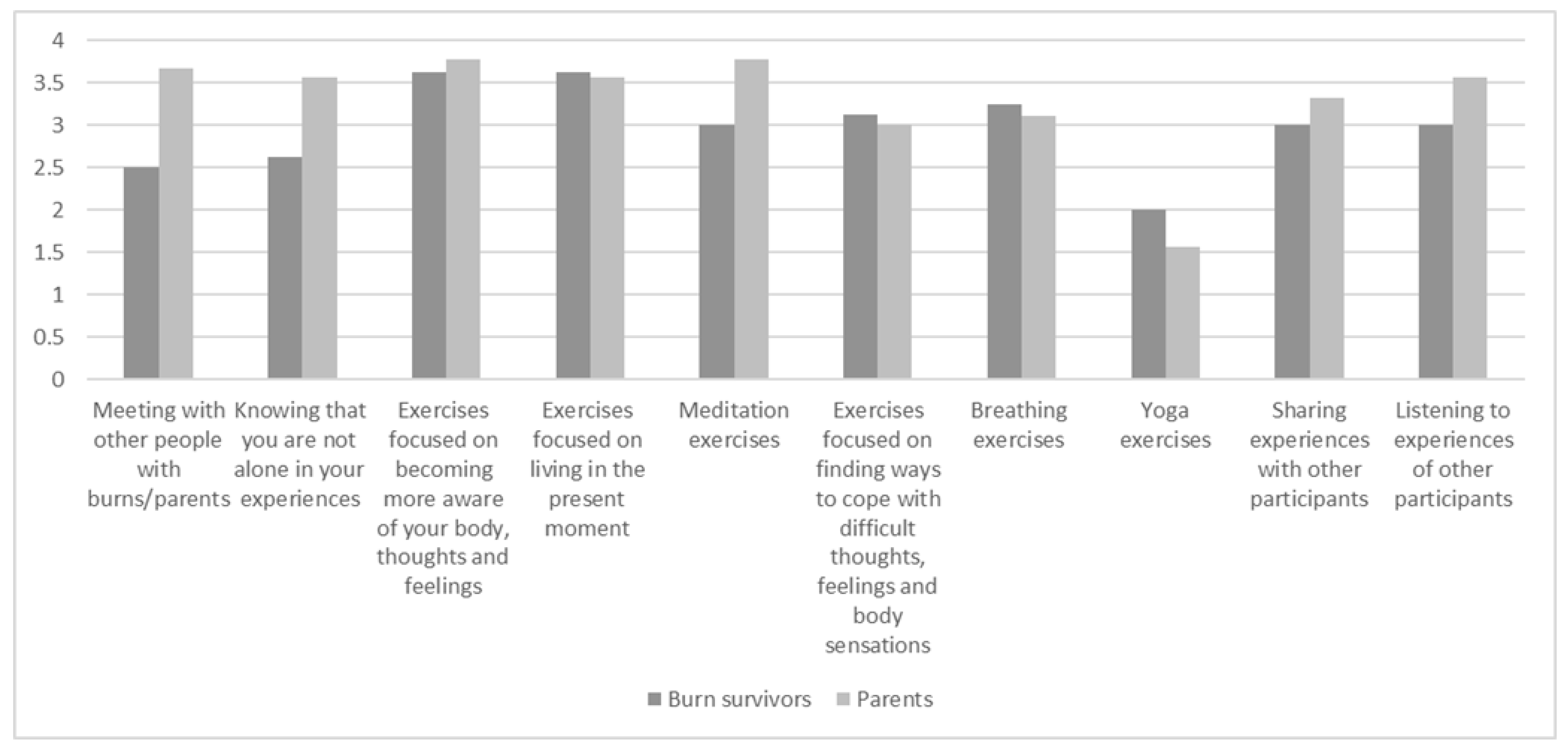
3.2. Feasibility and Acceptability
3.3. Effectiveness
3.3.1. Depressive and PTSD Symptoms
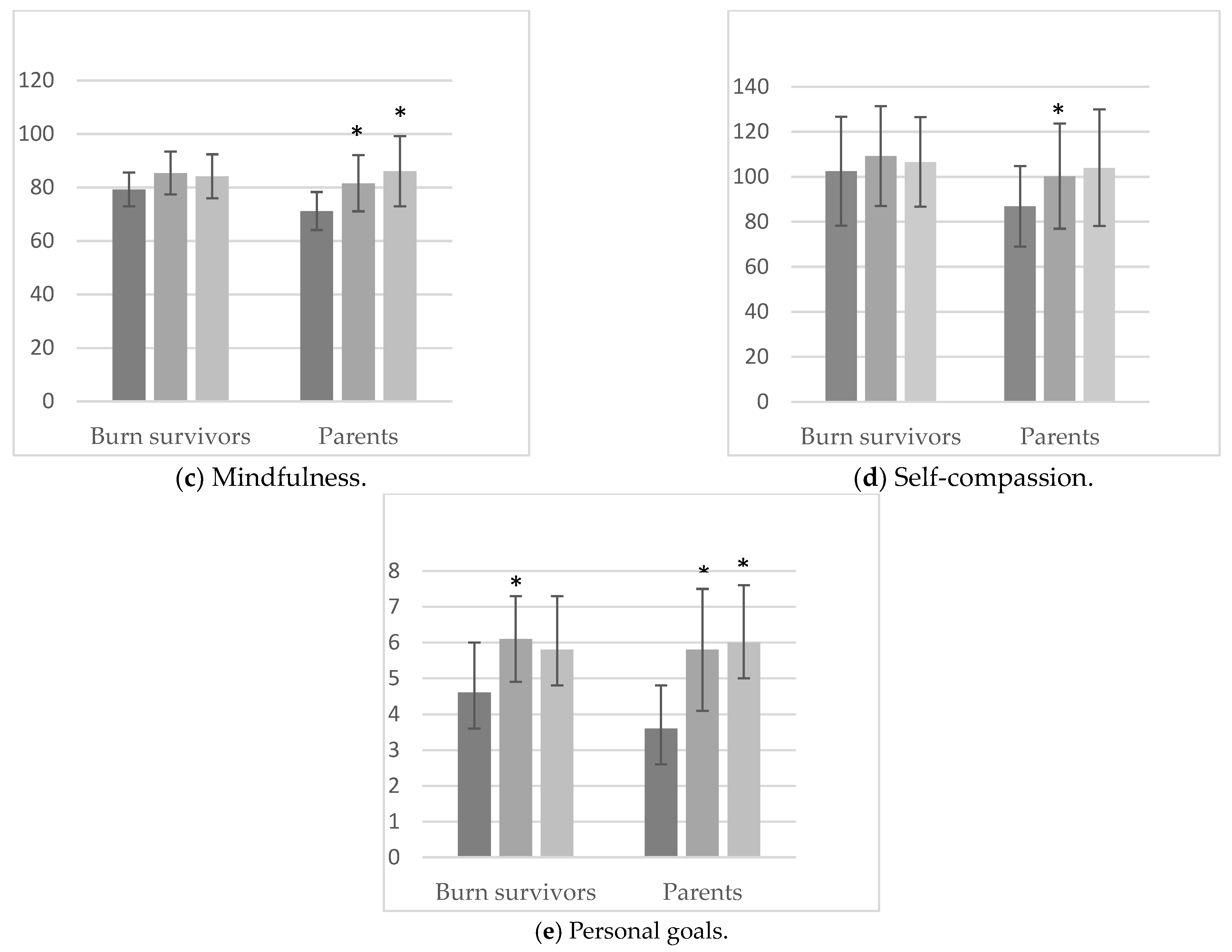
3.3.2. Mindfulness Skills and Self Compassion
“My thought process has changed (i.e., after participating in mindfulness intervention). I now think before I explode when something is bothering me or when I am arguing with someone.”
“I am much more aware of my thoughts and breathing. I still have a lot of practice to do but I’m getting better and better. [I am able] To stay with myself and to set my own boundaries.”
“I have learned to take a better look at myself, my emotions and complaints.”
“It has brought me inner peace. As a result, I can concentrate better on what I need to do. I am able to handle my emotions better.”
“I better understand what I think and feel. I have become much more aware of that. This gives me a lot of peace and growing confidence in myself.”
“I am much more aware of all sorts of feelings either positive or negative about what is going on in my family and work life right now and the physical reactions to it.”
“I have learned thoughts are just spins of the brain that run wild with you. This gave me peace of mind. I see that they are just thoughts.”
“I have better learned how to deal with stress, with compassion, and understanding for myself. More patience and love for the little one. More inner peace and a better relationship with my partner.”
“I have learned to cherish my feelings of guilt and let them go.”
3.3.3. Personal Goals
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chokshi, S.N.; Powell, C.M.; Gavrilova, Y.; Wolf, S.E.; Ozhathil, D.K. A Narrative Review of the History of Burn-Related Depression and Stress Reactions. Medicina 2022, 58, 1395. [Google Scholar] [CrossRef]
- Lerman, S.F.; Owens, M.A.; Liu, T.; Puthumana, J.; Hultman, C.S.; Caffrey, J.A.; Smith, M.T. Sleep after burn injuries: A systematic review and meta-analysis. Sleep Med. Rev. 2022, 65, 101662. [Google Scholar] [CrossRef] [PubMed]
- Moi, A.L.; Gjengedal, E. The lived experience of relationships after major burn injury. J. Clin. Nurs. 2014, 23, 2323–2331. [Google Scholar] [CrossRef] [PubMed]
- Van Loey, N.E.E.; de Jong, A.E.E.; Hofland, H.W.C.; van Laarhoven, A.I.M. Role of burn severity and posttraumatic stress symptoms in the co-occurrence of itch and neuropathic pain after burns: A longitudinal study. Front. Med. 2022, 9, 997183. [Google Scholar] [CrossRef] [PubMed]
- Wiechman, S.; Saxe, G.; Fauerbach, J.A. Psychological Outcomes Following Burn Injuries. J. Burn. Care Res. 2017, 38, e629–e631. [Google Scholar] [CrossRef] [PubMed]
- Wiechman, S.A.; McMullen, K.; Carrougher, G.J.; Fauerbach, J.A.; Ryan, C.M.; Herndon, D.N.; Holavanahalli, R.; Gibran, N.S.; Roaten, K. Reasons for Distress Among Burn Survivors at 6, 12, and 24 Months Postdischarge: A Burn Injury Model System Investigation. Arch. Phys. Med. Rehabil. 2018, 99, 1311–1317. [Google Scholar] [CrossRef] [PubMed]
- Spronk, I.; Polinder, S.; van Loey, N.E.; van der Vlies, C.H.; Pijpe, A.; Haagsma, J.A.; van Baar, M.E. Health related quality of life 5–7 years after minor and severe burn injuries: A multicentre cross-sectional study. Burns 2019, 45, 1291–1299. [Google Scholar] [CrossRef]
- Ohrtman, E.A.; Shapiro, G.D.; Simko, L.C.; Dore, E.; Slavin, M.D.; Saret, C.; Amaya, F.; Lomelin-Gascon, J.; Ni, P.; Acton, A.; et al. Social Interactions and Social Activities After Burn Injury: A Life Impact Burn Recovery Evaluation (LIBRE) Study. J. Burn. Care Res. 2018, 39, 1022–1028. [Google Scholar] [CrossRef]
- Bakker, A.; Maertens, K.J.; Van Son, M.J.; Van Loey, N.E. Psychological consequences of pediatric burns from a child and family perspective: A review of the empirical literature. Clin. Psychol. Rev. 2013, 33, 361–371. [Google Scholar] [CrossRef]
- Bakker, A.; Van Loey, N.E.E.; Van Son, M.J.M.; Van der Heijden, P.G.M. Brief Report: Mothers’ Long-term Posttraumatic Stress Symptoms Following a Burn Event of Their Child. J. Pediatr. Psychol. 2010, 35, 656–661. [Google Scholar] [CrossRef]
- Egberts, M.R.; Engelhard, I.M.; van de Schoot, R.; Bakker, A.; Geenen, R.; van der Heijden, P.G.; Van Loey, N.E. Mothers’ emotions after pediatric burn injury: Longitudinal associations with posttraumatic stress and depressive symptoms 18 months postburn. J. Affect. Disord. 2020, 263, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, L.; Centifanti, L.; Holman, N.; Taylor, P. Parental Adjustment following Pediatric Burn Injury: The Role of Guilt, Shame, and Self-Compassion. J. Pediatr. Psychol. 2019, 44, 229–237. [Google Scholar] [CrossRef]
- Kornhaber, R.; Childs, C.; Cleary, M. Experiences of guilt, shame and blame in those affected by burns: A qualitative systematic review. Burns 2018, 44, 1026–1039. [Google Scholar] [CrossRef] [PubMed]
- Tengvall, O.; Wickman, M.; Wengström, Y. Memories of Pain After Burn Injury—The Patient’s Experience. J. Burn. Care Res. 2010, 31, 319–327. [Google Scholar] [CrossRef]
- Ostrowski, S.A.; Ciesla, J.A.; Lee, T.J.; Irish, L.; Christopher, N.C.; Delahanty, D.L. The Impact of Caregiver Distress on the Longitudinal Development of Child Acute Post-Traumatic Stress Disorder Symptoms in Pediatric Injury Victims. J. Pediatr. Psychol. 2011, 36, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Gunlicks, M.L.; Weissman, M.M. Change in Child Psychopathology with Improvement in Parental Depression: A Systematic Review. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 379–389. [Google Scholar] [CrossRef]
- Bond, S.; Gourlay, C.; Desjardins, A.; Bodson-Clermont, P.; Boucher, M. Anxiety, depression and PTSD-related symptoms in spouses and close relatives of burn survivors: When the supporter needs to be supported. Burns 2017, 43, 592–601. [Google Scholar] [CrossRef]
- Boersma-van Dam, E.; van de Schoot, R.; Geenen, R.; Engelhard, I.M.; Van Loey, N.E. Prevalence and course of posttraumatic stress disorder symptoms in partners of burn survivors. Eur. J. Psychotraumatology 2021, 12, 1909282. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Gómez, A.F. Mindfulness-Based Interventions for Anxiety and Depression. Psychiatr. Clin. N. Am. 2017, 40, 739–749. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based stress reduction. In Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Dell Publishing: New York, NY, USA, 1990; p. 467. [Google Scholar]
- Querstret, D.; Cropley, M.; Fife-Schaw, C. The Effects of an Online Mindfulness Intervention on Perceived Stress, Depression and Anxiety in a Non-clinical Sample: A Randomised Waitlist Control Trial. Mindfulness 2018, 9, 1825–1836. [Google Scholar] [CrossRef]
- Khoury, B.; Sharma, M.; Rush, S.E.; Fournier, C. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J. Psychosom. Res. 2015, 78, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Hilton, L.; Hempel, S.; Ewing, B.A.; Apaydin, E.; Xenakis, L.; Newberry, S.; Colaiaco, B.; Maher, A.R.; Shanman, R.M.; Sorbero, M.E.; et al. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. Ann. Behav. Med. 2017, 51, 199–213. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Zelinski, E.; Toivonen, K.; Flynn, M.; Qureshi, M.; Piedalue, K.-A.; Grant, R. Mind-Body Therapies in Cancer: What Is the Latest Evidence? Curr. Oncol. Rep. 2017, 19, 67. [Google Scholar] [CrossRef]
- Shepherd, L.; Reynolds, D.P.; Turner, A.; O’boyle, C.P.; Thompson, A.R. The role of psychological flexibility in appearance anxiety in people who have experienced a visible burn injury. Burns 2019, 45, 942–949. [Google Scholar] [CrossRef]
- Al-Ghabeesh, S.H. Coping strategies, social support, and mindfulness improve the psychological well-being of Jordanian burn survivors: A descriptive correlational study. Burns 2022, 48, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghabeesh, S.H.; Mahmoud, M.M. Mindfulness and its Positive Effect on Quality of Life among Chronic Burn Survivors: A descriptive Correlational Study. Burns 2022, 48, 1130–1138. [Google Scholar] [CrossRef]
- Cuijpers, P.; Cristea, I.A.; Karyotaki, E.; Reijnders, M.; Huibers, M.J. How effective are cognitive behavior therapies for major depression and anxiety disorders? A meta-analytic update of the evidence. World Psychiatry 2016, 15, 245–258. [Google Scholar] [CrossRef]
- Schellekens, M.P.J.; Jansen, E.T.M.; Willemse, H.; Van Laarhoven, H.W.M.; Prins, J.B.; Speckens, A.E.M. A qualitative study on mindfulness-based stress reduction for breast cancer patients: How women experience participating with fellow patients. Support. Care Cancer 2016, 24, 1813–1820. [Google Scholar] [CrossRef]
- Jones, B.A.; Buchanan, H.; Harcourt, D. The experiences of older adults living with an appearance altering burn injury: An exploratory qualitative study. J. Health Psychol. 2017, 22, 364–374. [Google Scholar] [CrossRef]
- Kool, M.B.; Geenen, R.; Egberts, M.R.; Wanders, H.; Van Loey, N.E. Patients’ perspectives on quality of life after burn. Burns 2017, 43, 747–756. [Google Scholar] [CrossRef]
- Kornhaber, R.; Wilson, A.; Abu-Qamar, M.Z.; McLean, L. Adult burn survivors’ personal experiences of rehabilitation: An integrative review. Burns 2014, 40, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Neff, K.D.; Germer, C.K. A Pilot Study and Randomized Controlled Trial of the Mindful Self-Compassion Program. J. Clin. Psychol. 2013, 69, 28–44. [Google Scholar] [CrossRef]
- Cusens, B.; Duggan, G.B.; Thorne, K.; Burch, V. Evaluation of the breathworks mindfulness-based pain management programme: Effects on well-being and multiple measures of mindfulness. Clin. Psychol. Psychother. 2010, 17, 63–78. [Google Scholar] [CrossRef] [PubMed]
- Boeschoten, M.A.; Bakker, A.; Jongedijk, R.A.; Olff, M. PTSD Checklist for DSM-5 and Life Events Checklist for DSM-5 with Extended A Criterion–Nederlandstalige versie. Arq Psychotrauma Expert Groep: Diemen. 2014. Available online: https://www.ptsd.va.gov/professional/assessment/documents/PCL-5_LEC_criterionA.pdf (accessed on 15 November 2022).
- Beck, A.T.; Steer, R.A.; Brown, G.K. Handleiding bij de Nederlandse Versie van Beck Depression Inventory-Second Edition (BDI-II-NL) [Manual for the Dutch Version of the Beck Depression Inventory-Second Edition (BDI-II-NL)] (A. J. Van der Does, Trans.); Harcourt: Amsterdam, The Netherlands, 2002. [Google Scholar]
- Bohlmeijer, E.T.; Klooster, P.T.; Fledderus, M.; Veehof, M.; Baer, R. Psychometric Properties of the Five Facet Mindfulness Questionnaire in Depressed Adults and Development of a Short Form. Assessment 2011, 18, 308–320. [Google Scholar] [CrossRef] [PubMed]
- Veehof, M.M.; Klooster, P.M.T.; Taal, E.; Westerhof, G.J.; Bohlmeijer, E.T. Psychometric properties of the Dutch Five Facet Mindfulness Questionnaire (FFMQ) in patients with fibromyalgia. Clin. Rheumatol. 2011, 30, 1045–1054. [Google Scholar] [CrossRef] [PubMed]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and factorial validation of a short form of the Self-Compassion Scale. Clin. Psychol. Psychother. 2011, 18, 250–255. [Google Scholar] [CrossRef]
- Wu, H.; Li, F.; Zhang, F. The efficacy of mindfulness-based stress reduction vs. standard or usual care in patients with breast cancer: A systematic review and meta-analysis of randomized controlled trials. Transl. Cancer Res. 2022, 11, 4148–4158. [Google Scholar] [CrossRef]
- Papamikrouli, E.; Van Schie, C.M.H.; Schoenmaker, J.; Berge, A.B.-V.; Gebhardt, W.A. Peer Support Needs Among Adults with Burns. J. Burn. Care Res. 2017, 38, 112–120. [Google Scholar] [CrossRef]
- Minor, H.G.; Carlson, L.E.; MacKenzie, M.J.; Zernicke, K.; Jones, L. Evaluation of a Mindfulness-Based Stress Reduction (MBSR) Program for Caregivers of Children with Chronic Conditions. Soc. Work. Health Care 2006, 43, 91–109. [Google Scholar] [CrossRef]
- Mackenzie, M.J.; Carlson, L.E.; Munoz, M.; Speca, M. A qualitative study of self-perceived effects of mindfulness-based stress reduction (MBSR) in a psychosocial oncology setting. Stress Health: J. Int. Soc. Investig. Stress. 2007, 23, 59–69. [Google Scholar] [CrossRef]
- van Aalderen, J.R.; Breukers, W.J.; Reuzel, R.P.B.; Speckens, A. The Role of the Teacher in Mindfulness-Based Approaches: A Qualitative Study. Mindfulness 2014, 5, 170–178. [Google Scholar] [CrossRef]
- Egberts, M.R.; Engelhard, I.M.; de Jong, A.E.E.; Hofland, H.W.C.; Geenen, R.; Van Loey, N.E.E. Parents’ memories and appraisals after paediatric burn injury: A qualitative study. Eur. J. Psychotraumatol. 2019, 10, 1615346. [Google Scholar] [CrossRef] [PubMed]
- Lernevall, L.S.T.; Moi, A.L.; Gjengedal, E.; Dreyer, P. Parents’ lived experiences of parental needs for support at a burn centre. Int. J. Qual. Stud. Health Well-being 2021, 16, 1855749. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Session Theme | Mindfulness Practices/Exercises |
|---|---|
| 1. The automatic pilot | Raisin exercise and the body scan |
| 2. Attending and basic position | Attending versus interpreting, body scan and sitting meditation (breathing) |
| 3. Boundaries and attending to the present | Meditation, seeing and hearing exercise, stretch out yoga |
| 4. Stress and stress reactions | Sitting meditation, yoga and seeing-acting exercise |
| 5. Coping with stress | Sitting and walking meditation (cognitions and feelings) and stress patterns |
| 6. Cognitions are not facts | Sitting meditation and recognizing negative cognitions |
| 7. Taking care of one’s self: Awareness for action | Sitting meditation, energy devourers, relapse prevention |
| 8. Coping with stress and depressive moods in the future | Body scan, action plans, evaluation, and closing meditation |
| Characteristics | Burn Survivors 1 (n = 8) | Parents (n = 9) |
|---|---|---|
| Age, mean (SD) | 49.4 (16.7) | 52.2 (10.0) |
| Gender, female, n (%) | 7 (88%) | 6 (67%) |
| Education level, n (%) Primary Secondary Tertiary | 0 (0%) 4 (50%) 4 (50%) | 0 (0%) 6 (67%) 3 (33%) |
| Marital status, n (%) Single Married/partnered Divorced | 1 (13%) 5 (62%) 2 (25%) | 0 (0%) 9 (100%) 0 (0%) |
| Work status, n (%) Employed full-time Employed part-time Self-employed Retired Worker’s Compensation Act/Benefit | 0 (0%) 5 (63%) 0 (0%) 2 (25%) 1 (12%) | 1 (11%) 5 (56%) 2 (22%) 1 (11%) 0 (0%) |
| Years post-burn, Mdn (IQR) | 16 (7-22) | 5 (3–13) |
| TBSA burned, Mdn (IQR) | 29 (9–52) | 20 (6–63) |
| Face burned, n (%) | 3 (38%) | 6 (67%) |
| Genitalia burned, n (%) | 1 (12%) | 2 (22%) |
| Items | Burn Survivors Mean (SD) | Parents Mean (SD) |
|---|---|---|
| How useful did you find the intervention? | 8.9 (1.5) | 8.9 (0.9) |
| How satisfied are you with the intervention? | 8.8 (1.2) | 8.9 (0.9) |
| How confident are you that the intervention will help you cope better with the consequences of the burns? | 8.4 (1.4) | 8.6 (0.7) |
| How confident are you that the effects of the intervention will last more than 6 months? | 7.6 (1.8) | 8.7 (1.6) |
| Would you recommend the intervention to another person with burns or a parents of a child with burns? | 9.3 (1.4) | 9.4 (1.1) |
| Not Pleasant | Neutral | Pleasant | ||||
|---|---|---|---|---|---|---|
| Items | Burn survivors n (%) | Parents n (%) | Burn survivors n (%) | Parents n (%) | Burn survivors n (%) | Parents n (%) |
| Listening to experiences of other participants | 0 | 0 | 1 (12.5%) | 0 | 7 (87.5%) | 9 (100%) |
| Doing the training with peers | 0 | 0 | 0 | 0 | 8 (100%) | 9 (100%) |
| Meditation exercises | 0 | 0 | 1 (12.5%) | 1 (11%) | 7 (87%) | 8 (89%) |
| Yoga exercises | 0 | 3 (33%) | 3 (37.5%) | 1 (11%) | 5 (62.5%) | 5 (56%) |
| Breathing exercises | 0 | 0 | 1 (12.5%) | 1 (11%) | 7 (87.5%) | 8 (89%) |
| Completing homework assignments | 1 (12.5%) | 0 | 6 (75%) | 5 (56%) | 1 (12.5%) | 4 (44%) |
| Feelings and cognitions that arose as a result of practicing mindfulness | 1 (12.5%) | 1 (11%) | 2 (25%) | 1 (11%) | 5 (62.5%) | (78%) |
| Contact with participants of the other mindfulness group (training day) | 0 | 0 | 3 (37.5%) | 1 (11%) | 5 (62.5%) | 8 (89%) |
| Burn Survivors | Parents | |||||
|---|---|---|---|---|---|---|
| Subscales | Pre-Intervention Test M (SD) | Post-Intervention Test M (SD) | Follow-Up Test M (SD) | Pre-Intervention Test M (SD) | Post-Intervention Test M (SD) | Follow-Up Test M (SD) |
| Mindfulness | ||||||
| Describing Effect size (d) | 18.9 (2.2) | 17.3 (3.1) 0.80 | 18.8 (4.7) 0.03 | 13.8 (2.9) | 16.1 * (2.5) 1.50 | 16.9 * (4.9) 0.90 |
| Awareness Effect size (d) | 14.8 (3.5) | 17.9 (2.3) 0.77 | 16.3 (2.8) 0.47 | 14.0 (4.7) | 16.9 (4.8) 0.63 | 18.2 * (3.7) 1.06 |
| Non-judgmental Inner experience Effect size (d) | 16.0 (1.7) | 17.6 (3.3) 0.47 | 16.8 (3.0) 0.24 | 17.5 (3.2) | 16.3 (2.8) 0.27 | 16.9 (2.5) 0.18 |
| Non-reactivity Effect size (d) | 15.2 (2.9) | 16.9 (2.9) 0.38 | 15.5 (2.5) 0.11 | 12.2 (2.5) | 14.9 (3.0) 0.66 | 16.4 (4.9) 0.75 |
| Self-compassion | ||||||
| Self- kindness Effect size (d) | 17.0 (4.7) | 17.5 (5.0) 0.11 | 19.0 (5.2) 0.30 | 13.5 (4.9) | 18.1 * (4.8) 1.37 | 18.0 (6.4) 0.57 |
| Self-judgement Effect size (d) | 17.4 (4.8) | 18.8 (6.1) 0.21 | 18.1 (6.6) 0.13 | 15.0 (5.5) | 16.1 (4.7) 0.33 | 18.9 *(6.3) 1.00 |
| Common humanity Effect size (d) | 15.1 (4.5) | 14.8 (6.6) 0.06 | 13.9 (5.1) 0.27 | 13.3 (4.7) | 19.1 *(4.5) 1.15 | 14.3 (3.5) 0.26 |
| Isolation Effect size (d) | 20.0 (5.2) | 22.0 (4.3) 0.47 | 21.1 (5.1) 0.19 | 16.7 (4.5) | 16.0 (4.3) 0.15 | 18.2 (5.9) 0.25 |
| Mindfulness Effect size (d) | 17.9 (5.8) | 19.4 (4.1) 0.23 | 18.4 (4.9) 0.14 | 13.9 (3.7) | 18.7 * (4.6) 1.26 | 18.2 * (5.0) 0.80 |
| Over-identification Effect size (d) | 18.6 (6.1) | 21.5 (4.3) 0.45 | 20.3 (5.2) 0.28 | 17.4 (5.8) | 16.8 (5.9) 0.14 | 20.3 * (5.7) 0.73 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papamikrouli, E.; Kool, M.B.; van Schie, C.; Van Loey, N.E.E. Feasibility of Mindfulness for Burn Survivors and Parents of Children with Burns. Eur. Burn J. 2023, 4, 221-233. https://doi.org/10.3390/ebj4020020
Papamikrouli E, Kool MB, van Schie C, Van Loey NEE. Feasibility of Mindfulness for Burn Survivors and Parents of Children with Burns. European Burn Journal. 2023; 4(2):221-233. https://doi.org/10.3390/ebj4020020
Chicago/Turabian StylePapamikrouli, Eleni, Marianne B. Kool, Carine van Schie, and Nancy E. E. Van Loey. 2023. "Feasibility of Mindfulness for Burn Survivors and Parents of Children with Burns" European Burn Journal 4, no. 2: 221-233. https://doi.org/10.3390/ebj4020020
APA StylePapamikrouli, E., Kool, M. B., van Schie, C., & Van Loey, N. E. E. (2023). Feasibility of Mindfulness for Burn Survivors and Parents of Children with Burns. European Burn Journal, 4(2), 221-233. https://doi.org/10.3390/ebj4020020