
The Use of Intact Fish Skin as a Novel Treatment Method for Deep Dermal Burns Following Enzymatic Debridement: A Retrospective Case-Control Study

Abstract
:1. Background
2. Methods
2.1. Selection of Subjects
2.2. Objective and Subjective Wound-Quality Assessment
2.3. Wound-Size Measurement
2.4. Statistical Analysis
3. Results
3.1. Patient Data
3.2. Application of Fish Skin Graft Reduced Time to Complete Healing Compared to Both Suprathel and STSGs
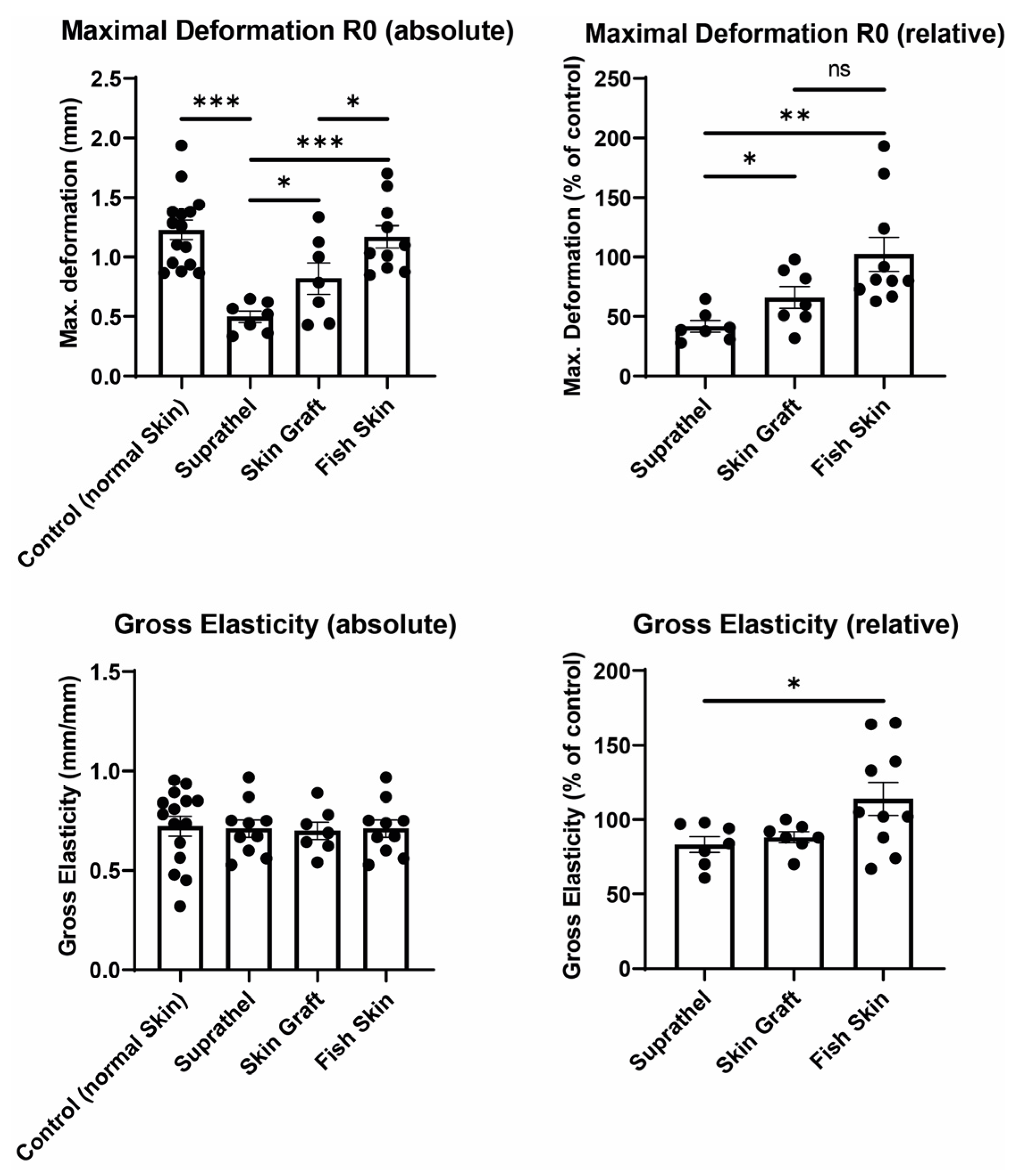
3.3. Fish Skin Graft and STSG Resulted in Significantly Superior Elasticity in Regenerated Skin Compared to Suprathel
3.4. Fish Skin Graft Was Superior to Suprathel for Regenerated Skin’s Sebum Content and Resulted in Significantly Higher Water Content Than Both Suprathel and STSG
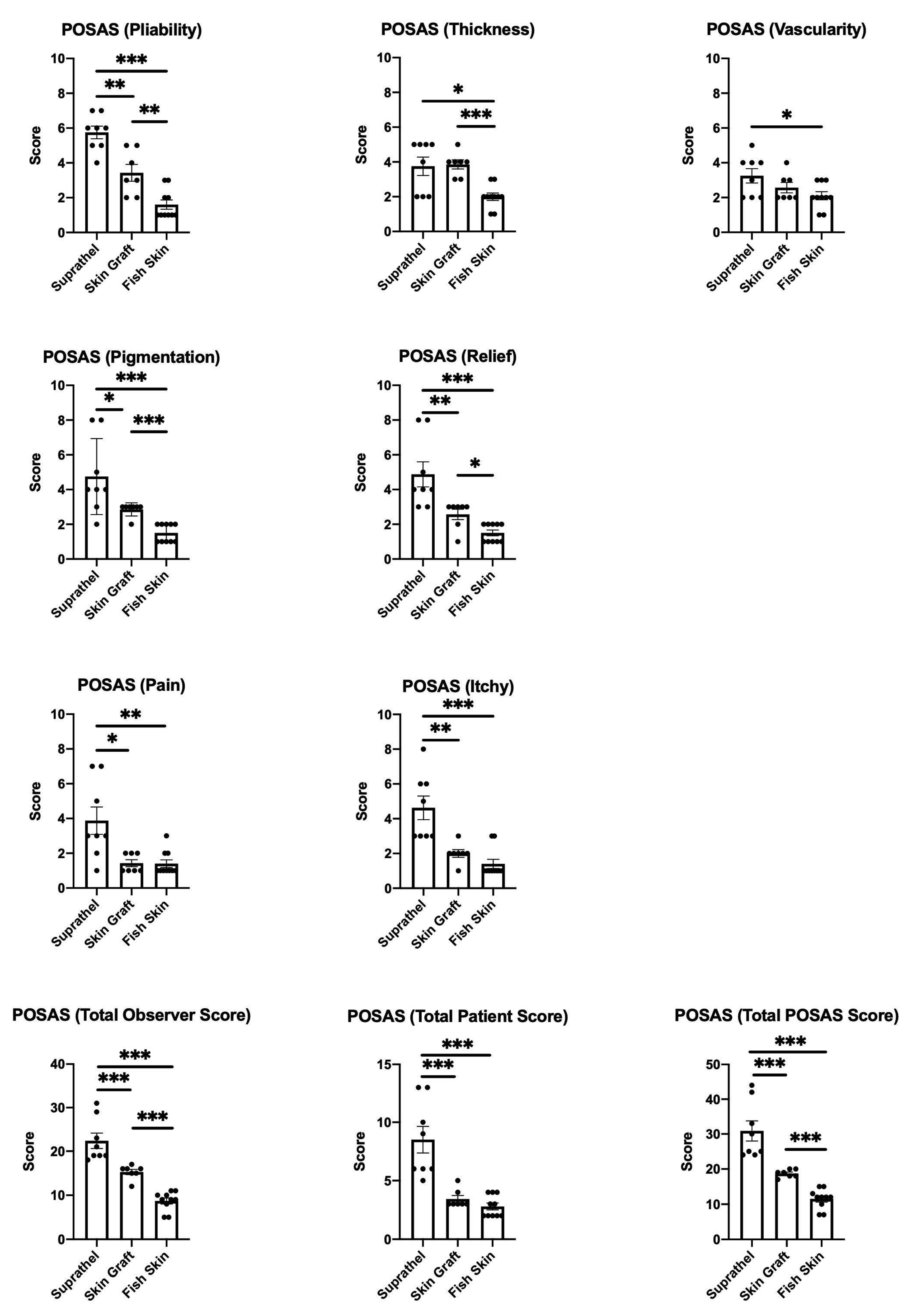
3.5. Fish Skin Graft Achieved Better Scar Quality Regarding Pliability, Thickness, Vascularity, Pigmentation, and Relief Categories as Well as Superior Alleviation of Pain and Itch Compared to Both Suprathel and STSGs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, K.C.; Joory, K.; Moiemen, N.S. History of burns: The past, present and the future. Burn. Trauma 2014, 2, 2321–3868. [Google Scholar]
- Wallner, C.; Wagner, J.M.; Dittfeld, S.; Drysch, M.; Lehnhardt, M.; Behr, B. Myostatin serum concentration as an indicator for deviated muscle metabolism in severe burn injuries. Scand. J. Surg. 2018, 108, 297–304. [Google Scholar] [CrossRef]
- Wallner, C.; Huber, J.; Drysch, M.; Schmidt, S.V.; Wagner, J.M.; Dadras, M.; Lehnhardt, M.; Behr, B. Myostatin Upregulation in Patients in the Chronic Phase of Severe Burn Injury Leads to Muscle Cell Catabolism. Eur. Surg. Res. 2019, 60, 86–96. [Google Scholar] [CrossRef]
- Alam, K.; Jeffery, S.L. Acellular Fish Skin Grafts for Management of Split Thickness Donor Sites and Partial Thickness Burns: A Case Series. Mil. Med. 2019, 184, 16–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puri, V.; Khare, N.A.; Chandramouli, M.; Shende, N.; Bharadwaj, S. Comparative Analysis of Early Excision and Grafting vs. Delayed Grafting in Burn Patients in a Developing Country. J. Burn Care Res. 2016, 37, 278–282. [Google Scholar] [CrossRef] [Green Version]
- Galeiras, R.; Mourelo, M.; Pértega, S.; López, M.; Esmorís, I. Procedural sedation and analgesia during enzymatic debridement of burn patients. Ann. Burn. Fire Disasters 2018, 31, 223–227. [Google Scholar]
- Rosenberg, L.; Krieger, Y.; Silberstein, E.; Arnon, O.; Sinelnikov, I.A.; Bogdanov-Berezovsky, A.; Singer, A.J. Selectivity of a bromelain based enzymatic debridement agent: A porcine study. Burns 2012, 38, 1035–1040. [Google Scholar] [CrossRef] [PubMed]
- Hirche, C.; Almeland, S.K.; Dheansa, B.; Fuchs, P.; Governa, M.; Hoeksema, H.; Korzeniowski, T.; Lumenta, D.B.; Marinescu, S.; Martinez-Mendez, J.R.; et al. Eschar removal by bromelain based enzymatic debridement (Nexobrid®) in burns: European consensus guidelines update. Burns 2020, 46, 782–796. [Google Scholar] [CrossRef] [PubMed]
- Di Lonardo, A.; Nardini, V.; De Rosa, M.; Pascone, C.; Graziano, A.; Criscuoli, A.M.; Ciappi, S. Enzymatic escharolysis with nexobrid® on partial thickness burn wounds: Pre- and post-debridement histological assessment. Ann. Burn. Fire Disasters 2018, 31, 23–27. [Google Scholar]
- Rosenberg, L.; Krieger, Y.; Bogdanov-Berezovski, A.; Silberstein, E.; Shoham, Y.; Singer, A.J. A novel rapid and selective enzymatic debridement agent for burn wound management: A multi-center RCT. Burns 2014, 40, 466–474. [Google Scholar] [CrossRef]
- Dadras, M.; Wagner, J.M.; Wallner, C.; Sogorski, A.; Sacher, M.; Harati, K.; Lehnhardt, M.; Behr, B. Enzymatic debridement of hands with deep burns: A single center experience in the treatment of 52 hands. J. Plast. Surg. Hand Surg. 2020, 54, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Singer, A.J.; McClain, S.A.; Taira, B.R.; Rooney, J.; Steinhauff, N.; Rosenberg, L. Rapid and Selective Enzymatic Debridement of Porcine Comb Burns with Bromelain-Derived Debrase®: Acute-Phase Preservation of Noninjured Tissue and Zone of Stasis. J. Burn Care Res. 2010, 31, 304–309. [Google Scholar] [CrossRef]
- Behr, B.; Megerle, K.O.; Germann, G.; Kloeters, O. Neue Konzepte in der Oberflächentherapie bei Verbrennungswunden. Handchir. Mikrochir. Plast. Chir. 2008, 40, 361–366. [Google Scholar] [CrossRef]
- Yan, Y.; Jiang, W.; Spinetti, T.; Tardivel, A.; Castillo, R.; Bourquin, C.; Guarda, G.; Tian, Z.; Tschopp, J.; Zhou, R. Omega-3 Fatty Acids Prevent Inflammation and Metabolic Disorder through Inhibition of NLRP3 Inflammasome Activation. Immunity 2013, 38, 1154–1163. [Google Scholar] [CrossRef] [Green Version]
- Magnusson, S.; Baldursson, B.T.; Kjartansson, H.; Thorlacius, G.E.; Axelsson, I.; Rolfsson, O.; Petersen, P.H.; Sigurjonsson, G.F. Decellularized fish skin: Characteristics that support tissue repair. Laeknabladid 2015, 101, 567–573. [Google Scholar]
- Magnusson, S.; Baldursson, B.T.; Kjartansson, H.; Rolfsson, Ó.; Sigurjonsson, G.F. Regenerative and Antibacterial Properties of Acellular Fish Skin Grafts and Human Amnion/Chorion Membrane: Implications for Tissue Preservation in Combat Casualty Care. Mil. Med. 2017, 182, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Dorweiler, B.; Trinh, T.T.; Dünschede, F.; Vahl, C.F.; Debus, E.S.; Storck, M.; Diener, H. The marine Omega3 wound matrix for treatment of complicated wounds: A multicenter experience report. Gefasschirurgie 2018, 23, 46–55. [Google Scholar] [CrossRef] [Green Version]
- Baldursson, B.T.; Kjartansson, H.; Konrádsdóttir, F.; Gudnason, P.; Sigurjonsson, G.F.; Lund, S.H. Healing rate and autoimmune safety of full-thickness wounds treated with fish skin acellular dermal matrix versus porcine small-intestine submucosa: A noninferiority study. Int. J. Low. Extrem. Wounds 2015, 14, 37–43. [Google Scholar] [CrossRef]
- Michael, S.; Winters, C.; Khan, M. Acellular Fish Skin Graft Use for Diabetic Lower Extremity Wound Healing: A Retrospective Study of 58 Ulcerations and a Literature Review. Wounds Compend. Clin. Res. Pract. 2019, 31, 262–268. [Google Scholar]
- Kirsner, R.S.; Margolis, D.J.; Baldursson, B.T.; Petursdottir, K.; Davidsson, O.B.; Weir, D.; Lantis, J.C. Fish skin grafts compared to human amnion/chorion membrane allografts: A double-blind, prospective, randomized clinical trial of acute wound healing. Wound Repair Regen. 2020, 28, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Jeschke, M.G.; Van Baar, M.E.; Choudhry, M.A.; Chung, K.K.; Gibran, N.S.; Logsetty, S. Burn injury. Nat. Rev. Dis. Prim. 2020, 6, 11. [Google Scholar] [CrossRef]
- Lee, K.C.; Dretzke, J.; Grover, L.; Logan, A.; Moiemen, N. A systematic review of objective burn scar measurements. Burn. Trauma 2016, 4, 1–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Draaijers, L.J.; Tempelman, F.R.H.; Botman, Y.A.M.; Tuinebreijer, W.E.; Middelkoop, E.; Kreis, R.W.; van Zuijlen, P. The Patient and Observer Scar Assessment Scale: A Reliable and Feasible Tool for Scar Evaluation. Plast. Reconstr. Surg. 2004, 113, 1960–1965. [Google Scholar] [CrossRef]
- Molnar, J.A.; Lew, W.K.; Rapp, D.A.; Gordon, E.S.; Voignier, D.; Rushing, S.; Willner, W. Use of Standardized, Quantitative Digital Photography in a Multicenter Web-based Study. Eplasty 2009, 9, e4. [Google Scholar]
- Ziegler, B.; Corterier, C.; Kremer, T.; Lumenta, D.B.; Plock, J.A.; Richter, S.; Sander, F.; Schiefer, J.L.; Siegwart, L.C.; Stauder, M.; et al. Implementierung der Behandlung durch enzymatisches Debridement bei Verbrennungen—Ergebnisse eines interprofessionellen, deutschsprachigen Expertenworkshops. Handchir. Mikrochir. Plast. Chir. 2020, 53, 175–184. [Google Scholar] [CrossRef]
- Siegwart, L.C.; Böcker, A.H.; Diehm, Y.F.; Kotsougiani-Fischer, D.; Erdmann, S.; Ziegler, B.; Kneser, U.; Hirche, C.; Fischer, S. Enzymatic debridement for burn wound care: Interrater reliability and impact of experience in post-intervention therapy decision. J. Burn Care Res. 2021, 42, 953–961. [Google Scholar] [CrossRef]
- AWMF. Behandlung Thermischer Verletzungen des Erwachsenen. Leitlin S2k 2018:AWMF-Register-Nr.: 044. Available online: https://www.awmf.org/uploads/tx_szleitlinien/044-001l_S2k_Behandlung-thermischer-Verletzungen-des-Erwachsenen_2021-07.pdf (accessed on 18 November 2021).
- Promny, D.; Billner, M.; Reichert, B. Objective burn depth assessment of hand burns. Handchir. Mikrochir. Plast. Chir. 2019, 51, 362–366. [Google Scholar]
- Neto, P.; Ferreira, M.; Bahia, F.; Costa, P. Improvement of the methods for skin mechanical properties evaluation through correlation between different techniques and factor analysis. Ski. Res. Technol. 2013, 19, 405–416. [Google Scholar] [CrossRef]
- Dobrev, H. Use of Cutometer to assess epidermal hydration. Ski. Res. Technol. 2000, 6, 239–244. [Google Scholar] [CrossRef]
- Ezerskaia, A.; Pereira, S.F.; Urbach, H.P.; Verhagen, R.; Varghese, B. Quantitative and simultaneous non-invasive measurement of skin hydration and sebum levels. Biomed. Opt. Express 2016, 7, 2311–2320. [Google Scholar] [CrossRef] [Green Version]
- Piérard, G.E.; Piérard-Franchimont, C.; Marks, R.; Paye, M.; Rogiers, V. EEMCO Guidance for the in vivo Assessment of Skin Greasiness. Ski. Pharmacol. Physiol. 2000, 13, 372–389. [Google Scholar] [CrossRef] [PubMed]
- Barel, A.O.; Clarys, P.; Gabard, B. In Vivo Evaluation of the Hydration State of the Skin: Measurements and Methods for Claim Support. In Cosmetics; Springer: Berlin/Heidelberg, Germany, 1999; pp. 57–80. [Google Scholar]
- Berardesca, E.; European Group for Efficacy Measurements on Cosmetics and Other Topical Products (EEMCO). EEMCO guidance for the assessment of stratum corneum hydration: Electrical methods. Ski. Res. Technol. 1997, 3, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Escoffier, C.; de Rigal, J.; Rochefort, A.; Vasselet, R.; Lévêque, J.L.; Agache, P.G. Age-Related Mechanical Properties of Human Skin: An In Vivo Study. J. Investig. Dermatol. 1989, 93, 353–357. [Google Scholar] [CrossRef]
- Agache, P.G.; Monneur, C.; Leveque, J.L.; De Rigal, J. Original Contributions Mechanical Properties and Young’s Modulus of Human Skin In Vivo. Arch. Dermatol. Res. 1980, 269, 221–232. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | TBSA (%) | Treated with Fish Skin Graft (%) | Treated with Suprathel (%) | Treated with Skin Graft (%) |
|---|---|---|---|---|
| #1 | 8 | 3 | 4 | n.a. |
| #2 | 6 | 5 | n.a. | 1 |
| #3 | 10 | 2 | 8 | 0 |
| #4 | 1 | 0.5 | n.a. | 0.5 |
| #5 | 5 | 3 | 2 | n.a. |
| #6 | 20 | 1 | 5 | 14 |
| #7 | 2 | 1 | n.a. | 1 |
| #8 | 24 | 9 | 15 | n.a. |
| #9 | 12 | 2 | 10 | n.a. |
| #10 | 15 | 6 | 7 | 2 |
| #11 * | 35 | 17 | n.a. | 18 |
| #12 * | 12 | 2 | 10 | n.a. |
| Patient | Total TBSA (%) | Treated with Fish Skin Graft (%) | Treated with Suprathel (%) | Treated with Skin Graft (%) |
| Mean TBSA (%) * | 12.5 ± 9.4 | 4.3 ± 4.5 | 7.6 ± 3.8 | 6.1 ± 7.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wallner, C.; Holtermann, J.; Drysch, M.; Schmidt, S.; Reinkemeier, F.; Wagner, J.M.; Dadras, M.; Sogorski, A.; Houschyar, K.S.; Becerikli, M.; et al. The Use of Intact Fish Skin as a Novel Treatment Method for Deep Dermal Burns Following Enzymatic Debridement: A Retrospective Case-Control Study. Eur. Burn J. 2022, 3, 43-55. https://doi.org/10.3390/ebj3010006
Wallner C, Holtermann J, Drysch M, Schmidt S, Reinkemeier F, Wagner JM, Dadras M, Sogorski A, Houschyar KS, Becerikli M, et al. The Use of Intact Fish Skin as a Novel Treatment Method for Deep Dermal Burns Following Enzymatic Debridement: A Retrospective Case-Control Study. European Burn Journal. 2022; 3(1):43-55. https://doi.org/10.3390/ebj3010006
Chicago/Turabian StyleWallner, Christoph, Jana Holtermann, Marius Drysch, Sonja Schmidt, Felix Reinkemeier, Johannes Maximilian Wagner, Mehran Dadras, Alexander Sogorski, Khosrow Siamak Houschyar, Mustafa Becerikli, and et al. 2022. "The Use of Intact Fish Skin as a Novel Treatment Method for Deep Dermal Burns Following Enzymatic Debridement: A Retrospective Case-Control Study" European Burn Journal 3, no. 1: 43-55. https://doi.org/10.3390/ebj3010006
APA StyleWallner, C., Holtermann, J., Drysch, M., Schmidt, S., Reinkemeier, F., Wagner, J. M., Dadras, M., Sogorski, A., Houschyar, K. S., Becerikli, M., Lehnhardt, M., & Behr, B. (2022). The Use of Intact Fish Skin as a Novel Treatment Method for Deep Dermal Burns Following Enzymatic Debridement: A Retrospective Case-Control Study. European Burn Journal, 3(1), 43-55. https://doi.org/10.3390/ebj3010006