
No Change in Fireworks-Related Burn Center Admissions: A 10-Year Analysis of the Admission Rates, Treatment, and Costs

 ,
, 
Abstract
1. Introduction
2. Results
2.1. Inclusions
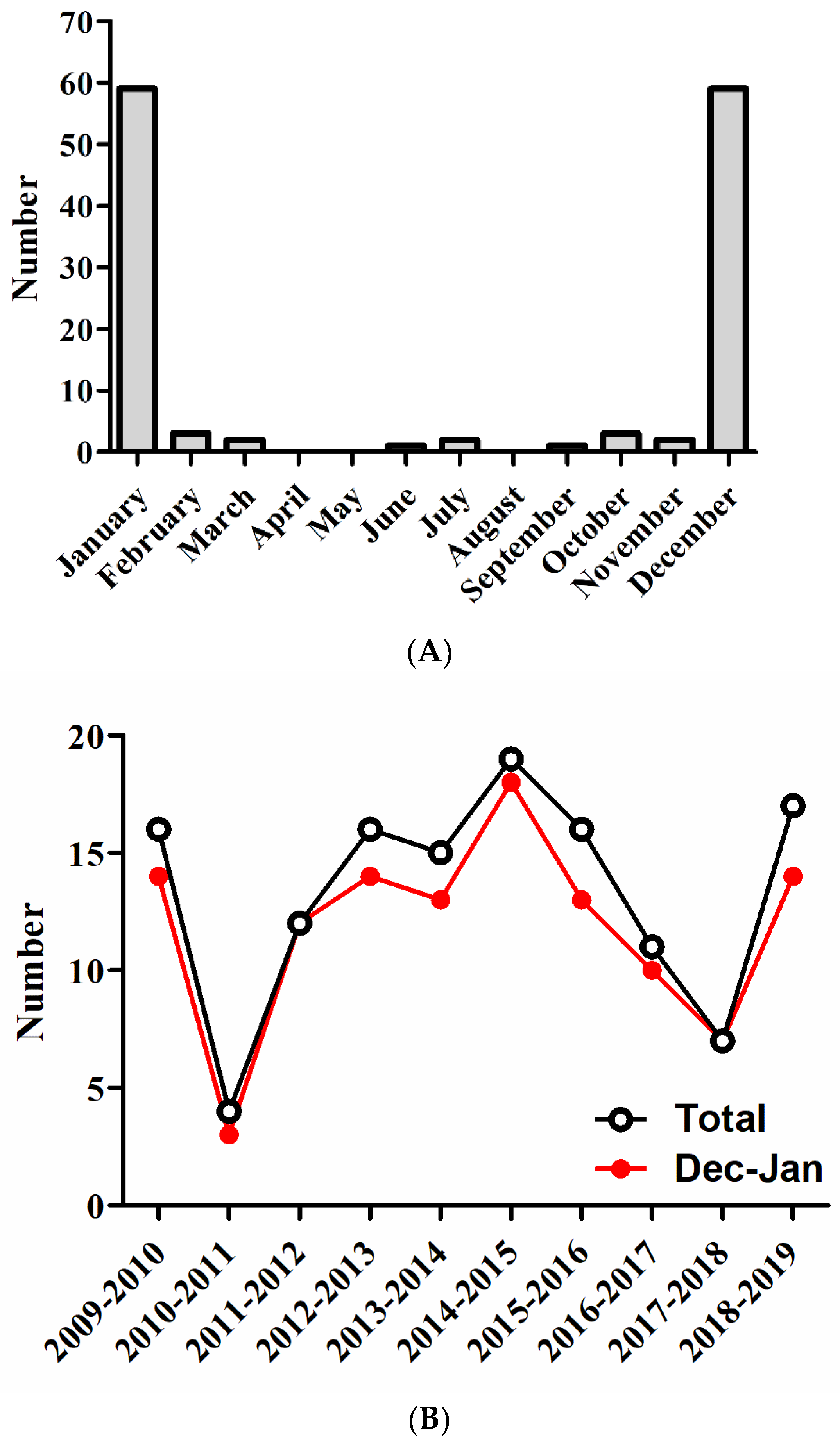
2.2. Trends in Admissions
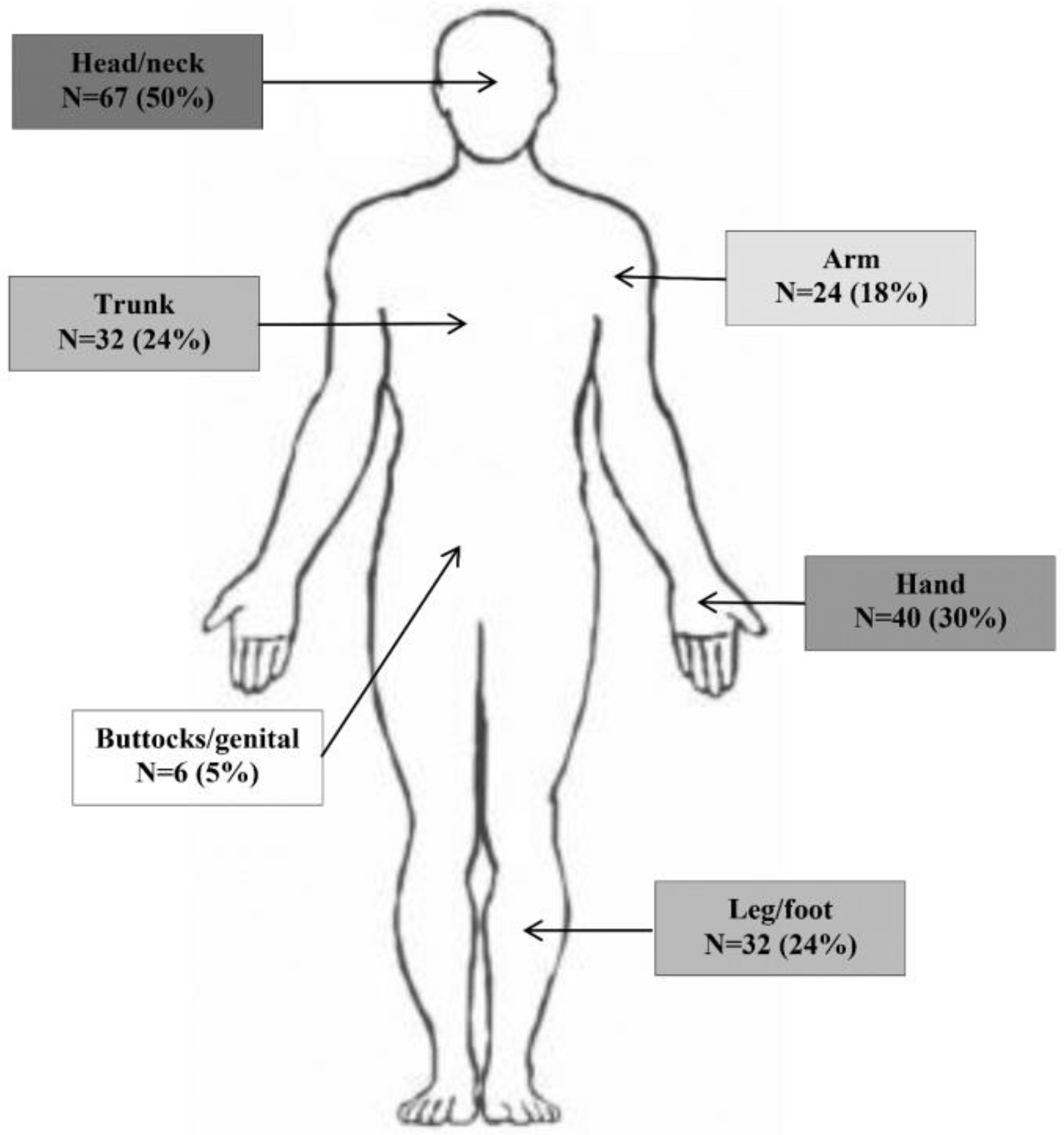
2.3. Patient and Injury Characteristics
2.4. Treatment Characteristics
2.5. Costs for Specialized Burn Care
3. Discussion
3.1. Strengths and Limitations
3.2. Materials and Methods
3.2.1. Study Design and Setting
3.2.2. Participants
3.2.3. Data Collection
3.2.4. Cost Analysis
3.2.5. Statistical Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Edwin, A.F.; Cubison, T.C.; Pape, S.A. The impact of recent legislation on paediatric fireworks injuries in the Newcastle upon Tyne region. Burns 2008, 34, 953–964. [Google Scholar] [CrossRef]
- Tavakoli, H.; Khashayar, P.; Amoli, H.A.; Esfandiari, K.; Ashegh, H.; Rezaii, J.; Salimi, J. Firework-related injuries in Tehran’s Persian Wednesday Eve Festival (Chaharshanbe Soori). J. Emerg. Med. 2011, 40, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Van Yperen, D.T.; Van Der Vlies, C.H.; De Faber, J.T.H.N.; Penders, C.J.M.; Smit, X.; Van Lieshout, E.M.M.; Verhofstad, M.H.J. Firework injuries in the south-western region of the Netherlands around the turn of the year 2017–2018. Ned. Tijdschr. Voor Geneeskd. 2018, 162, D3310. [Google Scholar]
- Puri, V.; Mahendru, S.; Rana, R.; Deshpande, M. Firework injuries: A ten-year study. J. Plast. Reconstr. Aesthet. Surg. 2009, 62, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Canner, J.K.; Haider, A.H.; Selvarajah, S.; Hui, X.; Wang, H.; Efron, D.T.; Haut, E.R.; Velopulos, C.G.; Schwartz, D.A.; Chi, A.; et al. US emergency department visits for fireworks injuries, 2006–2010. J. Surg. Res. 2014, 190, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Chaparro-Narváez, P.; Cotes-Cantillo, K.; Castañeda-Orjuela, C.; De La Hoz-Restrepo, F. Injuries due to fireworks use: A surveillance data analysis in Colombia, 2008–2013. Burns 2017, 43, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.X.; McGwin, G., Jr.; Griffin, R.L. The epidemiology of firework-related injuries in the United States: 2000–2010. Injury 2014, 45, 1704–1709. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Zhao, R.; Du, W.L.; Ning, F.G.; Zhang, G.A. Firework injuries at a major trauma and burn center: A five-year prospective study. Burns 2014, 40, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Bagri, N.; Saha, A.; Chandelia, S.; Dubey, N.K.; Bhatt, A.; Rai, A.; Bhattacharya, S.; Makhija, L.K. Fireworks injuries in children: A prospective study during the festival of lights. Emerg. Med. Australas. 2013, 25, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Sandvall, B.K.; Jacobson, L.; Miller, E.A.; Dodge, R.E., 3rd; Alex Quistberg, D.; Rowhani-Rahbar, A.; Vavilala, M.S.; Friedrich, J.B.; Keys, K.A. Fireworks type, injury pattern, and permanent impairment following severe fireworks-related injuries. Am. J. Emerg. Med. 2017, 35, 1469–1473. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.; Ng, J. Fireworks-Related Deaths, Emergency Department-Treated Injuries, and Enforcement Activities During 2018; Consumer Product Safety Commission: Washington, DC, USA, 2019.
- Valkenberg, H.; Nijman, S. Ongevallen Met Vuurwerk—Jaarwisseling 2018–2019; VeiligheidNL: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Joustra, T.H.J.; Muller, E.R.; Van Asselt, M.B.A.; Verheij, C.A.J.F. Safety Hazards of the Annual Change of Year; Dutch Safety Board: Den Haag, The Netherlands, 2017.
- Hop, M.J.; Wijnen, B.F.; Nieuwenhuis, M.K.; Dokter, J.; Middelkoop, E.; Polinder, S.; van Baar, M.E. Economic burden of burn injuries in the Netherlands: A 3 months follow-up study. Injury 2016, 47, 203–210. [Google Scholar] [CrossRef]
- Nizamoglu, M.; Frew, Q.; Tan, A.; Band, H.; Band, B.; Barnes, D.; El-Muttardi, N.; Dziewulski, P. The ten-year experience of firework injuries treated at a uk regional burns & plastic surgery unit. Ann. Burn. Fire Disasters 2018, 31, 13–16. [Google Scholar]
- Valkenberg, H.; Nijman, S. Ongevallen Met Vuurwerk—Jaarwisseling 2019–2020; VeiligheidNL: Amsterdam, The Netherlands, 2020. [Google Scholar]
- De Faber, J.T.; Kivela, T.T.; Gabel-Pfisterer, A. National studies from the Netherlands and Finland and the impact of regula-tions on incidences of fireworks-related eye injuries. Ophthalmologe 2020, 117, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.; Wang, L.; Xie, W.; Shen, C.; Guo, G.; Liu, J.; Han, C.; Ren, L.; Liang, Y.; Liu, J.; et al. Epidemiology and outcome analysis of facial burns: A retrospec-tive multicentre study 2011–2015. Burns 2020, 46, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Dokter, J.; Vloemans, A.; Beerthuizen, G.; Van Der Vlies, C.; Boxma, H.; Breederveld, R.; Tuinebreijer, W.; Middelkoop, E.; Van Baar, M. Epidemiology and trends in severe burns in the Netherlands. Burns 2014, 40, 1406–1414. [Google Scholar] [CrossRef] [PubMed]
- Frimmel, S.; De Faber, J.T.; Wubbels, R.J.; Kniestedt, C.; Paridaens, D. Type, severity, management and outcome of ocular and adnexal firework-related injuries: The Rotterdam experience. Acta Ophthalmol. 2018, 96, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Sandvall, B.K.; Keys, K.A.; Friedrich, J.B. Severe Hand Injuries From Fireworks: Injury Patterns, Outcomes, and Fireworks Types. J. Hand Surg. 2017, 42, 385.e1–385.e8. [Google Scholar] [CrossRef] [PubMed]
- Hakkaart-van Roijen, L.; Van der Linden, N.; Bouwmans, C.; Kanters, T.; Tan, S.S. Costing Manual: Methodology of Costing Research and Reference Prices for Economic Evaluations in Healthcare; In Dutch: Kostenhandleiding: Methodologie van kostenonderzoek en referentieprijzen voor economische evaluaties in de gezondheidszorg; Zorginstituut Nederland: Diemen, The Netherlands, 2016.
- Hop, M.; Langenberg, L.; Hiddingh, J.; Stekelenburg, C.; Van Der Wal, M.; Hoogewerf, C.; Van Koppen, M.; Polinder, S.; Van Zuijlen, P.; Van Baar, M.; et al. Reconstructive surgery after burns: A 10-year follow-up study. Burns 2014, 40, 1544–1551. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All (N = 133) | |
|---|---|
| Age (year) | 15 (11–25) |
| 0–4 | 5 (4) |
| 5–9 | 18 (14) |
| 10–14 | 39 (29) |
| 15–19 | 20 (15) |
| 20–29 | 27 (20) |
| 30–39 | 7 (5) |
| 40–49 | 9 (7) |
| 50–59 | 6 (5) |
| ≥60 | 2 (2) |
| Male | 103 (77) |
| TBSA (%) | 1.0 (0.5–2.5) |
| ≥15% TBSA | 2 (2) |
| Partial thickness | 100 (75) |
| Full thickness | 45 (34) |
| Additional injury | 23 (17) |
| Soft tissue damage | 11 (48) |
| Eye injury | 10 (43) |
| Fractures | 5 (22) |
| Subcutaneous emphysema | 1 (4) |
| All (N = 133) | |
|---|---|
| Length of stay (days) | 1 (0–5) |
| ICU admission needed | 13 (10) |
| Duration (days) | 2 (2–5) |
| Surgical treatment for wound closure | 66 (50) |
| Mechanical ventilation | 9 (7) |
| Type of surgery performed in acute phase | |
| Wound excision & primary closure | 12 (18) |
| Split skin graft | 54 (82) |
| Meek wall | 1 (2) |
| Full thickness graft | 1 (2) |
| Dermal substitute (Integra©) | 1 (2) |
| Vacuum Assisted Closure system | 2 (3) |
| Amputation | 2 (3) |
| Reconstructive surgery | 4 (3) |
| Day care treatment a | 47 (35) |
| Discharged home | 130 (98) |
| Re-admitted | 16 (12) |
| Patient | Age Category (Years) | TBSA on Injury (%) | Time to Reconstruction (Months) | Indication | Technique |
|---|---|---|---|---|---|
| 1 | 15–19 | 0.5 | 14 | Contractures | Release and random flap |
| 2 | 30–34 | 6.0 | 10 | Wound problems and contractures | Excision and split skin graft |
| 2 | 30–34 | 6.0 | 19 | Wound problems | Excision and primary closure |
| 3 | 15–19 | 0.5 | 5 | Webspace contracture | Excision and random flap |
| 4 | 25–29 | 40.0 | 18 | Contractures | Excision and full thickness graft |
| Cost Category | Direct Medical Costs per Patient (in €) |
|---|---|
| Transportation | 430 (290 to 580) |
| Non-ICU burn center days | 4160 (2830 to 5480) |
| ICU burn center days | 1810 (0 to 3620) |
| Day care | 150 (110 to 190) |
| Surgical treatment | 1410 (950 to 1870) |
| Reconstructive surgery | 50 (0 to 100) |
| Total costs | 8000 (5160 to 10,850) |
| Estimated extra costs * | 1040 (670 to 1410) |
| Total costs entire population | 9040 (5840 to 12,260) |
| Total costs patients treated in day care only | 975 (765 to 1185) |
| Total costs patients admitted but not operated | 5060 (3715 to 6400) |
| Total costs patients admitted and operated | 13,834 (7600 to 20,070) |
| Cost Categories | Unit | Source of Unit Prices (Cost Year) | Unit Price (in €) |
|---|---|---|---|
| Transportation | |||
| Own transport | Ride | Hop et al. 2016 (2012) | Upon request |
| Ambulance | Ride | NZa a (2018) | 702.00 |
| Mobile Intensive Care Unit | Ride | NZa a (2018) | 2321.95 |
| HEMS-assistance | Yes | Hospital data calculation (2008) | Upon request |
| Burn center stay | |||
| ICU burn center days | Days | Hop et al. 2016 (2012) | 948.12 |
| Non-ICU burn center days | Days | Hop et al. 2016 (2012) | 2965.71 |
| Day care | Days | Hop et al. 2016 (2012) | 350.80 |
| Surgery | |||
| Surgical treatment | Operation | Hop et al. 2016 (2012) | 1966.47 |
| Reconstructive surgery | Operation | Hop et al. 2014 (2011) | Upon request |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Yperen, D.T.; Van Baar, M.E.; Polinder, S.; Van Zuijlen, P.P.M.; Beerthuizen, G.I.J.M.; Lucas, Y.; Van Lieshout, E.M.M.; Verhofstad, M.H.J.; Van der Vlies, C.H.; Dutch Burn Repository Group. No Change in Fireworks-Related Burn Center Admissions: A 10-Year Analysis of the Admission Rates, Treatment, and Costs. Eur. Burn J. 2021, 2, 31-40. https://doi.org/10.3390/ebj2010003
Van Yperen DT, Van Baar ME, Polinder S, Van Zuijlen PPM, Beerthuizen GIJM, Lucas Y, Van Lieshout EMM, Verhofstad MHJ, Van der Vlies CH, Dutch Burn Repository Group. No Change in Fireworks-Related Burn Center Admissions: A 10-Year Analysis of the Admission Rates, Treatment, and Costs. European Burn Journal. 2021; 2(1):31-40. https://doi.org/10.3390/ebj2010003
Chicago/Turabian StyleVan Yperen, Daan T., Margriet E. Van Baar, Suzanne Polinder, Paul P.M. Van Zuijlen, Gerard I.J.M. Beerthuizen, Ymke Lucas, Esther M.M. Van Lieshout, Michael H.J. Verhofstad, Cornelis H. Van der Vlies, and Dutch Burn Repository Group. 2021. "No Change in Fireworks-Related Burn Center Admissions: A 10-Year Analysis of the Admission Rates, Treatment, and Costs" European Burn Journal 2, no. 1: 31-40. https://doi.org/10.3390/ebj2010003
APA StyleVan Yperen, D. T., Van Baar, M. E., Polinder, S., Van Zuijlen, P. P. M., Beerthuizen, G. I. J. M., Lucas, Y., Van Lieshout, E. M. M., Verhofstad, M. H. J., Van der Vlies, C. H., & Dutch Burn Repository Group. (2021). No Change in Fireworks-Related Burn Center Admissions: A 10-Year Analysis of the Admission Rates, Treatment, and Costs. European Burn Journal, 2(1), 31-40. https://doi.org/10.3390/ebj2010003