Abstract
Background/Objectives: Digital workflows for implant-supported full-arch restorations remain challenging. This study evaluated the accuracy and precision of digital impressions using reverse scan body (RSB) prototypes and intraoral scanners (IOSs) for rehabilitating fully edentulous patients following the All-on-4 protocol. Secondary objectives included comparing accuracy between expert clinicians and beginners, as well as desktop scanners and various RSB designs. Methods: An in vitro study was conducted using a fully edentulous mandible model with four Osstem TSIII implants. A final-year dental student and an expert clinician captured digital impressions using IOSs and desktop scanners. Four groups were analyzed: (A) original scan bodies with the IOS, (B) short RSBs with the IOS, (C) RSBs with desktop scanners (short sandblasted, long sandblasted, long coated), and (D) a control group using original scan bodies with a desktop scanner. Root mean square (RMS) values measured dimensional differences, with statistical analysis performed using the Wilcoxon signed-rank test and one-way ANOVA (α = 0.05). Results: A total of 42 scans were analyzed. No significant difference was found between expert and student for original scan bodies using the IOS (p = 0.220), while RSB prototypes showed significant differences (p = 0.008). No significant accuracy differences were noted between original scan bodies and RSBs with the IOS, but IOSs outperformed desktop scanners. Among RSBs scanned with desktop scanners, no significant differences were observed between designs. Conclusions: RSB prototypes are a viable alternative to original scan bodies for fully digital workflows in All-on-4 rehabilitations, with IOSs offering superior accuracy. However, proper training is crucial for optimizing RSB accuracy. Variations in height and coating did not impact overall accuracy.
1. Introduction
The adoption of fully digital workflows in implant dentistry is growing due to their potential for increased precision and efficiency [1]. While digital approaches for partially edentulous cases are well documented, managing completely edentulous cases remains challenging. Ensuring a precise and passive fit is essential, as inaccuracies can lead to mechanical and biological complications such as screw loosening, fractures, and peri-implant lesions [2]. Heckmann et al. [3] reported that 50% of precision-related errors stem from the clinician’s impression technique, while the remaining 50% result from laboratory inaccuracies. To enhance accuracy in digital protocols, various techniques and materials have been introduced [4,5,6,7].
Although numerous studies compare implant impression techniques for fully edentulous patients, research on hybrid methods integrating conventional impressions with digital scanning remains limited. Intraoral scan bodies (ISBs) are commonly used to capture optical impressions, enabling intraoral scanners (IOSs) to generate raw 3D data for virtual ISB reconstruction. The accuracy of these scans is influenced by factors such as scanning technology, strategy, and inter-implant distance [8]. However, fully edentulous arches present additional challenges due to the absence of distinct reference points, complicating stitching and superimposition required for precise ISB alignment [9,10]. Currently, desktop scanners and photogrammetry are considered the gold standard, though a metal try-in is still recommended for verification. To enhance chairside workflows, recent innovations have focused on refining scan body designs and scanning techniques, with horizontally extended and reverse scan bodies showing potential for improved 3D accuracy [11,12,13]. However, strong supporting evidence for these designs remains scarce.
Reverse scanning has emerged as a promising approach for full-arch restorations. This method involves creating a 3D cast of an implant-supported interim prosthesis using scannable implant analogs. While the IOS is not recommended for this application, laboratory scanners offer superior accuracy [5,6,7]. The chairside reverse scan body (RSB) technique digitally replicates the traditional back-pouring impression method by attaching the RSB to the interim prosthesis post-osseointegration and scanning the assembly extra-orally. This scan is then superimposed onto the prosthesis scan to facilitate precise digital positioning of scan bodies [14]. Papaspyridakos et al. demonstrated a 100% fit with this approach, underscoring its reliability for full-arch prosthesis fabrication [15,16]. However, limited evidence exists regarding the impact of material type and surface texture on the accuracy of reverse scanning. To address these gaps, researchers are exploring modifications in scan body design and surface treatment, though optimal configurations remain unclear. Additionally, achieving high accuracy requires proper scanning techniques and a steep learning curve, highlighting the need for novel methods leveraging advanced technologies.
A recent global consensus by Osstem Company defined “passive fit” as the absence of strain, static load, or separation between a screw-retained implant-supported prosthesis, implant-abutment interfaces, and surrounding bone when installed intraorally, with all screws tightened individually and collectively. Although a misfit of up to 150 µm is considered clinically acceptable [17,18,19], advancements in digital dentistry continue to push for even greater precision.
This study aims to evaluate the accuracy and precision of digital impressions using reverse scan body prototypes and IOSs for rehabilitating edentulous patients following the All-on-4 protocol. Additionally, it seeks to compare accuracy differences between experienced and novice clinicians, as well as various reverse scan body designs and coatings used alongside desktop scanners. The null hypothesis is that there are no differences between groups. By addressing current limitations and exploring innovative solutions, this research aims to optimize fully digital workflows in implant dentistry.
2. Materials and Methods
This study was designed as comparative, in vitro research. One dental student in their final year (FDR) and one expert clinician, with over 20 years of experience in digital dentistry, performed all the procedures. For all the experiments, models of a fully edentulous mandible with gingiva were utilized, specifically designed for implantology exercises. These models featured a dense, thick, porous cortical bone with an internal trabecular structure, mimicking D2 bone consistency (Dentalstore & Edizioni Lucisano SRL, Milan, Italy). A cone beam computed tomography (CBCT) scan (Cranex 3Dx, Soredex, Tuusula, Finland) was performed at 90 KV, 5.0 mA, with a field of view of 6 × 8 and a resolution of 0.2 mm. The resulting DICOM files were then aligned with STL files obtained from an optical scan of the same model (i700, Medit Corp., Yeongdeungpo-gu, Seoul, Republic of Korea). A virtual wax-up was created to facilitate the prosthetic planning of virtual implants using specialized software (Exoplan 3.1 Rijeka prototype, Exocad GmbH, Darmstadt, Germany).
Following this, four Osstem TSIII implants (Osstem Implants, Seoul, Republic of Korea) with a 4 mm diameter and 10 mm length were virtually planned using medical-grade software (Exoplan 3.1 Rijeka prototype, Exocad GmbH, Darmstadt, Germany), adhering to the original protocol proposed by Malò et al. in 2003 [20]. Additionally, three anchor pins were positioned in the buccal region to ensure proper fixation and stabilization of the surgical guide. Once the virtual implant planning was finalized, a modular surgical guide was fabricated. Given the surgical kit used (OneGuide Kit, Osstem Implants, Seoul, Republic of Korea), metallic sleeves were omitted, and templates were entirely 3D printed. The surgical guide was produced at a specialized milling center (New Ancorvis SRL, Bologna, Italy) using a DMP Dental 100 printer and a certified resin material (VisiJet M2R-CL, 3D Systems Inc., Rock Hill, SC, USA).
A total of four dummy implants were fully guided and inserted following the manufacturer’s guidelines. Subsequently, four multi-abutments and corresponding temporary cylinders were attached and secured with the recommended torque values. Finally, a temporary restoration was fixed (Resin Cement (Panavia SA resin cement, Kuraray Europe GmbH-Philipp-Reis-Str. 4-65795 Hattersheim, Germany) using the corresponding module, screwed on the surgical template. Before performing the scans, training was conducted with the student (EDR) in order to teach them the scanning technique to be performed. The training consisted of a theoretical introduction to scanning technology and the main functions of the scanner, a live demonstration of the scanning technique, and hands-on practice with the learned scanning technique. The training was performed by the same expert digital dentist (MT) who performed the other scans in order to ensure calibration between operators. After that, digital impressions were taken by the student and expert according to the following groups:
IOS Scans (n = 24, Figure 1).
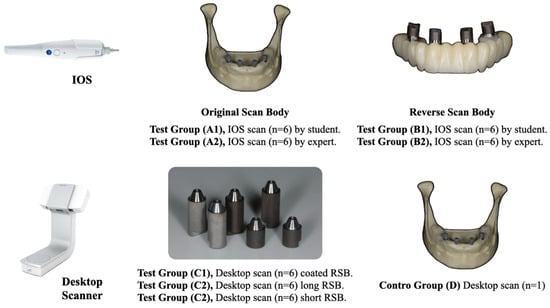
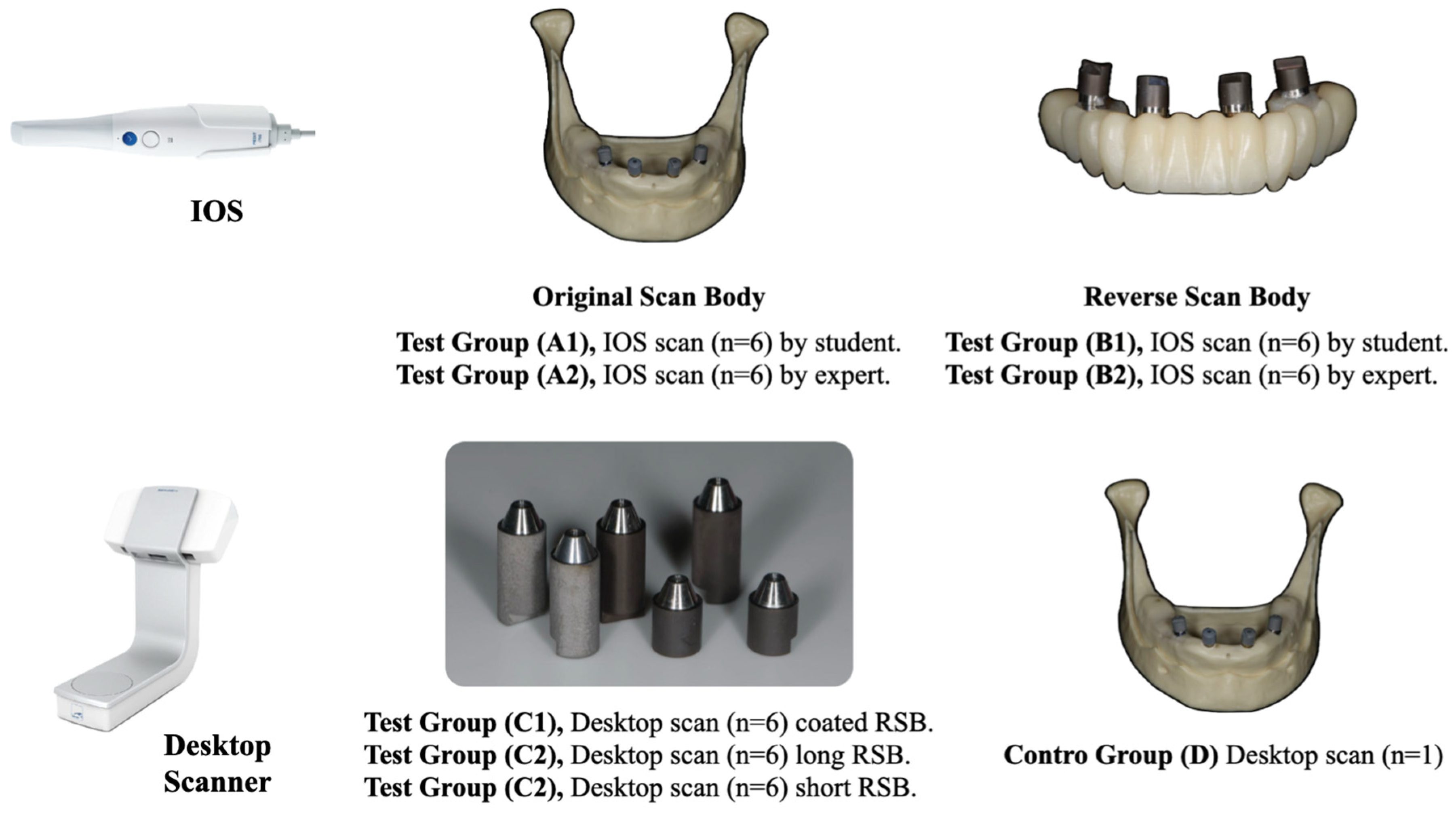
Figure 1.
Allocation of IOS and desktop scanner scans according to the groups.
- -
- In group A, 4 original scan bodies (OSSTEM IMPLANT Co., Seoul, Republic of Korea) were screwed on the multi abutments at 15 Ncm, and then 6 digital impressions (Medit i700, Medit Corp., Seoul, Republic of Korea) were performed by the dental student (subgroup A1), and six digital impressions were taken by the expert clinician (subgroup A2).
- -
- In group B, after the temporary restoration was unscrewed, four short, RSB prototypes (OSSTEM IMPLANT Co., Seoul, Republic of Korea) were screwed at 15 Ncm onto the temporary restoration, and then 6 digital impressions were taken by the dental student (subgroup B1), and 6 impressions were taken by the expert clinician (subgroup B2).
Desktop scans group (n = 18)
- -
- In subgroup C1, after the temporary restoration was unscrewed, four short, sandblasted RSB prototypes (OSSTEM IMPLANT Co., Seoul, Republic of Korea) were screwed at 15 Ncm onto the temporary restoration, and then six scans were taken with a desktop scanner (Nobil Metal SPA, 14018 VILLAFRANCA D’ASTI-AT-ITALIA).
- -
- In subgroup C2, after the temporary restoration was unscrewed, four long, sandblasted RSB prototypes (OSSTEM IMPLANT Co., Seoul, Republic of Korea) were screwed at 15 Ncm onto the temporary restoration, and then six scans were taken with the same desktop scanner (Nobil Metal SPA, 14018 VILLAFRANCA D’ASTI-AT-ITALIA).
- -
- In subgroup C3, after the temporary restoration was unscrewed, four long, coated RSB prototypes (OSSTEM IMPLANT Co., Seoul, Republic of Korea) were screwed at 15 Ncm onto the temporary restoration, and then six scans were taken with the same desktop scanner (Nobil Metal SPA, 14018 VILLAFRANCA D’ASTI-AT-ITALIA).
Control, group D (n = 1)
- -
- Finally, in control group D, four original scan bodies (OSSTEM IMPLANT Co., Seoul, Republic of Korea) were screwed on the multi abutments at 15 Ncm, and then a desktop scan was performed to compare the previous groups. The llocation of groups and subgroups is shown in Figure 1.
2.1. Outcome Measures
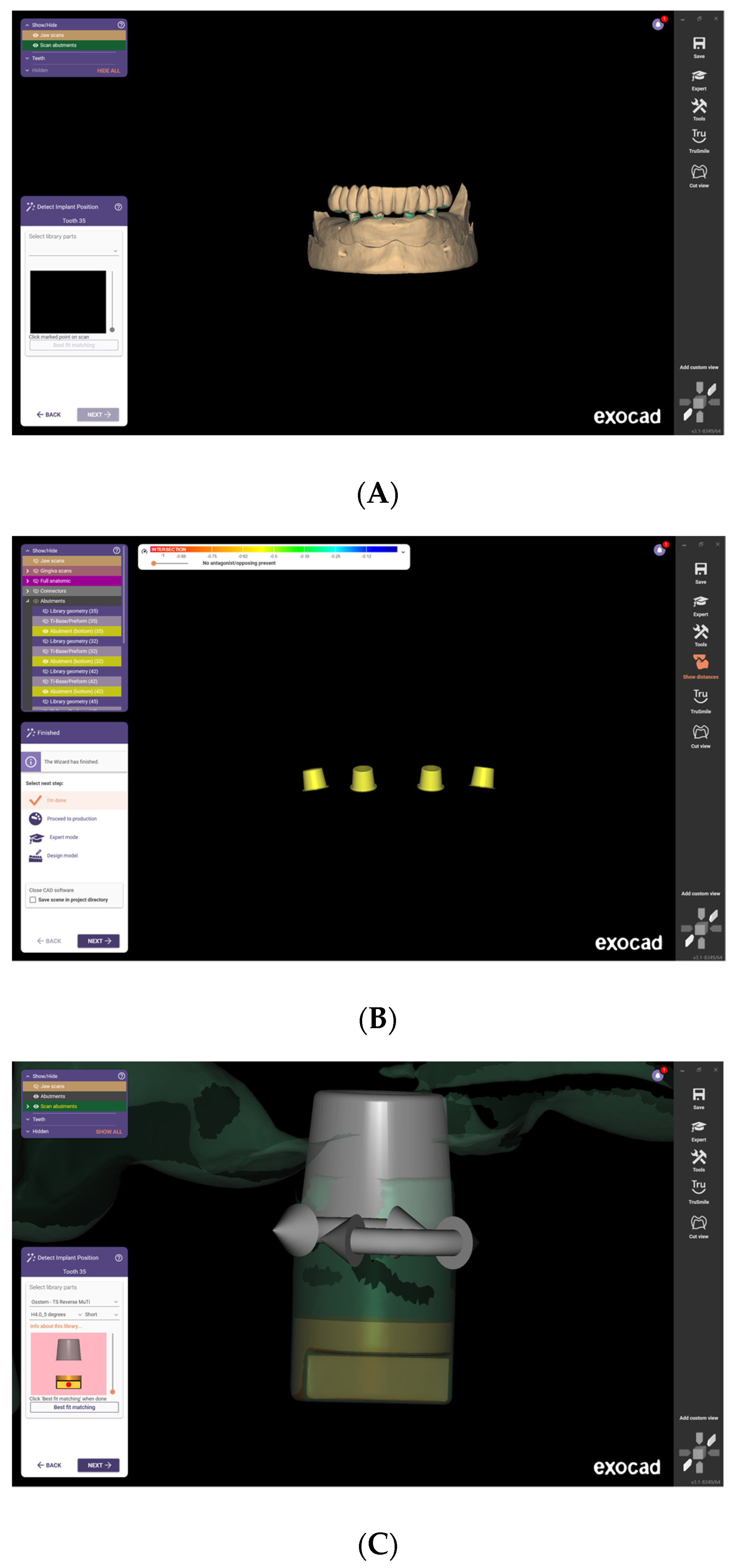
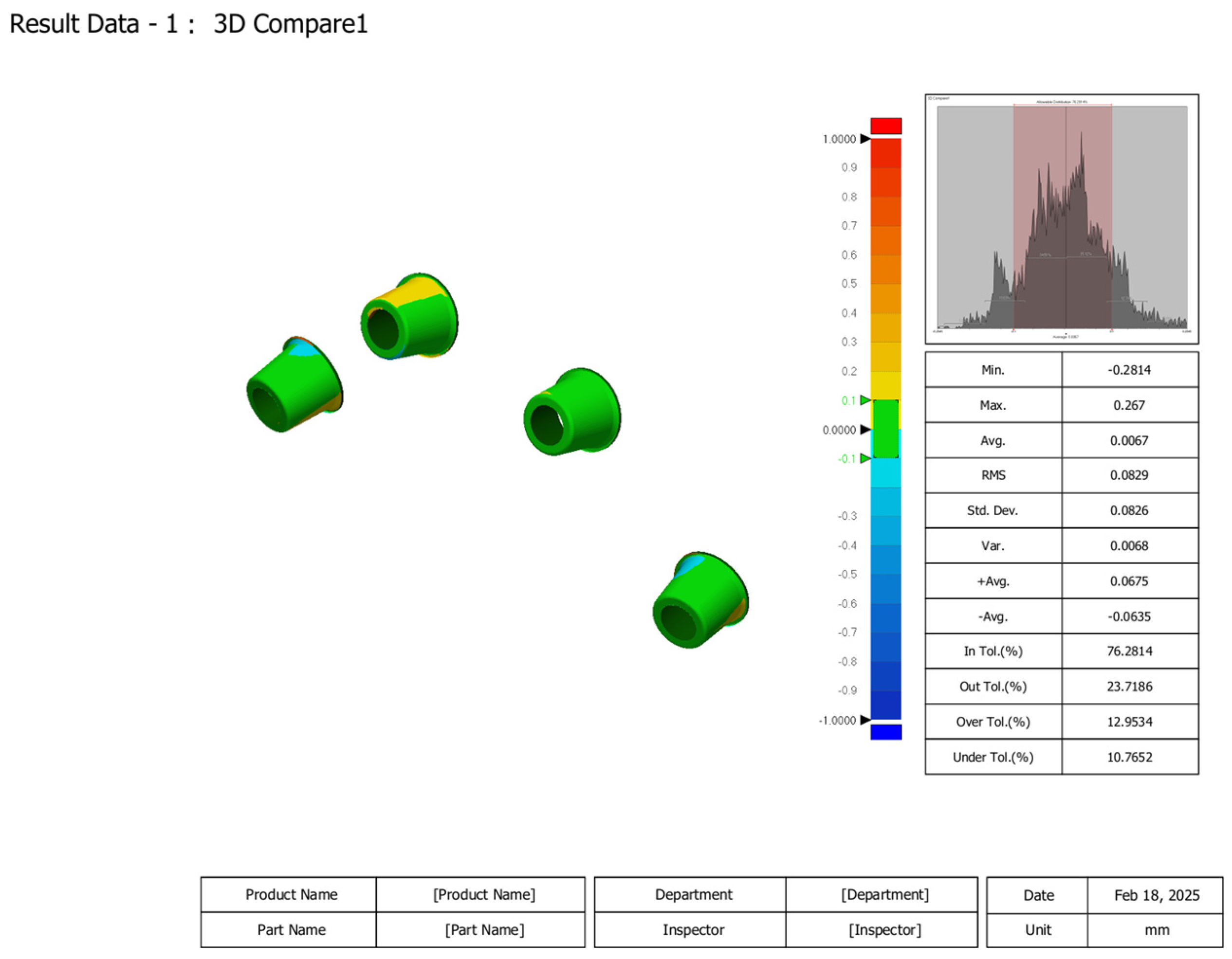
Accuracy refers to how close captured data are to actual dimensions. Precision describes measurement consistency. The STL files from the intraoral (IOS) and desktop scanner were imported into dental designing software (Exocad 3.1 Rijeka prototype, Exocad GmbH, Darmstadt, Germany). All scan bodies were aligned with their corresponding library analogs to evaluate factors influencing accuracy. Subsequently, the STL files of the abutment bottoms were exported, as they were not considered confidential components of implant accessories (Figure 2A–C). To evaluate the accuracy of all scans, dimensional differences were measured using the Root Mean Square (RMS) value resulting from 3D comparisons. The scan files were then imported into digital inspection software, Geomagic Control X, version 2022.1.0 by 3D Systems (Rock Hill, SC, USA), where each scan was compared to the control (desktop scan, group D) to assess dimensional discrepancies (Figure 3). An expert outcome measure performed all the measurements (MQ). Geomagic software does not require direct calibration. Calibration was conducted with scan-to-scan comparison using the master as both test and control. The accuracy of scans and outputs depends on properly calibrating the scanning device and optimizing the software settings. Software settings were adjusted accordingly. Both IOSs and desktop scanners were calibrated at the beginning of each subgroup.
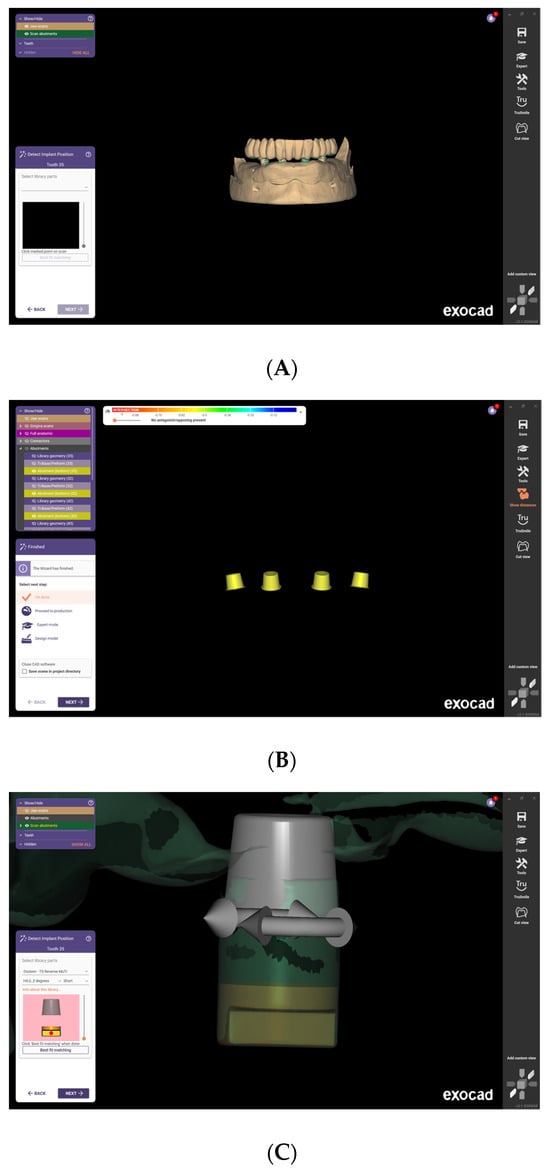
Figure 2.
(A–C) Sequence used to align the scan bodies with their corresponding library analogs in Exocad software (Exocad 3.1 Rijeka prototype, Exocad GmbH, Darmstadt, Germany).
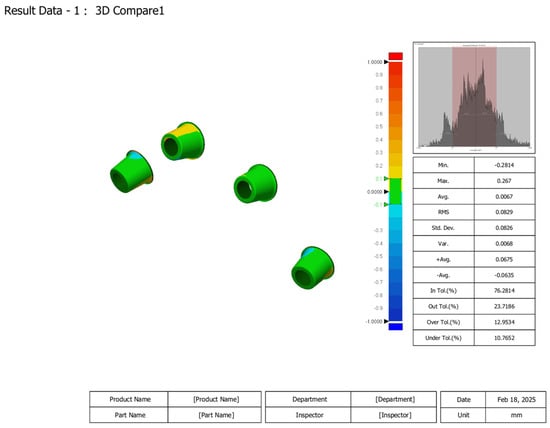
Figure 3.
RMS calculation using Geomagic Control X by 3D Systems (Rock Hill, SC, USA).
2.2. Statistical Analysis
The mean RMS value and SD were then calculated for each group of six scans. Differences in means between student and expert, as well as between groups were compared by a non-parametric Wilcoxon signed-rank test. One-way analysis of variance was performed for statistical comparison on three RSB prototype scans (α = 0.05).
3. Results
A total of 42 + 1 (test + control) scans were taken. Of these, 12 were taken by the student and the same number by the expert, both using IOS. The other scans were taken using a desktop scanner. Within these, four groups (from A to D) and seven subgroups were created. Each subgroup was composed of six scans, while only one scan was taken in the control group (D).
When scanned by the expert in digital dentistry with an IOS, original SBs showed a mean RMS value of 0.0678 ± 0.0088 (an example in Figure 3). When scanned by the student with an IOS, original SBs showed a mean RMS value 0.0773 ± 0.0152. No differences were found between operators (p = 0.220). When scanned by the expert in digital dentistry with an IOS, RSB prototypes showed a mean RMS value of 0.0722 ± 0.0096. When scanned by the student with IOS, original SBs showed a mean RMS value 0.0880 ± 0.0055. Statistically significant differences were found between operators (p = 0.008). Comparing the different SB designs, there was no statistically significant difference in RMS values between the original SBs and RSB prototypes of both the expert in digital dentistry (p = 0.426) and the student (p = 0.154), when IOS was used.
On the contrary, there was a statistically significant difference in RMS values between RSB prototypes scanned with the IOS and desktop scanner, for both the expert in digital dentistry (p = 0.000) and the student (p = 0.001), with better accuracy for IOSs.
Testing the three different RSB prototypes with a desktop scanner, the results were not statistically different. The mean RMS values were 0.104 ± 0.006 for short and lasting RSB prototypes; 0.106 ± 0.005 for long and sandblasted RSB prototypes; and 0.103 ± 0.008 for long and coated RSB prototypes. All the data are summarized in Table 1 and Table 2.

Table 1.
RMS values between groups for IOS scans.
Table 2.
RMS values between groups for Desktop Scanner.
4. Discussion
This study assessed the accuracy of digital impressions using reverse scan body (RSB) prototypes and intraoral scanners (IOSs) for rehabilitating edentulous patients following the All-on-4 protocol. The null hypothesis of no differences between groups was partially rejected against the hypothesis of differences. The results demonstrated that IOS-generated digital impressions were more accurate than those obtained with a desktop scanner, regardless of the operator’s experience. Additionally, no significant differences were observed between original scan bodies (SBs) and RSB prototypes when scanned with the IOS, supporting the potential of RSBs for fully digital workflows.
Statistical analysis revealed a significant difference in accuracy between digital impressions captured with the IOS and those obtained using a desktop scanner, with the IOS exhibiting superior precision (p = 0.000 for experts, p = 0.001 for students). This aligns with previous studies suggesting that advancements in scanning algorithms and image stitching techniques contribute to the high accuracy of IOSs in implant impressions [1,2]. However, fully edentulous arches present unique challenges due to the lack of distinct reference points, necessitating precise scanning protocols and the continuous refinement of scan body designs [3]. Given that accuracy losses occur equally across clinical and laboratory procedures, evaluating their combined impact remains essential [3].
An interesting finding was the lack of significant accuracy differences between expert and novice users when using original SBs with the IOS (p = 0.220). However, significant discrepancies emerged with RSB prototypes (p = 0.008), suggesting that while conventional SBs are user-friendly, RSBs require a more advanced skill set. This underscores the need for training and experience when integrating novel digital workflows. Prior studies have also emphasized the role of operator expertise in the precision of digital impressions [4,5]. According to a multicenter clinical trial, the accuracy of the digital impression on implant full-arch rehabilitations seems to be influenced by the clinician’s skills. However, in this research, a comparison of full-arch intraoral scans was performed immediately after implant insertion instead of after the tissue healed, potentially increasing the risk of inaccuracy [21].
Furthermore, comparisons between original SBs and RSB prototypes revealed no statistically significant differences in accuracy when scanned with the IOS, irrespective of the operator’s experience level. This suggests that RSB prototypes could serve as a viable alternative in digital implant workflows. However, when scanned with a desktop scanner, variations in RSB prototypes—including differences in length and surface treatment (long and coated, long and sandblasted, short and sandblasted)—did not significantly impact accuracy. These findings indicate both surface treatments have a similar effect in diffusing light and controlling reflectivity, allowing them to reach the same accuracy. On the other hand, even if shortened RSBs are suggested for the chairside workflow, RSB length has minimal influence when desktop scanning technologies are used.
Intraoral scanners project a patterned light onto the surface and reconstruct 3D geometry based on how that pattern is distorted, and metallic materials, like titanium, have high reflectivity and strong specular reflection, which causes light to bounce off in a single direction, making it difficult for the scanner to detect the pattern accurately. To overcome this drawback, modification of the titanium surfaces has been proposed. In the present study, sandblasting creates fine surface irregularities on the reverse scan body, which promotes diffuse reflection by scattering light in multiple directions. This not only reduces specular reflection but also enhances the scanner’s ability to detect spatial and depth information more precisely. Moreover, the micro-texture formed through blasting serves as a reference during scan alignment, improving the overall scan accuracy. Similarly, a matte coating is applied to the reverse scan body surface. This creates micro-textures that induce diffuse reflection, allowing the scanner to capture the shape more evenly and accurately.
Implications for Digital Workflows in Implant Dentistry
The findings of this study suggest that RSB prototypes are promising for enhancing chairside workflows in implant dentistry, particularly for fully edentulous cases treated with the All-on-4 protocol [22]. The absence of significant differences between RSB prototypes and original SBs when using the IOS indicates that RSBs can be seamlessly integrated into fully digital workflows without compromising accuracy. Furthermore, the enhanced accuracy observed with the IOS highlights its potential as a reliable alternative to traditional desktop scanning systems, potentially reducing clinical chair time and laboratory costs [23].
This study is pioneering in investigating the accuracy of novel RSB prototypes and in defining which design (height) and surface treatment can produce better results in terms of accuracy, both using IOS and desktop scanners. The main limitation of the present research is that this study was conducted under in vitro conditions, which may not fully replicate the complexities encountered in clinical practice, such as patient movement, saliva, and varying soft tissue dynamics. Additionally, the sample size was relatively small, particularly for the subgroup comparisons. Future studies with larger sample sizes and in vivo settings are recommended to validate these findings. Furthermore, investigating the long-term clinical performance of prostheses fabricated using RSB prototypes would provide valuable insights into the clinical applicability of this digital workflow.
5. Conclusions
In conclusion, this study demonstrated that the IOS provides superior accuracy compared to desktop scanners for digital impressions of edentulous arches using RSB prototypes. The findings suggest that RSB prototypes are a viable alternative to original SBs for fully digital workflows in All-on-4 rehabilitations. However, adequate training is essential to maximize the accuracy and reliability of RSBs. Height and coating of RSB prototypes did not influence the overall accuracy. Looking at the future, these results contribute to optimizing digital workflows in implant dentistry, paving the way for more efficient and accurate restorative solutions for edentulous patients; however, further randomized controlled trials with sample size calculations are needed to confirm these preliminary results.
Author Contributions
Conceptualization, M.T. and E.D.R.; Methodology, M.T. and M.Q.; Software, M.Q.; Investigation, E.D.R. and M.T.; Writing—original draft preparation, M.T. and C.C.; formal analysis, M.Q. and M.P.; validation, S.M.M. and A.I.L.; Resources, Y.J.J. and F.M.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. Scan body prototypes were donated by Osstem Implant.
Institutional Review Board Statement
Not needed for in vitro research.
Informed Consent Statement
Not needed for in vitro research.
Data Availability Statement
No extra data were created or analyzed in this study.
Conflicts of Interest
All the authors declare no conflicts of interest in this study.
References
- Cicciù, M.; Tallarico, M. Dental Implant Materials: Current State and Future Perspectives. Materials 2021, 14, 371. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, R.M.; Yilmaz, B.; McGlumphy, E.A., Jr.; Seidt, J.; Johnston, W.M. Accuracy of different digital scanning techniques and scan bodies for complete-arch implant-supported prostheses. J. Prosthet. Dent. 2020, 123, 96–104. [Google Scholar] [PubMed]
- Heckmann, S.M.; Karl, M.; Wichmann, M.G.; Winter, W.; Graef, F.; Taylor, T.D. Cement fixation and screw retention: Parameters of passive fit. Clin. Oral Implants Res. 2004, 15, 466–473. [Google Scholar]
- Tallarico, M.; Galiffi, D.; Scrascia, R.; Gualandri, M.; Zadrożny, Ł.; Czajkowska, M.; Catapano, S.; Grande, F.; Baldoni, E.; Lumbau, A.I.; et al. Digital Workflow for Prosthetically Driven Implants Placement and Digital Cross Mounting: A Retrospective Case Series. Prosthesis 2022, 4, 353–368. [Google Scholar] [CrossRef]
- Nuytens, P.; Vandeweghe, S.; D’haese, R. Accuracy of a chairside reverse scanbody workflow for a complete arch implant-supported prosthesis using four intraoral scanners versus a desktop scanner. J. Dent. 2023, 138, 104717. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Bedrossian, A.; Kudara, Y.; Ntovas, P.; Bokhary, A.; Chochlidakis, K. Reverse scan body: A complete digital workflow for prosthesis prototype fabrication. J. Prosthodont. 2023, 32, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Hyspler, P.; Urbanová, P.; Dostalova, T. Comparison of the reverse scan technique with an intraoral scanner and the traditional impression technique. J. Prosthet. Dent. 2024. [Google Scholar] [CrossRef] [PubMed]
- ISO-5725-1; Accuracy IS. of Measurement Methods and Results—Part 1: General Principles and Definitions. International Organization for Standardization: Geneva, Switzerland, 1994.
- Papaspyridakos, P.; Vazouras, K.; Gotsis, S.; Bokhary, A.; Sicilia, E.; Kudara, Y.; Bedrossian, A.; Chochlidakis, K. Complete digital workflow for prosthesis prototype fabrication with double digital scanning: A retrospective study with 45 edentulous jaws. J. Prosthodont. 2023, 32, 571–578. [Google Scholar] [CrossRef]
- Pereira, A.L.; Curinga, M.R.; Segundo, H.V.; Carreiro, A.D. Factors that influence the accuracy of intraoral scanning of total edentulous arches rehabilitated with multiple implants: A systematic review. J. Prosthet. Dent. 2023, 129, 855–862. [Google Scholar]
- Wu, H.K.; Chen, G.; Zhang, Z.; Lin, X.; Huang, X.; Deng, F.; Li, Y. Effect of artificial landmarks of the prefabricated auxiliary devices located at different arch positions on the accuracy of complete-arch edentulous digital implant scanning: An in-vitro study. J. Dent. 2023, 140, 104802. [Google Scholar]
- Huang, R.; Liu, Y.; Huang, B.; Zhang, C.; Chen, Z.; Li, Z. Improved scanning accuracy with newly designed scan bodies: An in vitro study comparing digital versus conventional impression techniques for complete-arch implant rehabilitation. Clin. Oral Implants Res. 2020, 31, 625–633. [Google Scholar] [CrossRef] [PubMed]
- García-Martínez, I.; Zarauz, C.; Morejón, B.; Ferreiroa, A.; Pradíes, G. Influence of customized over-scan body rings on the intraoral scanning effectiveness of a multiple implant edentulous mandibular model. J. Dent. 2022, 122, 104095. [Google Scholar] [CrossRef] [PubMed]
- Chochlidakis, K.; Papaspyridakos, P.; Tsigarida, A.; Romeo, D.; Chen, Y.W.; Natto, Z.; Ercoli, C. Digital Versus Conventional Full-Arch Implant Impressions: A Prospective Study on 16 Edentulous Maxillae. J. Prosthodont. 2020, 29, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Liaropoulou, G.; Kamposiora, P.; Quilez, J. Reverse impression technique: A fully digital protocol for the fabrication of the definitive fixed prosthesis for completely edentulous patients. J. Prosthet. Dent. 2024, 132, 132–1118. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Bedrossian, E.A.; Ntovas, P.; Kudara, Y.; Bokhary, A.; Chochlidakis, K. Reverse scan body: The scan pattern affects the fit of complete-arch prototype prostheses. J. Prosthodont. 2023, 32, 186–191. [Google Scholar] [CrossRef]
- Fiorillo, L.; D’Amico, C.; Ronsivalle, V.; Cicciù, M.; Cervino, G. Single Dental Implant Restoration: Cemented or Screw-Retained? A Systematic Review of Multi-Factor Randomized Clinical Trials. Prosthesis 2024, 6, 871–886. [Google Scholar] [CrossRef]
- Wulfman, C.; Naveau, A.; Rignon-Bret, C. Digital Scanning for Complete-Arch Implant-Supported Restorations: A Systematic Review. J. Prosthet. Dent. 2020, 124, 161–167. [Google Scholar] [CrossRef]
- Nulty, A. A novel methodology for analysing dental implant positional changes from virtual planning to placement without CBCT. Br. Dent. J. 2024, 1–6. [Google Scholar] [CrossRef]
- Maló, P.; Rangert, B.; Nobre, M. “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: A retrospective clinical study. Clin. Implant. Dent. Relat. Res. 2003, 5 (Suppl. S1), 2–9. [Google Scholar] [CrossRef]
- Bagnasco, F.; Menini, M.; Pesce, P.; Crupi, A.; Gibello, U.; Delucchi, F.; Carossa, M.; Pera, F. Comparison of Full-Arch Intraoral Scans Immediately After Implant Insertion Versus Healed Tissue: A Multicentric Clinical Study. Prosthesis 2024, 6, 1359–1371. [Google Scholar] [CrossRef]
- Cannizzaro, G.; Felice, P.; Gherlone, E.; Barausse, C.; Ferri, V.; Leone, M.; Trullenque-Eriksson, A.; Esposito, M. Immediate loading of two (fixed-on-2) vs four (fixed-on-4) implants placed with a flapless technique supporting mandibular cross-arch fixed prostheses: 3-year results from a pilot randomised controlled trial. Eur. J. Oral Implantol. 2017, 10, 133–145. [Google Scholar] [PubMed]
- Ferrini, F.; Mazzoleni, F.; Barbini, M.; Coppo, C.; Di Domenico, G.L.; Gherlone, E.F. Comparative Analysis of Intraoral Scanner Accuracy in a Six-Implant Complete-Arch Model: An In Vitro Study. Prosthesis 2024, 6, 401–412. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).