1. Introduction—3D Printing Prosthetic Limbs
Advances in 3D printing have enabled a wider range of people to explore and create potential prosthetic device solutions than ever before. This democratising of design has moved into many areas, but one that has enjoyed a particularly broad focus is the design of upper limb prosthetic hands and arms [
1]. Despite this, far fewer designs have progressed from the development phase into the field for clinical applications and very few use the one single biggest potential advantage of additive manufacture; the ability to make something easily that is hard or impossible to construct using more traditional methods [
2].
One advantage of 3D printing is the facility to realise a model of a design concept in three dimensions relatively quickly and cheaply. However, this comes at the cost that many forms of the 3D printed material are weak and brittle, and therefore cannot generate or withstand the forces that they will be subject to in the field by a prosthesis user. This becomes crucial when designing a prosthesis for Low and Middle Income Countries (LMICs), where more of the prosthesis usage tends towards heavier loads and rural agricultural tasks. Therefore, 3D printed upper limb solutions designed in the developed world must be made with strong, durable, robust materials before being deployed for field testing in LMICs if they are to have a chance of being accepted by the population they are intended for. Ikeda et al reached similar conclusions in their review of prosthetics and orthotics designs for resource-limited environments [
3].
However, the use of 3D printing in LMICs must consider the local population’s ability to sustainably reproduce and maintain the upper limb device. A single 3D printed object can take a comparatively long time to produce (many hours) and requires a stable power supply throughout the process. This could impact in places where the power supply is not stable due to local outages or a facility’s need to power down a workshop when no worker is present. This is where the discussion of local infrastructure becomes integral to 3D printing being regarded as a viable option.
Claims of 3D printing providing affordable access to prosthetic interventions in both high income countries and LMICs have previously ignored the costs of labour and time when advertising a solution. More recently 3D printing communities have distinguished between charities that operate through volunteer networks and donations, and prosthetic clinics that would need to reflect operation costs (wages, insurance, etc.) into any solution they provide. These distinctions are often reflected when 3D printing groups discuss ‘material costs’ or ‘production ‘costs’ or ‘manufacturing cost’ [
4] or admit that they are 3D printing the diagnostic socket and not a finalized device, or that the 3D printed device requires both a functional wrist and most of the palm to be intact. For upper limb specifically, some organizations now clearly state that their designs should not be seen as fully functional prosthetic devices [
5]. These details are important because they affect in-country costs in different ways, and this becomes a crucial consideration when providing any solution in LMICs. Some groups have gone to the effort of providing an estimate of overall local production cost [
6,
7] Even the provision of a 3D printed device at zero cost to the user may not be sufficient. For example, traveling to a location where the device is being provided may be unaffordable, which will keep any low cost prosthesis out of the hands of the people that it is meant for.
Transportation is but one of many accessibility issues that needs to be address when discussing how to create the infrastructure required for delivery of a prosthesis. Also, creating a 3D printed device in a wealthy nation may not be a solution for an LMIC if the fabrication materials are difficult to source locally or if the fabrication method requires significant long-term investment. This sort of investment is more attractive to funding bodies if the device is shown to be useful. This means that it assists the user in achieving their goals and desires. To do this, it is essential that the end user is a part of the design process early on, as different countries will not have the same societal attitudes towards those with limb loss. A 3D printed device that is heavily stylized with a robotic appearance may be accepted in one country but may be the source of social harassment in another.
The aim of the Fit for Purpose (F4P) project was to create a design for a practical prosthesis that was acceptable to potential Ugandan users, that ultimately could be produced and serviced in Uganda where its production would benefit the users by being more affordable than a device produced elsewhere. It was a collaboration between teams in the UK (Salford, University College London, Portsmouth, Southampton Universities), Uganda (Makere University), Jordan (University of Jordan) and the USA (Fillauer TRS). It began with a process of investigating the barriers to prosthetic provision [
8,
9] and then progressed to a co-design process to focus in on a viable design.
1.1. Needs Assessment in Uganda
Staats et al. [
10] estimated that by 1996, limb loss (lower and upper) affected more than 5000 individuals in Uganda, though exact numbers based on government records are not known. Huck et al. [
11] estimated that people with major limb loss in the Acholi region (northern Uganda) was 10,117. As there is no national registry, the specific number of individuals with upper limb loss is not known, though Muhumuza and Bangirana [
12] have indicated that trauma (e.g., road traffic accidents, violence, etc.) is the main indication for upper limb amputation, followed by diabetes, and then malignant tumors at the Mulago National Referral Hospital between 2000–2011. More recent work by Kenney et al. [
8] supports that trauma is the main source of upper limb loss, though this can vary by region.
A series of short studies conducted by the F4P team established that the prosthetic services in Uganda were both highly fragmented and under-resourced [
8]. Other factors included the relatively high cost of the imported devices they currently provide, the lack of knowledge within the profession or population of what is possible or available, the distance needed to be traversed to get to a clinic and the inconsistent nature of the prosthetic supply chains that make repairs difficult or impossible [
8,
13]. Unsurprisingly in a country with limited welfare, income generation was found to be a critical aspect of the need for a prosthesis, as self-sufficiency is paramount. A subsequent study interviewed 17 people living with upper limb absence in Uganda [
14]. The interviewees, only 3 of whom had any experience of using a prosthesis, reported facing many barriers to various aspects of life, including accessing work. When asked about what they wanted from a prosthesis, they prioritised a range of factors including skin tone match, as well as high reliability and good levels of function [
15].
A clinical prosthetic service aims to provide the basic provision of the prosthesis: user assessment, casting and manufacture of the socket, supply and fitting of the prosthesis and training of its use. This can take multiple visits as the socket and suspension/control harnessing is adjusted to optimise effective use. Prostheses also require routine maintenance and repair. While some of this can be done remotely (mailed to and from the clinic), other adjustments can only be done when the user is present. This assumes that the specific country has the infrastructure for routine transport which can occur smoothly, cheaply and securely. A study in parallel in Cambodia showed that the expense of prosthesis repair can lead to greater poverty [
16]. Farmers had to sell livestock to pay to travel to a distant centre for the repair of their limb, and this deficit was not made up before the next time they needed a repair, increasing their poverty long-term. This is also why a myoelectric device is not a viable solution, as the cost for the device, repair and maintenance is well above what the average Ugandan earns in a year, and such a device would not address the ADLs most people undertake without fear of damage (see ADL discussion below). For Uganda specifically, the design ethos must be rooted in the country’s daily reality. The design methodology needs to adhere to a wear and tear, with no possibility of repair approach, to avoid imposing added burdens to the individual (financial, cognitive, etc.), while ensuring that the prosthetic solution is not simply accepted by the individual and then quietly stored in a drawer, only to be used during community events.
This paper will address the specific problem of creating a terminal device that is culturally acceptable in Uganda and how 3D printing efficiently facilitates arriving at a solution. The peripheral infrastructure issues mentioned above are also being addressed by the F4P team (casting, materials supply, socket/suspension, access to trained specialists, funding). The mechanisms to deliver the physical device to the individual and training on device operation are also being analysed and will be mentioned later in this paper. The benefit of 3D printing is in providing local control and increasing local capacity to provide upper limb solutions that are tailored to the specific population.
1.2. Understanding Limitations and Building a Cultural Lens
Moving towards a solution required an acceptance of certain limitations that would impose on any design. Previous work in Uganda had indicated a high degree of social harassment and economic discrimination exists and those with limb loss were always aware of the visibility of disability. The appearance factor is high, and this was addressed in the design, as there was a need to build a level of trust between the F4P team and the potential users. This ensures continued user-centred development. A related design criteria is that of a suspension-control harness. Any suspension strap situated around the shoulders would immediately draw attention, even when worn under clothing. These suspension systems are also difficult to don, create friction, create discomfort, break down, and will require adjustments from a clinical specialist. They also limit the reachable and functional workspace of the user [
17].
The decision was made to avoid a shoulder-mounted suspension system in the novel design. This removed several of the barriers to an acceptable solution, but also removed the most traditional user input. The team also wanted to reduce reliance on the opposite hand to operate a device, which meant eliminating the need of the contra-lateral involvement in helping ‘form the grasp’ of the terminal device. Yet the novel design was intended to be more than a simple 3D printed passive device. The result of this was that any user input to the terminal device had to occur at the level of the terminal device, which forced a modular development of the prosthesis. As long as the proximal socket incorporated the standard ½-20 thread, the terminal device could be used at multiple-levels of upper limb loss.
The above design decisions create an envelope of potential solution paths that are not open-ended, as they are informed by the lived experience in Uganda. There are also basic design principles that need to be adhered to. For instance, the prosthesis cannot make it more difficult to perform a task that the individual is already doing, as asking someone to unlearn a developed coping strategy can result in immediate rejection of the prosthesis. Also, addressing the entire population need is not the same as designing for the population we were likely to interact with. Delivering prosthetic solutions in LMICs often comes with the added design constraints of limited time frames and budgetary restrictions. Gaining minimum traction with a smaller number of potential users is preferable to gaining no traction with a larger population.
Defining a profile for the potential user early on was seen as a necessity to ensuring a culturally acceptable solution. The 3D printed terminal device would therefore focus on a unilateral adult transradial user with an emphasis on reducing moving parts to avoid breakdown, as repair services were assumed to be costly or inaccessible [
8]. This meant that a durable material must be used, a 3D printer capable of printing this material must be employed, the design must reduce weight (i.e., comfort without a harness) and provide some function, all whilst contained in an overall acceptable aesthetic appearance that would prevent putting the individual’s disability on display.
2. Materials and Methods—Co-Design Approach for Direct User Input
The logistics of designing an upper limb prosthesis for use in an LMIC is best accomplished through direct user involvement. The approach taken was within a process called Patient and Public Involvement and Engagement (PPIE) and focused on performing a Co-design activity. This is a type of participatory framework where there is direct involvement from the participants and their lived experience can contribute strongly to the eventual solution, facilitating an iterative approach. As this approach promotes repeated regular meetings, it also promotes the development of a long-term relationship, which makes participants comfortable sharing their more personal needs and desires, resulting in a more suitable design. However, as the work was conducted under a PPIE framework, the team did not make any video or audio recordings of the events. The two Co-design activities took the form of a 2-Day workshop (5 months in between) organized locally in Uganda. There were no limitations placed on who could participate in these workshops (potential users, caregivers, organizers) as operating in an LMIC already brings with it added political volatility and the ongoing COVID-19 pandemic had imposed additional restrictions.
For both Co-design 1 and 2, two researchers (authors BM and RS) along with a local organizer facilitated the workshops and provided translation in the local language for the participants. The workshops made use of the KoboToolbox (
http://www.kobotoolbox.org, accessed on 26 October 2021) a digital data collection tool to present the participants with questions, descriptions of ADLs, photographs/videos of terminal device operations, and to record the feedback. Each co-design activity was designed by first establishing what the goals of each workshop would be (defined below) and then determining the nature and order of the questions to ask. The team also regularly met with industry consultants from Fillauer TRS, a manufacturer of upper limb terminal devices with a long history of designing durable upper limb solutions for both general use and specific ADLs. Their experiences with similar engagement activities in different countries guided the team in how to structure the questions in the co-design activities.
The co-design 1 activity exploited a discrete choice approach, often used in the design of healthcare services [
18], to encourage the users to explore the trade-offs between function and appearance. Discrete choice experiments result in the definitive feedback needed to make decisions on priority design features to create a working prototype. Co-design 2 followed a similar discrete choice approach, but focused on specific physical prototype features to advance decisions on physical characteristics (detailed in
Section 3.2).
2.1. Co-Design 1
The purpose of the first workshop was to establish the extremes for what would be acceptable and what would be rejected outright. Prosthetics industry consultants at Fillauer TRS had advised establishing the degree of anthropomorphic quality (hand-like nature) needed in the design to avoid rejection. As the design also intended to provide utility to perform certain tasks (e.g., grasping, lifting, etc.), the degree to which the terminal device could resemble a tool and not a hand was important. The answers to these questions are highly dependent on where a person lives (rural vs. urban), what tasks they need to perform, and the attitude of the people around them towards those with limb loss.
In sessions with individuals, the participants were shown photographs of four commercial upper limb terminal devices (
Figure 1) to explore options from functional (manipulative) to entirely cosmetic (anthropomorphic). They were also shown short videos of the terminal device being opened and closed by the opposite anatomical hand (excluding the fourth device which was a cosmetic glove to represent a passive hand). This was important as these terminal devices were all designed to be operated by a cable-system attached to a shoulder mounted harness, an input that the potential design would not have. Care was taken to avoid creating unrealistic expectation. No terminal devices were physically present.
The next stage was to describe a series of six Activities of Daily Living (ADLs) that were based on the results of an earlier scoping survey [
8]. The tasks were chosen as they were very common activities (in Uganda) and focused the participants on the ways they might grip the target object. For example, a woven basked (called a Kibbo) could be gripped in over hand, under hand or supported from below and the users could see themselves using one or more ways (
Figure 2).
Participants then rated the ADLs based on whether they felt the ADL was essential to their daily life or whether it was of no importance to them. The six ADLs were: Gardening (use of a shovel), carrying a jerry can full of water, peeling a Matoke (local fruit), clothes washing, manipulating a Kibbo basket and holding a football. The participants then rated the ADLs alongside the type of device the user considered best able to perform the tasks, combining two factors (aesthetics and function) and ADLs. Based on the results of this workshop, 3D printing was used to create initial prototypes with the intent of returning to the participants to further inform and refine the design.
Co-Design 1 Results
Co-design 1 identified two distinct factors: the participants (n = 21) wanted to be able to pick up objects and they did not want their prosthesis to draw attention to themselves. It was clear that they wanted both a tool and a hand.
Combining both of these features into a single design was deemed to have a high possibility of rejection. Though the initial intention was to find an acceptable balance between the two, the route pursued was to then create a solution that was composed of two devices. The first would be a passive device shaped to look like a hand, the second would be a functional device that would allow for grasping and manipulation activities. As a passive device has less complexity to it, it became the priority as it could be realised through 3D printing in a shorter timeframe. This would allow for an earlier second interaction with the potential users (maintaining trust), but also provide an opportunity to see if the aesthetic would be acceptable. In practice, because a user will visually assess the terminal device before donning it, the aesthetics will take priority.
The functional device would take the form of a prosthetic prehensor (wraps around objects in addition to grasping them) with the focus of addressing the six ADLs. Participants generally disliked an obvious hook because of its appearance, though some appreciated its utility. The passive hand design however provided the benefit of being able to address two of the ADLs: supporting the Kibbo from underneath and holding a football with two hands (bilateral opposition forces applied to objects).
Feedback from the first activity also allowed certain design criteria of the functional device to be defined using the ADLs. Informing the design with the ADLs the participants deemed important decreases the chance of rejection. This was also important to do at this stage as it would have an effect on what materials would be used to 3D print with and what type of shape the prehensor would require. For example, the design must be able to form a grip around the handle of the typical jerry can used for carrying water in Uganda without the handle sliding back and forth relative to the prehensor with every step that is taken when walking. The material choice must permit this shape to be achieved and the device must be able to withstand the weight of the carried load without failing. Specifically, the 3D print material and layer adhesion must provide a durable strength profile. Another ADL (washing clothes) required the terminal device to be submerged in soapy water for extended periods. Materials that rust and corrode need to be minimized (nuts, bolts, springs, etc) and the 3D printing material had to be chosen to reduce moisture absorption pre and post printing.
This approach of using these priority ADLs to drive design features allowed for a more efficient preparation to deliver the second workshop: Co-design 2.
3. Co-Design 2
Preparation for the second workshop and development of the prosthetic prototypes required certain decisions on 3D printing to be made, as what was presented directly influenced what feedback could be obtained. Co-design 2 focused on the passive hand and needed to result in feedback on the acceptability of shape, colour and surface finish. Surface finish has an effect on friction (when pushing or holding objects) and the way the material reflects light can indicate to an onlooker that a person is wearing a prosthetic device (potential for harassment). It is worth noting that a passive hand design with a cosmetic cover was rejected as it would create an additional consumable and any tears in the glove could result in abandonment, as reflected in earlier interviews [
8].
3D printing of the passive device provided the most efficient fabrication route to ensuring a prototype could be ready for Co-design 2 within an acceptable time-frame. Many prosthetic devices destined for the upper limb often employ forged steel or injection moulding, but these approaches require additional infrastructure to be in place as well as finalized shapes to make moulds. These routes do not lend themselves to rapid prototyping or the iterative design approach within the constraints of the co-design activities. Additionally, the funds to purchase adequate machinery and to hire, train and support a worker to manage this equipment ensures that these are not paths that can be taken for preparing a prototype at this stage and one that would need to be updated depending on participant feedback. 3D printing was the most adaptable solution. Previous work by Phillips found that 3D printing is better suited for LMICs because of the minimal skill required and low start up cost, and therefore is the most realistic approach [
4].
Fusion 360 was the chosen CAD software for this project as it is free for use by educators, university employees, and students. This ensured that the design files and 3D printing files remain accessible (to view and modify) to any team member without needing to purchase a software licence. Updates to prototypes in future iterations can be performed by team members with Fusion 360. This is an important consideration in projects that extend past the term of the specific team members that worked on contracts for only a few years, as this could severely limit the project’s forward progression.
The design and modifications to terminal devices in this project were done by one of the authors (AH), who is experienced in prosthetics design (including CAD), mechanical engineering and formally trained as a prosthetic technician. 3D scanning and 3D printing (and related technical consideration) were performed WK, a specialist technician at the University of Portsmouth, and local (Uganda) fabrication is directed by BM, a biomedical engineer at Makerere University.
3.1. 3D Printing the Passive Hand
An existing commercial terminal device (supplied by Fillauer TRS) was chosen to be the model on which to base the 3D printed hand. This device had a definite aesthetic quality and already existed in a number of colours, though it is not produced using a 3D printing process. The device’s ability to bend, flex, and absorb shock made it a good device to replicate. Two of these devices in different colours (right side, dark brown and black) were provided. A third modified version had a channel placed in between the digits. This was an aperture that created an opening from the palm to dorsum, designed to hold utensils (spoons, knives, etc.) and allowed the team to gauge feedback from the participants to holding utensils. It was eventually decided by the team that the functional device (prehensor) would address these tasks with its active grip.
One of these hands was then scanned using an EinScan Pro+ 3D scanner (Shining 3D, Hangzhou, China) and the resulting file was imported into the CAD software. The imported model was then processed to ensure that any voids in the scanning process were patched, before exporting the file to the 3D printer. The hand was printed upright on the printer bed (i.e., lowest layer is the wrist end) with a Prusa i3 MK2S (Prusa Research, Prague, Czech Republic) located at the University of Portsmouth. The main structure had 40% infill, print speed between 15–20 mm/s, and layer height of 0.2 mm. The flexible filament chosen was Ninjatek Chinchilla (Fenner Inc., 187 West Airport Road, Lititz PA 17543, USA). This is a thermoplastic elastomer (TPE) material with a Shore hardness of 75A, a matte finish, and resulted in a passive hand that could very closely mimic the flexible nature of the commercial terminal device it was modelled after. The local research group at Makerere University also have a similar printer (MK3S). This ensured that the passive device could be produced in multiple centres within the target country and that future updates of passive devices could be designed globally but produced locally which could reduce delivery times. The commercial device and the 3D printed hand are shown in (
Figure 3).
3.2. Co-Design 2 Results
Co-design 2 was structured with individual sessions followed by a group discussion. to obtain feedback from participants. The majority of participants found the shape of the passive hand acceptable and many remarked that they thought family and community members would react positively to its aesthetics. The feeling of being more independent was also expressed.
Though there was a preference for the smoother texture of the commercial device, the texture of the 3D print was deemed acceptable. Participants did indicate a desire for a darker brown colour (to match skin colour) than the black colour that the 3D printed device was prepared in. Some also remarked that the 3D printed device was lighter in weight than the three other devices.
The participants (
n = 17) were also asked about what activities they felt they could perform with the hand. This was also interpreted by some as what activities they would like to perform. Participants indicated that any device that would allow them to earn an income would be beneficial. In addition to performing tasks indoors (utensil manipulation, crafts, etc.) many of the participants were also from areas that performed small-scale farming, rearing animals, and general labouring. Similar feedback was received in Co-design 1, suggesting these were consistent desires and concerns that needed to be addressed. As 75% of the population of Uganda is rural [
15], farming activities are common and more likely to represent the population of limb absent Ugandans. The fact that the population was reflected in those that participated in the co-design activities meant that accomplishing the ADLs with the prehensor design could have a larger impact.
4. Designing the Prehensor
The prehensor terminal device was designed to be used without a cable-operated input. This sets it apart from the usual body-powered devices and it is better described as an ‘activity specific prosthetic tool’. An internal extension spring provides the closing action between the fixed jaw and thumb (i.e., mobile jaw). This creates the gripping force around objects and utensils. The voluntary-opening device has two modes of operation to open and grasp an object.
The first is a push-on/pull-off actuation that promotes more active and spontaneous usage. The device is pushed on to a handle (e.g., shovel handle, bicycle handlebar) with a downward and lateral force. The projected tip of the thumb allows the user to push against a surface to force the thumb to rotate outward, allowing a handle to enter the interior of the device. This mode of operation is seen in some existing devices, including the JAWS and L’iL E-Z Infant Hand (Fillauer TRS), though the prehensor’s surface finish lacks the same level of friction as these two commercial devices, so it may require some practice to master this input.
The pull-off function is achieved by pushing the prehensor forward in relation to the handle it is grasping, to move the handle out of the hook area. The device is then moved laterally to create a force against the thumb, forcing it open. The prehensor can then be pulled off with ease (
Figure 4).
The second mode of operation involves a lever, herein referred to as a ‘trigger lever’, concealed inside the mobile jaw. This novel design for operation requires the user to reach over with their opposite side and push down on a small, exposed section of the trigger lever to rotate the entire body out of the thumb cavity. The trigger lever has a rotation of approximately 60 degrees, after which point it encounters a hard stop and any further force causes the thumb to rotate around its pivot within the fixed jaw (
Figure 5).
In the majority of locations, unilateral loss is much more common in Uganda and so the terminal device design was aimed at this group of users [
11]. However, the trigger lever can be operated by the opposite side as long as the level of amputation permits an individual to rotate out and pull back on the trigger lever.
As the trigger lever itself is only 10 mm in width and is transmitting all the force to counter the closing force of the spring (to open the device), the 3D printing material chosen for the prosthetic prehensor needs to be able to withstand this force. The material must also be able to lift a jerry can filled with 20 L of water without failure and be printed on the same Prusa 3D printer as the passive hand.
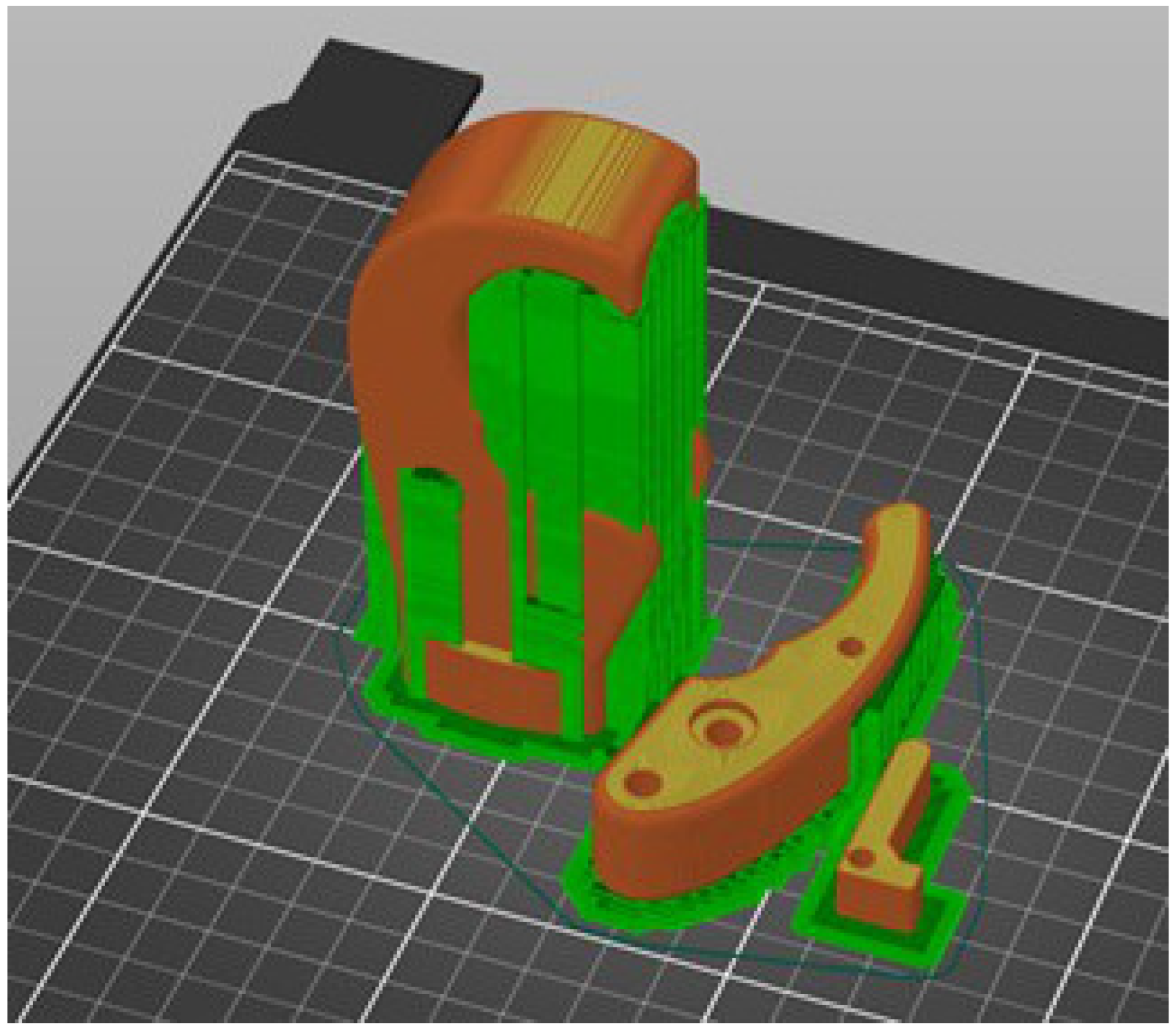
The filament chosen for the prosthetic prehensor was Prusament PC, a polycarbonate material also made by Prusa. This particular polycarbonate (PC) provides a durable, impact and temperature resistant print, that is not prone to wear (compared to other 3D print materials). It has a Shore hardness of 79D. The prototype was printed solid (full thickness) at the University of Portsmouth. The fixed jaw was printed upright (same orientation as passive hand) alongside the thumb and trigger lever which were printed on their sides (
Figure 6). This required approximately 16 h to print. The internal hardware (spring, nuts, bolts) were chosen from rust and corrosion resistant materials and the device was then assembled for testing.
Given the ADLs that this device would be subject to, the likely failure mode would be when the device experienced a high bending stress or high shock (shovel into ground). The properties of the PC material that were prioritized were the flexural strength and impact resistance. These material characteristics set PC apart from other 3D printing materials such as PLA, ABS, ASA, PETG, and Nylon/polyamides. Tough PLA, a proprietary material made by Ultimaker (Ultimaker B.V., Utrecht, The Netherlands) also provides a similar strength profile (impact and flexural strength) as polycarbonate material and can be considered for this application, provided the 3D printer can achieve the necessary printing temperature.
The overall dimensions as well as exterior and interior profiles of the prehensor dictate how effective the device can be at manipulating, gripping, and interacting with objects. The various shapes (curves, depressions, protrusions) contained within the overall device footprint, influence how an object can be held in different areas and how the prehensor can lock around handles to provide a secure grip. At times the dimensions and shapes that are meant for achieving one task can impose on the ability to perform a second task. Feedback from priorities received in Co-design 1 assisted in finding this balance. It is assumed that all of the six ADLs will not be achieved with this first prototype, but the intention was (and remains) to show the potential users what is achievable to continue the design partnership in future co-design activities.
The overall form factor for the prehensor when closed is within a footprint of 107 × 64 × 29 mm (4.25 × 2.5 × 1 1/8 inches). The current prototype was printed in orange, but prototypes destined for Uganda will be printed in black.
4.1. Using ADLs to Inform Design Features
The six priority ADLs used in the Uganda workshops directly influence the design features of the prosthetic prehensor. Below is a description of some of the ADLs to illustrate how they inform the design.
4.1.1. Lifting a 20 L Jerry Can
Fetching water using a 20 L military-style diesel jerry can (taller than it is wide) is very common in Uganda. Though many different styles and shapes exist around the world, the F4P team used one that resembled the handle area of the Ugandan varieties as closely as possible. This handle opening is narrower and has less space to manoeuvre the end of the prehensor into the opening. There is also a limited space underneath the device before the top of the main body. This is important to note, as when using the push-on functionality to open the prehensor, there is a forward distance that is travelled by the hooked area before the handle enters the interior.
Figure 7 shows the jerry can used as the model for design.
The larger inner profile was shaped based off the diameter of the jerry can handle and to ensure that as much of the handle as possible was in contact with the hooked area. Though designed for a load of 20 L of water (approximately 20 kg), anecdotal evidence from prosthetists suggested that the majority of transradial users would carry up to 5 kg, stopping to rest frequently. The 3D printing material was chosen to provide a sufficient factor of safety to accommodate for the dynamic inertial loads when walking or lifting the load quickly from the ground. This will also ensure that lighter carrying tasks (e.g., grocery bags) can be performed without failure of the prosthesis.
The inside profile of the device has two areas for holding handles. The smaller interior profile was designed to allow for smaller diameter broom handles to be grasped and controlled (
Figure 8).
Other ADLs (e.g., gardening) involve making use of the inner profiles, but need testing in the field to ensure grip and balance can be maintained when imparting an impact force (swinging a shovel/garden hoe).
4.1.2. Peeling Matoke
Matoke is a green fruit, indigenous to southwest Uganda, and a staple of the country’s cuisine. Though similar to a Plantain, a Matoke needs to be firmly gripped and peeled with a knife or machete. Any cylindrical fruit or vegetable is often peeled by holding it within the terminal device, peeling a section, releasing and rotating the fruit, and peeling another section. The task is made difficult because there is limited regulation possible by the user of the gripping force which would provide the counter force to the peeling direction when the knife is drawn towards the body. Creating a counter force is necessary for stability during peeling. For this reason, a cylindrical depression was designed into the fixed jaw where the end of the fruit can rest, holding it stable when peeling. This is referred to as the ‘Matoke nook’. For added stability, the thickness of the jaws can be increased, but this is at the expense of less of the fruit being exposed for peeling. When a user is trained to do this task, they will be instructed to expose the trigger lever, then pick up the knife and fruit with their opposite side, in this order. Using their smallest finger, they can then pull down on the lever and insert the fruit into the nook and release and proceed to peel. This ADL is illustrated below in
Figure 9 using a Zucchini.
4.1.3. Holding Utensils
A passthrough hole was added within the Matoke nook to allow the prehensor to hold utensils or long thin-handled tools (as shown in
Figure 10).
The utensil is retained using three points of contact: the tip of the thumb, the end of the hooked area in the fixed jaw, and the passthrough. This was designed to secure the handles of a variety of kitchen utensils that have different widths of handles. The handles also do not have to go all the way through the fixed jaw. As long as the handle end fits securely in the Matoke nook and there is enough pressure from the spring force, the tool can be used.
4.2. Initial Testing of the Devices
The passive hand and the prehensor have experienced some basic testing to ensure that they will be able to perform their functions adequately when they are field tested in Uganda. If the devices fail or tear, there will be a loss of confidence in the device by the user and they may not wish to continue to participate in the development. One consequence of the failure is it can be seen as putting their disability more on display. For this reason, the devices must be sufficiently robust.
Figure 11 shows a series of images of the passive hand’s compliance, friction, and usage around the home.
Initial testing of the passive hand (which now included a standard ½-20 bolt for socket attachment) proved to be successful and it is now being printed locally in Uganda. The flexibility may require fine tuning some of the print parameters (speed, infill percentage) but these can now be performed at Makerere University.
The prehensor prototype was tested for its ability to grip handles and absorb impact forces.
Figure 12 shows the prehensor (affixed to a forearm simulator device) gripping a bicycle handle and garden rake. Removing the prehensor from the bicycle handle is done with the pull-off technique. This is made easier when the bicycle handle is grasped towards the outside.
It was noticed that impact forces from long-handled garden equipment could not be transferred to the prehensor as it experienced varying degrees of gripping ability. A garden rake being used to move light weight leaves did not pose a problem. A garden shovel used to lift heavier loads caused the prehensor to slide along the handle during the task especially on impact with the soil.
Figure 13 presents this ADL. The lack of a secure grip on the handle results in a loss of control by the user, making it difficult to manage the task. This also meant that impact forces could not be assessed in any meaningful way.
The prehensor was also tested to ensure the hooked end of the fixed jaw could withstand a loading force without experiencing failure. To test this carrying capacity, the jerry can was filled with water for a total load of 12.9 kg. The prehensor was used by a team member to grasp around the handle and lift the jerry can. It was then carried at a comfortable walking pace for approximately one minute
Figure 14. It was noticed that in the first few steps, as the arm and jerry can swung, the prehensor shifted to the back of the handle as this was the most stable position. There was no further shifting of the prehensor relative to the handle afterwards which is likely due to the position internally where the water line was level.
The jerry can was then filled with water to 20 L and lifted straight up (no walking) for approximately ten seconds and then brought back to the ground (see
video in Supplementary Material). This was then repeated for another 10 s. The prehensor showed no signs of failure, warping, or damage. This is important as the hooked area has the smallest cross section of the fixed jaw but is designed to lift the biggest loads.
The overall profile of the two designs is unlikely to change in terms of size. This is often a challenge when attempting to provide single solutions to a range of potential users. Prostheses tend to appear larger than a similar sized natural hand. There was no feedback suggesting an aversion to the size of the passive hand during co-design 2. For comparison the two devices are show in
Figure 15 next to an adult male hand.
The final weight of the passive hand and prehensor prototypes were 200 g and 155 g respectively. This is inclusive of all the internal hardware in addition to the 3D printed parts.
5. Discussion
Throughout the initial iterations of designing the passive hand and prehensor a few benefits were noted that are important when meeting the challenges of designing for LMICs. Ensuring that the same or similar printers and filaments are at each location (e.g., UK and Uganda) allows robust and efficient product development. An inherent flaw in the 3D printing process is that although superficially straightforward, there are a significant number of parameters in the 3D printing process that need to be established and these need to be carefully replicated when printing devices at more than one location. The speed of print, the temperature of extruders and print beds, cooling fans are all considerable factors when achieving a successful print. Being able to share printer settings, model files, the difference object orientation can make, and other technical points, can allow for a coordinated approach to working out errors and build a level of trust across centres. This is important as it takes a level of coordination to organize workshops in Uganda. If a workshop can only be held every six months, the prototypes need to be much further along as transporting individuals to a central location often requires sourcing funding and scheduling trained staff.
During the co-design activities, it was noted that having local organizers who spoke the local language prevented a potential communication barrier. There are several local languages spoken in Uganda and depending on the particular location of the workshop there might be a local business language and a local common language. It is crucial that this be observed as part of the planning process, as it should not be assumed that anyone speaks English or Swahili, Uganda’s official languages. Being able to communicate in the local language made participants comfortable sharing their personal stories and situations. This feedback is important to understanding what activities a person is undertaking, what they are willing to try, and what they will avoid doing. This directly impacts the design of any prosthetic solution.
The passive hand required approximately 40 h to print in the UK. This represents a power supply stability that cannot be assumed in LMICs. Efficiencies need to be found in the printing parameters to reduce the print time, while maintaining an acceptable quality for the hand, or other sources of uninterrupted power supply need to be explored, as power outages remain a reality in Uganda. For both the passive hand and the prehensor (16 h to print), a shorter uninterrupted printing time (e.g., 12 h) should be pursued. Long printing times could result in the device becoming cost prohibitive (cost of technician, energy, etc.). Shorter printing times may make it possible to stagger worker shifts to cover the entire print time and respond/resume an interrupted print.
Testing the prehensor device for its ability to absorb shock could not be successfully performed. As testing with the shovel handle had shown, maintaining a grip on the handle in one location is necessary in order to transmit the impact forces successfully. The current prehensor prototype’s minimal gripping ability prevents this from occurring. A material offering better grip to the larger inner profile of the prehensor may need to be added, or a material may need to be wrapped around garden equipment handles to ensure the grip, similar to the bicycle handles.
Specifically with regard to the prosthetic prehensor, the effect of training the potential user on how to use this device is an integral part of its success and acceptance. This may be best accomplished by having participants attend a workshop activity where they will be provided with the terminal device (and socket/suspension) and then trained on how to employ the device to accomplish the ADLs mentioned above. This is important as the language barrier may exist depending on the region, and technology to watch an instructional video may not be accessible.
The co-design workshops proved to be an effective means by which users could input to the designs as they evolved. However, the challenges of a geographically very dispersed team, and Covid- and climate-emergency-driven limits on flying, made the delivery logistics difficult. The success was down to the enthusiastic local team and partnerships with clinicians and users in Uganda.
Future development will require updating the prototypes and repeating the field testing. The tests described above were performed in a high income country, but field testing in the LMIC is necessary to account for the different effects of climate (perspiration, dryness), soil composition (ADL with shovel), various handles of tools/utensils, and the community members reaction to an individual wearing and using the prosthetic devices.
6. Conclusions
This study shows the potential for the use of 3D printing in the production of prosthetics in Low and Middle Income Countries, however it also demonstrates that this technology alone is not sufficient to benefit users in these countries. It is only a technique to get to the goal of creating a solution for potential users. Any preconceptions from the team in the UK and USA needed to be re-evaluated and the knowledge and experience of team members based in Uganda directed the design process. This is the only way to create a solution that will be welcomed and used by those with a limb difference. It is important to stress that the solution created is appropriate for Uganda only. Simple adoption of the same design in another country, even in sub-Saharan Africa should be avoided, without some involvement of the locals to guide changes/adjustment.
Author Contributions
Conceptualization: A.H., P.K., B.M., R.S., L.K. and D.H.; Methodology: A.H., P.K., B.M., R.S., W.K., L.K. and D.H.; Writing—original draft: A.H., P.K., B.M. and R.S.; Writing—review and editing: A.H., P.K., B.M., R.S., W.K., L.K. and D.H.; Project administration: L.K.; Funding acquisition: L.K., P.K., D.H. and R.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Engineering and Physical Sciences Research Council and National Institute for Health Research, grant number EP/R013985/1.
Institutional Review Board Statement
Not applicable. The prototype devices were for material research purposes only, and not connected to a socket worn by any participant.
Informed Consent Statement
Not applicable. Information used to design devices was done through a PPIE framework and no individual data has been shared in this work.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank Bob Radocy and Sam Hale at Fillauer TRS for guidance on how to structure the questions in Co-design 1 with regard to terminal devices and for sharing their experience with similar processes in other countries. They also thank the volunteers for their time and insights.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ABS | Acrylonitrile butadiene styrene |
| ADLs | Activities of Daily Living |
| ASA | Acrylic Styrene Acrylonitrile |
| CAD | Computer Aided Design |
| F4P | Fit for Purpose project |
| LMIC | Low and Middle Income Countries |
| PC | Polycarbonate |
| PETG | Polyethylene Terephthalate Glycol |
| PLA | Polylactic acid |
| PPIE | Patient and Public Involvement and Engagement |
| TPE | Thermoplastic Elastomer |
| TRS | Therapeutic Recreational Services |
| UCL | University College London |
References
- Ten-Kate, J.; Smit, G.; Breedveld, P. 3D-printed upper limb prostheses: A Review. Disabil. Rehabil. Assist. Technol. 2017, 12, 300–314. [Google Scholar] [CrossRef] [PubMed]
- Kyberd, P. Making Hands: A History of Prosthetic Arms; Academic Press: Kidlington, UK, 2021. [Google Scholar]
- Ikeda, A.J.; Grabowski, A.M.; Lindsley, A.; Sadeghi-Demneh, E.; Reisinger, K.D. A scoping literature review of the provision of orthoses and prostheses in resource-limited environments 2000–2010. Part two: Research and Outcomes. Prosthetics Orthot. Int. 2014, 38, 343–362. [Google Scholar] [CrossRef] [PubMed]
- Phillips, B.; Zingalis, G.; Ritter, S.; Mehta, K. A review of current upper-limb prostheses for resource constrained settings. In Proceedings of the 2015 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 8–11 October 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 52–58. [Google Scholar] [CrossRef]
- Fairley, M. The O&P Edge:3D Printing of Upper-Limb Prosthetics: Present Reality, Future Potential. Available online: https://www.oandp.com/articles/2015-11_01.asp (accessed on 17 January 2023).
- van der Stelt, M.; Verhulst, A.; Slump, C.; Papenburg, M.; Grobusch, M.; Brouwers, L.; Maal, T. Design and Production of Low-Cost 3D-Printed Transtibial Prosthetic Sockets. JPO J. Prosthetics Orthot. 2022. [Google Scholar] [CrossRef]
- Cabibihan, J.-J.; Alkhatib, F.; Mudassir, M.; Lambert, L.A.; Kwif, A.S.; Diab, K.; Mahdi, E. Suitability of the Openly Accessible 3D Printed Prosthetic Hands for War-Wounded Children. Front. Robot. AI 2021, 7, 594196. [Google Scholar] [CrossRef] [PubMed]
- Kenney, L.; Ssekitoleko, R.; Chadwell, A.; Ackers, L.; Donovan-Hall, M.; Morgado-Ramirez, D.; Holloway, C.; Graham, P.; Cockroft, A.; Deere, B.; et al. Prosthetics services in Uganda: A Series of Studies to Inform the Design of a Low Cost, but Fit for Purpose, Body Powered Prosthesis. Global Perspectives on Assistive Technology: Proceedings of the GReAT Consultation; World Health Organisation: Geneva, Switzerland, 2019; pp. 414–426.
- Donovan-Hall, M.; Kenney, L.; Howard, D.; Chadwell, A.; Hussaini, A.; Kyberd, P.; Ssekitoleko, R.; Mulindwa, B.; Ackers, H. A distributed approach to co-design of an upper limb prosthesis suitable for use in Uganda. Disabil. Rehabil. 2023; in preparation. [Google Scholar]
- Staats, T. The rehabilitation of the amputee in the developing world: A review of the literature. Prosthetics Orthot. Int. 1996, 20, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Huck, J.; Atim, P.; Moro, E.; Nirmalan, M. Prevalence and Spatial Patterns of Major Limb Loss in the Acholi Sub-Region of Uganda. Prosthesis 2022, 4, 369–382. [Google Scholar] [CrossRef]
- Muhumuza, M.; Bangirana, A. Indications and the changing pattern of amputations at a tertiary hospital in Uganda. A 10-year retrospective study. ResearchGate 2015. [Google Scholar] [CrossRef]
- Okello, T.R.; Magada, S.M.; Atim, P.; Ezati, D.; Campion, A.; Moro, E.B.; Huck, J.; Byrne, G.; Redmond, A.; Nirmalan, M. Major limb loss (MLL): An overview of etiology, outcomes, experiences and challenges faced by amputees and service providers in the post-conflict period in Northern Uganda. J. Glob. Health Rep. 2019, 3, e2019028. [Google Scholar] [CrossRef]
- Morgado-Ramirez, D.Z.; Nakandi, B.; Ssekitoleko, R.; Ackers, L.; Mwaka, E.; Kenney, L.; Holloway, C.; Donovan-Hall, M. The lived experience of people with upper limb absence living in Uganda: A qualitative study. Afr. J. Disabil. 2022, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, D.; Nakandi, B.; Ssekitoleko, R.; Mwaka, E.; Ackers, L.; Miodownik, M.; Kenney, L.; Holloway, C.; Donnovan-Hall, M. People with upper limb loss living in urban Uganda: Experiences and expectations regarding design and provision of prosthetic devices. Disabil. Rehabil. 2023; in review. [Google Scholar]
- Donovan-Hall, M.; Ostler, C.; Sann, R.; Metcalf, C.; Dickinson, A.; Kheng, S. Exploring the experiences of individuals and their families using prosthetic devices and services in Cambodia following lower limb amputation. Disabil. Rehabil. 2023; in preparation. [Google Scholar]
- Chadwell, A.; Kenney, L.; Howard, D.; Ssekitoleko, R.; Nakandi, B.; Head, J. Evaluating reachable workspace and user control over prehensor aperture for a body-powered prosthesis. IEEE Trans. Neural Syst. Rehabil. 2020, 28, 2005–2014. [Google Scholar] [CrossRef] [PubMed]
- Lancsar, E.; Louviere, J. Conducting discrete choice experiments to inform healthcare decision making. Pharmacoeconomics 2008, 26, 661–677. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The four terminal devices presented were: (A) Split hook, (B) Adept Prehensor, (C) CAPP hand, and (D) passive cosmesis.
Figure 1.
The four terminal devices presented were: (A) Split hook, (B) Adept Prehensor, (C) CAPP hand, and (D) passive cosmesis.
Figure 2.
Grasping a Kibbo basket with an overhand or underhand grip or supported from beneath. Any one of the four terminal devices presented in the co-design activity can achieve at least one of these configurations.
Figure 2.
Grasping a Kibbo basket with an overhand or underhand grip or supported from beneath. Any one of the four terminal devices presented in the co-design activity can achieve at least one of these configurations.
Figure 3.
The commercial terminal device (tan colour) and the 3D printed device (black) The passive hand required approximately 40 h to print. This 3D printed hand did not include a ½-20 threaded bolt for mounting to a prosthetic arm but served the purpose of Co-design2.
Figure 3.
The commercial terminal device (tan colour) and the 3D printed device (black) The passive hand required approximately 40 h to print. This 3D printed hand did not include a ½-20 threaded bolt for mounting to a prosthetic arm but served the purpose of Co-design2.
Figure 4.
Pull-off is achieved by moving the handle out of the prehensor’s hook area and pushing against the thumb from the inside to create the opening force.
Figure 4.
Pull-off is achieved by moving the handle out of the prehensor’s hook area and pushing against the thumb from the inside to create the opening force.
Figure 5.
Trigger lever is concealed inside thumb and is rotated outward when needed for opening the terminal device.
Figure 5.
Trigger lever is concealed inside thumb and is rotated outward when needed for opening the terminal device.
Figure 6.
Orientation of prehensor parts on the print bed.
Figure 6.
Orientation of prehensor parts on the print bed.
Figure 7.
The taller 20 L yellow jerry has a smaller handle opening than the red jerry can and was used to determine dimensions for the inner profile of prehensor.
Figure 7.
The taller 20 L yellow jerry has a smaller handle opening than the red jerry can and was used to determine dimensions for the inner profile of prehensor.
Figure 8.
Inner profiles provide the shape to lock around handles for controlled manipulation.
Figure 8.
Inner profiles provide the shape to lock around handles for controlled manipulation.
Figure 9.
Inserting a fruit into the Matoke nook for facilitating peeling.
Figure 9.
Inserting a fruit into the Matoke nook for facilitating peeling.
Figure 10.
The handle of the wooden spoon is pushed through the passthrough hole in the fixed jaw. The fixed jaw and thumb tip provide the force to secure the grip.
Figure 10.
The handle of the wooden spoon is pushed through the passthrough hole in the fixed jaw. The fixed jaw and thumb tip provide the force to secure the grip.
Figure 11.
Passive hand being tested for flexibility, friction, and opening a cabinet using the handle.
Figure 11.
Passive hand being tested for flexibility, friction, and opening a cabinet using the handle.
Figure 12.
Bicycle handle with rubber grip provides secure hold for prehensor. Long smooth handled garden equipment result in varying degrees of gripping success. A garden rake is easy to manoeuvre because it does not have to carry a heavy load, providing the user with a greater sense of control.
Figure 12.
Bicycle handle with rubber grip provides secure hold for prehensor. Long smooth handled garden equipment result in varying degrees of gripping success. A garden rake is easy to manoeuvre because it does not have to carry a heavy load, providing the user with a greater sense of control.
Figure 13.
Use of a garden shovel begins with an impact force (foot used to drive shovel into ground), proceeds to a lever action (prehensor is the fulcrum) and then a final lifting force. A lack of secure grip on the handle causes the prehensor to move to different location on the handle which creates uncertainty for the user.
Figure 13.
Use of a garden shovel begins with an impact force (foot used to drive shovel into ground), proceeds to a lever action (prehensor is the fulcrum) and then a final lifting force. A lack of secure grip on the handle causes the prehensor to move to different location on the handle which creates uncertainty for the user.
Figure 14.
The prehensor is used to lift a load of 12.9 kg. As the arm swings in the first few steps, the prehensor moves to a stable position towards the rear of the handle.
Figure 14.
The prehensor is used to lift a load of 12.9 kg. As the arm swings in the first few steps, the prehensor moves to a stable position towards the rear of the handle.
Figure 15.
From left to right: prehensor, passive hand, adult male hand.
Figure 15.
From left to right: prehensor, passive hand, adult male hand.
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}














