
A Retrospective Analysis on Marginal Bone Loss around Tilted and Axial Implants in Immediate-Loaded All-On-4 with a Long-Term Follow-Up Evaluation

 and
and
Abstract
:1. Introduction
2. Material and Methods
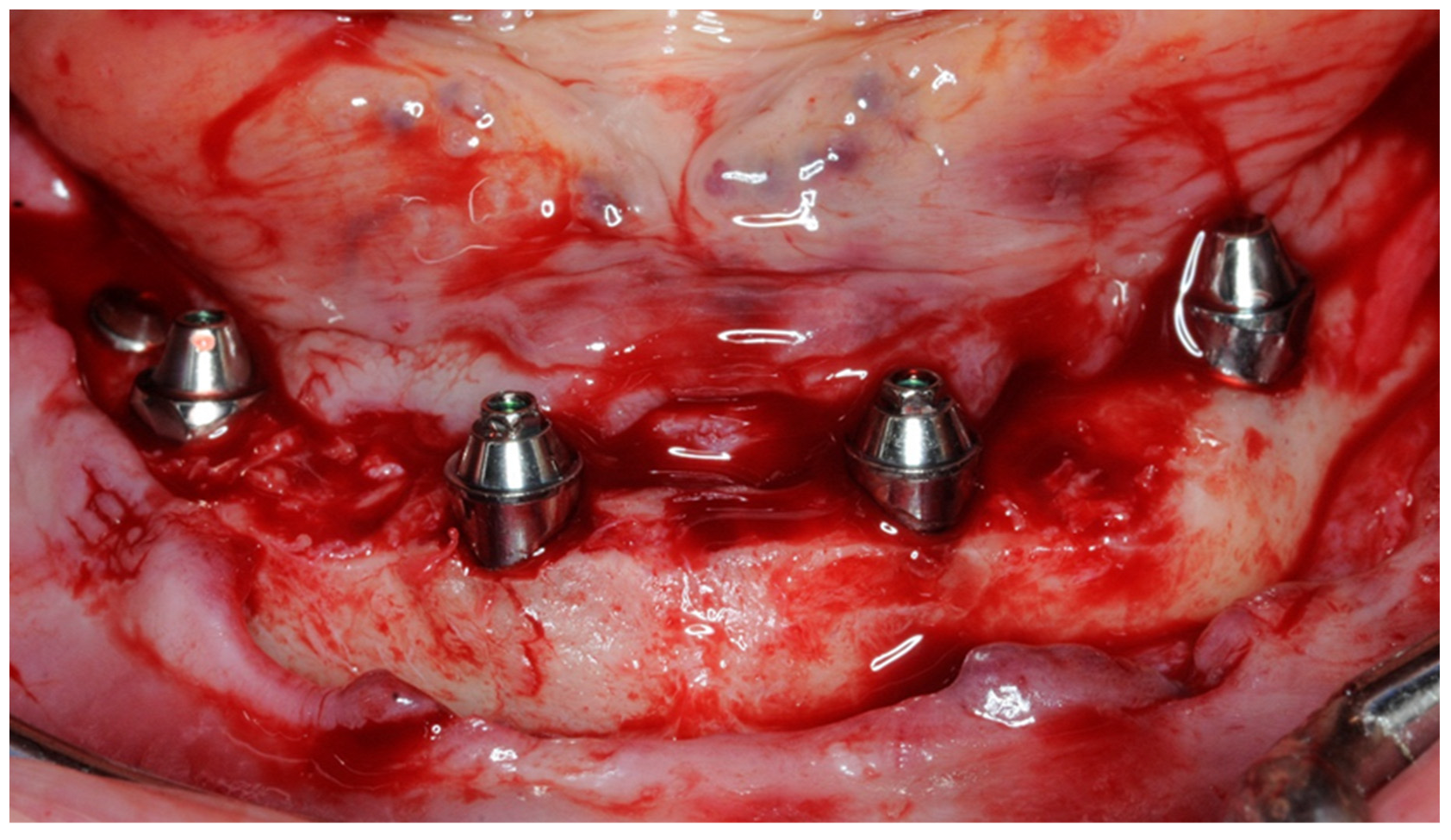
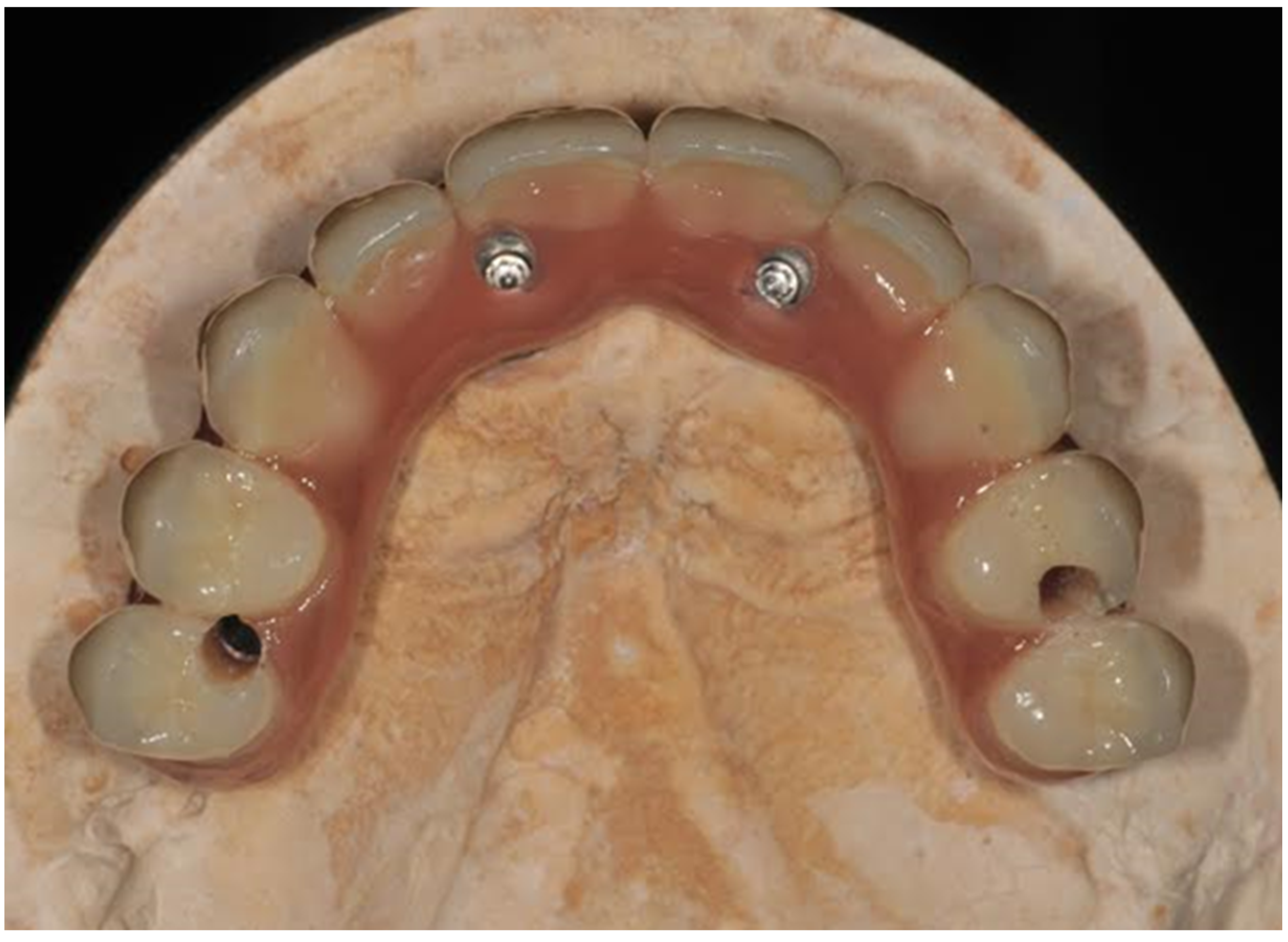
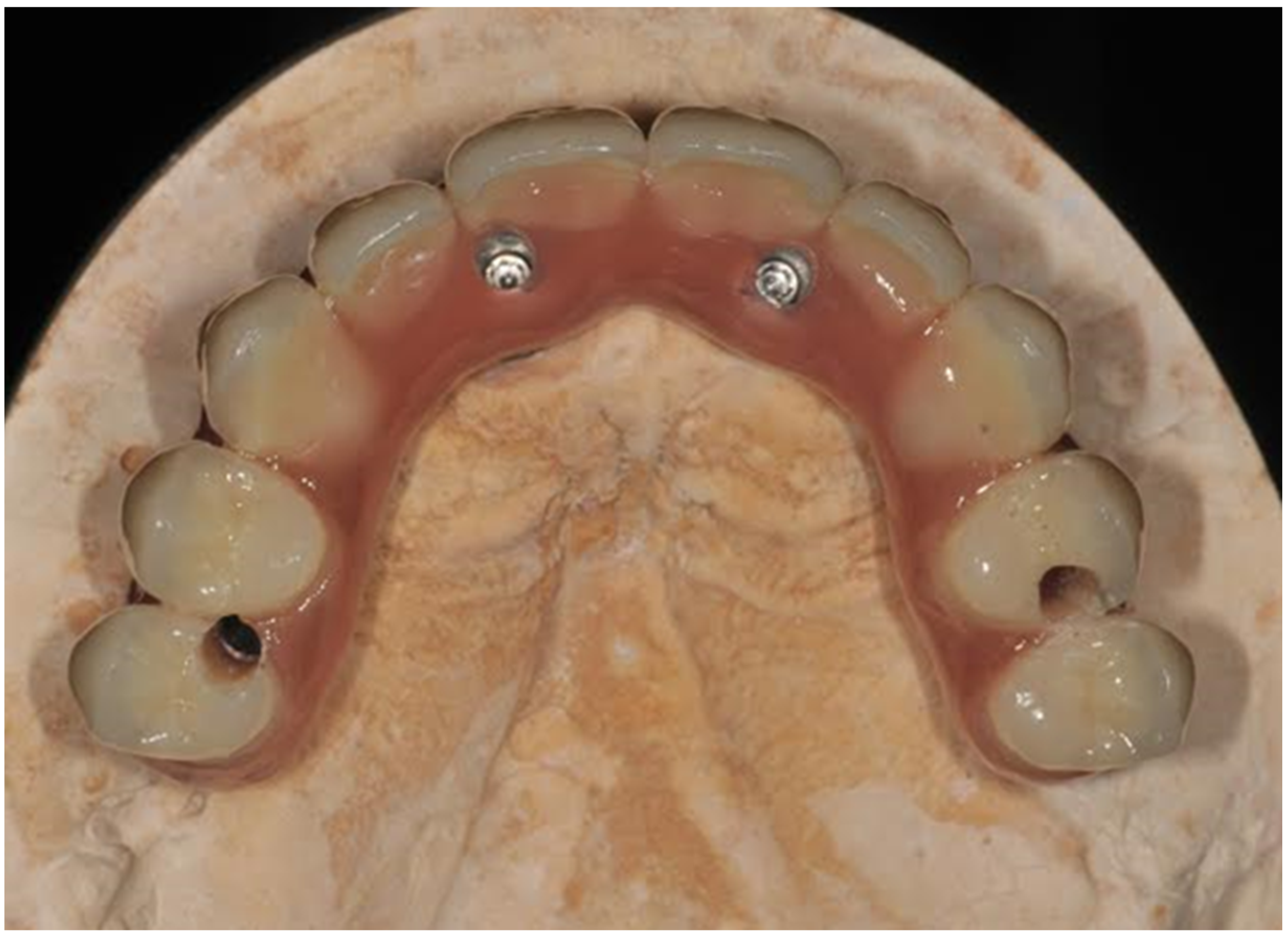
2.1. Patient Selection, Surgical and Prosthetic Procedure
- Presence of systemic pathologies that contraindicated surgery.
- Presence of untreated periodontal disease.
- Smokers > 10/die.
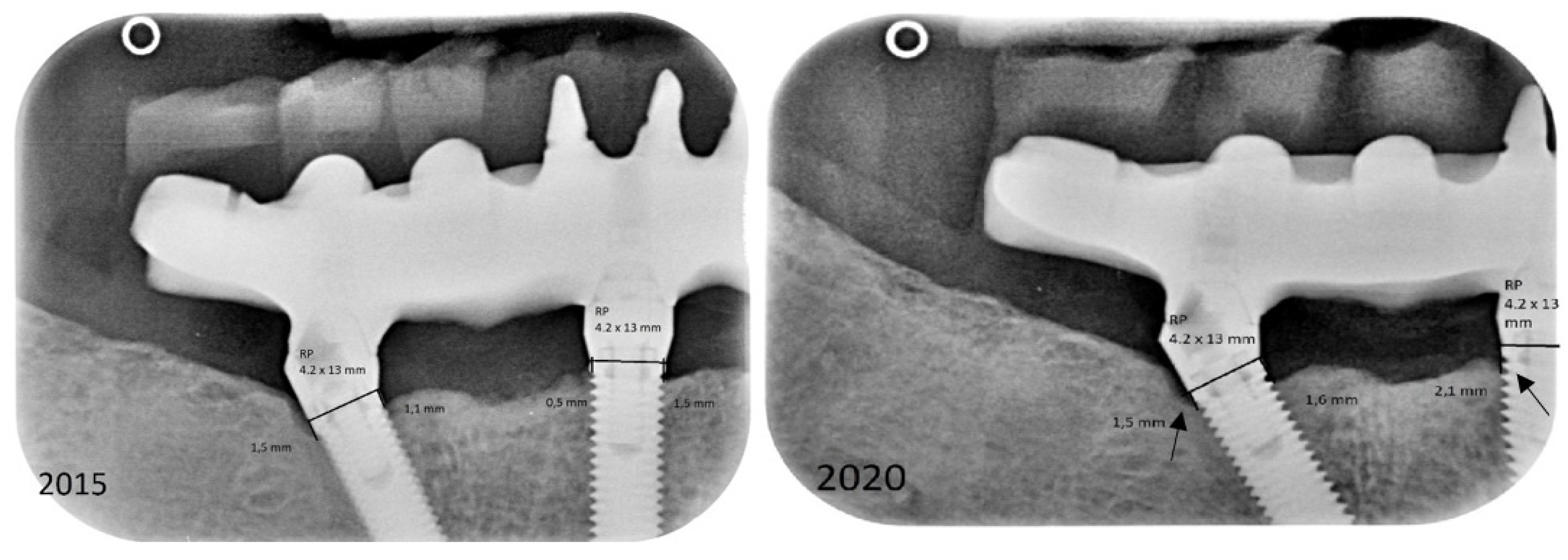
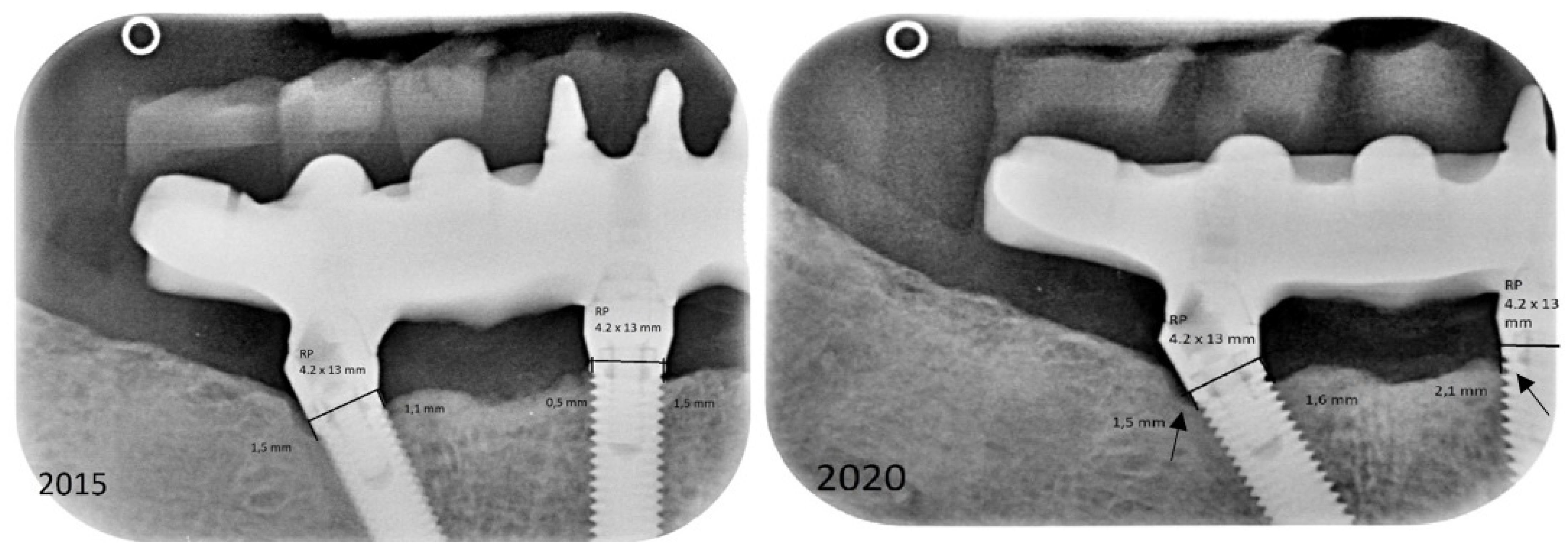
2.2. Data and Radiographic Assessment
2.3. Data Analysis
3. Results
3.1. Demographic and Clinical Variables
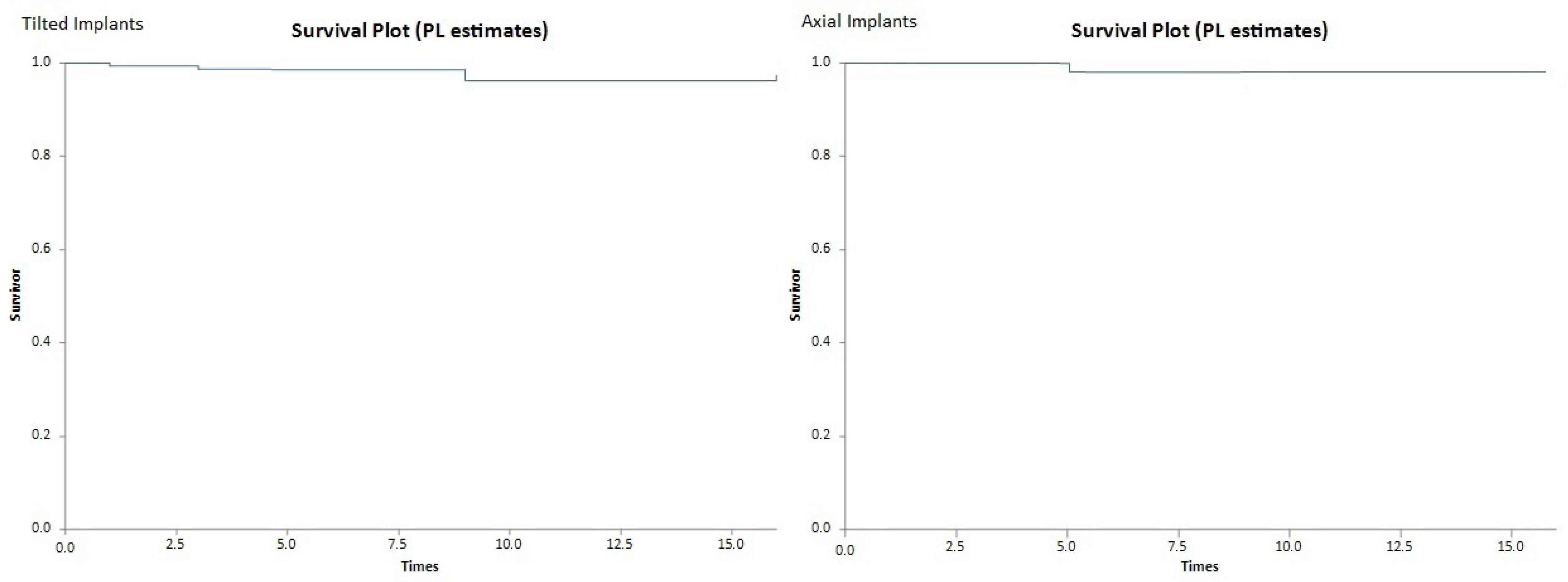
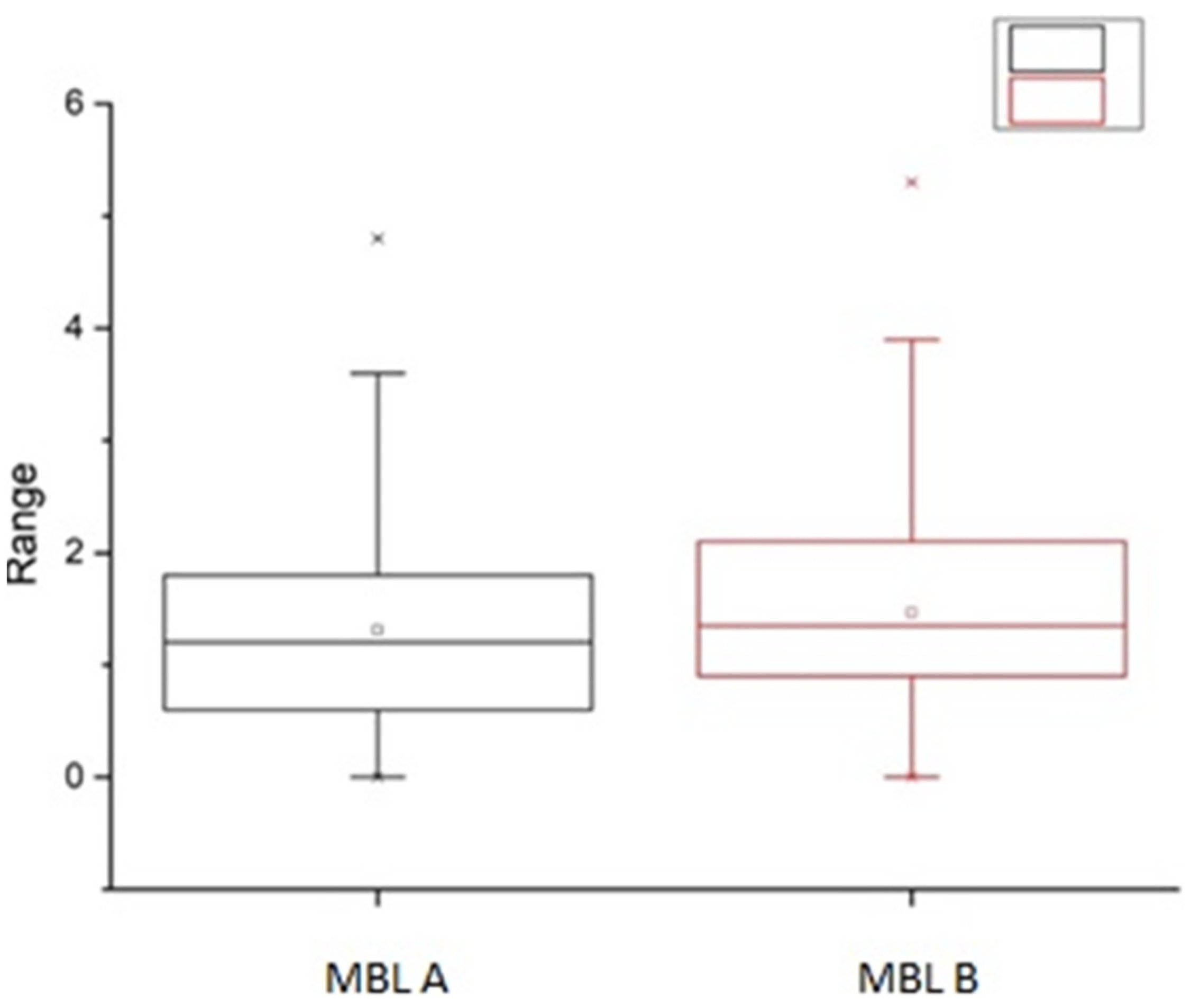
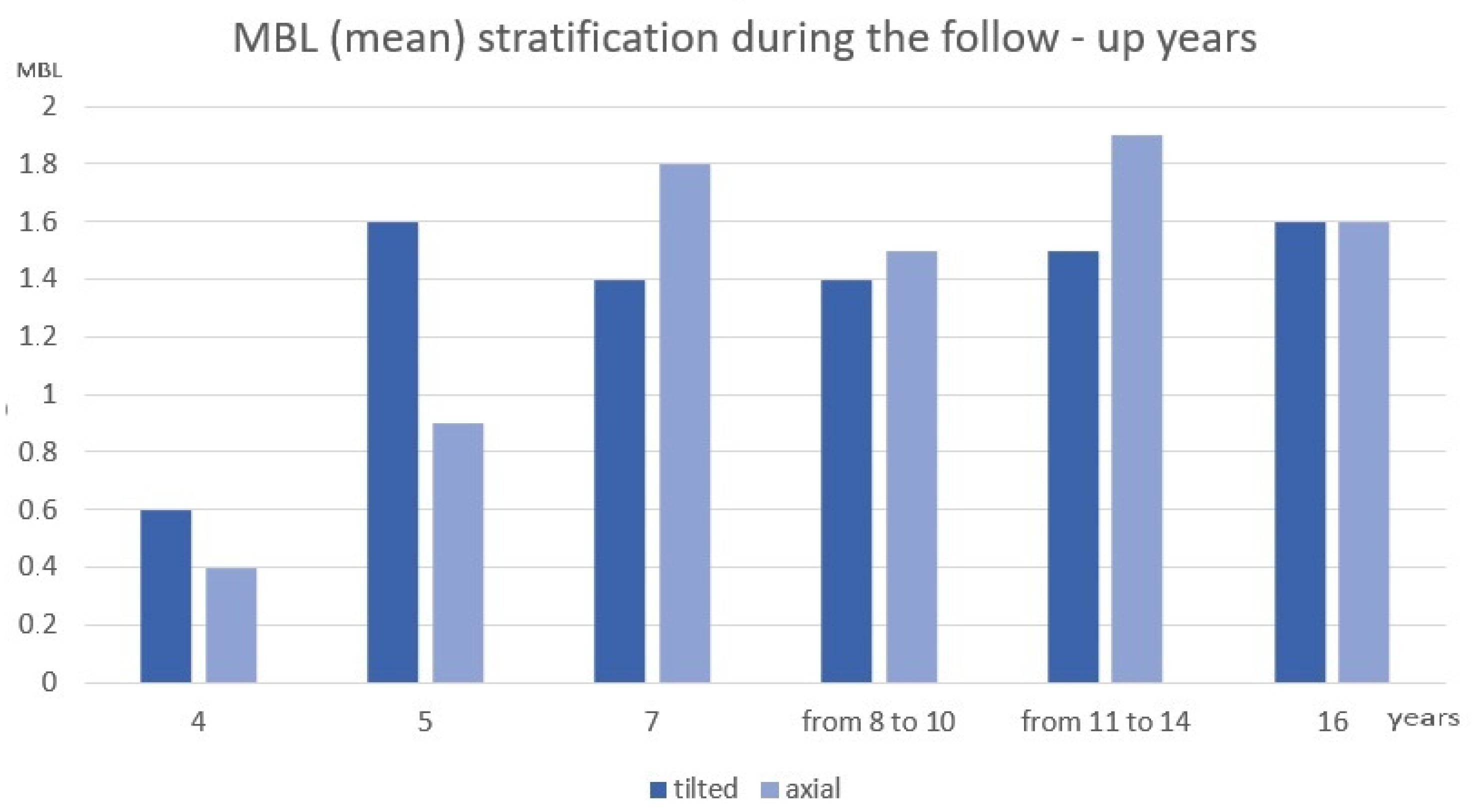
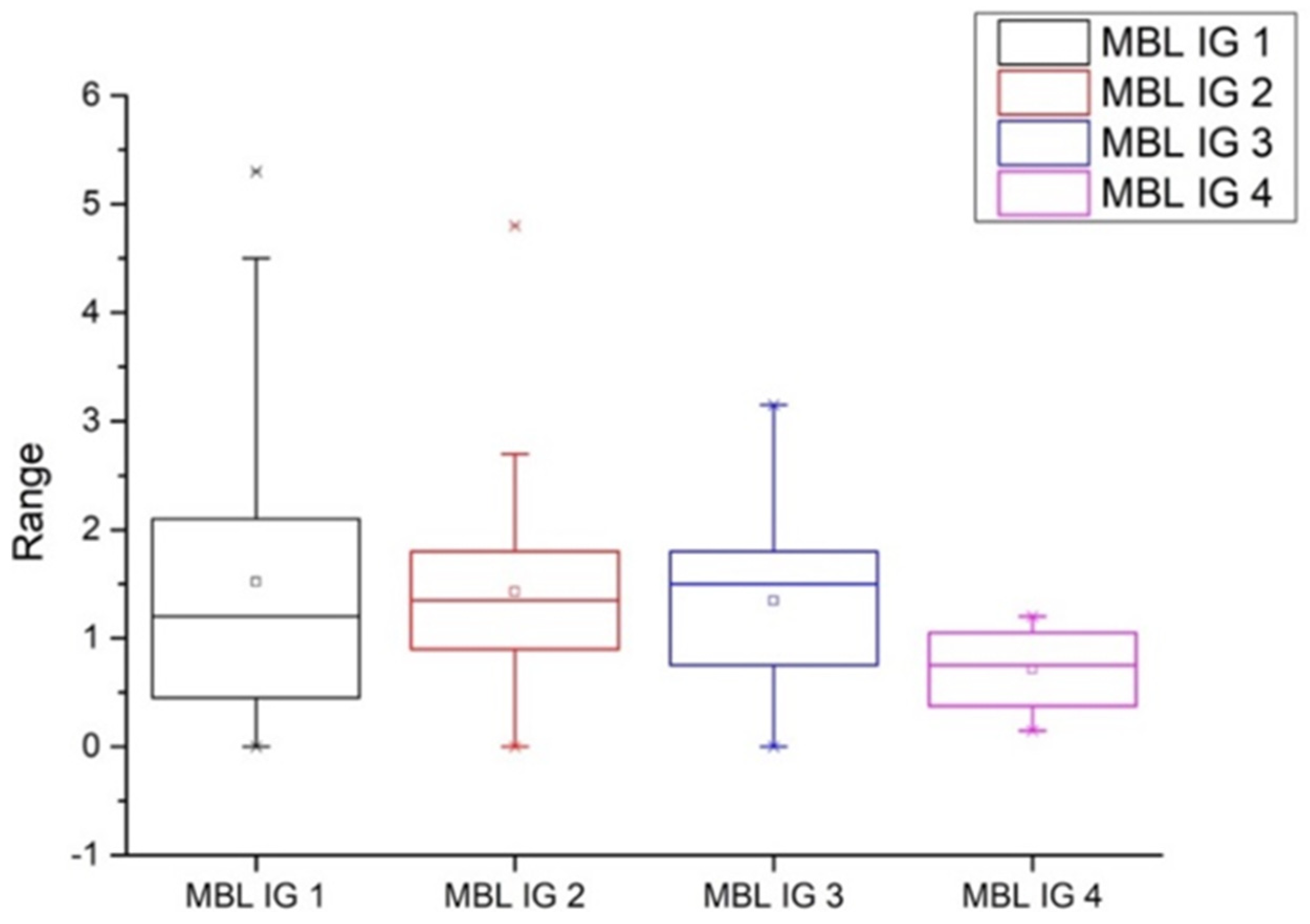
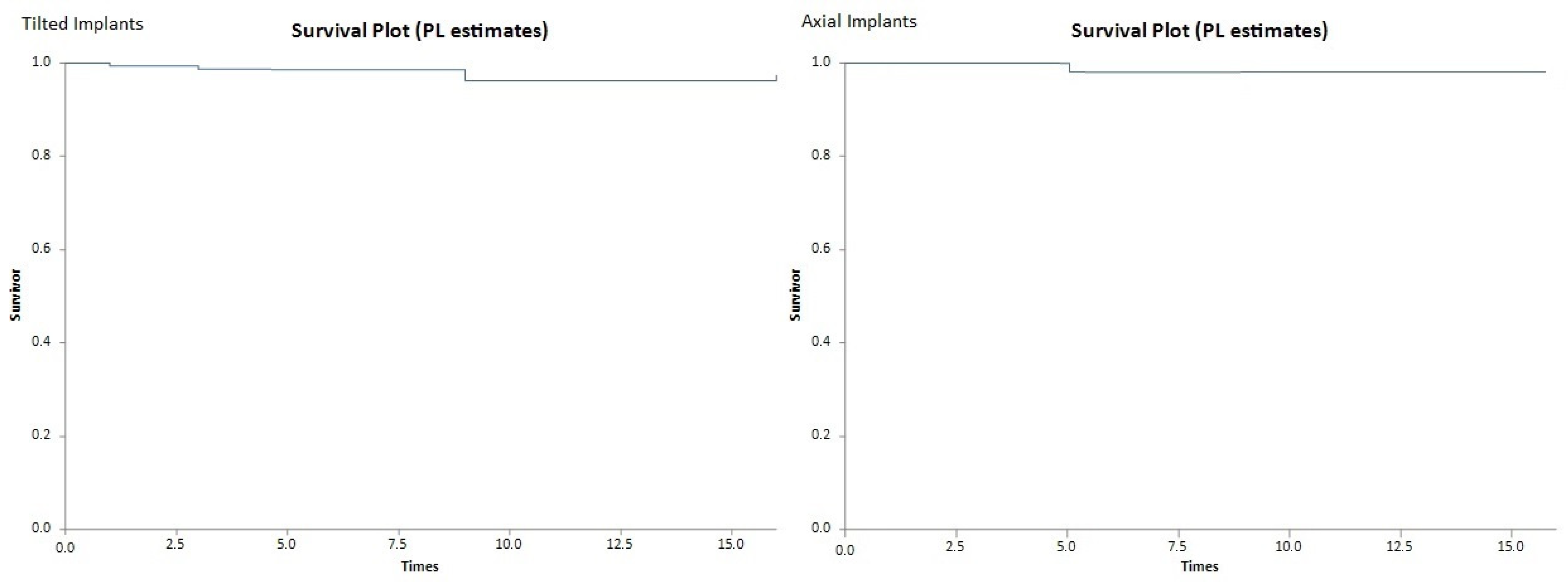
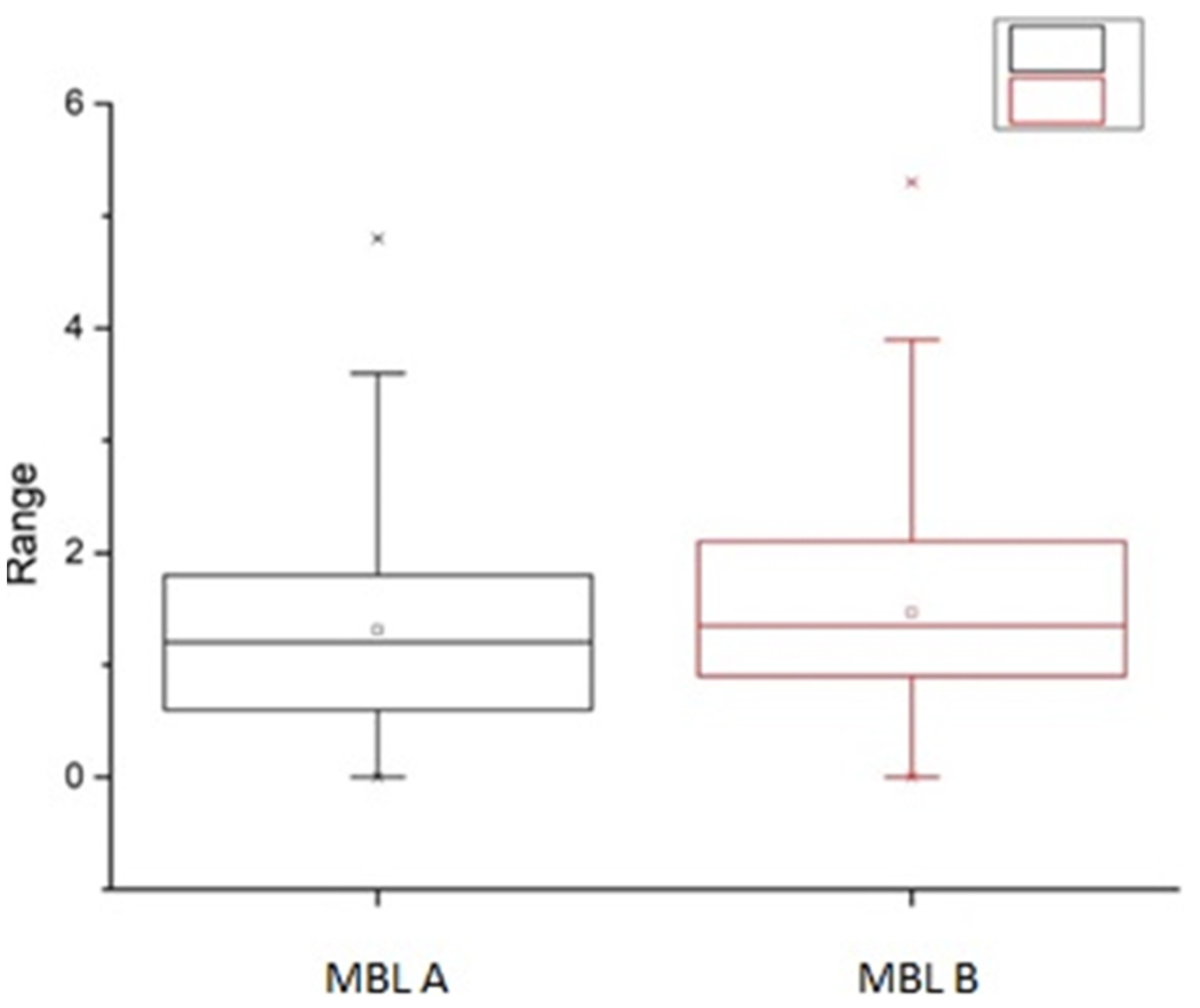
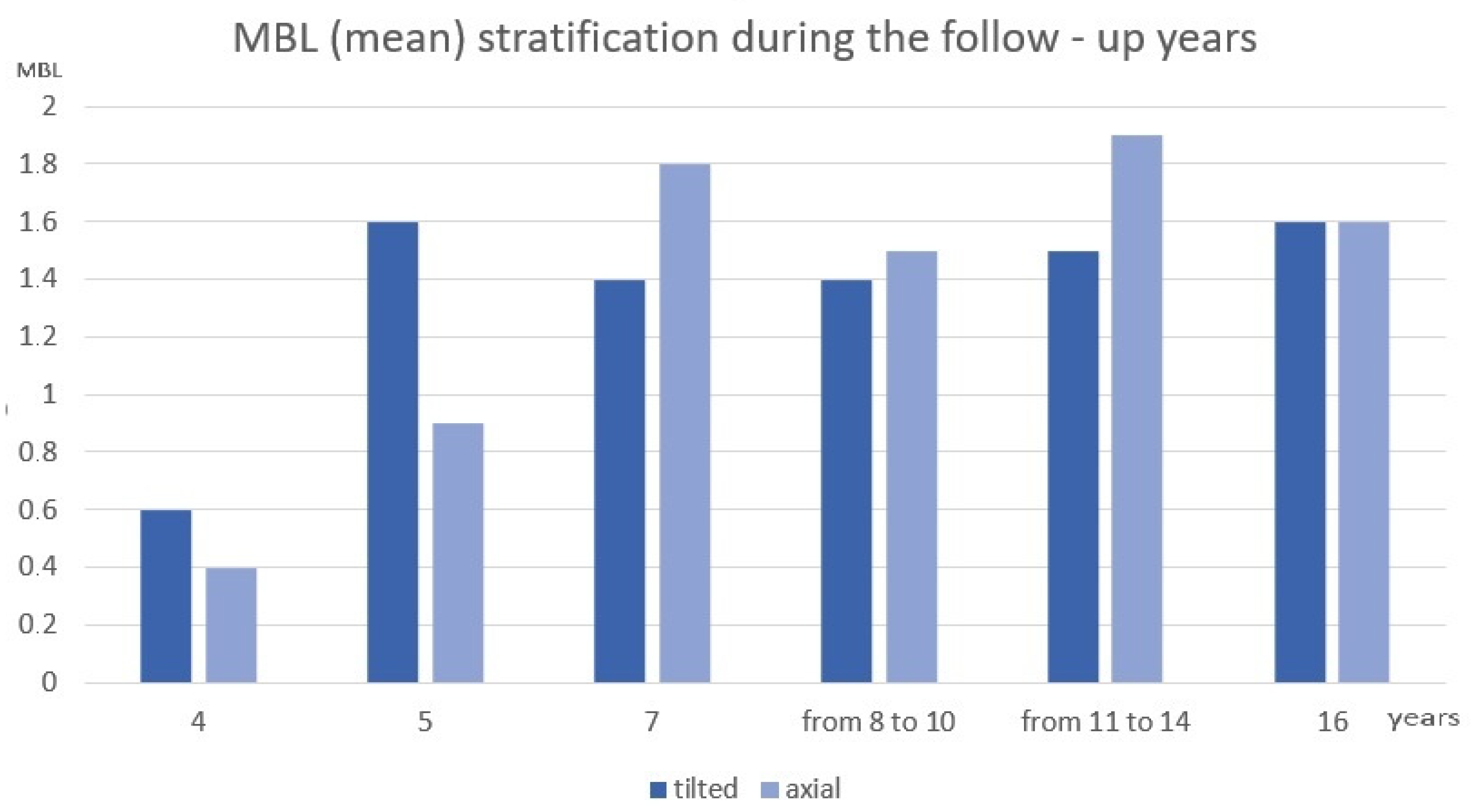
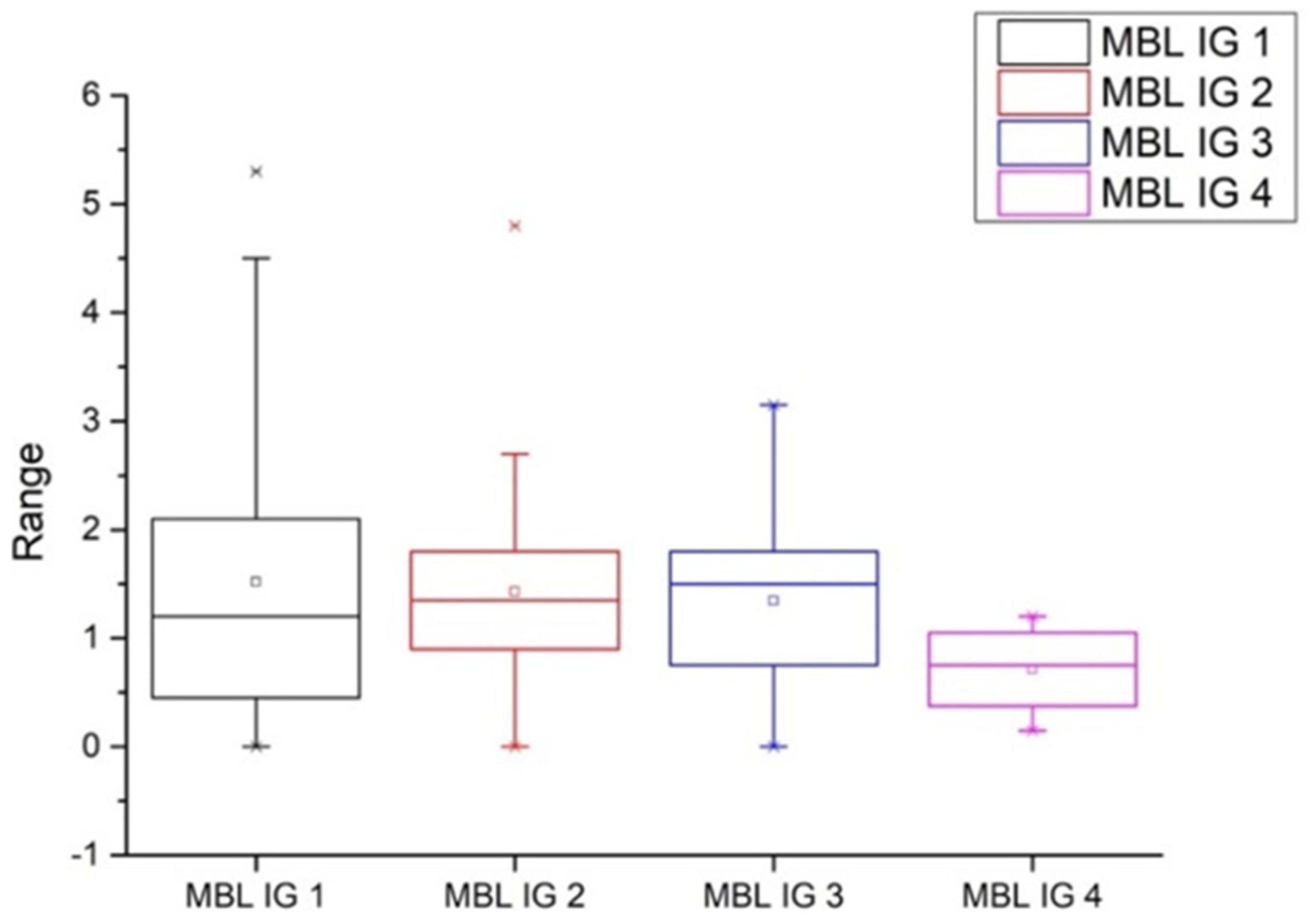
3.2. Radiographic Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jemt, T.; Johansson, J. Implant Treatment in the Edentulous Maxillae: A 15-Year Follow-Up Study on 76 Consecutive Patients Provided with Fixed Prostheses. Clin. Implant. Dent. Relat. Res. 2006, 8, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Åstrand, P.; Ahlqvist, J.; Gunne, J.; Nilson, H. Implant Treatment of Patients with Edentulous Jaws: A 20-Year Follow-Up. Clin. Implant. Dent. Relat. Res. 2008, 10, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Krekmanov, L.; Kahn, M.; Rangert, B.; Lindström, H. Tilting of posterior mandibular and maxillary implants for improved prosthesis support. Int. J. Oral Maxillofac. Implant. 2000, 15, 405–414. [Google Scholar]
- Aparicio, C.; Perales, P.; Rangert, B. Tilted implants as an alternative to maxillary sinus grafting: A clinical, radiologic, and periotest study. Clin. Implant Dent. Relat. Res. 2001, 3, 39–49. [Google Scholar] [CrossRef]
- Lazarof, S. Immediate-load implant quickens integration. Dent. Today 1992, 11, 44–45. [Google Scholar]
- Maló, B.R.; Miguel, N. “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: A retrospective clinical study. Clin. Implant Dent. Relat. Res. 2003, 5, 2–9. [Google Scholar] [CrossRef]
- Malo, P.; Rangert, B.; Nobre, M.D.A. All-on-4 Immediate-Function Concept with Branemark SystemR Implants for Completely Edentulous Maxillae: A 1-Year Retrospective Clinical Study. Clin. Implant Dent. Relat. Res. 2005, 7, s88–s94. [Google Scholar] [CrossRef]
- Bellini, C.M.; Romeo, D.; Galbusera, F.; Taschieri, S.; Raimondi, M.; Zampelis, A.; Francetti, L. Comparison of tilted versus nontilted implant-supported prosthetic designs for the restoration of the edentuous mandible: A biomechanical study. Int. J. Oral Maxillofac. Implant. 2009, 24, 511–517. [Google Scholar]
- Del Fabbro, M.; Ceresoli, V. The fate of marginal bone around axial vs. tilted implants: A systematic review. Eur. J. Oral. Implant. 2014, 7 (Suppl. 2), 171–189. [Google Scholar]
- Antonios, Z.; Bo, R. Lars Heijl Tilting of splinted implants for improved prosthodontic support: A two-dimensional finite element analysis. J. Prosthet. Dent. 2007, 97 (Suppl. 6), S35–S43. [Google Scholar]
- Erdem, K. Ozge Doganay Evaluation of Stress in Tilted Implant Concept With Variable Diameters in the Atrophic Mandible: Three-Dimensional Finite Element Analysis. J. Oral. Implantol. 2020, 46, 19–26. [Google Scholar]
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant Success, Survival, and Failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and periimplant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89 (Suppl. 1), S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.P.; Sutariya, P.V.; Pathan, M.R.; Upadhyay, H.H.; Patel, S.R.; Kantharia, N.D.G. Clinical success between tilted and axial implants in edentulous maxilla: A systematic review and meta-analysis. J. Indian Prosthodont. Soc. 2021, 21, 217–228. [Google Scholar]
- Agliardi, E.; Clericò, M.; Ciancio, P.; Massironi, D. Immediate loading of full-arch fixed prostheses supported by axial and tilted implants for the treatment of edentulous atrophic mandibles. Quintessence Int. 2010, 41, 285–293. [Google Scholar] [PubMed]
- Luca Francetti, D.; Romeo, D.; Spasari, C.; Tassera, C.; Folegatti, T.; Testori, M.; Basso, E.; Agliardi, M.; Del, F. Immediate rehabilitation of edentulous mandible by all-on-four technique. Ital. Oral. Surg. 2008, 7, 7–18. [Google Scholar]
- Francetti, L.; Cavalli, N.; Taschieri, S.; Corbella, S. Ten years follow-up retrospective study on implant survival rates and prevalence of peri-implantitis in implant-supported full-arch rehabilitations. Clin. Oral. Implant. Res. 2019, 30, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Francetti, L.; Romeo, D.; Corbella, S.; Taschieri, S.; Bsc, M.D.F. Bone Level Changes Around Axial and Tilted Implants in Full-Arch Fixed Immediate Restorations. Interim Results of a Prospective Study. Clin. Implant Dent. Relat. Res. 2010, 14, 646–654. [Google Scholar] [CrossRef]
- Cavalli, N.; Barbaro, B.; Spasari, D.; Azzola, F.; Ciatti, A.; Francetti, L. Tilted implants for full-arch rehabilitations in completely edentulous maxilla: A retrospective study. Int. J. Dent. 2012, 2012, 180379. [Google Scholar] [CrossRef]
- Apaza Alccayhuaman, K.A.; Soto-Peñaloza, D.; Nakajima, Y.; Papageorgiou, S.N.; Botticelli, D.; Lang, N.P. Biological and technical complications of tilted implants in comparison with straight implants supporting fixed dental prostheses. A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. 18), 295–308. [Google Scholar] [CrossRef]
- Simion, M.; Nevins, M.; Rasperini, G.; Tironi, F. A 13- to 32-Year Retrospective Study of Bone Stability for Machined Dental Implants. Int. J. Periodontics Restor. Dent. 2018, 38, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Ferrantino, L.; Tironi, F.; Pieroni, S.; Sironi, A.; Simion, M. A Clinical and Radiographic Retrospective Study on 223 Anodized Surface Implants with a 5- to 17-Year Follow-up. Int. J. Periodontics Restor. Dent. 2019, 39, 799–807. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Implants | |||
|---|---|---|---|
| Patients | 34 | ||
| N. of Rehabilitations | 39 | ||
| N. of implants | 156 | ||
| Maxillary rehab | 24 | ||
| Mandibular rehab | 15 | ||
| Overall | Group A | Group B | |
| Survival rate % | 97.4% | 96.2% | 98.2% |
| Success rate % | 77.6% | 80.8% | 74.4% |
| Failed implants n (%) | 4 (2.6%) | 3 | 1 |
| Peri-implantitis n (%) | 15 (9.6%) | 8 | 7 |
| MBL (mm) | ||
|---|---|---|
| Group A | Group B | |
| Implants | 1. (IQR 1.9–2.1) | 1.4 (IQR 0.6–1.8) |
| Maxillary | 1.4 (SD 0.7) | 1.6 (SD 0.9) |
| Mandibular | 1.3 (SD 1) | 1.5 (SD 1) |
| N. of Implants | Median (mm) | |
|---|---|---|
| IG1 | 56 | 1.2 (IQR 0.45–2.1) |
| IG2 | 48 | 1.35 (IQR 0.26–1.12) |
| IG3 | 28 | 1.5 (IQR 0.67–1.18) |
| IG4 | 4 | 0.75 (IQR 0.26–1.2) |
| Not Reported | 20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tironi, F.; Orlando, F.; Azzola, F.; Corbella, S.; Francetti, L.A. A Retrospective Analysis on Marginal Bone Loss around Tilted and Axial Implants in Immediate-Loaded All-On-4 with a Long-Term Follow-Up Evaluation. Prosthesis 2022, 4, 15-23. https://doi.org/10.3390/prosthesis4010002
Tironi F, Orlando F, Azzola F, Corbella S, Francetti LA. A Retrospective Analysis on Marginal Bone Loss around Tilted and Axial Implants in Immediate-Loaded All-On-4 with a Long-Term Follow-Up Evaluation. Prosthesis. 2022; 4(1):15-23. https://doi.org/10.3390/prosthesis4010002
Chicago/Turabian StyleTironi, Francesco, Francesco Orlando, Francesco Azzola, Stefano Corbella, and Luca Angelo Francetti. 2022. "A Retrospective Analysis on Marginal Bone Loss around Tilted and Axial Implants in Immediate-Loaded All-On-4 with a Long-Term Follow-Up Evaluation" Prosthesis 4, no. 1: 15-23. https://doi.org/10.3390/prosthesis4010002
APA StyleTironi, F., Orlando, F., Azzola, F., Corbella, S., & Francetti, L. A. (2022). A Retrospective Analysis on Marginal Bone Loss around Tilted and Axial Implants in Immediate-Loaded All-On-4 with a Long-Term Follow-Up Evaluation. Prosthesis, 4(1), 15-23. https://doi.org/10.3390/prosthesis4010002