
Ten Year Clinical and Aesthetic Outcomes of an Immediately Placed and Restored Implant in the Anterior Maxilla: A Case Report



Abstract
1. Introduction
2. Materials and Methods
- T0—Baseline/Implant placement.
- T1—Definitive crown placement.
- T2—1-year follow-up.
- T3—3-year follow-up.
- T4—5-year follow-up.
- T5—10-year follow-up.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Esposito, M.; Grusovin, M.G.; Polyzos, I.P.; Felice, P.; Worthington, H.V. Interventions for replacing missing teeth: Dental implants in fresh extraction sockets (immediate, immediate-delayed and delayed implants). Cochrane Database Syst. Rev. 2010, CD005968. [Google Scholar] [CrossRef] [PubMed]
- Den Hartog, L.; Huddleston Slater, J.J.; Vissink, A.; Meijer, H.J.; Raghoebar, G.M. Treatment outcome of immediate, early and conventional single-tooth implants in the aesthetic zone: A systematic review to survival, bone level, soft-tissue, aesthetics and patient satisfaction. J. Clin. Periodontol. 2008, 35, 1073–1086. [Google Scholar] [CrossRef] [PubMed]
- Khzam, N.; Arora, H.; Kim, P.; Fisher, A.; Mattheos, N.; Ivanovski, S. Systematic Review of Soft Tissue Alterations and Esthetic Outcomes Following Immediate Implant Placement and Restoration of Single Implants in the Anterior Maxilla. J. Periodontol. 2015, 86, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Pun, L.; Lau, K.Y.; Li, K.Y.; Wong, M.C. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. Clin. Oral Implants Res. 2012, 23 (Suppl. 5), 39–66. [Google Scholar] [CrossRef] [PubMed]
- Arora, H.; Khzam, N.; Roberts, D.; Bruce, W.L.; Ivanovski, S. Immediate implant placement and restoration in the anterior maxilla: Tissue dimensional changes after 2–5 year follow up. Clin. Implant Dent. Relat. Res. 2017, 19, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Martin, W.; Belser, U.C. Optimizing esthetics for implant restorations in the anterior maxilla: Anatomic and surgical considerations. Int. J. Oral Maxillofac. Implant 2004, 19 (Suppl. 7), 43–61. [Google Scholar]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score. Clin. Oral Implant Res. 2005, 16, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Noelken, R.; Moergel, M.; Kunkel, M.; Wagner, W. Immediate and flapless implant insertion and provisionalization using autogenous bone grafts in the esthetic zone: 5-year results. Clin. Oral Implant Res. 2018, 29, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Yang, Z.; Tan, J.; Chen, L.; Liu, H.; Yang, J. Immediate implant placement for a single anterior maxillary tooth with a facial bone wall defect: A prospective clinical study with a one-year follow-up period. Clin. Implant Dent. Relat. Res. 2019, 21, 1164–1174. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.S.; Buser, D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla—A systematic review. Int. J. Oral Maxillofac. Implant 2014, 29, 186–215. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.Y.K.; Rungcharassaeng, K.; Lozada, J.L.; Zimmerman, G. Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: A 2- to 8-year follow-up. Int. J. Oral Maxillofac. Implant 2011, 26, 179–187. [Google Scholar]
- Seyssens, L.; Eghbali, A.; Cosyn, J. 10-year prospective study on single immediate implants. J. Clin. Periodontol. 2020, 47, 1248–1258. [Google Scholar] [CrossRef] [PubMed]
- Fürhauser, R.; Mailath-Pokorny, G.; Haas, R.; Busenlechner, D.; Watzek, G.; Pommer, B. Immediate Restoration of Immediate Implants in the Esthetic Zone of the Maxilla Via the Copy-Abutment Technique: 5-Year Follow-Up of Pink Esthetic Scores. Clin. Implant Dent. Relat. Res. 2017, 19, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Arora, H.; Ivanovski, S. Immediate and early implant placement in single-tooth gaps in the anterior maxilla: A prospective study on ridge dimensional, clinical, and aesthetic changes. Clin. Oral Implant Res. 2018, 29, 1143–1154. [Google Scholar] [CrossRef] [PubMed]
- Arora, H.; Ivanovski, S. Clinical and aesthetic outcomes of immediately placed single-tooth implants with immediate vs. delayed restoration in the anterior maxilla: A retrospective cohort study. Clin. Oral Implant Res. 2018, 29, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Arora, H.; Ivanovski, S. Correlation between pre-operative buccal bone thickness and soft tissue changes around immediately placed and restored implants in the maxillary anterior region: A 2-year prospective study. Clin. Oral Implant Res. 2017, 28, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Noelken, R.; Oberhansl, F.; Kunkel, M.; Wagner, W. Immediately provisionalized OsseoSpeed Profile implants inserted into extraction sockets: 3-year results. Clin. Oral Implant Res. 2016, 27, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Cosyn, J.; Eghbali, A.; Hermans, A.; Vervaeke, S.; De Bruyn, H.; Cleymaet, R. A 5-year prospective study on single immediate implants in the aesthetic zone. J. Clin. Periodontol. 2016, 43, 702–709. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Soft Tissue Recession (in mm) | Bone Level Changes (in mm) | PES * | ||||
|---|---|---|---|---|---|---|
| Mesial Papilla | Midfacial | Distal Papilla | Mesial | Distal | ||
| T0 | - | - | - | - | - | 10 |
| T1 | 0.2 | −0.2 | 0.0 | 0 | 0 | 12 |
| T2 | 0.2 | −0.2 | 0.1 | −0.2 | −0.2 | 12 |
| T3 | 0.1 | −0.2 | 0.2 | −0.6 | −0.5 | 12 |
| T4 | 0.1 | −0.3 | 0.1 | −0.5 | −0.5 | 12 |
| T5 | 1.0 | −0.3 | 0.1 | −0.7 | −0.7 | 11 |
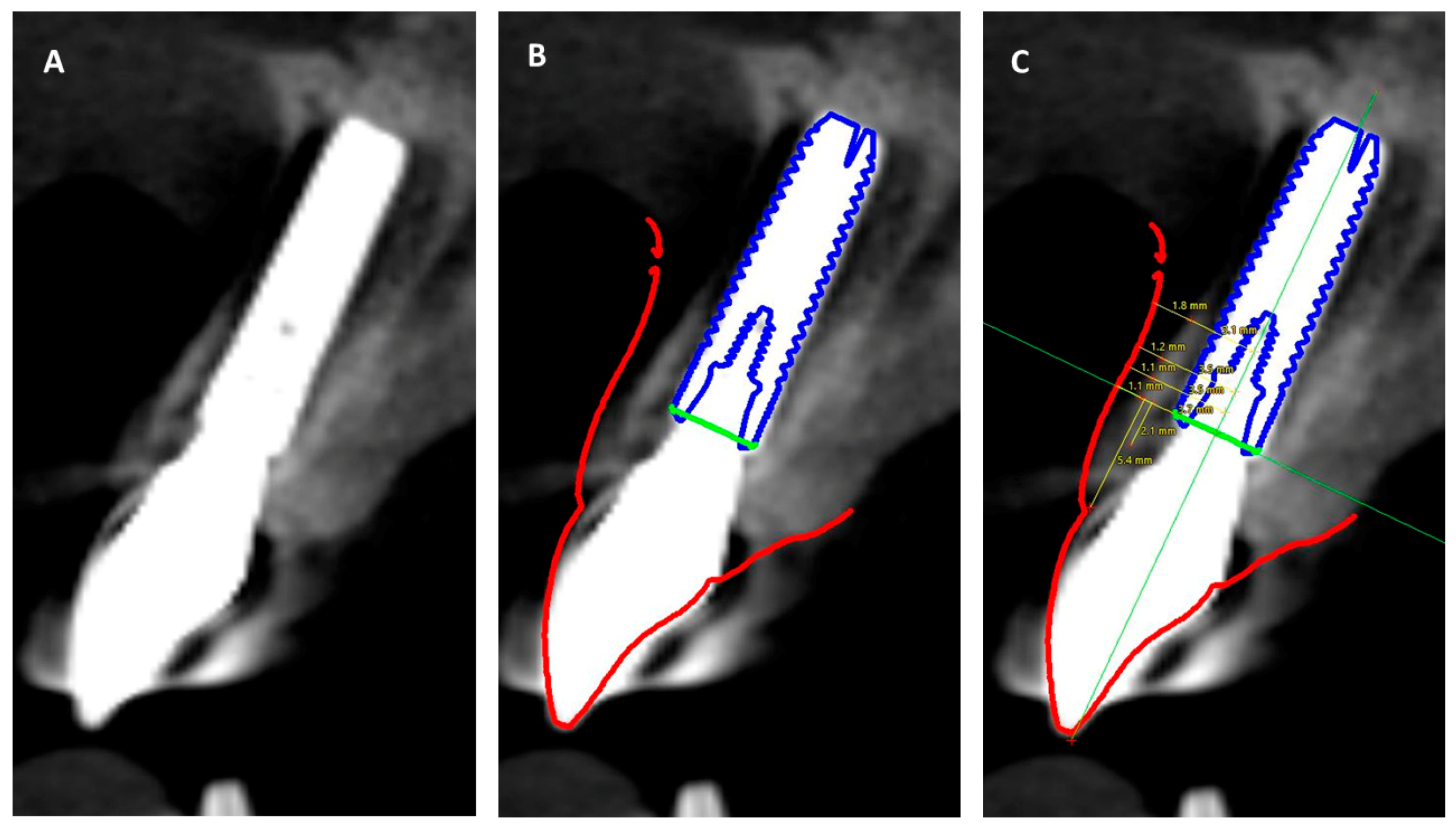
| Implant Shoulder | 1 mm | 2 mm | 4 mm | Mean Thickness | |
|---|---|---|---|---|---|
| Bone | 1.7 | 1.5 | 1.5 | 1.1 | 1.45 |
| Soft tissue | 1.1 | 1.1 | 1.2 | 1.8 | 1.3 |
| Combined tissue thickness | 2.8 | 2.6 | 2.7 | 2.9 | 2.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arora, H.; Ivanovski, S. Ten Year Clinical and Aesthetic Outcomes of an Immediately Placed and Restored Implant in the Anterior Maxilla: A Case Report. Prosthesis 2021, 3, 129-136. https://doi.org/10.3390/prosthesis3020014
Arora H, Ivanovski S. Ten Year Clinical and Aesthetic Outcomes of an Immediately Placed and Restored Implant in the Anterior Maxilla: A Case Report. Prosthesis. 2021; 3(2):129-136. https://doi.org/10.3390/prosthesis3020014
Chicago/Turabian StyleArora, Himanshu, and Sašo Ivanovski. 2021. "Ten Year Clinical and Aesthetic Outcomes of an Immediately Placed and Restored Implant in the Anterior Maxilla: A Case Report" Prosthesis 3, no. 2: 129-136. https://doi.org/10.3390/prosthesis3020014
APA StyleArora, H., & Ivanovski, S. (2021). Ten Year Clinical and Aesthetic Outcomes of an Immediately Placed and Restored Implant in the Anterior Maxilla: A Case Report. Prosthesis, 3(2), 129-136. https://doi.org/10.3390/prosthesis3020014