
Gut and Other Differences Between Female and Male Veterans—Vive La Différence? Bringing It All Together

 ,
,
Abstract
1. Introduction
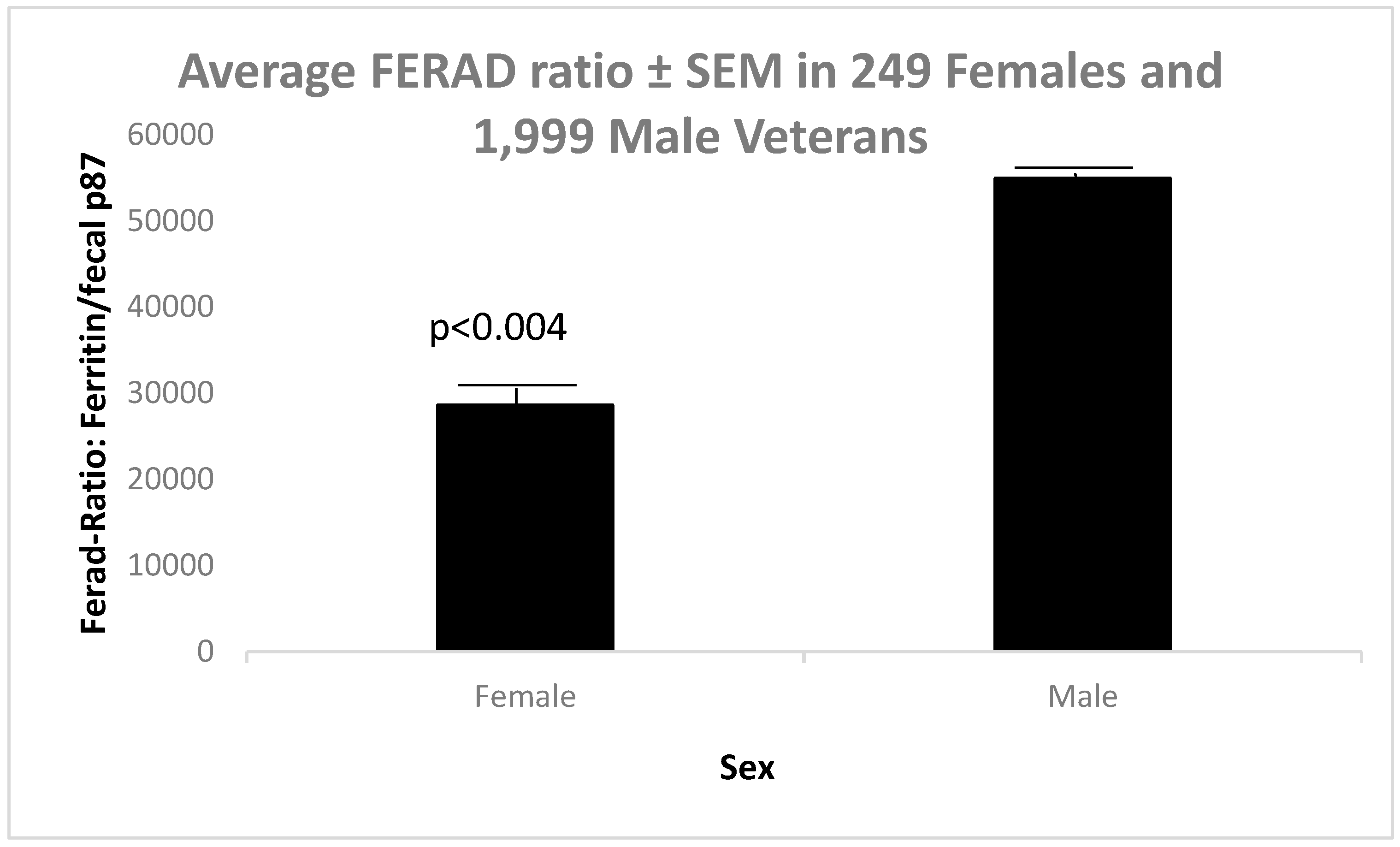
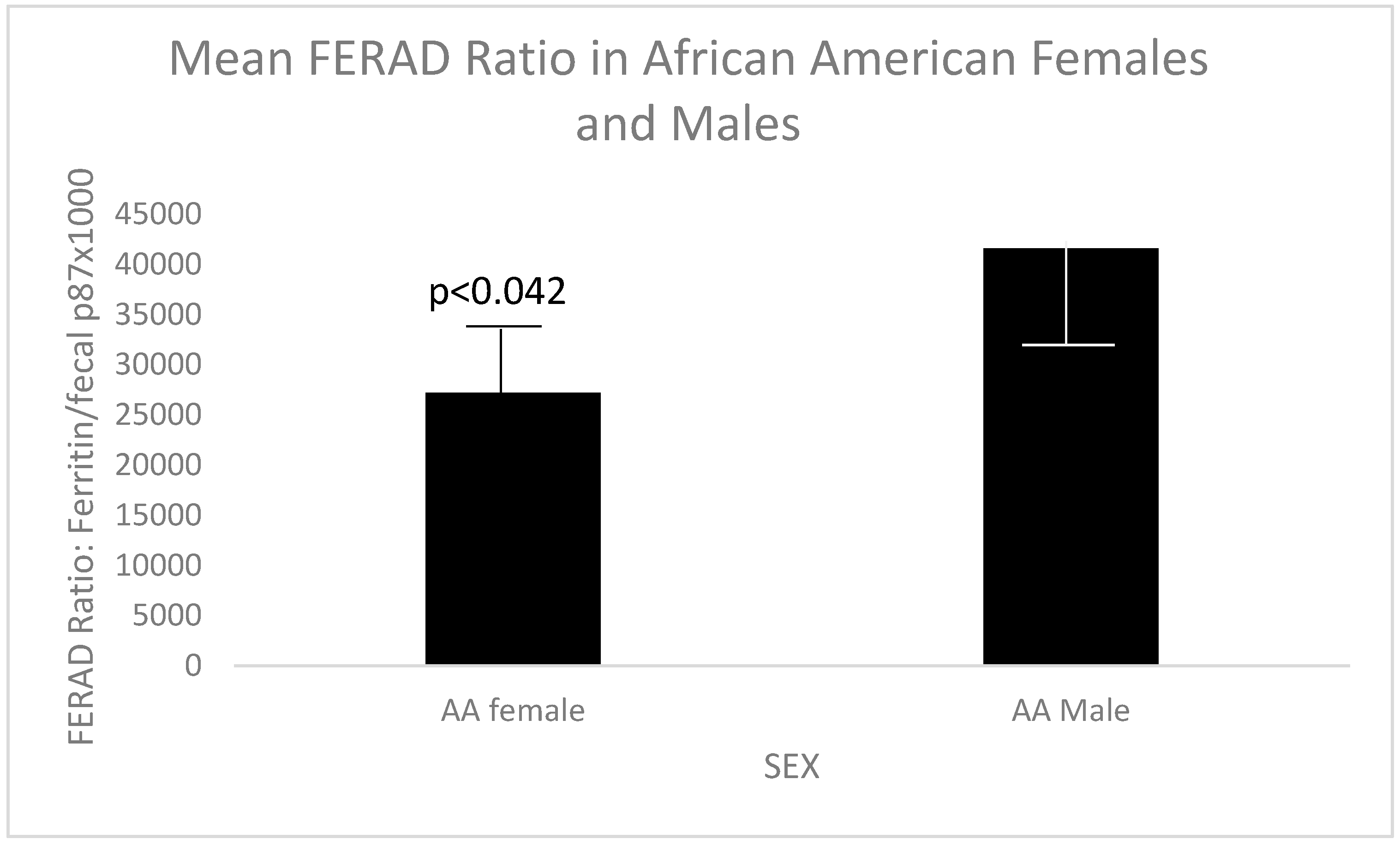
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=Differences+between+male+and+female+veterans+in+the+USA (accessed on 23 March 2025).
- Ahnen, D.J.; Guerciolini, R.; Hauptman, J.; Blotner, S.; Woods, C.J.; Wargovich, M.J. Effect of orlistat on fecal fat, fecal biliary acids, and colonic cell proliferation in obese subjects. Clin. Gastroenterol Hepatol. 2007, 5, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Tamas, M.J.; Khakharia, A.; Rothenberg, R.B.; Phillips, L.S. Weight Trends in Veterans with and Without Diabetes, 2000 to 2014. Obesity (Silver Spring) 2018, 26, 1949–1957. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Batch, B.C.; Goldstein, K.; Yancy, W.S., Jr.; Sanders, L.L.; Danus, S.; Grambow, S.C.; Bosworth, H.B. Outcome by Gender in the Veterans Health Administration Motivating Overweight/Obese Veterans Everywhere Weight Management Program. J. Womens Health 2018, 27, 32–39. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moin, T.; Damschroder, L.J.; AuYoung, M.; Maciejewski, M.L.; Datta, S.K.; Weinreb, J.E.; Steinle, N.I.; Billington, C.; Hughes, M.; Makki, F.; et al. Diabetes Prevention Program Translation in the Veterans Health Administration. Am. J. Prev. Med. 2017, 53, 70–77. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tobi, M.; Antaki, F.; Rambus, M.A.; Yang, Y.-X.; Kaplan, D.; Rodriguez, R.; Maliakkal, B.; Majumdar, A.; Demian, E.; Tobi, Y.Y.; et al. The Non-Invasive Prediction of Colorectal Neoplasia (NIPCON) Study 1995-2022: A Comparison of Guaiac-Based Fecal Occult Blood Test (FOBT) and an Anti-Adenoma Antibody, Adnab-9. Int. J. Mol. Sci. 2023, 24, 17257. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tobi, M.; Bluth, M.H.; Rossi, N.F.; Demian, E.; Talwar, H.; Tobi, Y.Y.; Sochacki, P.; Levi, E.; Lawson, M.; McVicker, B. In the SARS-CoV-2 Pandora Pandemic: Can the Stance of Premorbid Intestinal Innate Immune System as Measured by Fecal Adnab-9 Binding of p87:Blood Ferritin, Yielding the FERAD Ratio, Predict COVID-19 Susceptibility and Survival in a Prospective Population Database? Int. J. Mol. Sci. 2023, 19, 7536. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tobi, M.; Khoury, N.; Al-Subee, O.; Sethi, S.; Talwar, H.; Kam, M.; Hatfield, J.; Levi, E.; Hallman, J.; Moyer, M.P.; et al. Predicting Regression of Barrett’s Esophagus-Can All the King’s Men Put It Together Again? Biomolecules 2024, 14, 1182. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tobi, M.; Talwar, H.; Rossi, N.F.; Lockette, W.; McVicker, B. A Practical Format to Organize Cancer Constellations Using Innate Immune System Biomarkers: Implications for Early Diagnosis and Prognostication. Int. J. Transl. Med. 2024, 4, 726–739. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Frayne, S.M.; Yu, W.; Yano, E.M.; Ananth, L.; Iqbal, S.; Thrailkill, A.; Phibbs, C.S. Gender and use of care: Planning for tomorrow’s Veterans Health Administration. J. Womens Health 2007, 16, 1188–1199. [Google Scholar] [CrossRef] [PubMed]
- Frayne, S.M.; Parker, V.A.; Christiansen, C.L.; Loveland, S.; Seaver, M.R.; Kazis, L.E.; Skinner, K.M. Health status among 28,000 women veterans. The VA Women’s Health Program Evaluation Project. J. Gen. Intern. Med. 2006, 21 (Suppl. 3), S40–S46. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Garcia-Davis, S.; Tyagi, P.; Bouldin, E.D.; Hansen, J.; Brintz, B.; Noel, P.; Rupper, R.; Trivedi, R.; Kinosian, B.; Intrator, O.; et al. Sex differences in unmet needs between male and female older Veterans. J. Women Aging 2024, 36, 518–533. [Google Scholar] [CrossRef] [PubMed]
- Zickmund, S.L.; Burkitt, K.H.; Gao, S.; Stone, R.A.; Jones, A.L.; Hausmann, L.R.M.; Switzer, G.E.; Borrero, S.; Rodriguez, K.L.; Fine, M.J. Racial, Ethnic, and Gender Equity in Veteran Satisfaction with Health Care in the Veterans Affairs Health Care System. J. Gen. Intern. Med. 2018, 33, 305–331. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Duggal, M.; Goulet, J.L.; Womack, J.; Gordon, K.; Mattocks, K.; Haskell, S.G.; Justice, A.C.; A Brandt, C. Comparison of outpatient health care utilization among returning women and men veterans from Afghanistan and Iraq. BMC Health Serv. Res. 2010, 10, 175. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kroll-Desrosiers, A.; Copeland, L.A.; Mengeling, M.A.; Mattocks, K.M. Infertility Services for Veterans Enrolled in Veterans Health Administration Care. J. Gen. Intern. Med. 2023, 38, 2347–2353. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mancuso, A.C.; Mengeling, M.A.; Holcombe, A.; Ryan, G.L. Lifetime infertility and environmental, chemical, and hazardous exposures among female and male US veterans. Am. J. Obstet. Gynecol. 2022, 22, 744.e1–744.e12. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Adepoju, B.; Yacur, M.; Maron, D.; Sharma, M.C. Gender Disparity in Breast Cancer: A Veteran Population-Based Comparison. Clin. Breast Cancer 2021, 21, e471–e478. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.K.; Lim, Y.J.; Kim, W. Breast Cancer Metastasis to the Parotid: A Case Report with Imaging Findings. Am. J. Case Rep. 2021, 22, e934311. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- St Cyr, K.; Aiken, A.B.; Cramm, H.; Whitehead, M.; Kurdyak, P.; Mahar, A.L. Sex-specific differences in physical health and health services use among Canadian Veterans: A retrospective cohort study using healthcare administrative data. BMJ Mil Health 2023, 169, 430–435. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vimalananda, V.G.; Miller, D.R.; Christiansen, C.; Wang, W.; Tremblay, P.; Fincke, B.G. Cardiovascular disease risk factors among women veterans at VA medical facilities. J. Gen. Intern. Med. 2013, 28 (Suppl. S2), S517–S523. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, N.S.; Keddem, S.; Sorrentino, A.E.; Jenkins, K.A.; Long, J.A. Health Equity in the Veterans Health Administration from Veterans’ Perspectives by Race and Sex. JAMA Netw. Open 2024, 5, e2356600. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hasin, D.S.; Grant, B.F. The National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) Waves 1 and 2: Review and summary of findings. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1609–1640. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Brown, D.W. Smoking prevalence among US veterans. J. Gen. Intern. Med. 2010, 25, 147–149. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Verne, Z.T.; Fields, J.Z.; Verne, G.N.; Zhang, B.B.; Thacker, A.L.; Zhou, Q. Onset of Irritable Bowel Syndrome, Dyspepsia, Diarrhea, Bloating, and Constipation in Deployed Gulf War Veterans. Int. J. Gasteroenterol. 2024, 8, 5–10. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Weeda, E.R.; Bishu, K.G.; Ward, R.; Axon, R.N.; Taber, D.J.; Gebregziabher, M. Joint effect of race/ethnicity or location of residence and sex on low density lipoprotein-cholesterol among veterans with type 2 diabetes: A 10-year retrospective cohort study. BMC Cardiovasc. Disord. 2020, 20, 449. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Upchurch, D.M.; Wong, M.S.; Yuan, A.H.; Haderlein, T.P.; McClendon, J.; Christy, A.; Washington, D.L. COVID-19 Infection in the Veterans Health Administration: Gender-specific Racial and Ethnic Differences. Womens Health Issues 2022, 32, 41–50. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stainbrook, K.; Hartwell, S.; James, A. Female Veterans in Jail Diversion Programs: Differences from and Similarities to Their Male Peers. Psychiatr. Serv. 2016, 67, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Stainbrook, K.; Penney, D.; Elwyn, L. The opportunities and challenges of multi-site evaluations: Lessons from the jail diversion and trauma recovery national cross-site evaluation. Eval. Program Plan. 2015, 50, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.B.; Gray, K.E.; Hoerster, K.D.; Fortney, J.C.; Simpson, T.L. Differences in functional and structural social support among female and male veterans and civilians. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 375–386. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
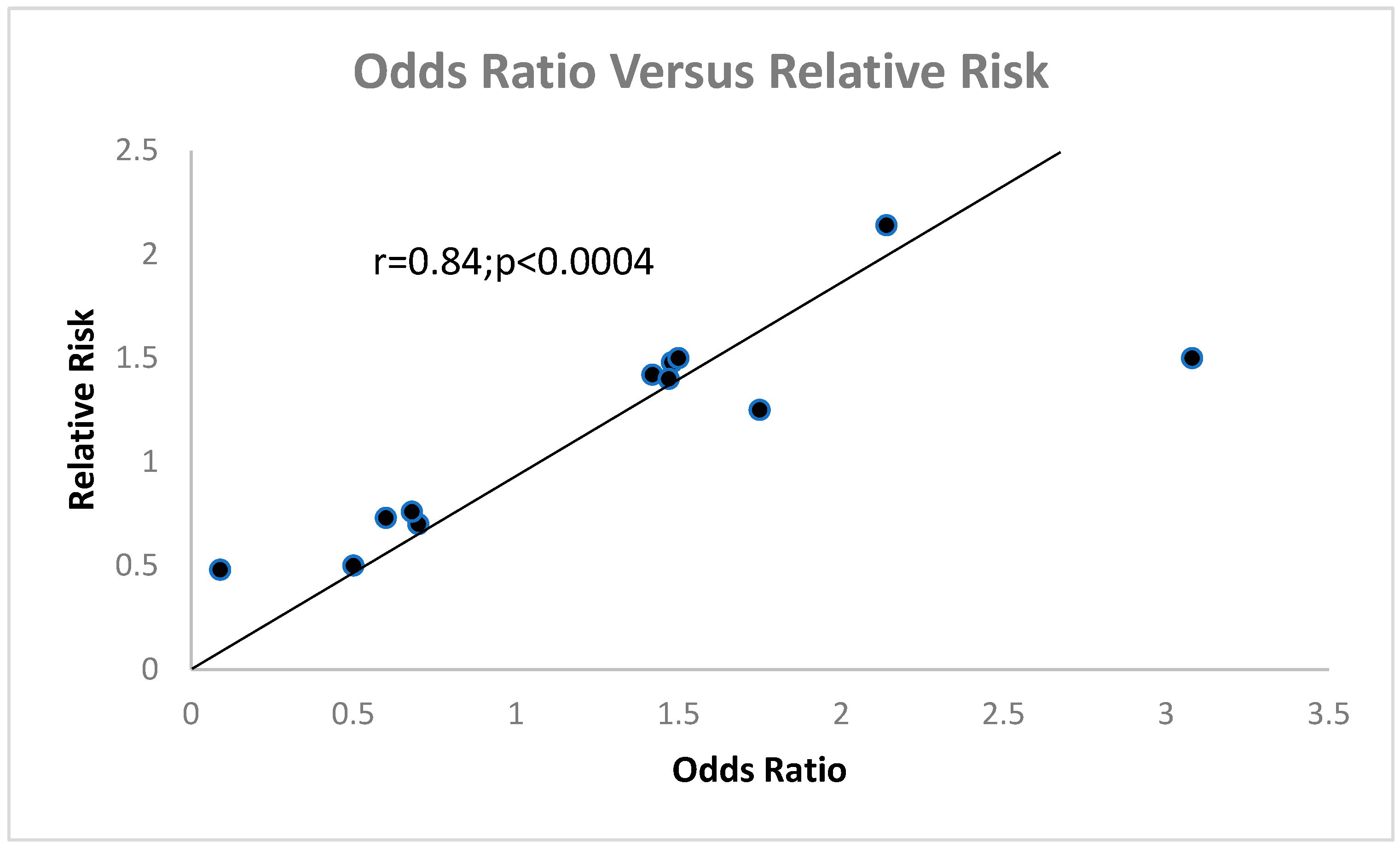
- Schmidt, C.O.; Kohlmann, T. When to use the odds ratio or the relative risk? Int. J. Public Health 2008, 53, 165–167. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Female 449 | Male 1624 | Age > 50 Veterans | Confidence Interval: p |
|---|---|---|---|---|
| Age mean ± sd | 47.51 ± 10.78 | 64.51 ± 9.73 | F28% M99.7% | RR3.55 [3.06–4.12]; p < 0.0001 |
| Race AA: C: H: A | 208: 195: 7: 0 | 877: 799: 19: 6 | M%AA52.3 F%51.6 | p = 0.800 |
| Alive + Dead | 309 + 98 − (24) | 831 + 811 − (49.4) | N/A | RR1.50 [1.40–1.61] < 0.0001 |
| Survival (days) | 4850 ± 6858 | 3152 ± 2461 | p = 0.300 |
| Parameter | Female (%) | Male (%) | Confidence Interval | p-Value |
|---|---|---|---|---|
| Diabetes | 109 + 262 − (29.4) | 492 + 829 − (37.3) | RR0.70 [0.55–0.90] | <0.006 |
| GI Symptoms | 264 + 132 − (66.7) | 866 + 758 − (53.3) | RR1.25 [1.15–2.21] | <0.0001 |
| Vit D serum | 101 + 29 − (22.3) | 169 + 55 − (25) | N/A | 0.600 |
| IBD | UC = 7; Cr = 10 | UC = 25; Cr = 9 | N/A | 0.700 |
| Smoking | 131 + 164 − (44.4) | 366 + 650 − (36) | RR1.42 [1.10–1.44] | <0.01 |
| Alcohol | 143 + 74 − (65.9) | 487 + 373 − (49.7) | RR1.48 [1.08–2.02] | <0.014 |
| Illicit Drugs | 38 + 117 − (30.4) | 91 + 413 − (18) | RR1.36 [0.97–1.89] | =0.08 |
| COVID-19 exposure | 17 + 57 − (23) | 30 + 125 − (19.4) | N/A | 0.6 |
| Hepatitis C | 47 + 204 − (18.7) | 131 + 549 − (19.3) | N/A | 0.9 |
| Tonsillectomy | 12 + 47 − (20.3) | 26 + 151 − (14.7) | N/A | 0.41 |
| Appendicectomy | 7 + 49 − (29) | 28 + 155 − (15.4) | N/A | 0.7 |
| Barrett’s Es | 12 + 140 − (7.9) | 69 + 399 − (14.7) | RR0.50 [0.30–0.96) | <0.037 |
| Modality | Female | Male | Relative Risk [PI]; p-Value |
|---|---|---|---|
| Flu Vaccination | 42 + 90 − (31.8%) | 327 + 421 − (43.7%) | RR0.73 [0.56–0.95]; p < 0.012 |
| Papanicolaou Smear (PS) | 87 + 39–69% | N/A | Male PSA vs. Female (PS) p = 0.5 |
| Mammography (PSA in males) | 50 + 60 − 45.5% | Insufficient (use PSA) | (m)OR2.14 [1.42–3.21]; p < 0.0003 |
| Prostate-Specific Antigen | N/A | 559 + 218 − (71.9%) | Vide supra. |
| Aspirin | 62 + 354 − (14.7%) | 185 + 1552 − (10.7%) | 1.4 [1.07–2.00]; p < 0.015 |
| Proton Pump Inhibitor | 35 + 113 − (23.7%) | 127 + 487 − (20.7%) | p = 0.400 |
| Clarithromycin | 30 + 116 − (20.6%) | 163 + 214 − (43.2%) | RR0.48 [0.34–0.67]; p < 0.0001 |
| Modality | Female (%) | Male (%) | Odds Ratio [PI]; p-Value |
|---|---|---|---|
| Flexible sigmoidoscopy | 90 + 305 − (22.8) | 479 + 1111 − (30) | RR0.76 [0.53–0.89]; p < 0.004 |
| Colonoscopy | 213 + 174 − (55) | 940 + 649 − (59.2) | p = 0.140 |
| FOBT submitted or not | 212 + 217 − (49) | 820 + 887 − (48) | p = 100 |
| Detection outcomes | 30 sig 48 insig | 204 sig 273 insig | p = 0.700 |
| History of neoplasia 16.9% vs. 58.2% | 109 sig 92 insig | 500 sig 301 insig | OR1.5 [0.62–0.92]; p < 0.004 |
| Parameter | Our Database | Female | Male | p-Value RR [CI] 95% | Citation p |
|---|---|---|---|---|---|
| Alcohol | 65.9%F (217) 49.7%M(860) | 356 | 2569 | 0.13 (1.17–1.48) | 22 p < 0.0001 |
| Smokers | 44.4%F 36%M | 25% | 22% | 1.23 (1.03–1.46) | 23 p < 0.03 |
| GI symptoms | 66.7%F 53.3%M | 16 | 88 | 0.896 [0.84–0.95] | 24 p < 0.0004 |
| Diabetes | 29.4%F37.1%M | 11% | 22% | 0.80 (0.64–0.98) | 25 p < 0.04 |
| COVID-19 | 23%F 19.4%M | 39,223 11% | 316,380 89% | <0.001 | 26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tobi, M.; Bradley, D.; Antaki, F.; Rambus, M.; Rossi, N.F.; Hatfield, J.; Fligiel, S.; McVicker, B. Gut and Other Differences Between Female and Male Veterans—Vive La Différence? Bringing It All Together. Gastrointest. Disord. 2025, 7, 48. https://doi.org/10.3390/gidisord7030048
Tobi M, Bradley D, Antaki F, Rambus M, Rossi NF, Hatfield J, Fligiel S, McVicker B. Gut and Other Differences Between Female and Male Veterans—Vive La Différence? Bringing It All Together. Gastrointestinal Disorders. 2025; 7(3):48. https://doi.org/10.3390/gidisord7030048
Chicago/Turabian StyleTobi, Martin, Donald Bradley, Fadi Antaki, MaryAnn Rambus, Noreen F. Rossi, James Hatfield, Suzanne Fligiel, and Benita McVicker. 2025. "Gut and Other Differences Between Female and Male Veterans—Vive La Différence? Bringing It All Together" Gastrointestinal Disorders 7, no. 3: 48. https://doi.org/10.3390/gidisord7030048
APA StyleTobi, M., Bradley, D., Antaki, F., Rambus, M., Rossi, N. F., Hatfield, J., Fligiel, S., & McVicker, B. (2025). Gut and Other Differences Between Female and Male Veterans—Vive La Différence? Bringing It All Together. Gastrointestinal Disorders, 7(3), 48. https://doi.org/10.3390/gidisord7030048