Abstract
Background: Technological advances in pediatric gastrointestinal (GI) endoscopy require highly specialized physicians. Therefore, proper training is fundamental. The aim of this study was to assess the level of competence of pediatric surgery residents to determine areas that should be addressed to design better training programs focused on pediatric GI endoscopy. Methods: An observational study was performed on all Italian pediatric surgery trainees that concluded the training program by the end of 2021, who were asked to answer a questionnaire about the quality of the GI endoscopy education received during their 5 years of residency. Results: 12 out 14 (86%) pediatric surgery trainees answered the questionnaire. A total of 50% (6/12) of the trainees declared they were interested in pediatric GI endoscopy, and 42% (5/12) said that they would be interested in dedicating themselves to this discipline in the future. Only 33% (4/12) of them were in a center equipped with endoscopy simulators. Among them, 17% (2/12) never took part in GI endoscopic procedures while working in centers in which GI endoscopy is performed exclusively by pediatric gastroenterologists, 25% (3/12) had never performed GI endoscopic procedures as a first operator and 17% (2/12) not even as assistant. Overall, 50% (6/12) were not satisfied with the level of education received and only 17% (2/12) declared that they felt confident enough to perform routine endoscopies alone. Conclusions: Our study highlights great inhomogeneity between different schools and some important failings. Better programs should be designed to educate proficient pediatric GI endoscopists.
1. Introduction
It is nowadays well accepted that gastrointestinal (GI) endoscopy is a fundamental tool in the diagnosis and treatment of GI diseases in children. Additionally, the miniaturization of instruments led to an increase in the number of operative procedures now performable on children [1,2,3].
Considering what we mentioned before, it is extremely important in the pediatric field that strongly dedicated and highly specialized pediatric GI endoscopists can be counted on. Therefore, pediatricians and pediatric surgeons who desire to acquire competence in GI endoscopy should be guaranteed a well-structured endoscopy fellowship during their training program.
Currently, in Italy, pediatric GI endoscopy is performed by both pediatric surgeons and pediatricians.
The pediatric surgery training program in Italy has a duration of 5 years, during which trainees achieve competence in a large variety of surgical interventions as well as diagnostic and operative GI endoscopy. Nevertheless, Italy does not have a standardized pediatric GI endoscopy fellowship.
Similarly, the pediatrics training program in Italy lasts 5 years and, generally, during their last 2 years, trainees can decide whether they want to pursue a certain subspecialty (e.g., pediatric cardiology, pediatric gastroenterology, etc.).
Regarding the pediatric surgery training program, Italy is a latecomer to this field compared with other countries; Italy only recently started a serious discussion on how many procedures are necessary to acquire competence and how to guarantee a minimum standard. Only recently trainees have been equipped with an electronic portfolio to take note of every surgical procedure performed. In the portfolio itself, the minimum number of requested procedures per year of residency previously decided by the Italian training program directors is reported.
Considering the novelty of the concept of establishing and guaranteeing minimum procedure thresholds, the training process for pediatric GI endoscopy, a subspeciality procedure not even performed in all centers, has not undergone this process of reorganization yet. This is true for the pediatrics training program as well.
Considering the various failings briefly expressed above, we hypothesized that pediatric surgery training programs lack a guaranteed, well-structured, and complete education in pediatric endoscopy.
The aim of this study was therefore to analyze and verify the level of competence reached in pediatric GI endoscopy by pediatric surgery trainees at the end of their education to highlight the limits of the training programs so that efforts can be made to improve them.
2. Results
Overall, 12 out the 14 (86%) pediatric surgery trainees all over Italy that concluded their training program by the end of 2021 answered the questionnaire.
The survey showed a slightly higher prevalence of pediatric gastroenterologists compared with pediatric surgeons performing GI endoscopy, respectively, 75% (9/12) vs. 67% (8/12), even if the data suggest that in some cases, the two collaborate in this field (Figure 1 Q2).
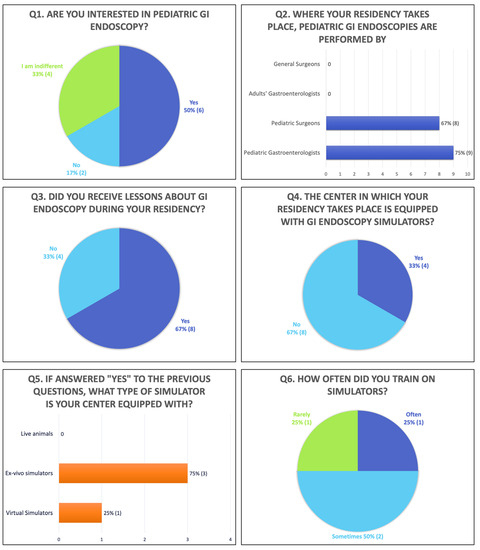
Figure 1.
First part of the questionnaire (Q: question).
Overall, 50% (6/12) of trainees declared that they were interested in pediatric GI endoscopy, 17% (2/12) were not, and 33% (4/12) were indifferent (Figure 1 Q1); moreover, 42% (5/12) said they would be interested in performing GI endoscopy in the future, while 25% (3/12) did not know and 33% (4/12) were not interested (Figure 2 Q12).
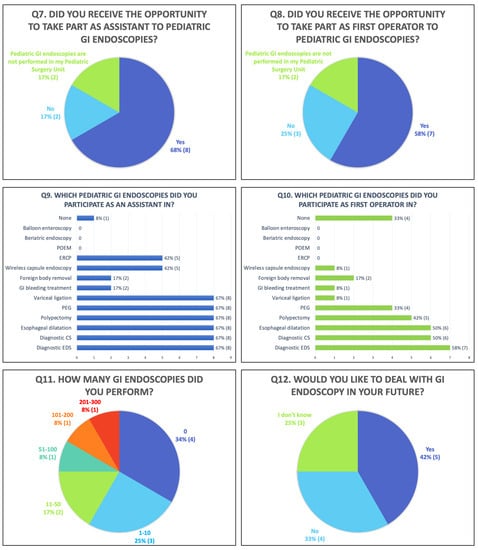
Figure 2.
Second part of the questionnaire (Q: question; POEM: peroral endoscopic myotomy; ERCP: endoscopic retrograde cholangiopancreatography; PEG: percutaneous endoscopic gastrostomy; CS: colonoscopy; EGD: esophagogastroduodenoscopy).
Overall, 67% (8/12) of trainees received some lessons about pediatric GI endoscopy, while 33% (4/12) never had one (Figure 1 Q3).
Only 33% (4/12) of the residents said they worked in a center equipped with GI endoscopy simulators (Figure 1 Q4), which were in 75% (3/4) of cases ex vivo models and in 25% of cases (1/4) virtual simulators (Figure 1 Q5). Concerning the frequency of training on simulators where they were available, 50% (2/4) of trainees answered that they regularly used them, 25% (1/4) sometimes, and 25% (1/4) rarely (Figure 1 Q6).
As regards the possibility of participating in GI endoscopic procedures (Figure 2 Q7, Q8), 17% (2/12) working in a center in which GI endoscopy is performed exclusively by pediatric gastroenterologists had never observed one, 68% (8/12) had assisted his/her consultant, and 58% (7/12) had performed pediatric GI endoscopies himself/herself (Figure 2 Q9, Q10 presents the details about the procedures performed as first and second operators).
Considering the number of procedures performed as a first operator during the entire residency program, 8% (1/12) took part in 201–300 GI endoscopic procedures; 8% (1/12) 101–200; 8% (1/12) 51–100; 17% (2/12) 11–50; 25% (3/12) 1–10; and 34% (4/12) 0 (Figure 2 Q11).
When it comes to the self-assessment of their residency in terms of GI endoscopy education, 50% (6/12) of trainees were not satisfied (Figure 3 Q13) and only 17% (2/12) felt confident enough to perform routine procedures alone (Figure 3 Q15).
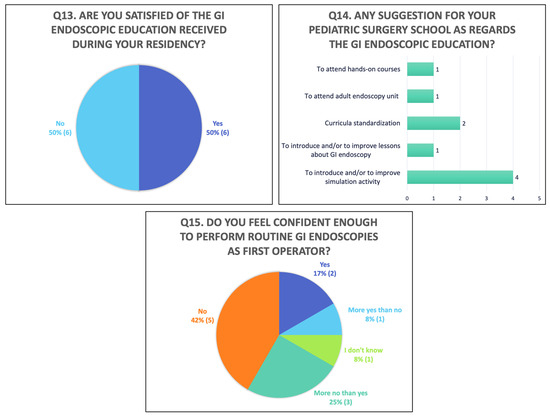
Figure 3.
Third part of the questionnaire (Q: question).
Residents suggested in the questionnaire that simulation activities be introduced or enhanced and lessons on this topic be taught during residency to standardize the endoscopy curricula between all Italian pediatric surgery departments and suggested that trainees be offered the possibility of attending hand-on courses and participating in adult endoscopy units (Figure 3 Q14).
3. Discussion
In the past, pediatric GI endoscopy was recognized to be just of diagnostic value, but, some decades on, it is undergoing a process of expansion which has led to the advent of a wide range of procedures, some of which are extremely complex [1,2,3].
The evolution of techniques and the extension of their indications in pediatrics were made feasible by the miniaturization of instruments and technological advances in the endoscopes themselves [4,5,6,7,8,9].
Therefore, nowadays, endoscopy for either diagnostic or therapeutic purposes requires appropriate pediatric training to achieve a proper level of clinical knowledge, judgment skills, and technical competence that guarantees safe and effective procedures.
The meaning of “competence” itself was recently clarified by the North American Society For Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN), which distinguishes diagnostic competence, defined as the ability to recognize abnormalities and to understand the pathologic features of the lesions that can occur, from a therapeutic competence, that is, the ability to recognize whether a therapeutic procedure is indicated in a given patient and the ability to perform that procedure safely and successfully [10].
However, pediatric GI endoscopy training encounters some complex challenges to overcome.
First, the incidence of diseases with an endoscopic indication at pediatric ages is very low, especially when compared to adults. This means that the volume of patients that need to be treated is sometimes very small, making it difficult to acquire competence just based on procedural numbers.
Furthermore, in Europe, and especially in Italy, there is a lack of centralization of diseases, leading to a fragmentation of cases across different centers and the risk of not being able to reach the minimum requirements to develop high specialization.
Finally, in some countries, such as Italy, it is not yet clearly defined which health providers should be dedicated to pediatric GI endoscopy, and that is why in some Italian centers, GI endoscopy is performed by pediatric surgeons and in others by pediatric gastroenterologists and sometimes even by adult gastroenterologists or general surgeons.
The abovementioned challenge certainly complicates efforts to create a structured endoscopy training program during residency in pediatric surgery and pediatrics as well.
The difficulties in conceiving proper endoscopy training are well known to the main international pediatric gastroenterology and endoscopy societies, which have been looking for a solution for quite some time, arriving at proposals that sometimes differ between one another, as follows.
The NASPGHAN divides the training process into three levels [10]:
- Level 1 trainees should achieve competence in the procedural skills of diagnostic and therapeutic endoscopy to provide comprehensive care to pediatric patients with GI disorders.
- Level 2 training encompasses new, advanced, or higher-risk endoscopic procedures.
- Level 3 training is recommended for those who plan to perform specialized endoscopic procedures required for the care of patients with particularly complex disorders.
Procedures that fall under the categories of level 1 (routine), level 2 (complex), and level 3 (advanced) are shown in Table 1.

Table 1.
NASPGHAN training levels and procedural number thresholds.
To achieve competence in each level, the NASPGHAN requires a minimum number of procedures to be performed as a first operator under expert supervision (the threshold for every procedure is reported in Table 1).
Competence threshold numbers have been issued by several scientific societies and have long been used as indicators of competency [11,12].
Studies on adult endoscopy learning curves have recommended 100–200 esophagogastroduodenoscopies and 200–300 ileocolonoscopies as minimum thresholds for achieving competence [13,14,15,16,17,18,19].
Some societies (e.g., ESPGHAN, British Society for Paediatric Gastroenterology, Hepatology and Nutrition) have stated that not all trainees will reach the abovementioned numbers [20], which are based on expert opinions. Indeed, some studies found that these thresholds were underestimated. Therefore, the European Society for Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) guidelines on training in endoscopy state that thresholds are untenable and contradict available evidence [15,21].
Therefore, a minimum number of procedures should be kept in mind, but competence-based teaching may provide adequate experience without the formal definition of minimum numbers, if the desired goals are to be achieved [13,14,22].
With these preconditions in mind, the purpose of the present study was to evaluate whether, in Italian pediatric surgery residency, it is possible to train a routine/advanced pediatric GI endoscopist (using the American definition: a first-/second-level endoscopist).
An answer was found by analyzing the experiences of pediatric surgery residents currently in their last year of training via a questionnaire sent to all 14 of them. We received 12 answers (86%), and the results are discussed below.
The pediatric surgery residents demonstrated an interest in pediatric GI endoscopy, and 50% of them (or 67% if we consider both the “yes” and “I don’t know” answers) were willing to perform GI endoscopy in the future (Figure 1 Q1, Figure 2 Q12).
Unfortunately, some critical issues emerged when analyzing the section dedicated to training.
First, not all trainees had the opportunity to observe GI endoscopies: indeed, 17% were attending residency in a place in which digestive endoscopic procedures were performed by gastroenterologists. As a matter of fact, our questionnaire shows a slight prevalence of pediatric gastroenterologists (75%) over pediatric surgeons (67%) in performing GI endoscopy in Italy (Figure 1 Q2, Figure 2 Q7, Q8).
Second, the questionnaire showed limited opportunity for hands-on training: only 58% performed endoscopies as a first operator, with (Figure 2 Q8) diagnostic endoscopy as the most represented (67% performed diagnostic esophagogastroduodenoscopies and 50% diagnostic colonoscopies) followed by a very low number of therapeutic endoscopies (Figure 2 Q9,10).
The overall number of procedures performed also reflects the lack of opportunities during residency: only 16% performed at least 100 endoscopies (Figure 2 Q11); this means that, if compared with the threshold recommended in the NASPGHAN training guidelines, most residents will not reach the minimum number required [10].
The section of the questionnaire focused on education showed failings and inhomogeneity between Italian schools: only 67% of trainees received lectures on digestive endoscopy (Figure 1 Q3) and just 33% of centers were equipped with endoscopy simulators (Figure 1 Q4).
Finally, trainees’ overall perception of their GI endoscopy education during residency was quite negative, considering that 50% of trainees were not satisfied with the education received (Figure 3 Q13) and two-thirds of them did not feel confident enough to routinely perform GI endoscopies without supervisors at the end of their residency (Figure 3 Q15).
The abovementioned questionnaire showed an important level of criticality in GI endoscopy education during residency in pediatric surgery. Nevertheless, most of the issues can be overcome with more dialogue between the Italian schools of pediatric surgery in order to design a common structured program.
For instance, every school should aim to ensure lectures on GI endoscopy along with the ones already planned on more classical pediatric surgical themes.
Moreover, centers in which surgeons do not perform GI endoscopy should plan rotations in pediatric endoscopy units to let trainees become familiar with this branch of pediatric GI care.
Finally, it is important to guarantee that trainees spend enough time in a simulation center. Simulation of pediatric GI endoscopy can be performed on live animal models, ex vivo models, and computer-based simulators. In a study on pediatric gastroenterology trainees performing a colonoscopy, the ones that received virtual training had a significant advantage in the rate of skill acquisition and lesion recognition compared with peers undergoing standard training without simulation [23]. Similar results have been reported in a multicenter randomized controlled trial of novice trainees performing a colonoscopy in adults [24]. The potential advantages of simulation training include offering trainees direct experience in the manipulation of an endoscope without exposing patients to discomfort or risks [25,26,27,28,29]. In addition, learning basic skills outside a clinical setting can decrease the time spent on basic instruction and improve efficiency in the operating room [26,30,31,32,33,34].
However, we recognize that the experience of operating on live patients cannot replaced since the sensation of resistance, as well as training for difficult maneuvers for novices, such as intubating the esophagus and the ileocecal valve or traversing the sigmoid colon, cannot be perfectly reproduced by simulators.
As mentioned above, after all, this is exactly what some trainees suggested in our survey. Indeed (Figure 3 Q14), they asked for the standardization of curricula, the introduction or enhancement of simulation activities and lectures, and more opportunities to attend hands-on courses or participate in adult endoscopy units.
The literature agrees that participating in adult endoscopy units is an important way to acquire basic skills. Morita et al., in their paper, also express the difficulty of guaranteeing adequate training in pediatric GI endoscopy during pediatrics residency. However, they report the experience of 10 pediatric trainees who spent three months in an adult GI unit. During this period, they reached a mean number of 651.7 EGDs, 159.2 colonoscopies and 25.8 polypectomies, thus satisfying the NASPGHAN’s suggestions (Table 1) [35].
As we mentioned previously, not all pediatric surgeries in Italy perform endoscopies or have all departments of pediatrics. Moreover, a structured training program could be extremely demanding and expensive and therefore not reasonable for units not needing to train endoscopists. A possible solution could be to establish an elective training program organized by centers with a high volume of endoscopies for both pediatric surgeons and pediatric gastroenterologists during their last years of residency.
Cooperation between pediatric surgeons and pediatricians in creating a proper training center is another key point. We believe that pediatric gastroenterologists’ extensive knowledge of pediatric GI disorders is extremely important to train young future endoscopists to recognize the endoscopic pattern of diseases. On the other hand, surgical knowledge and the ability to manage complications, for instance, are important prerequisites for those who would like to be trained in therapeutic endoscopy. According to what was mentioned above, the ideal training center should guarantee the presence of both specialties.
Finally, another important topic when designing training programs should be considered: time restrictions. We cannot ask trainees to dedicate extra time to subspecialties. Pediatric surgery trainees in Italy already spend a lot of time working, sometimes more than the maximum number of hours indicated by European guidelines. It is therefore preferable that a period dedicated only to GI endoscopy in centers identified as appropriate be established.
Nonetheless, we would like to highlight one more time that dedicating a well-defined period of training to GI endoscopy is not sufficient if this is not spent in a high-procedural-volume center, and the literature confirms this. Indeed, Lerner DG et al. collected experiences from 12 pediatric gastroenterology fellowships in the United States and, despite their 3-year duration, they discovered that most training programs do not have the volume of therapeutic endoscopy procedures necessary for all of the fellows to meet the NASPGHAN’s training guidelines [24].
Limits of the Study
First, two trainees are missing. The questionnaire was anonymous, so we do not know if we are missing data from two centers or if the two trainees that we did not receive answers from come from the same centers as the other 12. Additionally, we think that 12 out of 14 answers (more than 85%) is sufficient to describe a reliable Italian panorama. Someone could argue that maybe, to increase the number of participants, we should have administered the questionnaire to even younger trainees. We do not think the latter option would be a wise choice: younger trainees are necessarily exposed to fewer endoscopies (because, e.g., they are too young to manage some procedures, there is not enough time to reach the minimum threshold, efforts are more focused on teaching the basics of pediatric surgery than a subspecialty like pediatric GI endoscopy), and thus could lead to underestimating the results. Furthermore, if training programs were sufficiently structured, every trainee would have the same opportunities. Therefore, the results of our survey would not have in any case been influenced by the size of the sample but rather by considering trainees with the same number of years of experience.
Moreover, we recognize that to have a complete picture of Italian GI endoscopy training, pediatrics trainees should have been interviewed too. However, considering that, as surgeons, we can modify and improve only our surgical training programs, we focused exclusively on our trainees.
Second, the national nature of the study does not allow us to generalize our results.
Nevertheless, we think it is important to share our findings to encourage other centers to question their training programs, especially ones having a similar Italian organization.
We therefore encourage pediatric surgeries worldwide to analyze their pediatric surgery programs to determine weaknesses that could be addressed to improve education in this extremely important branch of the GI care of pediatric patients.
4. Materials and Methods
An observational study was performed on all Italian pediatric surgery trainees that concluded the training program by the end of 2021. All the trainees were asked to answer an online questionnaire that investigated the quality of the pediatric GI endoscopy education received during their 5-year fellowship (the questionnaire is presented in Figure 1, Figure 2 and Figure 3).
The questionnaire examined whether trainees were given the chance to observe and perform pediatric GI endoscopies as well as the availability of lessons and simulations, and the number of procedures performed as a first operator and ended with trainees’ self-assessment about their confidence in performing a GI endoscopy.
Data are presented with descriptive statistics.
Ethical review and approval were not necessary since the study did not involve patients, but written consent for publication was obtained from all the participants.
5. Conclusions
Pediatric GI endoscopy is undergoing a process of expansion in terms of procedures and indications and therefore requires trained health providers. In Italy, like other countries in Europe, a clear and structured training program in GI endoscopy for pediatric surgeons is not clearly defined, and sometimes, there are not even programs dedicated to it. Our study shows the Italian picture of GI endoscopy training during pediatric surgery residency, highlighting great inhomogeneity between different schools and sometimes important failings. Even if the Italian experience cannot be generalized, our results represent an opportunity for other centers to question their training programs.
We are far from having a structured training program in GI endoscopy, and the schools of pediatric surgery should cooperate more in order to meet the need for educating highly specialized pediatric GI endoscopists.
Author Contributions
G.P. participated in the design of the study and performed the statistical analysis. G.P. and M.D.M. conceived the study and participated in its design and coordination and helped to draft the manuscript. M.L. and T.G. supervised the study. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. No personal or patient data were involved.
Informed Consent Statement
A written consent to participate was obtained from the participants. Written informed consent for publication was obtained from the study participants.
Data Availability Statement
Please contact the authors for data requests.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tringali, A.; Thomson, M.; Dumonceau, J.-M.; Tavares, M.; Tabbers, M.M.; Furlano, R.; Spaander, M.; Hassan, C.; Tzvinikos, C.; Ijsselstijn, H.; et al. Pediatric gastrointestinal endoscopy: European Society of Gastrointestinal Endoscopy (ESGE) and European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) Guideline Executive summary. Endoscopy 2017, 49, 83–91. [Google Scholar] [CrossRef]
- Macchini, F.; Parente, G.; Farris, G.; Gentilino, V.; Leva, E.; Morandi, A. Classification of Esophageal Strictures following Esophageal Atresia Repair. Eur. J. Pediatr. Surg. 2018, 28, 243–249. [Google Scholar] [CrossRef]
- Parente, G.; Gargano, T.; Ruggeri, G.; Maffi, M.; D′Antonio, S.; Sacchet, E.; Lima, M. Anastomotic Stricture Definition After Esophageal Atresia Repair: Role of Endoscopic Stricture Index. J. Surg. Res. 2021, 257, 572–578. [Google Scholar] [CrossRef]
- Gkouvatsos, K.; Mathys, P.; Bastid, C.; Frossard, J.L.; Lepilliez, V.; Bichard, P. Innovations en endoscopie [Innovations in endos-copy]. Rev. Med. Suisse 2019, 15, 1478–1482. [Google Scholar]
- Teh, J.-L.; Shabbir, A.; Yuen, S.; So, J.B.-Y. Recent advances in diagnostic upper endoscopy. World J. Gastroenterol. 2020, 26, 433–447. [Google Scholar] [CrossRef]
- Sumiyama, K. Past and current trends in endoscopic diagnosis for early stage gastric cancer in Japan. Gastric Cancer 2017, 20, 20–27. [Google Scholar] [CrossRef]
- Mori, Y.; Kudo, S.; Mohmed, H.E.N.; Misawa, M.; Ogata, N.; Itoh, H.; Oda, M.; Mori, K. Artificial intelligence and upper gastrointestinal endoscopy: Current status and future perspective. Dig. Endosc. 2019, 31, 378–388. [Google Scholar] [CrossRef]
- Wang, L.; Song, H.; Wang, M.; Wang, H.; Ge, R.; Shen, Y.; Yu, Y. Utilization of Ultrasonic Image Characteristics Combined with Endoscopic Detection on the Basis of Artificial Intelligence Algorithm in Diagnosis of Early Upper Gastrointestinal Cancer. J. Healthc. Eng. 2021, 2021, 2773022. [Google Scholar] [CrossRef]
- Parente, G.; Thomas, E.; Cravano, S.; Di Mitri, M.; Vastano, M.; Gargano, T.; Cerasoli, T.; Ruspi, F.; Libri, M.; Lima, M. ArtiSential® Articulated Wrist-Like Instruments and Their First Application in Pediatric Minimally Invasive Surgery: Case Reports and Literature Review of the Most Commonly Available Robot-Inspired Devices. Children 2021, 8, 603. [Google Scholar] [CrossRef]
- Leichtner, A.M.; Gillis, L.A.; Gupta, S.; Heubi, J.; Kay, M.; Narkewicz, M.R.; Rider, E.A.; Rufo, P.A.; Sferra, T.J.; Teitelbaum, J.; et al. NASPGHAN Guidelines for Training in Pediatric Gastroenterology. J. Pediatr. Gastroenterol. Nutr. 2013, 56, S1–S8. [Google Scholar] [CrossRef]
- Walsh, C.M. In-training gastrointestinal endoscopy competency assessment tools: Types of tools, validation and impact. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 357–374. [Google Scholar] [CrossRef]
- Siau, K.; Hawkes, N.D.; Dunckley, P. Training in Endoscopy. Curr. Treat. Options Gastroenterol. 2018, 16, 345–361. [Google Scholar] [CrossRef]
- Ward, S.T.; Mohammed, M.A.; Walt, R.; Valori, R.; Ismail, T.; Dunckley, P. An analysis of the learning curve to achieve competency at colonoscopy using the JETS database. Gut 2014, 63, 1746–1754. [Google Scholar] [CrossRef]
- Ward, S.T.; Hancox, A.; Mohammed, M.A.; Ismail, T.; Griffiths, E.A.; Valori, R.; Dunckley, P. The learning curve to achieve satisfactory completion rates in upper GI endoscopy: An analysis of a national training database. Gut 2017, 66, 1022–1033. [Google Scholar] [CrossRef]
- Shahidi, N.; Ou, G.; Telford, J.; Enns, R. Establishing the learning curve for achieving competency in performing colonoscopy: A systematic review. Gastrointest. Endosc. 2014, 80, 410–416. [Google Scholar] [CrossRef]
- Adler, D.G.; Bakis, G.; Coyle, W.J.; DeGregorio, B.; Dua, K.S.; Lee, L.S.; McHenry, L.; Pais, S.A.; Rajan, E.; Sedlack, R.E.; et al. Principles of training in GI endoscopy. Gastrointest. Endosc. 2012, 75, 231–235. [Google Scholar] [CrossRef]
- Sedlack, R.E.; Coyle, W.J. Assessment of competency in endoscopy: Establishing and validating generalizable competency benchmarks for colonoscopy. Gastrointest. Endosc. 2016, 83, 516–523. [Google Scholar] [CrossRef]
- Mehta, T.; Dowler, K.; McKaig, B.C.; Valori, R.M.; Dunckley, P. Development and roll out of the JETS e-portfolio: A web based electronic portfolio for endoscopists. Front. Gastroenterol. 2011, 2, 35–42. [Google Scholar] [CrossRef]
- Siau, K.; Pelitari, S.; Green, S.; McKaig, B.; Rajendran, A.; Feeney, M.; Thoufeeq, M.; Anderson, J.; Ravindran, V.; Hagan, P.; et al. JAG consensus statements for training and certification in colonoscopy. Front. Gastroenterol. 2023, 14, 201–221. [Google Scholar] [CrossRef]
- Siau, K.; Beales, I.L.P.; Haycock, A.; Alzoubaidi, D.; Follows, R.; Haidry, R.; Mannath, J.; McConnell, S.; Murugananthan, A.; Ravindran, S.; et al. JAG consensus statements for training and certification in oesophagogastroduodenoscopy. Front. Gastroenterol. 2022, 13, 193–205. [Google Scholar] [CrossRef]
- Broekaert, I.; Tzivinikos, C.; Narula, P.; Antunes, H.; Dias, J.A.; van der Doef, H.; Isoldi, S.; Norsa, L.; Romano, C.; Scheers, I.; et al. European Society for Paediatric Gastroenterology, Hepatology and Nutrition Position Paper on Training in Paediatric Endoscopy. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 127–140. [Google Scholar] [CrossRef]
- Parente, G.; De Marziani, L.; Cordola, C.; Gargano, T.; Libri, M.; Lima, M. Training minimally invasive surgery’s basic skills: Is expensive always better? Pediatr. Surg. Int. 2021, 37, 1287–1293. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; deBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Lerner, D.G.; Li, B.U.; Mamula, P.; Fishman, D.S.; Kramer, R.; Goh, V.L.; El-Chammas, K.; Pentiuk, S.P.; Rothbaum, R.; Gurrum, B.; et al. Challenges in meeting fellowship procedural guidelines in pediatric therapeutic en-doscopy and liver biopsy. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 27–33. [Google Scholar] [CrossRef]
- Sauer, C.G.; Walsh, C.M. Pediatric Colonoscopy Quality Indicators: Teamwork and Transparency. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 607–608. [Google Scholar] [CrossRef]
- Broekaert, I.J.; Jahnel, J.; Moes, N.; van der Doef, H.; Ernst, A.; Dias, J.A.; Thomson, M.; Tzivinikos, C. Evaluation of a European-wide survey on paediatric endoscopy training. Front. Gastroenterol. 2019, 10, 188–193. [Google Scholar] [CrossRef]
- Gabrani, A.; Monteiro, I.M.; Walsh, C.M. Exploring Use of Endoscopy Simulation in North American Pediatric Gastroenterology Fellowship Training Programs. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 25–30. [Google Scholar] [CrossRef]
- Maurice, J.; Wood, E.; Jack, K. Endoscopy simulation for medical students. Clin. Teach. 2014, 11, 416–420. [Google Scholar] [CrossRef]
- Goodman, A.J.; Melson, J.; Aslanian, H.R.; Bhutani, M.S.; Krishnan, K.; Lichtenstein, D.R.; Navaneethan, U.; Pannala, R.; Parsi, M.A.; Schulman, A.R.; et al. Endoscopic simulators. Gastrointest. Endosc. 2019, 90, 1–12. [Google Scholar] [CrossRef]
- Yu, S.; Roh, Y.S. Needs assessment survey for simulation-based training for gastrointestinal endoscopy nurses. Nurs. Health Sci. 2018, 20, 247–254. [Google Scholar] [CrossRef]
- Nguyen-Vu, T.; Malvar, C.; Chin, Y.K.; Kaltenbach, T.; Liu, A.; Myint, T.; Asokkumar, R.; Shergill, A.; Soetikno, R. Simulation-based mastery learning (SBML) for rapid acquisition of upper endoscopy knowledge and skills–initial observation. Videogie 2020, 5, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Hann, A.; Walter, B.M.; Mehlhase, N.; Meining, A. Virtual reality in GI endoscopy: Intuitive zoom for improving diagnostics and training. Gut 2019, 68, 957–959. [Google Scholar] [CrossRef]
- Walsh, C.M.; Cohen, J.; Woods, K.L.; Wang, K.K.; Andersen, D.K.; Anderson, M.A.; Dunkin, B.J.; Edmundowicz, S.A.; Faigel, D.O.; Law, J.K.; et al. ASGE EndoVators Summit: Simulators and the future of endoscopic training. Gastrointest. Endosc. 2019, 90, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Ritter, E.M.; Taylor, Z.A.; Wolf, K.R.; Franklin, B.R.; Placek, S.B.; Korndorffer, J.R.; Gardner, A.K. Simulation-based mastery learning for endoscopy using the endoscopy training system: A strategy to improve endoscopic skills and prepare for the fundamentals of endoscopic surgery (FES) manual skills exam. Surg. Endosc. 2018, 32, 413–420. [Google Scholar] [CrossRef]
- Morita, A.; Kudo, T.; Horiuchi, A.; Kajiyama, M.; Tanaka, N.; Takada, H. Short-term intensive gastrointestinal endoscopy training program. Pediatr. Int. 2022, 64, e14721. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).