
Urinary Tract Infections in Patients Hospitalized in a Gastroenterology Department—Study from a Tertiary Regional Hospital in South-East Poland


Abstract
1. Introduction
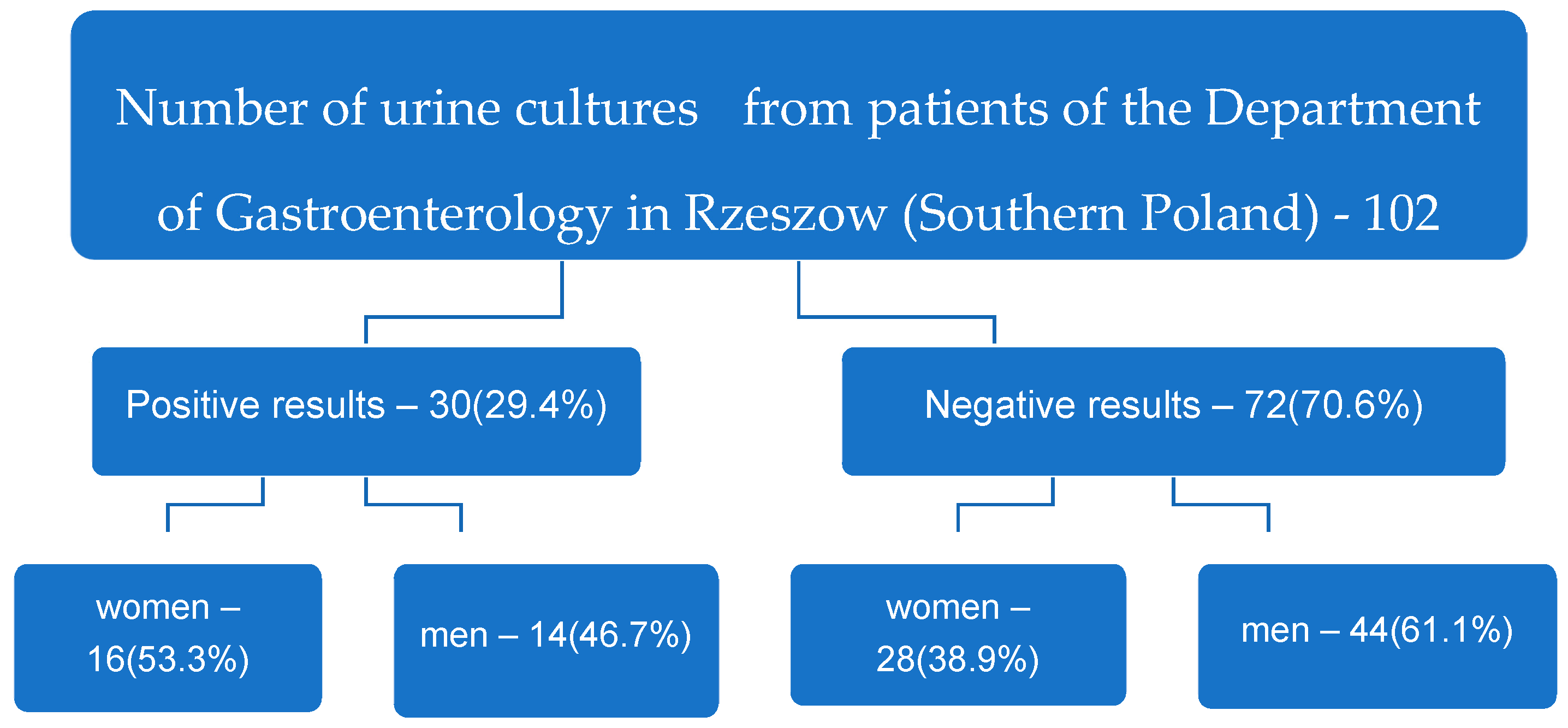
2. Results
3. Discussion
4. Materials and Methods
Ethics Statement
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zilberberg, M.D.; Shorr, A.F. Secular trends in gram-negative resistance among urinary tract infection hospitalizations in the United States, 2000–2009. Infect Control Hosp. Epidemiol. 2013, 34, 940–946. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, C.; Das-Mondal, M.; Gupta, D.; Sarkar, A.K.; Kar-Purkayastha, S.; Konar, A. Infection in cirrhosis: A prospective study. Ann. Hepatol. 2019, 18, 862–868. [Google Scholar] [CrossRef]
- Cohn, E.B.; Schaeffer, A.J. Urinary Tract Infections in Adults. Sci. World J. 2004, 4, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Hughes, T.; Juliebø-Jones, P.; Saada, L.; Saeed, K.; Somani, B.K. Recurrent urinary tract infections in adults: A practical guide. Br. J. Hosp. Med. 2021, 82, 1–11. [Google Scholar] [CrossRef]
- Ofek, I.; Beachey, E.H. General concepts and principles of bacterial adherence in animals and man, receptors and recognition. In Bacterial Adherence; Beachey, E.H., Ed.; Chapman and Hall: London, UK, 1980; pp. 3–29. [Google Scholar]
- Bonkat, G.; Cai, T.; Veeratterapillay, R.; Bruyère, F.; Bartoletti, R.; Pilatz, A.; Köves, B.; Geerlings, S.E.; Pradere, B.; Pickard, R.; et al. Management of Urosepsis in 2018. Eur. Urol. Focus 2019, 5, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Mazzariol, A.; Bazaj, A.; Cornaglia, G. Multi-drug-resistant Gram-negative bacteria causing urinary tract infections: A review. J. Chemother. 2017, 29, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Tandogdu, Z.; Wagenlehner, F.M. Global epidemiology of urinary tract infections. Curr. Opin. Infect. Dis. 2016, 29, 73–79. [Google Scholar] [CrossRef]
- Czajkowski, K.; Broś-Konopielko, M.; Teliga-Czajkowska, J. Urinary tract infection in women. Menopause Rev. 2021, 20, 40–47. [Google Scholar] [CrossRef]
- Ukashi, O.; Barash, Y.; Klang, E.; Zilberman, T.; Ungar, B.; Kopylov, U.; Ben-Horin, S.; Veisman, I. Adverse Clinical Outcomes among Inflammatory Bowel Disease Patients Treated for Urinary Tract Infection. J. Clin. Med. 2022, 11, 1359. [Google Scholar] [CrossRef]
- Kim, Y.N.; Jung, Y. Renal and Urinary Manifestations of Inflammatory Bowel Disease. Korean J. Gastroenterol. 2019, 73, 260–268. [Google Scholar] [CrossRef]
- Herbert, J.; Teeter, E.; Burstiner, L.S.; Doka, R.; Royer, A.; Owings, A.H.; Liu, J.; Glover, S.C.; Hosseini-Carroll, P. Urinary manifestations in African American and Caucasian infammatory bowel disease patients: A retrospective cohort study. BMC Urology. 2022, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, B.; Fasugba, O.; Beckingham, W.; Bennett, N.; Gardner, A. A point prevalence study of healthcare associated urinary tract infections in Australian acute and aged care facilities. Infect. Dis. Health 2016, 21, 26–31. [Google Scholar] [CrossRef]
- Dzierżanowska, D. Zakażenia układu moczowo-płciowego. In Antybiotykoterapia Praktyczna, 6th ed.; Alfa-Medica Press: Bielsko Biała, Poland, 2018; pp. 633–664. [Google Scholar]
- Escherich, T. Die darmbakterien des neugeborenen und säuglings. Fortschr. Med. 1885, 3, 515–522, 547–554. [Google Scholar]
- Pappelbaum, K.; Kasprzak, J.; Czaczyk, K. Występowanie werotoksycznych Escherichia coli w żywności, ze szczególnym uwzględnieniem serotypu O104:H4. Żywność. Nauka. Technologia. Jakość. 2015, 5, 33–48. [Google Scholar]
- Mazur, E.; Chmiel, M.J. Piaskownice jako potencjalne źródło zagrożenia lekoopornymi szczepami Escherichia coli oraz Staphylococcus aureus. Postępy Mikrobiol.-Adv. Microbiol. 2021, 60, 77–89. [Google Scholar] [CrossRef]
- Kim, K.S. Human meningitis-associated Escherichia coli. EcoSal Plus 2016, 7, 1–20. [Google Scholar] [CrossRef]
- Maslikowska, J.A.; Walker, S.A.N.; Elligsen, M.; Palmay, L.; Daneman, N.; Simor, A. Impact of infection with extended-spectrum β-lactamase-producing Escherichia coli or Klebsiella species on outcome and hospitalization costs. J. Hosp. Infect. 2016, 92, 33–41. [Google Scholar] [CrossRef]
- Korsak, D.; Popowska, M. Oporność bakterii na antybiotyki. In Antybiotyki w Dobie Narastającej Lekooporności; Markiewicz, Z., Korsak, D., Popowska, M., Eds.; Wydawnictwo Naukowe PWN: Warsaw, Poland, 2021; pp. 187–337. [Google Scholar]
- Bush, K.; Bradford, P.A. β-Lactams and β-Lactamase Inhibitors: An Overview. Cold Spring Harb. Perspect. Med. 2016, 6, a025247. [Google Scholar] [CrossRef]
- Dzierżanowska-Fangrat, K. Zakażenia układu moczowo-płciowego. In Przewodnik Antybiotykoterapii, 26th ed.; Alfa-Medica Press: Bielsko Biała, Poland, 2021; pp. 60–79. [Google Scholar]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Multistate point-prevalence survey of healthcare-associated infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef]
- Bushman, W.; Le, B.V. Nawracające zakażenia dróg moczowych po menopauzie. Ginekologia po Dyplomie. 2017, 1, 47–49. [Google Scholar]
- Bajaj, J.S.; O’Leary, J.G.; Reddy, K.R.; Wong, F.; Olson, J.C.; Subramanian, R.M.; Brown, G.; Noble, N.A.; Thacker, L.R.; Kamath, P.S. Second Infections Independently increase mortality in hospitalized patients with cirrhosis: The North American Consortium for the study of end stage liver disease (NACSELD) experience. Hepatology 2012, 56, 2328–2335. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.; Acevedo, J.; Castro, M.; Garcia, O.; de Lope, C.R.; Roca, D.; Pavesi, M.; Sola, E.; Moreira, L.; Silva, A.; et al. Prevalence and risk factors of infections by multiresistant bacteria in cirrhosis: A prospective study. Hepatology 2012, 55, 1551–1561. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.; Harris, P.N.; Williamson, D.A.; Liss, M.A.; Doi, S.A.R.; Roberts, M.J. The effectiveness of targeted relative to empiric prophylaxis on infectious complications after transrectal ultrasound-guided prostate biopsy: A meta-analysis. World J. Urol. 2018, 36, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- EAU Guidelines; Edn. presented at the EAU Annual Congress Amsterdam, the Netherlands; EAU Guidelines Office: Arnhem, The Netherlands, 2022; ISBN 978-94-92671-16-5. p. 9. Available online: http://uroweb.org/guidelines/compilations-of-all-guidelines/ (accessed on 20 March 2023).
- Strus, M. Zakażenia narządów płciowych i układu moczowego. In Mikrobiologia Lekarska; Heczko, P.B., Wróblewska, M., Pietrzyk, A., Eds.; PZWL (National Institute of Medical Publications): Warsaw, Poland, 2022; pp. 715–718. [Google Scholar]
- Jung, J.; Kim, S.Y.; Park, Y.J.; Lee, J.; Suk, H.S.; Ha, S.I.; Shin, J.S.; Park, K.G.; Kim, Y. Comparison of the ASTA MicroIDSys and VITEK MS matrix-assisted laser desorption/ionization time-of-flight mass spectrometry systems for identification of clinical bacteria and yeasts. J. Infect Chemother. 2020, 26, 1328–1333. [Google Scholar] [CrossRef]
- Luo, Y.; Siu, K.H.; Yeung, A.S.F.; Chen, J.H.K.; Ho, P.L.; Leung, K.W.; Tsang, J.L.Y.; Cheng, V.C.C.; Guo, L.; Yang, J.; et al. Performance of the VITEK MS matrix-assisted laser desorption ionization-time of flight mass spectrometry system for rapid bacterial identification in two diagnostic centres in China. J. Med. Microbiol. 2015, 64, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Kovaleva, J. Infectious complications in gastrointestinal endoscopy and their prevention. Best. Pr. Res. Clin. Gastroenterol. 2016, 30, 689–704. [Google Scholar] [CrossRef]
- Sanguinetti, M.; Posteraro, B. Identification of Molds by Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry. J. Clin. Mikrobiol. 2017, 55, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Knabl, L.; Huber, S.; Lass-Flörl, C.; Fuchs, S. Comparison of novel approaches for expedited pathogen identification and antimicrobial susceptibility testing against routine blood culture diagnostics. Lett. Appl. Microbiol. 2021, 73, 2–8. [Google Scholar] [CrossRef]


{kind=link}
| The Microorganisms Identified n | E. coli 8 | E. coli, ESBL 2 | E. faecalis 5 | E. faecium 4 | K. pneumoniae, ESBL 3 | P. mirabilis 3 | P. aeruginosa 1 | S. epidermidis, MRCNS 1 | S. capitis, MRCNS 1 | C. albicans 1 | C. tropicalis 1 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| The Number of Sensitive Microorganisms, n (Percentages) | ||||||||||||
| AK | 8 (100%) | 1 (50%) | 3 (100%) | 3 (100%) | 1 (100%) | 1 (100%) | ||||||
| AMC | 4 (50%) | 2 (100%) | 2 (66.6%) | |||||||||
| ATM | 1 (100%) | |||||||||||
| CAZ | 8 (100%) | 3 (100%) | 1 (100%) | |||||||||
| CTX | 8 (100%) | 1 (33.3%) | 3 (100%) | |||||||||
| CXM | 8 (100%) | 1 (33.3%) | 2 (66.6%) | |||||||||
| CIP | 6 (75%) | 1 (33.3%) | 3 (100%) | |||||||||
| CT | 8 (100%) | 2 (66.6%) | ||||||||||
| FEP | 8 (100%) | 1 (33.3%) | 3 (100%) | 1 (100%) | ||||||||
| GM | 7 (87.5%) | 1 (50%) | 1 (33.3%) | 3 (100%) | 1 (100%) | |||||||
| IPM | 8 (100%) | 2 (100%) | 5 (100%) | 3 (100%) | 3 (100%) | 1 (100%) | ||||||
| MEM | 8 (100%) | 2 (100%) | 3 (100%) | 3 (100%) | 1 (100%) | |||||||
| TZP | 8 (100%) | 2 (100%) | 3 (100%) | 1 (100%) | ||||||||
| TGC | 8 (100%) | 2 (100%) | 5 (100%) | 4 (100%) | 1 (100%) | 1 (100%) | ||||||
| TM | 8 (100%) | 1 (50%) | 3 (100%) | 1 (100%) | ||||||||
| TIM | 1 (33.3%) | 1 (100%) | ||||||||||
| SXT | 7 (87.5%) | 1 (50%) | 2 (66.6%) | 2 (66.6%) | 1 (100%) | |||||||
| AM | 5 (100%) | |||||||||||
| LEV | 1 (20%) | |||||||||||
| LZD | 5 (100%) | 4 (100%) | 1 (100%) | 1 (100%) | ||||||||
| F | 5 (100%) | |||||||||||
| S | ||||||||||||
| TEC | 5 (100%) | 1 (100%) | 1 (100%) | |||||||||
| VA | 5 (100%) | 4 (100%) | 1 (100%) | 1 (100%) | ||||||||
| CM | 1 (100%) | 1 (100%) | ||||||||||
| E | 1 (100%) | 1 (100%) | ||||||||||
| OX | ||||||||||||
| TE | 1 (100%) | 1 (100%) | ||||||||||
| PIP | 1 (100%) | |||||||||||
| AmB | 1 (100%) | 1 (100%) | ||||||||||
| CAS | 1 (100%) | 1 (100%) | ||||||||||
| FLU | 1 (100%) | 1 (100%) | ||||||||||
| AFY | 1 (100%) | |||||||||||
| MYC | 1 (100%) | 1 (100%) | ||||||||||
| VO | 1 (100%) | 1 (100%) | ||||||||||
| Characteristics of the Patients | Positive Urine Culture Results (n = 30) | Negative Urine Culture Results (n = 72) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Women (n = 16) | Men (n = 14) | Women (n = 28) | Men (n = 44) | |||||||||
| Age of patients, years | 33–101 | 27–93 | 30–87 | 26–99 | ||||||||
| Age of patients—arithmetic mean, years (standard deviation) | 75.6 (17.17) | 61.7 (18.3) | 66.1 (18.7) | 63.2 (17.2) | ||||||||
| Duration of hospitalization, days | 2–35 | |||||||||||
| Duration of hospitalization—arithmetic mean, days (standard deviation) | 11.6 (7.1) | |||||||||||
| The diagnoses with which the patients reported to the hospital (concerns all 102 examined patients), n | IBD, 4 | Liver cirrhosis, 35 | Pancreatitis, 14 | Gastrointestinal bleeding, 18 | Diverticulosis of the large intestine, 2 | Other, 29 ** | ||||||
| Urine culture result/quantity (%) * | −/4 | +/0 | −/23 | +/12 (34.3) | −/13 | +/1 (7.1) | −/13 | +/5 (27.8) | −/0 | +/2 (100) | −/19 | +/10 (34.5) |
| Origin of the infection | community-acquired | hospital-acquired | ||||||||||
| n = 20 | n = 10 | |||||||||||
| Women—11 | Men—9 | Women—5 | Men—5 | |||||||||
| Diagnoses with which the patients reported to the hospital (applies to the 30 patients with positive urine cultures), n | Liver cirrhosis, 14 | Pancreatitis, 8 | Diverticulosis of the large intestine, 2 | Cholecystitis, 2 | Duodenitis, 2 | Duodenalulcer, 2 | ||||||
| Treatment effect | Improvement—21 | Death—9 | ||||||||||
| Patients with a positive urine culture and a urinary catheter, n | 26 | |||||||||||
| Women—13 | Men—13 | |||||||||||
| Taking samples for testing | All samples were taken during hospitalization. | |||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gruszecka, J.; Filip, R. Urinary Tract Infections in Patients Hospitalized in a Gastroenterology Department—Study from a Tertiary Regional Hospital in South-East Poland. Gastrointest. Disord. 2023, 5, 198-208. https://doi.org/10.3390/gidisord5020017
Gruszecka J, Filip R. Urinary Tract Infections in Patients Hospitalized in a Gastroenterology Department—Study from a Tertiary Regional Hospital in South-East Poland. Gastrointestinal Disorders. 2023; 5(2):198-208. https://doi.org/10.3390/gidisord5020017
Chicago/Turabian StyleGruszecka, Jolanta, and Rafał Filip. 2023. "Urinary Tract Infections in Patients Hospitalized in a Gastroenterology Department—Study from a Tertiary Regional Hospital in South-East Poland" Gastrointestinal Disorders 5, no. 2: 198-208. https://doi.org/10.3390/gidisord5020017
APA StyleGruszecka, J., & Filip, R. (2023). Urinary Tract Infections in Patients Hospitalized in a Gastroenterology Department—Study from a Tertiary Regional Hospital in South-East Poland. Gastrointestinal Disorders, 5(2), 198-208. https://doi.org/10.3390/gidisord5020017