The Impact of EMG Biofeedback on Evacuation Difficulty Level and Pain Grade During Defecation in Chronically Constipated Elderly Female Patients Due to Dyssynergic Defecation



Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Measures
4.3. Procedure
4.4. Design
4.5. Data Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Rao, S.S.; Patcharatrakul, T. Diagnosis and treatment of dyssynergic defecation. J. Neurogastroenterol. Motil. 2016, 22, 423–435. [Google Scholar] [CrossRef] [PubMed]
- Chiarioni, G.; Heymen, S.; Whitehead, W.E. Biofeedback therapy for dyssynergic defecation. World J. Gastroenterol. 2006, 12, 7069–7074. [Google Scholar] [CrossRef] [PubMed]
- Cadeddu, F.; Salis, F.; De Luca, E.; Ciangola, I.; Milito, G. Efficacy of biofeedback plus transanal stimulation in the management of pelvic floor dyssynergia: A randomized trial. Tech. Coloproctol. 2015, 19, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Hart, S.L.; Lee, J.W.; Berian, J.; Patterson, T.R.; Del Rosario, A.; Varma, M.G. A randomized controlled trial of anorectal biofeedback for constipation. Int. J. Colorectal. Dis. 2012, 27, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Heymen, S.; Scarlett, Y.; Jones, K.; Ringel, Y.; Drossman, D.; Whitehead, W.E. Randomized controlled trial shows biofeedback to be superior to alternative treatments for patients with pelvic floor dyssynergia-type constipation. Dis. Colon Rectum 2007, 50, 428–441. [Google Scholar] [CrossRef] [PubMed]
- Simón, M.A.; Bueno, A.M. Behavioural treatment of the dyssynergic defecation in chronically constipated elderly patients: A randomized controlled trial. Appl. Psychophysiol. Biofeedback 2009, 34, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Simón, M.A.; Bueno, A.M. Efficacy of biofeedback therapy in the treatment of dyssynergic defecation in community-dwelling elderly women. J. Clin. Gastroenterol. 2017, 51, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.S.; Valestin, J.; Brown, C.K.; Zimmerman, B.; Schulze, K. Long-term efficacy of biofeedback therapy for dyssynergic defecation: Randomized controlled trial. Am. J. Gastroenterol. 2010, 105, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Boo, S.J.; Jung, K.W.; Han, S.; Seo, S.Y.; Koo, H.S.; Yoon, I.J.; Park, S.H.; Yang, D.H.; Kim, K.J.; et al. Long-term efficacy of biofeedback therapy in patients with dyssynergic defecation: Results of a median 44 months follow-up. Neurogastroenterol. Motil. 2015, 27, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Simón, M.A.; Bueno, A.M. Relevance of the clinical and psychophysiological variables in the dyssynergic defecation: A comparative study in elderly subjects. Appl. Psychophysiol. Biofeedback 2017, 42, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Mason, H.J.; Serrano-Ikkos, E.; Kamm, M.A. Psychological morbidity in women with idiopathic constipation. Am. J. Gastroenterol. 2000, 95, 2852–2857. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Chan, A.O.; Hui, W.M.; Lam, S.K. Coping strategis, illness perception, anxiety and depression of patients with idiopathic constipation: A population-based study. Aliment. Pharmacol. Ther. 2003, 18, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.S.; Seaton, K.; Miller, M.J.; Schulze, K.; Brown, C.K.; Paulson, J.; Zimmerman, B. Psychological profiles and quality of life differ between patients with dyssynergia and those with slow transit constipation. J. Psychosomat. Res. 2007, 63, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Belsey, J.; Greenfield, S.; Candy, D.; Geraint, M. Systematic review: Impact of constipation on quality of life in adults and children. Aliment. Pharmacol. Ther. 2010, 31, 938–949. [Google Scholar] [CrossRef] [PubMed]
- Wald, A.; Bharucha, A.E.; Enck, P.; Rao, S.S. Functional anorectal disorders. In Rome III. The functional gastrointestinal disordersI, 3rd ed.; Drossman, D.A., Corazziari, E., Eds.; Degnon Associates: McLean, VA, USA, 2006; pp. 639–685. ISBN 0-9656837-5-3. [Google Scholar]

{kind=link}
{kind=link}
| EMG-BF (n = 8) | Conventional (n = 8) | |
|---|---|---|
| Age (years) | 77.12 (±3.18) | 73.50 (±4.31) |
| Disease duration (years) | 9.00 (±2.14) | 11.25 (±3.45) |
| Weekly stool frequency | 1.87 (±0.35) | 1.50 (±0.53) |
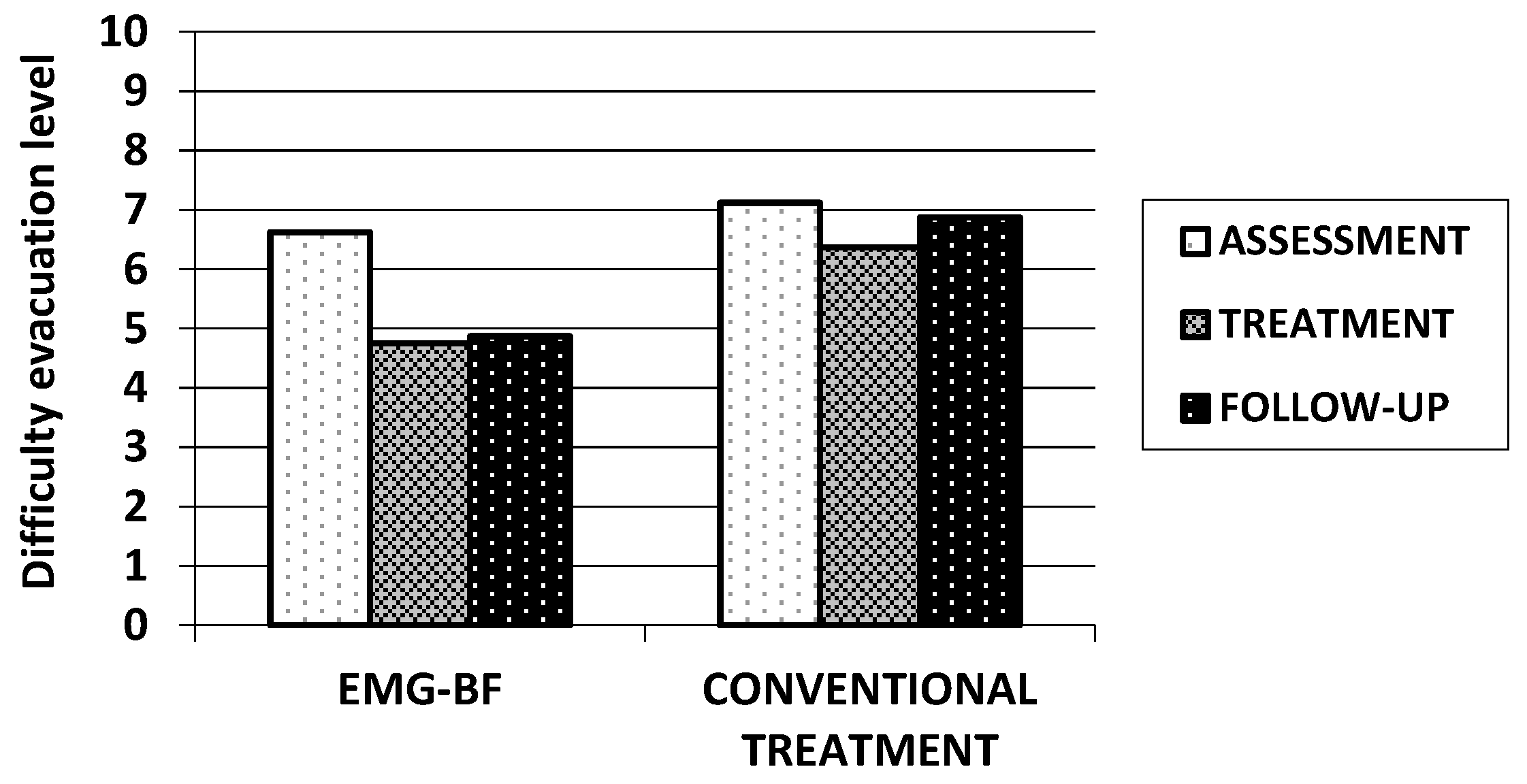
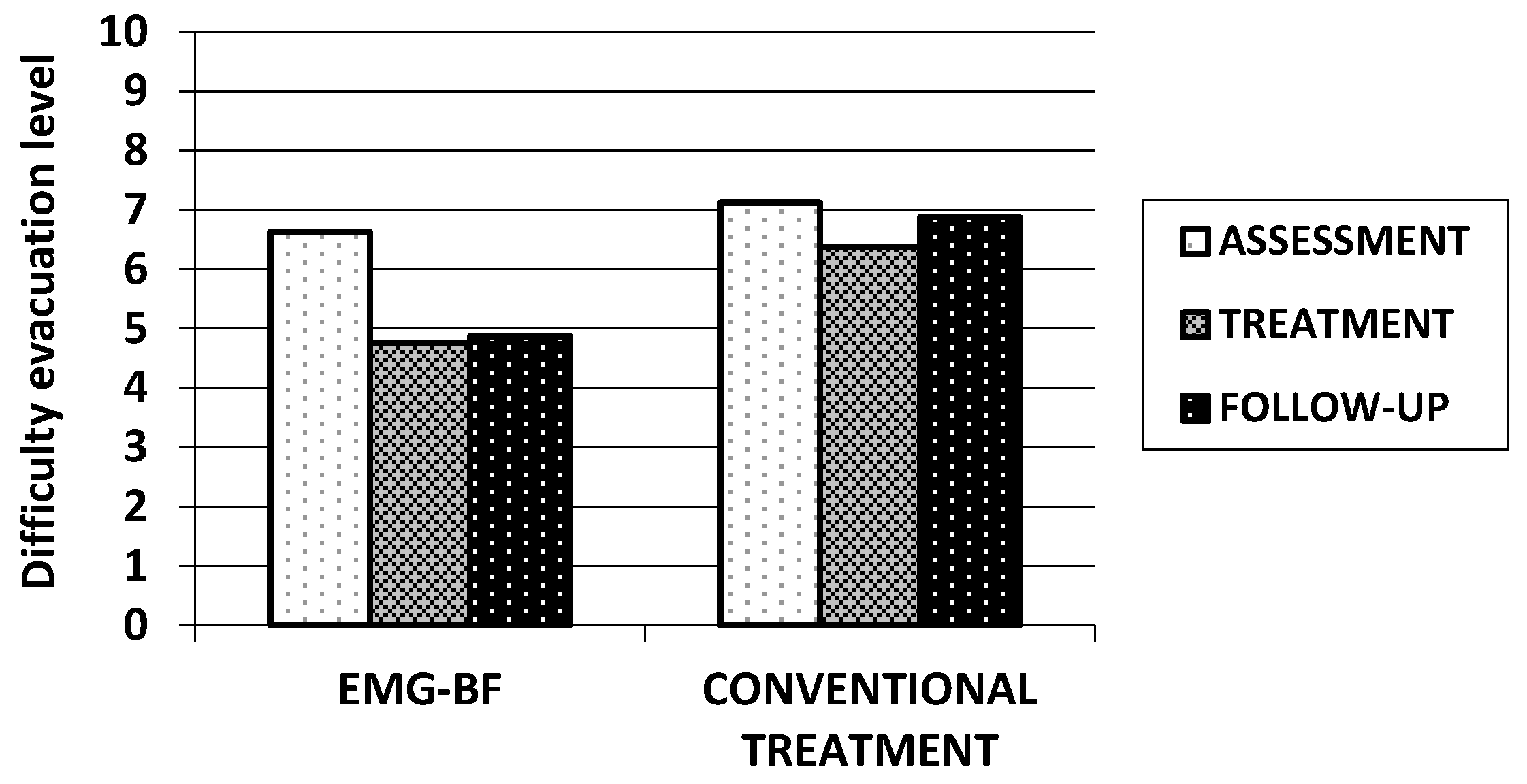
| Evacuation difficulty level | 6.62 (±0.92) | 7.12 (±0.35) |
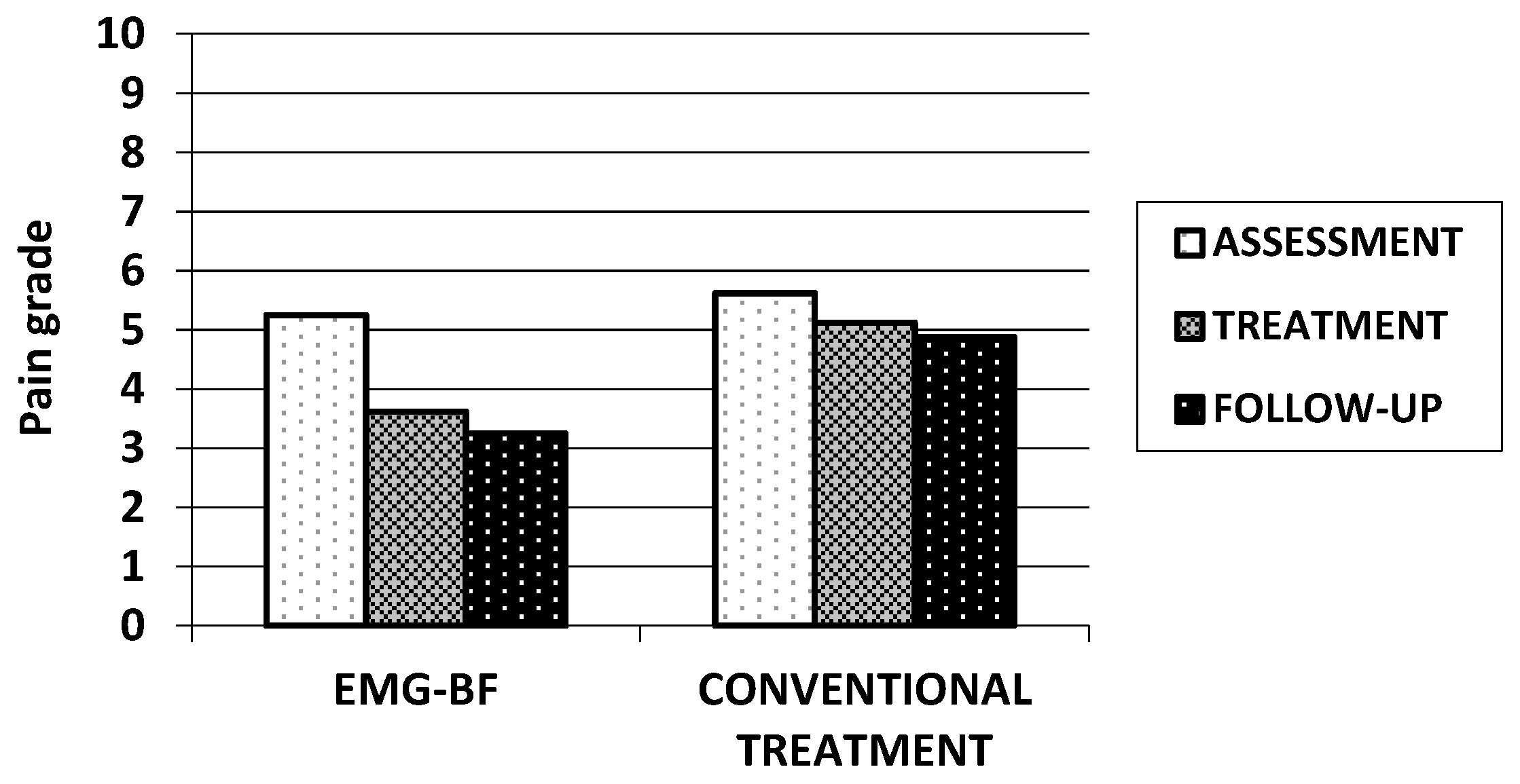
| Pain grade during defecation | 5.25 (±0.71) | 5.62 (±0.74) |
| EMG activity (µV) during straining to defecate | 10.04 (±2.15) | 11.05 (±3.16) |
| EMG-BF (n = 8) | Conventional (n = 8) | F Value * | |
|---|---|---|---|
| Weekly stool frequency | 3.62 (±0.52) | 1.75 (±0.46) | 58.33 |
| Evacuation difficulty level | 4.75 (±0.89) | 6.37 (±0.52) | 20.05 |
| Pain grade during defecation | 3.62 (±0.74) | 5.12 (±0.83) | 14.40 |
| EMG activity (µV) during straining to defecate | 5.56 (±1.32) | 11.46 (±2.91) | 27.28 |
| EMG-BF (n = 8) | Conventional (n = 8) | F Value * | |
|---|---|---|---|
| Weekly stool frequency | 3.50 (±0.53) | 1.62 (±0.52) | 50.81 |
| Evacuation difficulty level | 4.87 (±0.83) | 6.87 (±0.64) | 28.90 |
| Pain grade during defecation | 3.25 (±0.46) | 4.88 (±0.66) | 33.80 |
| EMG-activity (µV) during straining to defecate | 4.82 (±0.75) | 10.11 (±2.46) | 33.97 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simón, M.A.; Bueno, A.M.; Otero, P. The Impact of EMG Biofeedback on Evacuation Difficulty Level and Pain Grade During Defecation in Chronically Constipated Elderly Female Patients Due to Dyssynergic Defecation. Gastrointest. Disord. 2019, 1, 308-313. https://doi.org/10.3390/gidisord1030026
Simón MA, Bueno AM, Otero P. The Impact of EMG Biofeedback on Evacuation Difficulty Level and Pain Grade During Defecation in Chronically Constipated Elderly Female Patients Due to Dyssynergic Defecation. Gastrointestinal Disorders. 2019; 1(3):308-313. https://doi.org/10.3390/gidisord1030026
Chicago/Turabian StyleSimón, Miguel A., Ana M. Bueno, and Patricia Otero. 2019. "The Impact of EMG Biofeedback on Evacuation Difficulty Level and Pain Grade During Defecation in Chronically Constipated Elderly Female Patients Due to Dyssynergic Defecation" Gastrointestinal Disorders 1, no. 3: 308-313. https://doi.org/10.3390/gidisord1030026
APA StyleSimón, M. A., Bueno, A. M., & Otero, P. (2019). The Impact of EMG Biofeedback on Evacuation Difficulty Level and Pain Grade During Defecation in Chronically Constipated Elderly Female Patients Due to Dyssynergic Defecation. Gastrointestinal Disorders, 1(3), 308-313. https://doi.org/10.3390/gidisord1030026