
Risk of Comorbid Insomnia Disorder Associated with Major Depression in Apneic Patients: A Cross-Sectional Study

 ,
,
Abstract
1. Introduction
2. Results
2.1. Polysomnographic Data (Table 1)
2.2. Demographic Data (Table 2)
2.3. Multivariate Analyses (Table 3)
3. Discussion
Limitations and Strengths
4. Materials and Methods
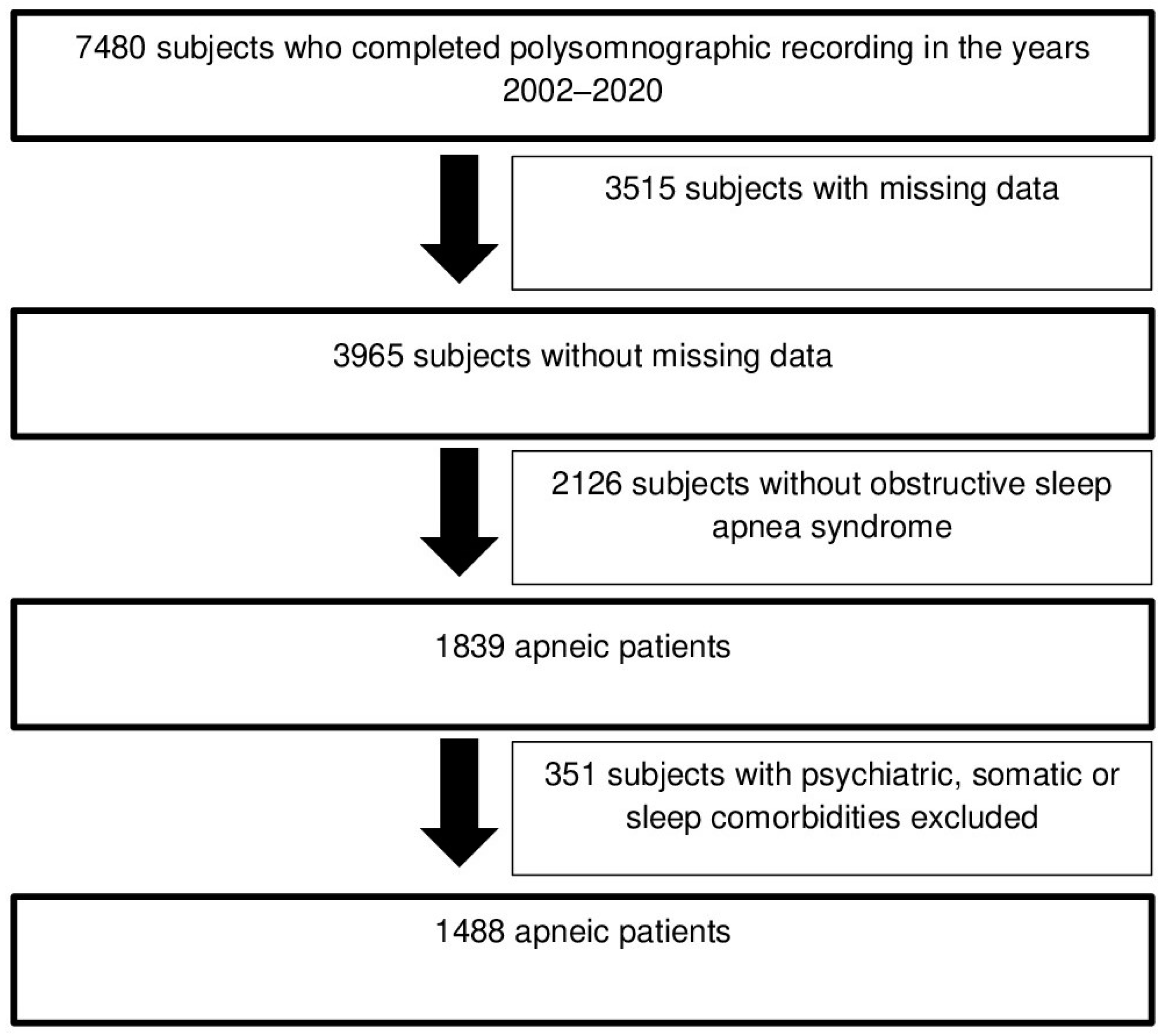
4.1. Population
4.2. Method
4.2.1. Medical and Psychiatric Assessment
- The Beck Depression Inventory (reduced to 13 items) was used to investigate the presence of depressive symptoms. The 13 items of this scale may be scored from 0 to 3, which means that the total score may vary from 0 to 39. A final score of 0–4 indicates an absence of depressive symptoms, 5–7 indicates mild depressive symptoms, 8–15 indicates moderate depressive symptoms, and ≥16 indicates severe depressive symptoms [49]. The internal consistency reliability measure showed a Cronbach α coefficient of 0.90 for the French version of The Beck Depression Inventory (reduced to 13 items) [50].
- The Insomnia Severity Index was used to investigate the severity of insomnia complaints. The 7 items of this index may be scored from 0 to 4, which means that the total score may vary from 0 to 28. A final score of 0–7 indicates an absence of insomnia complaints, 8–14 indicates subclinical insomnia complaints, 15–21 indicates moderate insomnia complaints, and 22–28 indicates severe insomnia complaints [51]. The internal consistency reliability measure showed a Cronbach α coefficient of 0.92 for the French version of the Insomnia Severity Index [52].
- The Epworth Sleepiness Scale was used to investigate daytime sleepiness. The 8 items of this scale assessing sleepiness in different daytime situations may be scored from 0 to 3, which means that the total score may vary from 0 to 24. A final score greater than 10 indicates excessive daytime sleepiness [53]. The internal consistency reliability measure showed a Cronbach α coefficient of 0.88 for the French version of the Epworth Sleepiness Scale [54].
4.2.2. Sleep Evaluation and Study
4.3. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vozoris, N.T. Sleep apnea-plus: Prevalence, risk factors, and association with cardiovascular diseases using United States population-level data. Sleep Med. 2012, 13, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Hein, M.; Lanquart, J.P.; Loas, G.; Hubain, P.; Linkowski, P. Prevalence and risk factors of excessive daytime sleepiness in insomnia sufferers: A study with 1311 individuals. J. Psychosom. Res. 2017, 103, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Hein, M.; Wacquier, B.; Lanquart, J.P.; Loas, G. Risk of Cardiovascular Disease in Apnoeic Individuals: Role of Comorbid Insomnia Disorder. Life 2022, 12, 944. [Google Scholar] [CrossRef] [PubMed]
- Hein, M.; Lanquart, J.P.; Mungo, A.; Loas, G. Cardiovascular risk associated with co-morbid insomnia and sleep apnoea (COMISA) in type 2 diabetics. Sleep Sci. 2022, 15, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Draelants, L.; Point, C.; Wacquier, B.; Lanquart, J.P.; Loas, G.; Hein, M. 10-Year Risk for Cardiovascular Disease Associated with COMISA (Co-Morbid Insomnia and Sleep Apnea) in Hypertensive Subjects. Life 2023, 13, 1379. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.C.; Crawford, M.R.; Wallace, D.M. Sleep Apnea and Insomnia: Emerging Evidence for Effective Clinical Management. Chest 2021, 159, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.M.; Sawyer, A.M.; Shafazand, S. Comorbid insomnia symptoms predict lower 6-month adherence to CPAP in US veterans with obstructive sleep apnea. Sleep Breath. 2018, 22, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Bach, M.; Popp, R.; Jara, C.; Crönlein, T.; Hajak, G.; Geisler, P. Insomnia symptoms influence CPAP compliance. Sleep Breath. 2013, 17, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Hein, M.; Lanquart, J.P.; Loas, G.; Hubain, P.; Linkowski, P. Prevalence and risk factors of excessive daytime sleepiness in major depression: A study with 703 individuals referred for polysomnography. J. Affect. Disord. 2019, 243, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Dosogne, M.; Wacquier, B.; Al Faker, M.; Willame, H.; Point, C.; Loas, G.; Hein, M. Risk of current suicidal ideations associated with lifelong anhedonia and recent change of anhedonia in individuals with insomnia: A cross-sectional study. J. Psychiatr. Res. 2022, 150, 338–345. [Google Scholar] [CrossRef]
- Li, L.; Wu, C.; Gan, Y.; Qu, X.; Lu, Z. Insomnia and the risk of depression: A meta-analysis of prospective cohort studies. BMC Psychiatry 2016, 16, 375. [Google Scholar] [CrossRef]
- Bao, Y.P.; Han, Y.; Ma, J.; Wang, R.J.; Shi, L.; Wang, T.Y.; He, J.; Yue, J.L.; Shi, J.; Tang, X.D.; et al. Cooccurrence and bidirectional prediction of sleep disturbances and depression in older adults: Meta-analysis and systematic review. Neurosci. Biobehav. Rev. 2017, 75, 257–273. [Google Scholar] [CrossRef] [PubMed]
- Kwaśny, A.; Włodarczyk, A.; Dywel, A.; Szarmach, J.; Strandberg, O.; Cubała, W.J. Residual insomnia in major depressive disorder: A systematic review. Front. Psychiatry 2023, 14, 1190415. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, H.; Suzuki, T.; Yoshimura, K.; Mimura, M.; Uchida, H. Predicting relapse with individual residual symptoms in major depressive disorder: A reanalysis of the STAR*D data. Psychopharmacology 2017, 234, 2453–2461. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.L.; Tolson, J.; Bartlett, D.; Berlowitz, D.J.; Varma, P.; Barnes, M. Clinical depression in untreated obstructive sleep apnea: Examining predictors and a meta-analysis of prevalence rates. Sleep Med. 2019, 62, 22–28. [Google Scholar] [CrossRef]
- Sweetman, A.; Melaku, Y.A.; Lack, L.; Reynolds, A.; Gill, T.K.; Adams, R.; Appleton, S. Prevalence and associations of co-morbid insomnia and sleep apnoea in an Australian population-based sample. Sleep Med. 2021, 82, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Stelzer, F.G.; Garcia, E.; Schorr, F.; Barea, L.M.; Barros, H.T. Prevalence of chronic insomnia in patients with obstructive sleep apnea. Braz. J. Psychiatry 2021, 43, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.M.; Wohlgemuth, W.K. Predictors of Insomnia Severity Index Profiles in United States Veterans with Obstructive Sleep Apnea. J. Clin. Sleep Med. 2019, 15, 1827–1837. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.J.; Appleton, S.L.; Vakulin, A.; McEvoy, R.D.; Wittert, G.A.; Martin, S.A.; Catcheside, P.G.; Antic, N.A.; Lack, L.; Adams, R.J. Co-morbid OSA and insomnia increases depression prevalence and severity in men. Respirology 2017, 22, 1407–1415. [Google Scholar] [CrossRef] [PubMed]
- Hagen, C.; Patel, A.; McCall, W.V. Prevalence of insomnia symptoms in sleep laboratory patients with and without sleep apnea. Psychiatry Res. 2009, 170, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.W.; Kim, K.T.; Moon, H.J.; Korostyshevskiy, V.R.; Motamedi, G.K.; Yang, K.I. Comorbid Insomnia with Obstructive Sleep Apnea: Clinical Characteristics and Risk Factors. J. Clin. Sleep Med. 2018, 14, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, B.L.; Hagen, K.; Engstrøm, M.; Stjern, M.; Gravdahl, G.B.; Sand, T. The relationship between obstructive sleep apnea and insomnia: A population-based cross-sectional polysomnographic study. Sleep Med. 2019, 54, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Hein, M.; Lanquart, J.P.; Loas, G.; Hubain, P.; Linkowski, P. Prevalence and risk factors of moderate to severe obstructive sleep apnea syndrome in insomnia sufferers: A study on 1311 subjects. Respir. Res. 2017, 18, 135. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.Y.; Chang, L.Y.; Hsieh, Y.J.; Tsai, P.S. A meta-analysis of diagnostic accuracy of three screening tools for insomnia. J. Psychosom. Res. 2016, 87, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ren, R.; Lei, F.; Zhou, J.; Zhang, J.; Wing, Y.K.; Sanford, L.D.; Tang, X. Worldwide and regional prevalence rates of co-occurrence of insomnia and insomnia symptoms with obstructive sleep apnea: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 45, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Al Faker, M.; Wacquier, B.; Willame, H.; Point, C.; Dosogne, M.; Loas, G.; Hein, M. The association between type 2 diabetes and major depression in apnoeic individuals. Sleep Biol. Rhythm. 2022, 20, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Schröder, C.M.; O’Hara, R. Depression and Obstructive Sleep Apnea (OSA). Ann. Gen. Psychiatry 2005, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Glozier, N.; Ratnavadivel, R.; Grunstein, R.R. Obstructive sleep apnea and depression. Sleep Med. Rev. 2009, 13, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Ejaz, S.M.; Khawaja, I.S.; Bhatia, S.; Hurwitz, T.D. Obstructive sleep apnea and depression: A review. Innov. Clin. Neurosci. 2011, 8, 17–25. [Google Scholar] [PubMed]
- Hein, M.; Lanquart, J.P.; Loas, G.; Hubain, P.; Linkowski, P. Contribution to the study of physiology and pathophysiology of sleep in healthy individual and patients suffering from major depression and primary insomnia. Rev. Med. Brux. 2020, 41, 137–142. [Google Scholar] [CrossRef]
- Hein, M.; Senterre, C.; Lanquart, J.P.; Montana, X.; Loas, G.; Linkowski, P.; Hubain, P. Hyperarousal during sleep in untreated primary insomnia sufferers: A polysomnographic study. Psychiatry Res. 2017, 253, 71–78. [Google Scholar] [CrossRef]
- Hein, M.; Senterre, C.; Lanquart, J.P.; Montana, X.; Loas, G.; Linkowski, P.; Hubain, P. Hyperarousal during sleep in untreated, major depressed subjects with prodromal insomnia: A polysomnographic study. Psychiatry Res. 2017, 258, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Hein, M.; Lanquart, J.P.; Loas, G.; Hubain, P.; Linkowski, P. Similar polysomnographic pattern in primary insomnia and major depression with objective insomnia: A sign of common pathophysiology? BMC Psychiatry 2017, 17, 273. [Google Scholar] [CrossRef] [PubMed]
- Dombrovski, A.Y.; Cyranowski, J.M.; Mulsant, B.H.; Houck, P.R.; Buysse, D.J.; Andreescu, C.; Thase, M.E.; Mallinger, A.G.; Frank, E. Which symptoms predict recurrence of depression in women treated with maintenance interpersonal psychotherapy? Depress. Anxiety 2008, 25, 1060–1066. [Google Scholar] [CrossRef] [PubMed]
- Meaklim, H.; Saunders, W.J.; Byrne, M.L.; Junge, M.F.; Varma, P.; Finck, W.A.; Jackson, M.L. Insomnia is a key risk factor for persistent anxiety and depressive symptoms: A 12-month longitudinal cohort study during the COVID-19 pandemic. J. Affect. Disord. 2023, 322, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Manber, R.; Chambers, A.S. Insomnia and depression: A multifaceted interplay. Curr. Psychiatry Rep. 2009, 11, 437–442. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; text rev; American Psychiatric Publishing: Arlington, VA, USA, 2000. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Heck, T.; Zolezzi, M. Obstructive sleep apnea: Management considerations in psychiatric patients. Neuropsychiatr. Dis. Treat. 2015, 11, 2691–2698. [Google Scholar] [PubMed]
- Benca, R.M.; Krystal, A.; Chepke, C.; Doghramji, K. Recognition and Management of Obstructive Sleep Apnea in Psychiatric Practice. J. Clin. Psychiatry 2023, 84, 22r14521. [Google Scholar] [CrossRef]
- Hertenstein, E.; Trinca, E.; Wunderlin, M.; Schneider, C.L.; Züst, M.A.; Fehér, K.D.; Su, T.; Straten, A.V.; Berger, T.; Baglioni, C.; et al. Cognitive behavioral therapy for insomnia in patients with mental disorders and comorbid insomnia: A systematic review and meta-analysis. Sleep Med. Rev. 2022, 62, 101597. [Google Scholar] [CrossRef] [PubMed]
- Manber, R.; Buysse, D.J.; Edinger, J.; Krystal, A.; Luther, J.F.; Wisniewski, S.R.; Trockel, M.; Kraemer, H.C.; Thase, M.E. Efficacy of Cognitive-Behavioral Therapy for Insomnia Combined with Antidepressant Pharmacotherapy in Patients with Comorbid Depression and Insomnia: A Randomized Controlled Trial. J. Clin. Psychiatry 2016, 77, e1316–e1323. [Google Scholar] [CrossRef]
- Fu, W.; Li, L.; Zhang, S.; Liu, S.; Liu, W. Effects of CPAP and Mandibular Advancement Devices on depressive symptoms in patients with obstructive sleep apnea: A meta-analysis of randomized controlled trials. Sleep Breath. 2023, 27, 2123–2137. [Google Scholar] [CrossRef] [PubMed]
- Sweetman, A.; Lack, L.; McEvoy, R.D.; Smith, S.; Eckert, D.J.; Osman, A.; Carberry, J.C.; Wallace, D.; Nguyen, P.D.; Catcheside, P. Bi-directional relationships between co-morbid insomnia and sleep apnea (COMISA). Sleep Med. Rev. 2021, 60, 101519. [Google Scholar] [CrossRef] [PubMed]
- Skarupke, C.; Schlack, R.; Lange, K.; Goerke, M.; Dueck, A.; Thome, J.; Szagun, B.; Cohrs, S. Insomnia complaints and substance use in German adolescents: Did we underestimate the role of coffee consumption? Results of the KiGGS study. J. Neural Transm. 2017, 124 (Suppl. S1), 69–78. [Google Scholar] [CrossRef] [PubMed]
- Hein, M.; Lanquart, J.P.; Loas, G.; Hubain, P.; Linkowski, P. Prevalence and risk factors of moderate to severe obstructive sleep apnea syndrome in major depression: A observational and retrospective study on 703 subjects. BMC Pulm. Med. 2017, 17, 165. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Dixon-Williams, S.; Thornton, J.D. Where there is smoke…there is sleep apnea: Exploring the relationship between smoking and sleep apnea. Chest 2014, 146, 1673–1680. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W. Comparison of Beck Depression Inventories-IA and-II in Psychiatric Outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Bourque, P.; Beaudette, D. Psychometric study of the Beck Depression Inventory on a sample of French-speaking university students. Can. J. Behav. Sci.-Rev. Can. Sci. Comport. 1982, 14, 211–218. [Google Scholar]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Gagnon, C.; Bélanger, L.; Ivers, H.; Morin, C.M. Validation of the Insomnia Severity Index in Primary Care. J. Am. Board Fam. Med. 2013, 26, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Kaminska, M.; Jobin, V.; Mayer, P.; Amyot, R.; Perraton-Brillon, M.; Bellemare, F. The Epworth Sleepiness Scale: Self-Administration Versus Administration by the Physician, and Validation of a French Version. Can. Respir. J. 2010, 17, e27–e34. [Google Scholar] [CrossRef] [PubMed]
- Kushida, C.A.; Littner, M.R.; Morgenthaler, T.; Alessi, C.A.; Bailey, D.; Coleman, J., Jr.; Friedman, L.; Hirshkowitz, M.; Kapen, S.; Kramer, M.; et al. Practice Parameters for the Indications for Polysomnography and Related Procedures: An Update for 2005. Sleep 2005, 28, 499–521. [Google Scholar] [CrossRef] [PubMed]
- Iber, C.; Ancoli-Israel, S.; Chesson, A.; Quan, S.F. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, 1st ed.; American Academy of Sleep Medicine: Westchester, IL, USA, 2007. [Google Scholar]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed]
- Ferri, R.; Koo, B.B.; Picchietti, D.L.; Fulda, S. Periodic leg movements during sleep: Phenotype, neurophysiology, and clinical significance. Sleep Med. 2017, 31, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Fleetham, J.; Ayas, N.; Bradley, D.; Ferguson, K.; Fitzpatrick, M.; George, C.; Hanly, P.; Hill, F.; Kimoff, J.; Kryger, M.; et al. Canadian Thoracic Society guidelines: Diagnosis and treatment of sleep disordered breathing in adults. Can. Respir. J. 2006, 13, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Edinger, J.D.; Bonnet, M.H.; Bootzin, R.R.; Doghramji, K.; Dorsey, C.M.; Espie, C.A.; Jamieson, A.O.; McCall, W.V.; Morin, C.M.; Stepanski, E.J. Derivation of research diagnostic criteria for insomnia: Report of an American Academy of Sleep Medicine Work Group. Sleep 2004, 27, 1567–1596. [Google Scholar] [CrossRef] [PubMed]
- Haba-Rubio, J.; Marti-Soler, H.; Tobback, N.; Andries, D.; Marques-Vidal, P.; Vollenweider, P.; Preisig, M.; Heinzer, R. Clinical significance of periodic limb movements during sleep: The HypnoLaus study. Sleep Med. 2018, 41, 45–50. [Google Scholar] [CrossRef]
- Allen, R.P.; Picchietti, D.L.; Garcia-Borreguero, D.; Ondo, W.G.; Walters, A.S.; Winkelman, J.W.; Zucconi, M.; Ferri, R.; Trenkwalder, C.; Lee, H.B.; et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: Updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria–History, rationale, description, and significance. Sleep Med. 2014, 15, 860–873. [Google Scholar] [CrossRef] [PubMed]
- Hein, M.; Lanquart, J.P.; Loas, G.; Hubain, P.; Linkowski, P. Insomnia with short sleep duration as risk factor for type 2 diabetes: A systematic review of the literature. Rev. Med. Brux. 2020, 41, 98–104. [Google Scholar] [CrossRef]
- Krell, S.B.; Kapur, V.K. Insomnia complaints in patients evaluated for obstructive sleep apnea. Sleep Breath. 2005, 9, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Hu, N.; Wang, C.; Liao, Y.; Dai, Q.; Cao, S. Smoking and incidence of insomnia: A systematic review and meta-analysis of cohort studies. Public Health 2021, 198, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Luyster, F.S.; Buysse, D.J.; Strollo, P.J., Jr. Comorbid insomnia and obstructive sleep apnea: Challenges for clinical practice and research. J. Clin. Sleep Med. 2010, 6, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Peduzzi, P.; Concato, J.; Feinstein, A.R.; Holford, T.R. Importance of events per independent variable in proportional hazards regression analysis II. Accuracy and precision of regression estimates. J. Clin. Epidemiol. 1995, 48, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Whole Sample (n = 1488) | Subjects without Insomnia (n = 880) | Subjects with Insomnia (n = 608) | p-Value | |
|---|---|---|---|---|
| Sleep latency (min) | 25.2 (13.0–51.5) | 22.5 (12.5–46.0) | 29.0 (14.5–60.0) | <0.001 |
| Sleep efficiency (%) | 77.9 (67.8–85.1) | 78.4 (68.2–85.8) | 76.9 (67.2–84.1) | 0.017 |
| Sleep period time (min) | 452.3 (412.0–485.5) | 455.5 (415.3–486.5) | 446.0 (406.5–481.8) | 0.014 |
| Total sleep time (min) | 381.0 (334.0–426.3) | 383.0 (336.3–428.0) | 375.4 (331.6–424.0) | 0.073 |
| % stage 1 | 8.7 (6.0–12.4) | 8.8 (6.3–12.4) | 8.5 (5.5–12.3) | 0.107 |
| % stage 2 | 53.8 (47.0–59.8) | 54.2 (47.3–60.6) | 53.0 (46.5–59.2) | 0.088 |
| % stage 3 | 2.9 (0.2–9.2) | 2.8 (0.2–8.5) | 3.1 (0.1–10.4) | 0.383 |
| % REM sleep | 15.7 (11.4–20.1) | 15.7 (11.3–20.0) | 15.6 (11.4–20.2) | 0.815 |
| REM latency (min) | 83.0 (59.5–126.7) | 83.6 (60.0–124.3) | 81.5 (58.8–135.0) | 0.644 |
| % WASO | 13.2 (7.6–21.4) | 13.2 (7.7–21.3) | 13.0 (7.4–21.8) | 0.799 |
| Number of awakenings | 32 (22–48) | 33 (22–50) | 32 (21–46) | 0.131 |
| Micro-arousal index | 14 (8–23) | 14 (9–24) | 13 (8–21) | 0.003 |
| Apnoea-hypopnoea index | 14 (8–29) | 15 (8–33) | 13 (7–26) | 0.001 |
| Oxygen desaturation index | 6 (2–15) | 7 (2–17) | 5 (1–14) | 0.002 |
| Total time under 90% of SaO2 (min) | 11.5 (1.0–60.5) | 13.3 (1.5–61.8) | 8.8 (0.5–59.0) | 0.043 |
| PLMS index | 1 (0–10) | 1 (0–10) | 2 (0–9) | 0.897 |
| Median (P25–P75) | Median (P25–P75) | Median (P25–P75) | Wilcoxon test |
| Variables | Categories | % | Subjects without Insomnia | Subjects with Insomnia | p-Value Chi2 | OR (CI 95%) | p-Value |
|---|---|---|---|---|---|---|---|
| Sex | Female (n = 343) male (n = 1145) | 23.0% 77.0% | 19.6% 80.4% | 28.1% 71.9% | <0.001 | 1 0.62 (0.49 to 0.79) | <0.001 |
| Age (years) | <50 (n = 708) ≥50 (n = 780) | 47.6% 52.4% | 45.0% 55.0% | 51.3% 48.7% | 0.016 | 1 0.78 (0.63 to 0.95) | 0.017 |
| BMI (kg/m2) | <25 (n = 289) ≥25 (n = 1199) | 19.4% 80.6% | 17.6% 82.4% | 22.0% 78.0% | 0.034 | 1 0.76 (0.58 to 0.98) | 0.034 |
| Antidepressant therapy | No (n = 1231) Yes (n = 257) | 82.7% 17.3% | 88.5% 11.5% | 74.3% 25.7% | <0.001 | 1 2.66 (2.02 to 3.51) | <0.001 |
| Benzodiazepine receptor agonists | No (n = 1346) Yes (n = 142) | 90.5% 9.5% | 93.8% 6.2% | 85.7% 14.3% | <0.001 | 1 2.50 (1.76 to 3.57) | <0.001 |
| Smoking | No (n = 1177) Yes (n = 311) | 79.1% 20.9% | 79.0% 21.0% | 79.3% 20.7% | 0.889 | 1 0.98 (0.76 to 1.27) | 0.889 |
| Alcohol | No (n = 933) Yes (n = 555) | 62.7% 37.3% | 61.4% 38.6% | 64.6% 35.4% | 0.199 | 1 0.87 (0.70 to 1.08) | 0.199 |
| Cardiometabolic comorbidities | 0 (n = 305) 1–2 (n = 744) ≥3 (n = 439) | 20.5% 50.0% 29.5% | 18.9% 49.3% 31.8% | 22.9% 51.0% 26.1% | 0.031 | 1 0.85 (0.65 to 1.12) 0.68 (0.50 to 0.91) | 0.032 |
| OSAS severity | Mild (n = 772) Moderate (n = 347) Severe (n = 369) | 51.9% 23.3% 24.8% | 48.6% 23.5% 27.9% | 56.6% 23.0% 20.4% | 0.002 | 1 0.84 (0.65 to 1.09) 0.63 (0.49 to 0.82) | 0.002 |
| Sleep movement disorders | No (n = 1178) Moderate to severe PLMs alone (n = 90) RLS alone or combined with PLMs (n = 220) | 79.2% 6.0% 14.8% | 78.6% 6.4% 15.0% | 79.9% 5.6% 14.5% | 0.780 | 1 0.86 (0.56 to 1.34) 0.95 (0.71 to 1.27) | 0.780 |
| Sleep duration (hours) | ≥6 (n = 934) <6 (n = 554) | 62.8% 37.2% | 65.0% 35.0% | 59.5% 40.5% | 0.032 | 1 1.26 (1.02 to 1.56) | 0.032 |
| EDS | No (n = 873) Yes (n = 615) | 58.7% 41.3% | 65.5% 34.5% | 48.9% 51.1% | <0.001 | 1 1.98 (1.61 to 2.45) | <0.001 |
| Major depression status | No (n = 886) Remitted (n = 247) Current (n = 355) | 59.5% 16.6% 23.9% | 71.4% 15.2% 13.4% | 42.4% 18.6% 39.0% | <0.001 | 1 2.05 (1.54 to 2.74) 4.89 (3.75 to 6.37) | <0.001 |
| Insomnia disorder | No (n = 880) Yes (n = 608) | 59.1% 40.9% | |||||
| Median (P25–P75) | Wilcoxon test | ||||||
| Age (years) | 51 (43–59) | 52 (43–60) | 50 (42–58) | 0.023 | |||
| BMI (kg/m2) | 29.0 (25.8–33.1) | 29.0 (26.1–33.2) | 28.7 (25.5–33.0) | 0.143 | |||
| ESS | 9 (6–13) | 9 (5–12) | 11 (7–14) | <0.001 | |||
| ISI | 13 (8–17) | 9 (6–12) | 18 (16–21) | <0.001 | |||
| BDI | 3 (1–7) | 2 (1–5) | 6 (3–11) | <0.001 |
| Variables | Model 1 OR Adjusted (CI 95%) | p-Value | Model 2 OR Adjusted (CI 95%) | p-Value | Model 3 OR Adjusted (CI 95%) | p-Value | Model 4 OR Adjusted (CI 95%) | p-Value |
|---|---|---|---|---|---|---|---|---|
| Major depression | <0.001 | <0.001 | <0.001 | <0.001 | ||||
| No | 1 | 1 | 1 | 1 | ||||
| Remitted | 2.03 (1.52 to 2.72) | 1.73 (1.23 to 2.43) | 1.73 (1.23 to 2.43) | 1.75 (1.24 to 2.47) | ||||
| Current | 4.67 (3.57 to 6.11) | 4.08 (3.03 to 5.47) | 4.09 (3.05 to 5.50) | 3.68 (2.73 to 4.97) |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| OSAS according to the diagnostic criteria of the American Academy of Sleep Medicine | Presence of acute and/or uncontrolled somatic, infectious or inflammatory pathologies |
| Absence of psychiatric disorders other than major depression | Presence of central hypersomnia, parasomnia, predominantly central sleep apnea syndrome or OSAS being treated before hospitalization at the Sleep Laboratory |
| Absence of substance abuse | Presence of craniofacial or thoracic malformations |
| Absence of pregnancy | Presence of brain damage or head trauma |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hein, M.; Wacquier, B.; Conenna, M.; Lanquart, J.-P.; Point, C. Risk of Comorbid Insomnia Disorder Associated with Major Depression in Apneic Patients: A Cross-Sectional Study. Clocks & Sleep 2024, 6, 389-401. https://doi.org/10.3390/clockssleep6030026
Hein M, Wacquier B, Conenna M, Lanquart J-P, Point C. Risk of Comorbid Insomnia Disorder Associated with Major Depression in Apneic Patients: A Cross-Sectional Study. Clocks & Sleep. 2024; 6(3):389-401. https://doi.org/10.3390/clockssleep6030026
Chicago/Turabian StyleHein, Matthieu, Benjamin Wacquier, Matteo Conenna, Jean-Pol Lanquart, and Camille Point. 2024. "Risk of Comorbid Insomnia Disorder Associated with Major Depression in Apneic Patients: A Cross-Sectional Study" Clocks & Sleep 6, no. 3: 389-401. https://doi.org/10.3390/clockssleep6030026
APA StyleHein, M., Wacquier, B., Conenna, M., Lanquart, J.-P., & Point, C. (2024). Risk of Comorbid Insomnia Disorder Associated with Major Depression in Apneic Patients: A Cross-Sectional Study. Clocks & Sleep, 6(3), 389-401. https://doi.org/10.3390/clockssleep6030026