
Determinants of Health Inequalities in Iran and Saudi Arabia: A Systematic Review of the Sleep Literature


Abstract
1. Introduction
2. Results
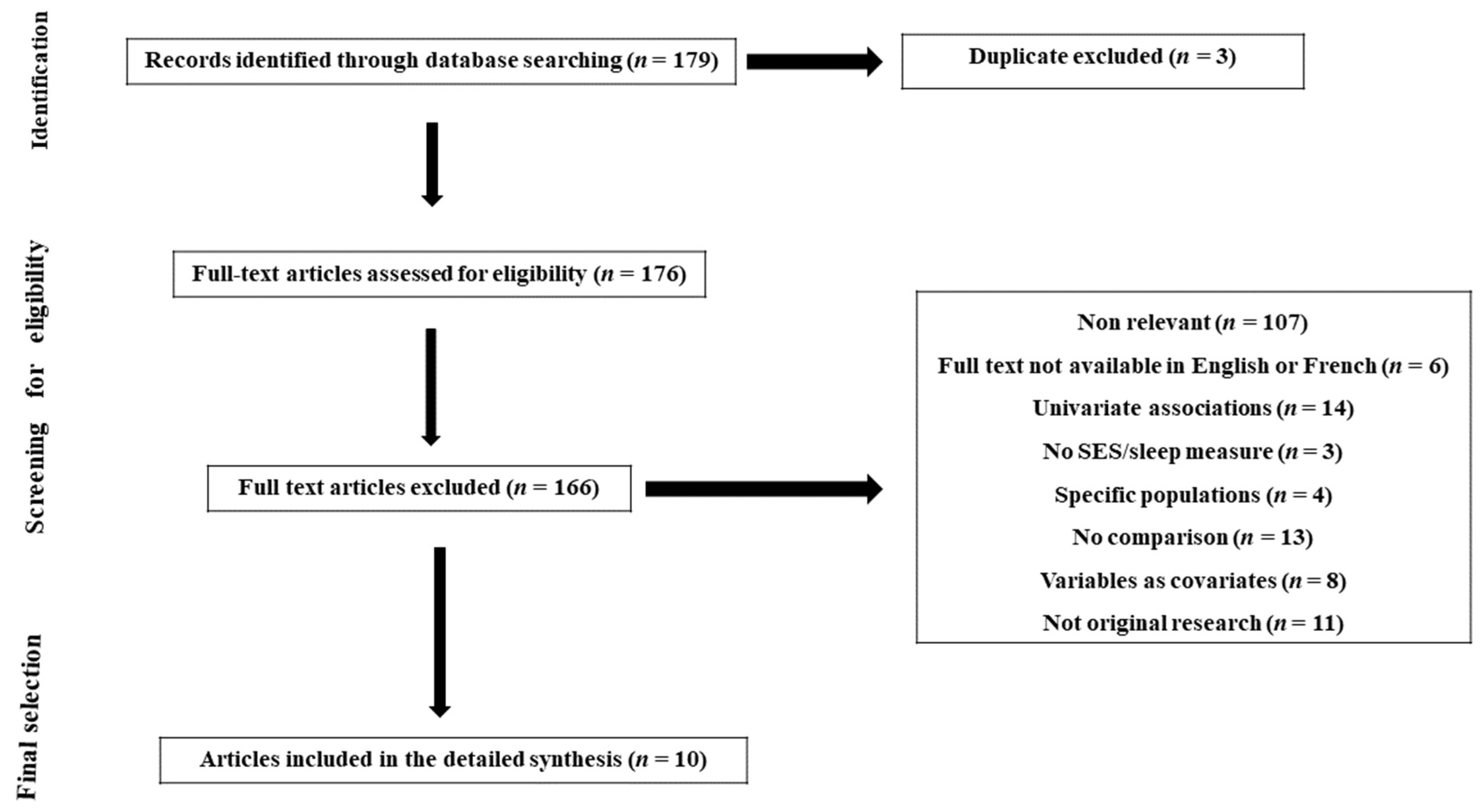
2.1. Characteristics of Studies Selected
2.2. Determinants of Sleep Health Inequalities in Iran
2.3. Determinants of Sleep Health Inequalities in Saudi Arabia
3. Discussion
3.1. Summary of Findings
3.2. Relation with Current Knowledge
3.3. Recommendations for Future Research
3.4. Limitations of This Review
4. Methods
4.1. Literature Search
4.2. Inclusion and Excusion Criteria
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Etindele Sosso, F.A. Measuring Sleep Health Disparities with Polysomnography: A Systematic Review of Preliminary Findings. Clocks Sleep 2022, 4, 80–87. [Google Scholar] [CrossRef]
- Etindele Sosso, F.A.; Holmes, S.D.; Weinstein, A.A. Influence of socioeconomic status on objective sleep measurement: A systematic review and meta-analysis of actigraphy studies. Sleep Health 2021, 7, 417–428. [Google Scholar] [CrossRef]
- Papadopoulos, D.; Sosso, F.E.; Khoury, T.; Surani, S.R. Sleep Disturbances Are Mediators between Socioeconomic Status and Health: A Scoping Review. Int. J. Ment. Health Addict. 2020, 20, 480–504. [Google Scholar] [CrossRef]
- Hale, L.; Troxel, W.; Buysse, D.J. Sleep Health: An Opportunity for Public Health to Address Health Equity. Annu. Rev. Public Health 2020, 41, 81–99. [Google Scholar] [CrossRef]
- Berwick, D.M. The Moral Determinants of Health. JAMA 2020, 324, 225–226. [Google Scholar] [CrossRef]
- Rodriguez, J.M.; Karlamangla, A.S.; Gruenewald, T.L.; Miller-Martinez, D.; Merkin, S.S.; Seeman, T.E. Social stratification and allostatic load: Shapes of health differences in the MIDUS study in the United States. J. Biosoc. Sci. 2019, 51, 627–644. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, D.; Etindele Sosso, F.A. Socioeconomic status and sleep health: A narrative synthesis of three decades of empirical research. J. Clin. Sleep Med. 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Bendaoud, I.; Etindele Sosso, F.A. Socioeconomic Position and Excessive Daytime Sleepiness: A Systematic Review of Social Epidemiological Studies. Clocks Sleep 2022, 4, 240–259. [Google Scholar] [CrossRef]
- Meneton, P.; Hoertel, N.; Wiernik, E.; Lemogne, C.; Ribet, C.; Bonenfant, S.; Ménard, J.; Goldberg, M.; Zins, M. Work environment mediates a large part of social inequalities in the incidence of several common cardiovascular risk factors: Findings from the Gazel cohort. Soc. Sci. Med. 2018, 216, 59–66. [Google Scholar] [CrossRef]
- Petrovic, D.; Haba-Rubio, J.; Carmeli, C.; Vollenweider, P.; Heinzer, R.; Stringhini, S. Social inequalities in sleep-disordered breathing: Evidence from the CoLaus|HypnoLaus study. J. Sleep Res. 2019, 28, e12799. [Google Scholar] [CrossRef]
- Grandner, M.A. (Ed.) Chapter 5—Social-Ecological Model of Sleep Health. In Sleep and Health; Academic Press: Cambridge, MA, USA, 2019; pp. 45–53. [Google Scholar]
- Sosso, F.A.E.; Kreidlmayer, M.; Pearson, D.; Bendaoud, I. Towards A Socioeconomic Model of Sleep Health among the Canadian Population: A Systematic Review of the Relationship between Age, Income, Employment, Education, Social Class, Socioeconomic Status and Sleep Disparities. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1143–1167. [Google Scholar]
- Ribeiro, A.I.; Amaro, J.; Lisi, C.; Fraga, S. Neighborhood Socioeconomic Deprivation and Allostatic Load: A Scoping Review. Int. J. Environ. Res. Public Health 2018, 15, 1092. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Bahammam, A.; Bin Saeed, A.; Al-Faris, E.; Shaikh, S. Sleep duration and its correlates in a sample of Saudi elementary school children. Singap. Med. J. 2006, 47, 875–881. [Google Scholar]
- Al-Hazzaa, H.M.; Alhussain, M.H.; Alhowikan, A.M.; Obeid, O.A. Insufficient Sleep Duration and Its Association with Breakfast Intake, Overweight/Obesity, Socio-Demographics and Selected Lifestyle Behaviors among Saudi School Children. Nat. Sci. Sleep 2019, 11, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Al-Hazzaa, H.M.; Al-Hussain, M.H.; Alhowikan, A.M.; Obeid, O.A. Prevalence of short sleep duration and effect of co-morbid medical conditions—A cross-sectional study in Saudi Arabia. J. Fam. Med. Prim. Care 2019, 8, 3334–3339. [Google Scholar]
- Nasim, M.; Saade, M.; AlBuhairan, F. Sleep deprivation: Prevalence and associated factors among adolescents in Saudi Arabia. Sleep Med. 2019, 53, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Amra, B.; Farajzadegan, Z.; Golshan, M.; Fietze, I.; Penzel, T. Prevalence of sleep apnea-related symptoms in a Persian population. Sleep Breath 2011, 15, 425–429. [Google Scholar] [CrossRef]
- Hassani, S.; Rahnama, N.; Seyedmehdi, S.M.; Yazdanparast, T.; Roozbahani, R.; Attarchi, M.; Naghan, P.A.; Jamaati, H. Association between Occupational Accidents and Sleep Apnea in Hospital Staff. Tanaffos 2015, 14, 201–207. [Google Scholar]
- Heshmat, R.; Qorbani, M.; Ghoreshi, B.; Djalalinia, S.; Tabatabaie, O.R.; Safiri, S.; Noroozi, M.; Motlagh, M.E.; Ahadi, Z.; Asayesh, H.; et al. Association of socioeconomic status with psychiatric problems and violent behaviours in a nationally representative sample of Iranian children and adolescents: The CASPIAN-IV study. BMJ Open 2016, 6, e011615. [Google Scholar] [CrossRef]
- Seyedmehdi, S.M.; Rahnama, N.; Yazdanparast, T.; Jamaati, H.; Attarchi, M.; Naghan, P.A.; Hassani, S. Prevalence of snoring and the risk of sleep apnea in hospital staff. Work 2016, 55, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Foroughi, M.; Malekmohammad, M.; Sharafkhaneh, A.; Emami, H.; Adimi, P.; Khoundabi, B. Prevalence of Obstructive Sleep Apnea in a High-Risk Population Using the Stop-Bang Questionnaire in Tehran, Iran. Tanaffos 2017, 16, 217–224. [Google Scholar]
- Ahmed, A.E.; Al-Jahdali, H.; Fatani, A.; Al-Rouqi, K.; Al-Jahdali, F.; Al-Harbi, A.; Baharoon, S.; Ali, Y.Z.; Khan, M.; Rumayyan, A. The effects of age and gender on the prevalence of insomnia in a sample of the Saudi population. Ethn. Health 2017, 22, 285–294. [Google Scholar] [CrossRef]
- van de Straat, V.; Cheval, B.; Schmidt, R.E.; Sieber, S.; Courvoisier, D.; Kliegel, M.; Burton-Jeangros, C.; Cullati, S.; Bracke, P. Early predictors of impaired sleep: A study on life course socioeconomic conditions and sleeping problems in older adults. Aging Ment. Health 2018, 24, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Sim, C.S.; Sung, J.H.; Lee, J.; Ahn, J.H.; Choe, Y.M.; Park, J. Low Income as a Vulnerable Factor to the Effect of Noise on Insomnia. Psychiatry Investig. 2018, 15, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Matthews, K.A.; Jennings, J.R.; Lee, L. Socioeconomic status in childhood predicts sleep continuity in adult Black and White men. Sleep Health 2018, 4, 49–55. [Google Scholar] [CrossRef]
- Seo, W.H.; Kwon, J.H.; Eun, S.-H.; Kim, G.; Han, K.; Choi, B.M. Effect of socio-economic status on sleep. J. Paediatr. Child Health 2017, 53, 592–597. [Google Scholar] [CrossRef]
- Hawkins, S.S.; Takeuchi, D.T. Social determinants of inadequate sleep in US children and adolescents. Public Health 2016, 138, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Kolla, B.P.; He, J.-P.; Mansukhani, M.; Frye, M.A.; Merikangas, K. Excessive sleepiness and associated symptoms in the U.S. adult population: Prevalence, correlates, and comorbidity. Sleep Health 2020, 6, 79–87. [Google Scholar] [CrossRef]
- Wu, W.; Wang, W.; Dong, Z.; Xie, Y.; Gu, Y.; Zhang, Y.; Li, M.; Tan, X. Sleep Quality and Its Associated Factors among Low-Income Adults in a Rural Area of China: A Population-Based Study. Int. J. Environ. Res. Public Health 2018, 15, 2055. [Google Scholar] [CrossRef]
- Doane, L.D.; Breitenstein, R.S.; Beekman, C.; Clifford, S.; Smith, T.J.; Lemery-Chalfant, K. Early Life Socioeconomic Disparities in Children’s Sleep: The Mediating Role of the Current Home Environment. J. Youth Adolesc. 2018, 48, 56–70. [Google Scholar] [CrossRef] [PubMed]
- Counts, C.J.; Grubin, F.C.; John-Henderson, N.A. Childhood socioeconomic status and risk in early family environments: Predictors of global sleep quality in college students. Sleep Health 2018, 4, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Habte-Gabr, E.; Wallace, R.B.; Colsher, P.L.; Hulbert, J.R.; White, L.R.; Smith, I.M. Sleep patterns in rural elders: Demographic, health, and psychobehavioral correlates. J. Clin. Epidemiol. 1991, 44, 5–13. [Google Scholar] [CrossRef]
- Touitou, Y.; Motohashi, Y.; Reinberg, A.; Bourdeleau, P.; Bogdan, A. Effect of shift work on the night-time secretory patterns of melatonin, prolactin, cortisol and testosterone. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 60, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cheng, Z. Cross-Sectional Studies: Strengths, Weaknesses, and Recommendations. Chest 2020, 158 (Suppl. 1), S65–S71. [Google Scholar] [CrossRef]
- Caruana, E.J.; Roman, M.; Hernández-Sánchez, J.; Solli, P. Longitudinal studies. J. Thorac. Dis. 2015, 7, E537–E540. [Google Scholar]
- Vermeiren, A.P.; Willeboordse, M.; Oosterhoff, M.; Bartelink, N.; Muris, P.; Bosma, H. Socioeconomic multi-domain health inequalities in Dutch primary school children. Eur. J. Public Health 2018, 28, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Wendt, A.; da Silva, I.C.M.; Gonçalves, H.; Assunção, M.C.F.; Menezes, A.M.B.; Wehrmeister, F.C. Sleep parameters measured by accelerometry: Descriptive analyses from the 22-year follow-up of the Pelotas 1993 birth cohort. Sleep Med. 2020, 67, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Etindele-Sosso, F.A. Insomnia, excessive daytime sleepiness, anxiety, depression and socioeconomic status among customer service employees in Canada. Sleep Sci. 2020, 13, 54–64. [Google Scholar] [PubMed]
- Chami, H.A.; Ghandour, B.; Isma’Eel, H.; Nasreddine, L.; Nasrallah, M.; Tamim, H. Sleepless in Beirut: Sleep duration and associated subjective sleep insufficiency, daytime fatigue, and sleep debt in an urban environment. Sleep Breath 2020, 24, 357–367. [Google Scholar] [CrossRef]


{kind=link}
| Study | Study Design | Population | % Women | Age (Mean § SD or Range) | Sample Size | SES Indicators | Sleep Measures | Statistically Significant Findings | Conclusions |
|---|---|---|---|---|---|---|---|---|---|
| Bahammam, 2006 | Cross-sectional | Children recruited from regular governmental elementary schools in all grades (1 to 6) in Riyadh | 49.5 | 6–13 y | 1012 |
| Self-administrated questionnaires addressed to parents to assess:
|
|
|
| Ahmed, 2017 | Cross-sectional | Adults recruited from blood bank donors, preemployment clinics, and KAMC employees | 40.7 | 42.4 ± 15.5 y | 2095 |
| Arabic version of the ICSD-2 instrument to assess insomnia symptoms | The gender-adjusted prevalence of insomnia was higher for females, 88.7% (95% CI = 86.4–90.7%) than for males, 70.4% (95% CI = 67.8–72.9%), p-value = 0.001. The age-adjusted prevalence of insomnia was higher for the elderly, 93.7% (95% CI = 90.6–96.0%) than for the middle aged, 79.8% (95% CI = 77.4–82.1%), or for the young group, 64.2% (95% CI = 59.9–68.4%), p-value = 0.001 | Insomnia is most prevalent among Saudi females and the elderly Saudi population. |
| Al hazza, 2019 | Cross-sectional | Children enrolled in elementary school in Riyadh | 50.2 | 5.9–13.4 y | 1051 |
|
|
|
|
| Al althakafi, 2019 | Cross-sectional | Adults randomly recruited in known social media platforms using Google form in Saudi Arabia | 63 | 21.8 ± 10.7 y | 805 |
| Self-reported sleep duration using online questionnaire |
| No association found between SES and Sleep duration after controlling for cofounders |
| Nasim, 2019 | Cross-sectional | Adolescents recruited in intermediate and secondary schools in Saudi Arabia | 49 | 10–19 y | 12,121 |
|
|
| Adolescents with poorer perceived SES were more likely to report SD |
| Amra, 2011 | Cross-sectional | Randomly selected sample of adults living in urban cities in Ispaphan, Iran | 53.3 | 15–92 y | 3529 | Educational level (junior high school or less, high school, university) | Risk of OSA diagnosed by self-report Berlin questionnaire | Low educational level was associated to high risk of OSA in chi-square test (p < 0.001) | No association between SES and risk of OSA after controlling for cofounders |
| Hassani, 2015 | Cross-sectional | Adults working at a hospital in Iran | 62.8 | 33.51 y (SD = 7.65) | 715 | Educational level (graduate or postgraduate vs. undergraduate) |
|
| In hospital staff, high educational level and high risk of OSA are associated to an increased risk for occupational accidents |
| Heshmat, 2016 | Cross-sectional | Children and adolescents randomly selected in 48 provinces in Iran | 49.2 | 12.47 ± 3.36 y | 13,486 |
| Sleep duration and Insomnia assessed by questionnaire administered to parents and children by trained interviewers |
| A low SES is associated with insomnia in children and adolescents |
| Seyedmehdi, 2016 | Cross-sectional | Staff employees of a hospital in Tehran, Iran | 62.8 | 33.51 ± 7.65 y | 715 | Education (undergraduate vs. graduate or postgraduate) | OSA risk (Berlin questionnaire, high vs. low risk) | The association between the risk of sleep apnea and night sleep less than 4 h (OR = 2.273, CI = 1.142–4.523, p-value = 0.019) and difficulty in staying asleep (OR = 2.515, CI = 1.258–5.031, p value = 0.009) showed to be statistically significant | There was no association between education and OSA risk |
| Foroughi, 2017 | Cross-sectional | A random sample of adults living in Tehran, Iran | 51.6 | 18–97 y | 4021 | Educational level (Illiterate, High school or less, University degree or higher) | OSA assessed by the self-reported Stop-Bang questionnaire which consists of 8 simple but efficient items for OSA screening, and respondents with 3 (or more) out of 8 items are scored positive. | The prevalence of high risk for OSA was significantly higher in less educated participants |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ndiaye, C.; Ayedi, Y.; Etindele Sosso, F.A. Determinants of Health Inequalities in Iran and Saudi Arabia: A Systematic Review of the Sleep Literature. Clocks & Sleep 2023, 5, 141-151. https://doi.org/10.3390/clockssleep5010013
Ndiaye C, Ayedi Y, Etindele Sosso FA. Determinants of Health Inequalities in Iran and Saudi Arabia: A Systematic Review of the Sleep Literature. Clocks & Sleep. 2023; 5(1):141-151. https://doi.org/10.3390/clockssleep5010013
Chicago/Turabian StyleNdiaye, Comsar, Yosr Ayedi, and Faustin Armel Etindele Sosso. 2023. "Determinants of Health Inequalities in Iran and Saudi Arabia: A Systematic Review of the Sleep Literature" Clocks & Sleep 5, no. 1: 141-151. https://doi.org/10.3390/clockssleep5010013
APA StyleNdiaye, C., Ayedi, Y., & Etindele Sosso, F. A. (2023). Determinants of Health Inequalities in Iran and Saudi Arabia: A Systematic Review of the Sleep Literature. Clocks & Sleep, 5(1), 141-151. https://doi.org/10.3390/clockssleep5010013