A Pilot Study of 24-h Motor Activity Patterns in Multiple Sclerosis: Pre-Planned Follow-Up at 2 Years

 ,
, 
 ,
,  and
and
Abstract
:1. Introduction
2. Results
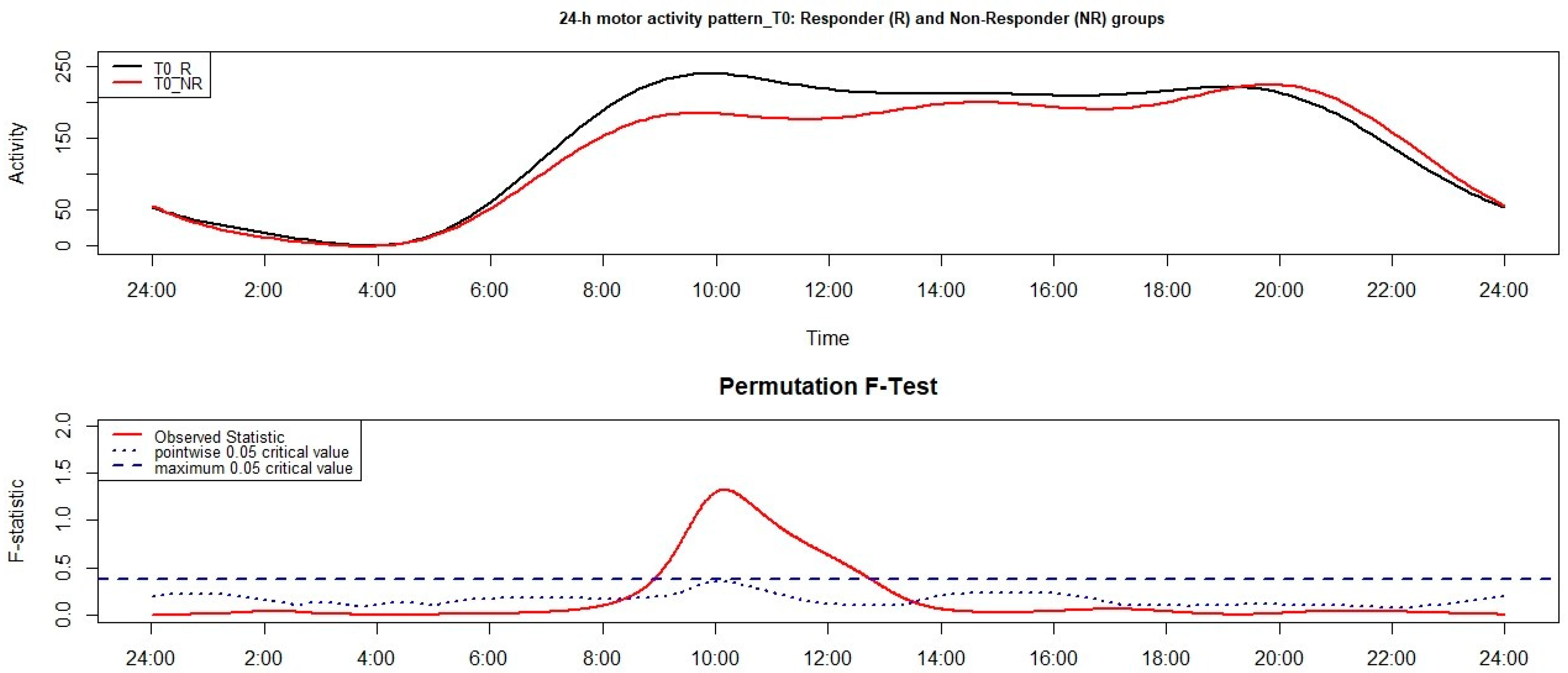
2.1. Between-Subjects Comparison at T0 between the Non-Responder (NR) Group and the Responder (R) Group
2.1.1. Actigraphic Parameters
2.1.2. 24-h Motor Activity Pattern
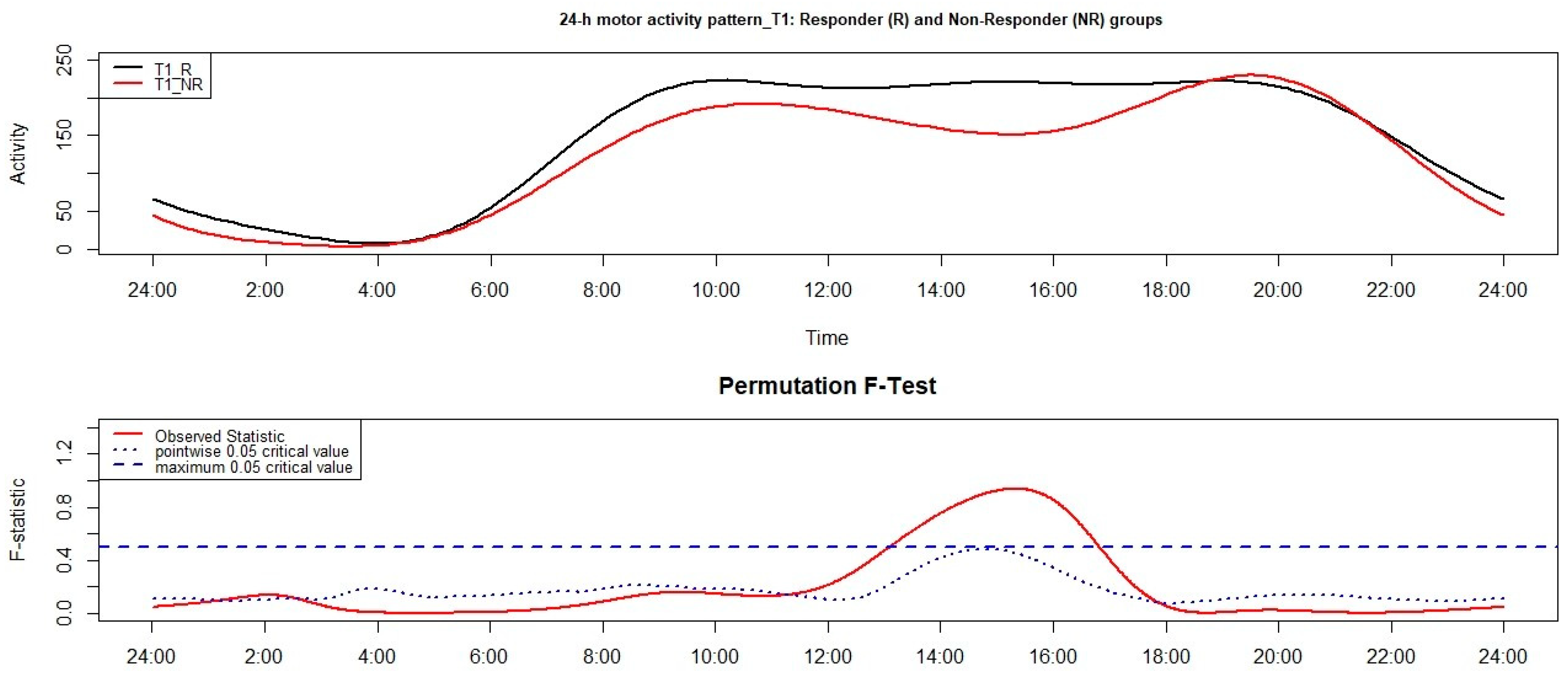
2.2. Between-Subjects Comparison at T1 between the NR Group and the R Group
2.2.1. Actigraphic Parameters
2.2.2. 24-h Motor Activity Pattern
2.3. R Group: Within-Subject Comparison between T0 and T1
2.3.1. Actigraphic Parameters
2.3.2. 24-h Motor Activity Pattern
2.4. NR Group: Within-Subject Comparison between T0 and T1
2.4.1. Actigraphic Parameters
2.4.2. 24-h Motor Activity Pattern
3. Discussion
4. Methods
4.1. Participants
4.2. Actigraphy
4.3. Actigraphic Sleep/Wake Measures
4.4. 24-h Motor Activity Pattern
4.5. Procedure
4.6. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [Green Version]
- The Multiple Sclerosis International Federation. Atlas of MS, 3rd ed.; The Multiple Sclerosis International Federation (MSIF): London, UK, 2020; Available online: https://www.atlasofms.org/ (accessed on 7 February 2021).
- Lavtar, P.; Rudolf, G.; Maver, A.; Hodzic, A.; Cizmarevic, N.S.; Živković, M.; Jazbec, S.S.; Ketis, Z.K.; Kapovic, M.; Dinčić, E.; et al. Association of circadian rhythm genes ARNTL/BMAL1 and CLOCK with multiple sclerosis. PLoS ONE 2018, 13, e0190601. [Google Scholar] [CrossRef] [PubMed]
- Gasperoni, F.; Turini, P.; Agostinelli, E. A novel comprehensive paradigm for the etiopathogenesis of multiple sclerosis: Therapeutic approaches and future perspectives on its treatment. Amino Acids 2019, 51, 745–759. [Google Scholar] [CrossRef]
- Tonetti, L.; Camilli, F.; Giovagnoli, S.; Natale, V.; Lugaresi, A. Circadian Activity Rhythm in Early Relapsing–Remitting Multiple Sclerosis. J. Clin. Med. 2019, 8, 2216. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Xian, H.; Licis, A.; Deych, E.; Ding, J.; McLeland, J.; Toedebusch, C.; Li, T.; Duntley, S.; Shannon, W. Measuring the impact of apnea and obesity on circadian activity patterns using functional linear modeling of actigraphy data. J. Circadian Rhythm. 2011, 9, 11. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, L.; Conca, A.; Giupponi, G.; Filardi, M.; Natale, V. Circadian activity rhythm in adult attention-deficit hyperactivity disorder. J. Psychiatr. Res. 2018, 103, 1–4. [Google Scholar] [CrossRef]
- Brown, J.W.L.; Coles, A.; Horakova, D.; Havrdova, E.; Izquierdo, G.; Prat, A.; Girard, M.; Duquette, P.; Trojano, M.; Lugaresi, A.; et al. Association of Initial Disease-Modifying Therapy With Later Conversion to Secondary Progressive Multiple Sclerosis. JAMA 2019, 321, 175–187. [Google Scholar] [CrossRef] [Green Version]
- Harding, K.; Williams, O.; Willis, M.; Hrastelj, J.; Rimmer, A.; Joseph, F.; Tomassini, V.; Wardle, M.; Pickersgill, T.; Robertson, N.; et al. Clinical Outcomes of Escalation vs Early Intensive Disease-Modifying Therapy in Patients With Multiple Sclerosis. JAMA Neurol. Am. Med. Assoc. 2019, 76, 536–541. [Google Scholar] [CrossRef]
- Río, J.; Comabella, M.; Montalban, X. Predicting responders to therapies for multiple sclerosis. Nat. Rev. Neurol. 2009, 5, 553–560. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Blikman, L.J.; Huisstede, B.M.; Kooijmans, H.; Stam, H.J.; Bussmann, J.B.; van Meeteren, J. Effectiveness of energy conservation treatment in reducing fatigue in multiple sclerosis: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2013, 94, 1360–1376. [Google Scholar] [CrossRef]
- Motl, R.W.; Dlugonski, D.; Pilutti, L.; Sandroff, B.; McAuley, E. Premorbid physical activity predicts disability progression in relapsing-remitting multiple sclerosis. J. Neurol. Sci. 2012, 323, 123–127. [Google Scholar] [CrossRef]
- Waterhouse, J.; Drust, B.; Weinert, D.; Edwards, B.; Gregson, W.; Atkinson, G.; Kao, S.; Aizawa, S.; Reilly, T. The Circadian Rhythm of Core Temperature: Origin and some Implications for Exercise Performance. Chronobiol. Int. 2005, 22, 207–225. [Google Scholar] [CrossRef]
- Christogianni, A.; Bibb, R.; Davis, S.L.; Jay, O.; Barnett, M.; Evangelou, N.; Filingeri, D. Temperature sensitivity in multiple sclerosis: An overview of its impact on sensory and cognitive symptoms. Temperature 2018, 5, 208–223. [Google Scholar] [CrossRef] [PubMed]
- Filippi, M.; Rocca, M.A.; Ciccarelli, O.; De Stefano, N.; Evangelou, N.; Kappos, L.; Rovira, A.; Sastre-Garriga, J.; Tintorè, M.; Frederiksen, J.L.; et al. MRI criteria for the diagnosis of multiple sclerosis: MAGNIMS consensus guidelines.-PubMed-NCBI. Lancet Neurol. 2016, 15, 292–303. [Google Scholar] [CrossRef] [Green Version]
- Rovira, A.; Wattjes, M.P.; Tintoré, M.; Tur, C.; Yousry, T.A.; Sormani, M.P.; De Stefano, N.; Filippi, M.; Auger, C.; Rocca, M.A.; et al. Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis-clinical implementation in the diagnostic process. Nat. Rev. Neurol. 2015, 11, 471–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wattjes, M.P.; Rovira, A.; Miller, D.; Yousry, T.A.; Sormani, M.P.; de Stefano, M.P.; Tintoré, M.; Auger, C.; Tur, C.; Filippi, M.; et al. Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis--establishing disease prognosis and monitoring patients. Nat. Rev. Neurol. 2015, 11, 597–606. [Google Scholar]
- Gasperini, C.; Prosperini, L.; Tintoré, M.; Sormani, M.P.; Filippi, M.; Rio, J.; Palace, J.; Rocca, M.A.; Ciccarelli, O.; Barkhof, F.; et al. Unraveling treatment response in multiple sclerosis: A clinical and MRI challenge. Neurology 2019, 92, 180–192. [Google Scholar] [CrossRef]
- Cole, R.J.; Kripke, D.F. Progress in automatic sleep/wake scoring by wrist actigraph. Sleep Res. 1988, 17, 331. [Google Scholar]
- Cole, R.J.; Kripke, D.F.; Gruen, W.; Mullaney, D.J.; Gillin, J.C. Automatic sleep/wake identification from wrist activity. Sleep 1992, 15, 461–469. [Google Scholar] [CrossRef]
- Natale, V.; Leger, D.; Bayon, V.; Erbacci, A.; Tonetti, L.; Fabbri, M.; Martoni, M. The Consensus Sleep Diary: Quantitative Criteria for Primary Insomnia Diagnosis. Psychosom. Med. 2015, 77, 413–418. [Google Scholar] [CrossRef]
- Carney, C.E.; Buysse, D.; Ancoli-Israel, S.; Edinger, J.D.; Krystal, A.D.; Lichstein, K.L.; Morin, C.M. The consensus sleep diary: Standardizing prospective sleep self-monitoring. Sleep 2012, 35, 287–302. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| NR | R | Statistics | |||
|---|---|---|---|---|---|
| t(16) | pa | Cohen’s d | |||
| Sleep | |||||
| BT | 23:32 ± 0:31 | 23:13 ± 1:07 | 0.55 | 0.59 | 0.31 |
| GUT | 07:26 ± 0:58 | 06:47 ± 0:52 | 1.31 | 0.21 | 0.73 |
| TIB | 470.1 ± 64.36 | 455.1 ± 60.06 | 0.43 | 0.67 | 0.25 |
| MS | 03:31 ± 0:34 | 02:59 ± 0:52 | 1.15 | 0.27 | 0.65 |
| SMA | 14.85 ± 6.95 | 12.44 ± 3.77 | 0.94 | 0.36 | 0.53 |
| SOL | 10.75 ± 4.97 | 13.3 ± 7.22 | −0.66 | 0.52 | 0.37 |
| TST | 416.1 ± 31.60 | 424.16 ± 57.27 | −0.27 | 0.79 | 0.15 |
| WASO | 42.25 ± 39.70 | 18.57 ± 9.98 | 2.15 | 0.05 | 1.22 |
| SE | 89.32 ± 7.66 | 93.16 ± 2.87 | −1.61 | 0.13 | 0.91 |
| AWK | 12.05 ± 8.31 | 9.44 ± 3.93 | 0.91 | 0.38 | 0.52 |
| AWK > 5 | 3.9 ± 3.39 | 1.91 ± 0.76 | 2.16 | 0.05 | 0.52 |
| Wake | |||||
| DMA | 191.93 ± 15.46 | 215.04 ± 23.66 | −1.82 | 0.09 | 1.03 |
| DTST | 34.06 ± 37.19 | 34.45 ± 40.98 | −0.02 | 0.99 | 0.01 |
| NAP | 4 ± 4.04 | 4.07 ± 3.38 | −0.04 | 0.97 | 0.02 |
| NAPD | 19 ± 15.27 | 18.64 ± 21.29 | 0.03 | 0.98 | 0.02 |
| NR | R | Statistics | |||
|---|---|---|---|---|---|
| t(16) | pa | Cohen’s d | |||
| Sleep | |||||
| BT | 23:04 ± 0:39 | 23:34 ± 1:28 | −0.65 | 0.52 | 0.37 |
| GUT | 07:19 ± 0:40 | 06:58 ± 1:19 | 0.51 | 0.61 | 0.29 |
| TIB | 500.35 ± 54.76 | 444.04 ± 51.38 | 1.91 | 0.07 | 1.08 |
| MS | 03:08 ± 0:24 | 03:16 ± 1:19 | −0.17 | 0.87 | 0.10 |
| SMA | 16.24 ± 5.70 | 12.86 ± 3.69 | 1.44 | 0.17 | 0.82 |
| SOL | 19.35 ± 11.50 | 14.78 ± 6.73 | 1.03 | 0.32 | 0.58 |
| TST | 434.7 ± 31.55 | 409.68 ± 52.55 | 0.90 | 0.38 | 0.51 |
| WASO | 45.95 ± 31.67 | 19.69 ± 9.96 | 2.83 | 0.01 | 1.60 |
| SE | 90.83 ± 6.16 | 95.34 ± 2.44 | −2.30 | 0.03 | 1.31 |
| AWK | 12.1 ± 5.34 | 9.48 ± 3.28 | 1.23 | 0.24 | 0.70 |
| AWK > 5 | 4.6 ± 2.48 | 2.33 ± 0.98 | 2.88 | 0.01 | 1.63 |
| Wake | |||||
| DMA | 184.59 ± 12.55 | 211.52 ± 23.93 | −2.14 | 0.05 | 1.21 |
| DTST | 40.21 ± 34.96 | 28.40 ± 27.75 | 0.71 | 0.49 | 0.40 |
| NAP | 3.46 ± 3.15 | 3.83 ± 2.63 | −0.24 | 0.81 | 0.14 |
| NAPD | 22.79 ± 16.67 | 13.05 ± 11.61 | 1.35 | 0.20 | 0.77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tonetti, L.; Camilli, F.; Giovagnoli, S.; Natale, V.; Lugaresi, A. A Pilot Study of 24-h Motor Activity Patterns in Multiple Sclerosis: Pre-Planned Follow-Up at 2 Years. Clocks & Sleep 2021, 3, 366-376. https://doi.org/10.3390/clockssleep3030023
Tonetti L, Camilli F, Giovagnoli S, Natale V, Lugaresi A. A Pilot Study of 24-h Motor Activity Patterns in Multiple Sclerosis: Pre-Planned Follow-Up at 2 Years. Clocks & Sleep. 2021; 3(3):366-376. https://doi.org/10.3390/clockssleep3030023
Chicago/Turabian StyleTonetti, Lorenzo, Federico Camilli, Sara Giovagnoli, Vincenzo Natale, and Alessandra Lugaresi. 2021. "A Pilot Study of 24-h Motor Activity Patterns in Multiple Sclerosis: Pre-Planned Follow-Up at 2 Years" Clocks & Sleep 3, no. 3: 366-376. https://doi.org/10.3390/clockssleep3030023
APA StyleTonetti, L., Camilli, F., Giovagnoli, S., Natale, V., & Lugaresi, A. (2021). A Pilot Study of 24-h Motor Activity Patterns in Multiple Sclerosis: Pre-Planned Follow-Up at 2 Years. Clocks & Sleep, 3(3), 366-376. https://doi.org/10.3390/clockssleep3030023