
Bayesian Mediation Analysis with an Application to Explore Racial Disparities in the Diagnostic Age of Breast Cancer


Abstract
1. Background
2. Data Set and Variable Description
3. Methods
3.1. Method 1: Functions of Estimated Coefficients
3.2. Method 2: Mediation Effects as the Product of Partial Differences
3.3. Method 3: Re-Sampling Method
3.4. Prior Distribution and Computational Method
4. Results
5. Conclusions and Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- F.Alwin, D.; Hauser, R.M. The Decomposition of Effects in Path Analysis. Am. Sociol. Rev. 1975, 40, 37–47. [Google Scholar] [CrossRef]
- Mackinnon, D.P.; Dwyer, J.H. Estimating mediated effects in prevention studies. Am. Sociol. Rev. 1993, 17, 144–158. [Google Scholar] [CrossRef]
- M.Robins, J.; Greenland, S. Identifiability and Exchangeability for Direct and Indirect Effects. Epidemiology 1992, 3, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Pearl, J. Direct and indirect effects. In Proceedings of the Seventeenth Conference on Uncertainty in Artificial Intelligence, Barcelona, Spain, 14–17 July 2001; pp. 411–420. [Google Scholar]
- Albert, J.M. Mediation analysis via potential outcomes models. Stat. Med. 2008, 27, 1282–1304. [Google Scholar] [CrossRef] [PubMed]
- Have, T.R.T.; Joffe, M.M.; Lynch, K.G.; Brown, G.K. Causal mediation analyses with rank preserving models. Biometrics 2007, 63, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Fan, Y.; Wu, X. General Multiple Mediation Analysis With an Application to Explore Racial Disparities in Breast Cancer Survival. J. Biom. Biostat. 2014, 5, 189. [Google Scholar]
- Vanderweele, T.J.; Vansteelandt, S. Conceptual issues concerning mediation, interventions and composition. Stat. Interface 2009, 2, 457–468. [Google Scholar] [CrossRef]
- Vansteelandt, S.; Daniel, R.M. Interventional effects for mediation analysis with multiple mediators. Epidemiology 2017, 28, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Wu, X.; Li, B.; Scribner, R.A. Multiple mediation analysis with survival outcomes: With an application to explore racial disparity in breast cancer survival. Stat. Med. 2019, 38, 398–412. [Google Scholar] [CrossRef]
- Yuan, Y.; MacKinnon, D.P. Bayesian mediation analysis. Psychol. Methods 2009, 14, 301–322. [Google Scholar] [CrossRef]
- Miočević, M.; Gonzalez, O.; Valente, M.J.; MacKinnon, D.P. A Tutorial in Bayesian Potential Outcomes Mediation Analysis. Struct. Equ. Model. Multidiscip. J. 2017, 25, 121–136. [Google Scholar] [CrossRef] [PubMed]
- Miočević, M.; MacKinnon, D.P.; Levy, R. Power in Bayesian Mediation Analysis for Small Sample Research. Struct. Equ. Model. Multidiscip. J. 2017, 24, 666–683. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kaplan, D. Bayesian Causal Mediation Analysis for Group Randomized Designs with Homogeneous and Heterogeneous Effects: Simulation and Case Study. Multivar. Behav. Res. 2015, 50, 316–333. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Daniels, M.J.; Hogan, J.W.; Choirat, C.; Zigler, C.M. Bayesian methods for multiple mediators: Relating principal stratification and causal mediation in the analysis of power plant emission controls. Ann. Appl. Stat. 2019, 13, 1927–1956. [Google Scholar] [CrossRef] [PubMed]
- Gao, T.; Albert, J.M. Bayesian causal mediation analysis with multiple ordered mediators. Stat. Model. 2018, 19, 634–652. [Google Scholar] [CrossRef] [PubMed]
- Aung, M.T.; Song, Y.; Ferguson, K.K.; Cantonwine, D.E.; Zeng, L.; McElrath, T.F.; Pennathur, S.; Meeker, J.D.; Mukherjee, B. Application of a novel analytical pipeline for high-dimensional multivariate mediation analysis of environmental data. Nat. Commun. 2020, 11, 5624. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Cao, W.; Li, B. Bayesian mediation analysis methods to explore racial/ethnic disparities in anxiety among cancer survivors. Behaviormetrika 2023, 50, 361–383. [Google Scholar] [CrossRef]
- Rosenberg, J.; Chia, Y.L.; Plevritis, S. The effect of age, race, tumor size, tumor grade, and disease stage on invasive ductal breast cancer survival in the U.S. SEER database. Breast Cancer Res. Treat. 2015, 89, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Sassi, F.; Luft, H.S.; Guadagnoli, E. Reducing racial/ethnic disparities in female breast cancer: Screening rates and stage at diagnosis. Am. J. Public Health 2006, 96, 2165–2172. [Google Scholar] [CrossRef] [PubMed]
- Gerend, M.A.; Pai, M. Social determinants of black-white disparities in breast cancer mortality: A review. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2913–2923. [Google Scholar] [CrossRef]
- Bain, R.P.; Greenberg, R.S.; Whitaker, J. Racial differences in survival of women with breast cancer. J. Chronic Dis. 1986, 39, 631–642. [Google Scholar] [CrossRef] [PubMed]
- Warner, E.T.; Tamimi, R.M.; Hughes, M.E.; Ottesen, R.A.; Wong, Y.-N.; Edge, S.B.; Theriault, R.L.; Blayney, D.W.; Niland, J.C.; Winer, E.P.; et al. Racial and ethnic differences in breast cancer survival: Mediating effect of tumor characteristics and sociodemographic and treatment factors. J. Clin. Oncol. 2015, 33, 2254–2261. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Ma, H.; Malone, K.E.; Norman, S.A.; Sullivan-Halley, J.; Strom, B.L.; Marchbanks, P.A.; Spirtas, R.; Burkman, R.T.; Deapen, D.; et al. Obesity and Survival among Black Women and White Women 35 to 64 Years of Age at Diagnosis with Invasive Breast Cancer. J. Clin. Oncol. 2011, 29, 3358–3365. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Scribner, R.A.; Leonardi, C.; Zhang, L.; Park, C.; Chen, L.; Simonsen, N.R. Exploring racial disparity in obesity: A mediation analysis considering geo-coded environmental factors. Spat.-Spatio-Temporal Epidemiol. 2017, 21, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, U.; Arvidsson, D.; Gebel, K.; Ohlsson, H.; Sundquist, K. Walkability parameters, active transportation and objective physical activity: Moderating and mediating effects of motor vehicle ownership in a cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 123. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Cust, A.E. Physical activity and breast cancer risk: Impact of timing, type and dose of activity and population subgroup effects. Br. J. Sports Med. 2008, 42, 636–647. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, E.M.; Al-Homaidh, A. Physical activity and survival after breast cancer diagnosis: Meta-analysis of published studies. Med. Oncol. 2011, 28, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.; Hayes, S.C.; Newman, B. Level of physical activity and characteristics associated with change following breast cancer diagnosis and treatment. Psycho-Oncol. 2009, 18, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Gelman, A. Prior distributions for variance parameters in hierarchical models. J. Am. Stat. Assoc. 2005, 100, 1278–1281. [Google Scholar]
- Congdon, P.D. Bayesian analysis options in R, and coding for BUGS, JAGS, and Stan. In Bayesian Hierarchical Models; Chapman and Hall/CRC: Boca Raton, FL, USA, 2019; pp. 45–57. ISBN 9780429113352. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Potential Mediators | Black | White | p-Value 1 | p-Value 2 |
|---|---|---|---|---|
| Categorical Variables | Frequency (%) | Frequency (%) | ||
| Insurance: | <0.0001 | <0.0001 | ||
| no insurance | 3.74% | 1.77% | ||
| public insuance | 34.63% | 14.00% | ||
| private insurance | 61.64% | 84.23% | ||
| Marital status: | <0.0001 | <0.0001 | ||
| single | 34.63% | 11.97% | ||
| married | 35.49% | 59.15% | ||
| separated or divorced | 14.51% | 11.97% | ||
| widowed | 15.37% | 16.91% | ||
| Comorbidity: | <0.0001 | <0.0001 | ||
| no/mild | 33.91% | 40.53% | ||
| moderate | 59.20% | 56.87% | ||
| severe | 6.90% | 2.60% | ||
| Stage: | <0.0001 | 0.0010 | ||
| 1. localized | 53.74% | 61.56% | ||
| 2. regional by direct extension only | 1.58% | 1.84% | ||
| 3. ipsilateral regional lymph nodes only | 32.18% | 26.54% | ||
| 4. regional by both 2 and 3 | 4.89% | 3.10% | ||
| 5. distant sites | 7.61% | 6.97% | ||
| Body mass index: | 0.0030 | 0.0700 | ||
| underweight | 1.72% | 2.15% | ||
| healthy weight | 14.80% | 29.58% | ||
| overweight | 27.44% | 30.59% | ||
| obese | 56.03% | 37.68% | ||
| Continuous Variables | Mean (SD) | Mean (SD) | p-Value 1 | p-Value 2 |
| Street density | 15.29 (13.34) | 9.87 (10.73) | 0.3410 | <0.0001 |
| Intersection density | 94.47 (105.26) | 51.90 (73.45) | 0.9180 | <0.0001 |
| Connected node ratio | 0.71 (0.15) | 0.63 (0.13) | 0.0004 | <0.0001 |
| Language isolation | 0.58 (0.15) | 0.48 (0.17) | 0.0270 | <0.0001 |
| Percent of persons under age 18 | 25.58 (5.50) | 23.99 (5.01) | 0.1000 | <0.0001 |
| Poverty index | 25.29 (12.79) | 15.04 (9.19) | <0.0001 | <0.0001 |
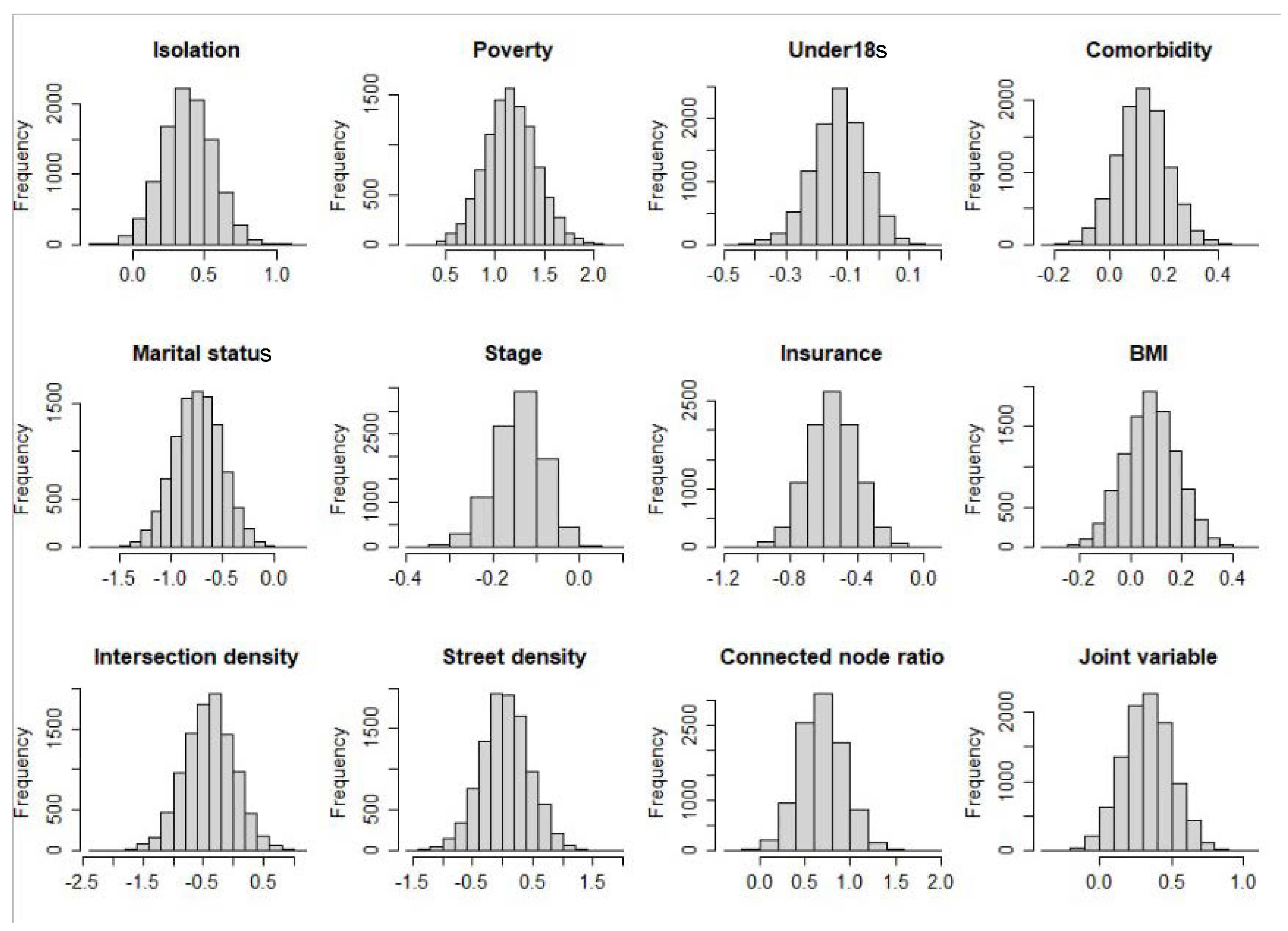
| Mediators | Effect (95% Credible Sets) | Relative Effect (%) |
|---|---|---|
| Insurance | −0.55 (−0.85, −0.26) | 12.90 (6.05, 21.26) |
| Marital status | −0.74 (−1.20, −0.28) | 17.17 (6.99, 28.22) |
| Comorbidity | 0.12 (−0.05, 0.30) | −2.85 (−7.53, 1.23) |
| Stage | −0.14 (−0.26, −0.03) | 3.27 (0.78, 6.33) |
| BMI | 0.08 (−0.13, 0.28) | −1.81 (−7, 3.1) |
| Isolation | 0.39 (0.04, 0.73) | −9.03 (−18.33, −1.11) |
| Poverty index | 1.16 (0.65, 1.68) | −27.18 (−43.5, −14.53) |
| Under 18s | −0.13 (−0.30, 0.03) | 3.07 (−0.63, 7.42) |
| J1 (walkability) | 0.33 (0, 0.6642) | −7.79 (−16.28, −0.08) |
| Street density | 0.04 (−0.76, 0.83) | −0.79 (−19.39, 18.45) |
| Intersection density | −0.40 (−1.21, 0.41) | 9.02 (−10.21, 29.13) |
| Connected node ratio | 0.68 (0.21, 1.16) | −16.02 (−28.85, −5.07) |
| Direct effect | −4.88 (−6.12, −3.65) | 112.24 (94.02, 133.04) |
| Total effect | −4.37 (−5.47, −3.26) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, W.; Hagan, J.; Yu, Q. Bayesian Mediation Analysis with an Application to Explore Racial Disparities in the Diagnostic Age of Breast Cancer. Stats 2024, 7, 361-372. https://doi.org/10.3390/stats7020022
Cao W, Hagan J, Yu Q. Bayesian Mediation Analysis with an Application to Explore Racial Disparities in the Diagnostic Age of Breast Cancer. Stats. 2024; 7(2):361-372. https://doi.org/10.3390/stats7020022
Chicago/Turabian StyleCao, Wentao, Joseph Hagan, and Qingzhao Yu. 2024. "Bayesian Mediation Analysis with an Application to Explore Racial Disparities in the Diagnostic Age of Breast Cancer" Stats 7, no. 2: 361-372. https://doi.org/10.3390/stats7020022
APA StyleCao, W., Hagan, J., & Yu, Q. (2024). Bayesian Mediation Analysis with an Application to Explore Racial Disparities in the Diagnostic Age of Breast Cancer. Stats, 7(2), 361-372. https://doi.org/10.3390/stats7020022