
Clinical Features and PTCH1 Expression in Gorlin–Goltz Syndrome: A Case Report †

 , and
, and
Abstract
1. Introduction and Clinical Significance
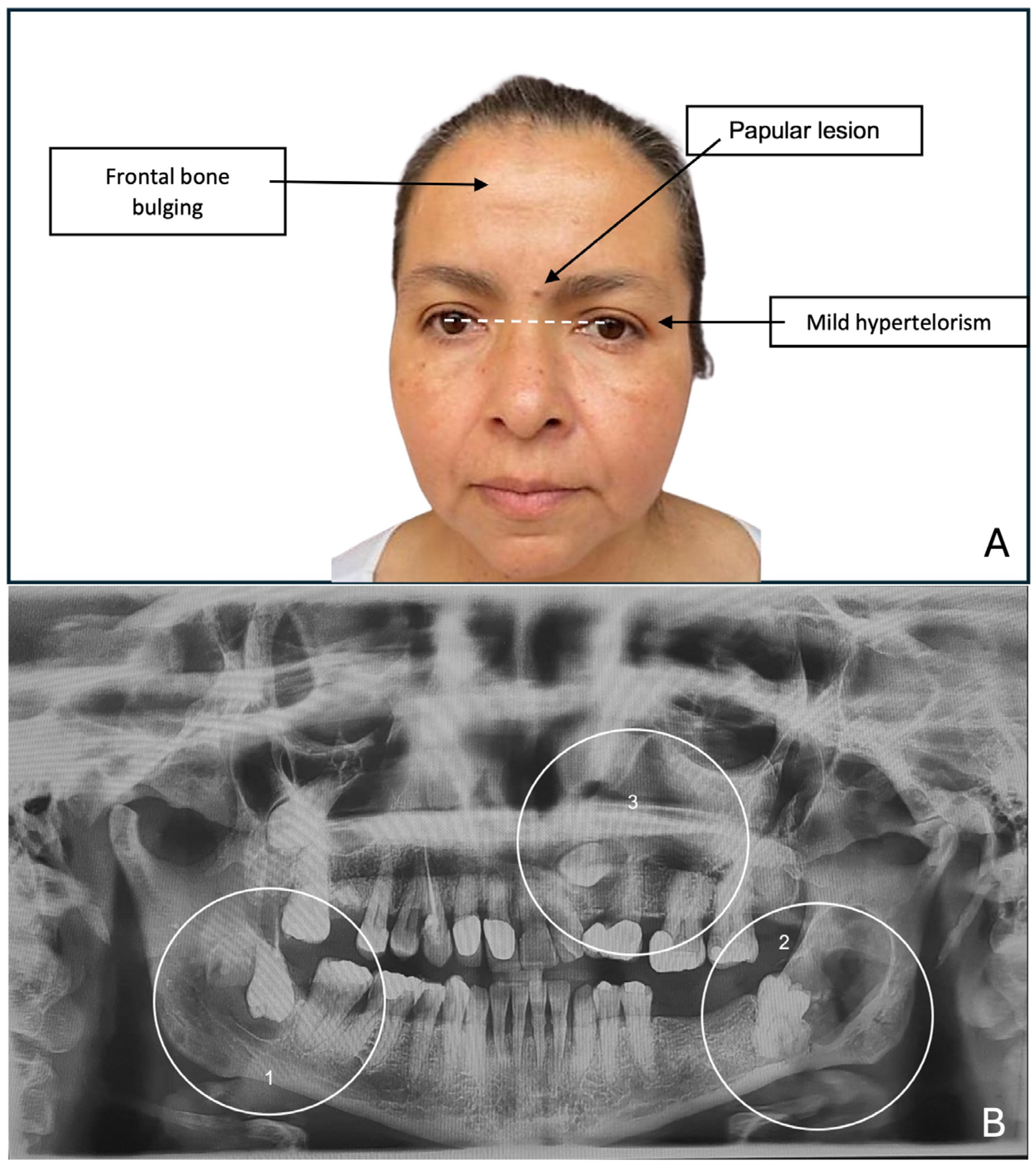
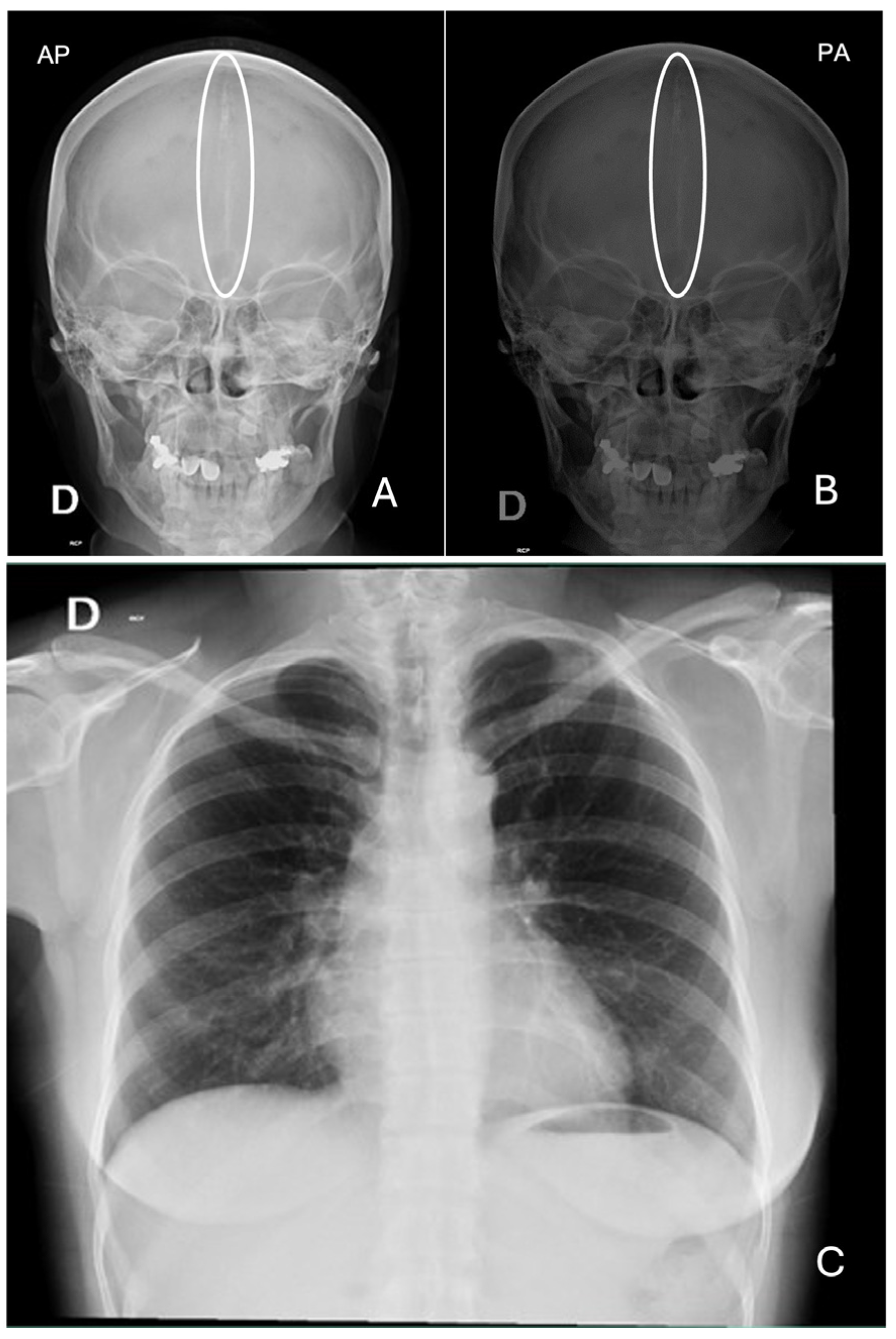
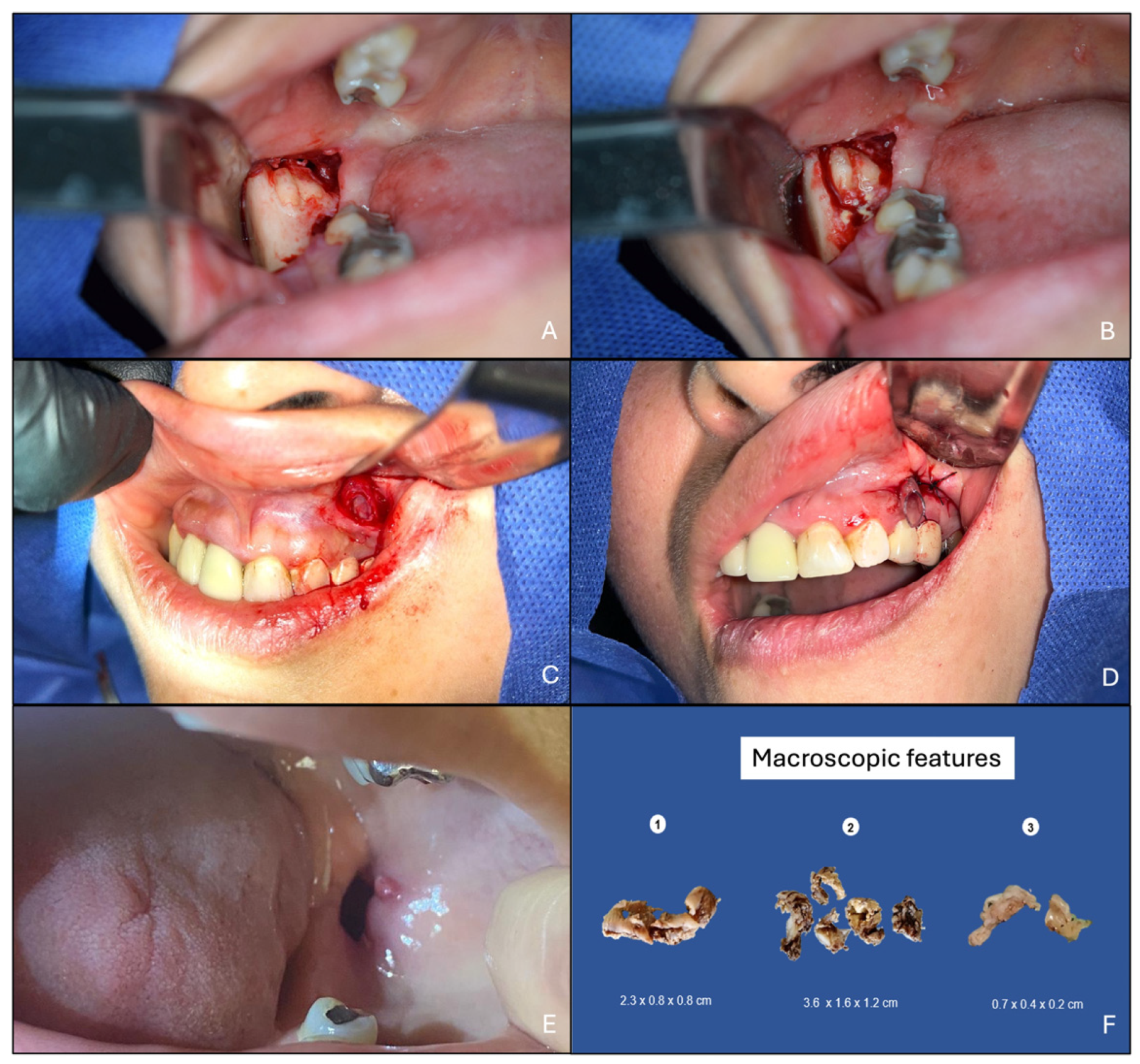
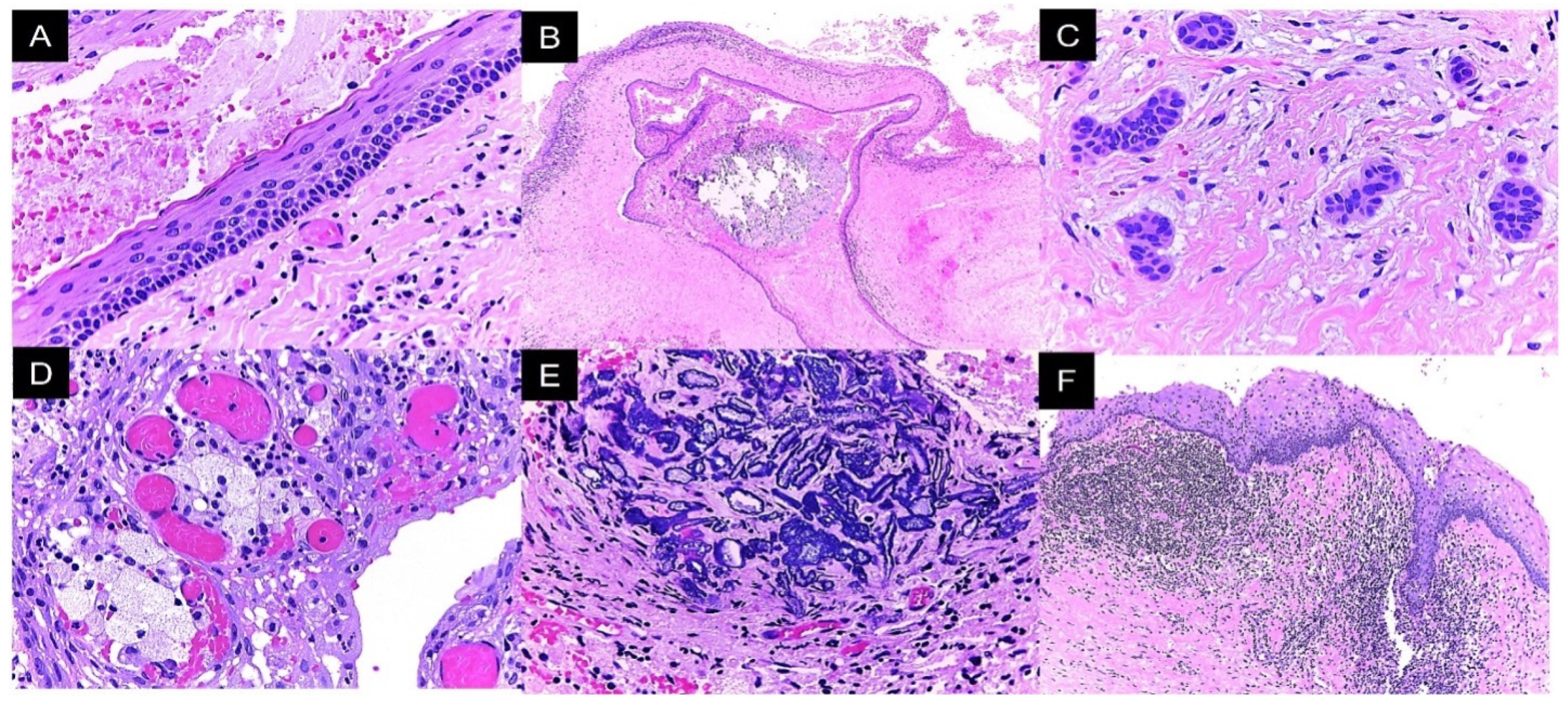
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GGS | Gorlin–Goltz Syndrome |
| SHH | Sonic HedgeHog |
| PTCH1 | Patched 1 |
| OKC | Odontogenic keratocyst |
| BCC | Basal cell carcinoma |
References
- Speight, P.; Devilliers, P.; Li, T.J.; Odell, E.W.; Wright, J.M. Odontogenic keratocyst. In WHO Classification of Head and Neck Tumours, 4th ed.; El-Naggar, A.K., Chan, J.K.C., Grandis, J.R., Takata, T., Slootweg, P.J., Eds.; IARC: Lyon, France, 2017; pp. 235–236. [Google Scholar]
- Neville, B.; Allen, C.; Damm, D.; Chi, A. Oral and Maxillofacial Pathology, 5th ed.; Elsevier: Toronto, ON, Canada, 2023. [Google Scholar]
- Stojanov, I.J.; Schaefer, I.M.; Menon, R.S.; Wasman, J.; Gokozan, H.N.; Garcia, E.P.; Baur, D.A.; Woo, S.B.; Sholl, L.M. Biallelic PTCH1 Inactivation Is a Dominant Genomic Change in Sporadic Keratocystic Odontogenic Tumors. Am. J. Surg. Pathol. 2020, 44, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Charazac, A.; Fayyad, N.; Beal, D.; Bourgoin-Voillard, S.; Seve, M.; Sauvaigo, S.; Lamartine, J.; Soularue, P.; Moratille, S.; Martin, M.T.; et al. Impairment of Base Excision Repair in Dermal Fibroblasts Isolated From Nevoid Basal Cell Carcinoma Patients. Front. Oncol. 2020, 10, 1551. [Google Scholar] [CrossRef]
- Phatak, A.; Athar, M.; Crowell, J.A.; Leffel, D.; Herbert, B.S.; Bale, A.E.; Kopelovich, L. Global gene expression of histologically normal primary skin cells from BCNS subjects reveals “single-hit” effects that are influenced by rapamycin. Oncotarget 2019, 10, 1360–1387. [Google Scholar] [CrossRef]
- Beltrami, B.; Prada, E.; Tolva, G.; Scuvera, G.; Silipigni, R.; Graziani, D.; Bulfamante, G.; Gervasini, C.; Marchisio, P.; Milani, D. Unexpected phenotype in a frameshift mutation of PTCH1. Mol. Genet. Genom. Med. 2020, 8, e987. [Google Scholar] [CrossRef]
- Kimonis, V.E.; Goldstein, A.M.; Pastakia, B.; Yang, M.L.; Kase, R.; DiGiovanna, J.J.; Bale, A.E.; Bale, S.J. Clinical manifestations in 105 persons with nevoid basal cell carcinoma syndrome. Am. J. Med. Genet. 1997, 69, 299–308. [Google Scholar] [CrossRef]
- Palacios-Álvarez, I.; González-Sarmiento, R.; Fernández-López, E. Gorlin Syndrome. Actas Dermo-Sifiliográficas (Engl. Ed.) 2018, 109, 207–217. [Google Scholar] [CrossRef]
- Onodera, S.; Nakamura, Y.; Azuma, T. Gorlin Syndrome: Recent Advances in Genetic Testing and Molecular and Cellular Biological Research. Int. J. Mol. Sci. 2020, 21, 7559. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Xu, N.; Yang, C.; Yang, K.; Bian, Z. Novel PTCH1 mutation in Gorlin-Goltz syndrome potentially altered interactions with lipid bilayer. Oral. Dis. 2021, 27, 475–483. [Google Scholar] [CrossRef]
- Hoyos-Cadavid, A.M.; Kaminagakura, E.; Rodrigues, M.F.S.D.; Pinto, C.A.L.; Teshima, T.H.N.; Alves, F.A. Immunohistochemical evaluation of Sonic Hedgehog signaling pathway proteins (Shh, Ptch1, Ptch2, Smo, Gli1, Gli2, and Gli3) in sporadic and syndromic odontogenic keratocysts. Clin. Oral. Investig. 2019, 23, 153–159. [Google Scholar] [CrossRef]
- Gurgel, C.A.; Buim, M.E.; Carvalho, K.C.; Sales, C.B.; Reis, M.G.; de Souza, R.O.; de Faro Valverde, L.; de Azevedo, R.A.; Dos Santos, J.N.; Soares, F.A.; et al. Transcriptional profiles of SHH pathway genes in keratocystic odontogenic tumor and ameloblastoma. J. Oral. Pathol. Med. 2014, 43, 619–626. [Google Scholar] [CrossRef]
- Garcia-Garcia, M.; García-González, S.; Cabañuz, C.; Prieto-Torres, L. Gorlin-Like Phenotype in a Young Girl With a De Novo PTCH2 Variant Mutation of Uncertain Significance. Am. J. Dermatopathol. 2024, 46, 247–251. [Google Scholar] [CrossRef]
- Lin, M.J.; Dubin, D.P.; Khorasani, H.; Giordano, C.N. Basal cell nevus syndrome: From DNA to therapeutics. Clin. Dermatol. 2020, 38, 467–476. [Google Scholar] [CrossRef]
- Kalogirou, E.M.; Thermos, G.; Zogopoulos, V.; Foutadakis, S.; Michalopoulos, I.; Agelopoulos, M.; Tosios, K.I. The immunohistochemical profile of basal cell nevus syndrome-associated and sporadic odontogenic keratocysts: A systematic review and meta-analysis. Clin. Oral. Investig. 2021, 25, 3351–3367. [Google Scholar] [CrossRef]
- Gorlin, R.; Cohen, M.; Hennekam, R. Syndromes of the Head and Neck, 4th ed.; Oxford University Press: New York, NY, USA, 2001. [Google Scholar]
- Shimada, Y.; Morita, K.; Kabasawa, Y.; Taguchi, T.; Omura, K. Clinical manifestations and treatment for keratocystic odontogenic tumors associated with nevoid basal cell carcinoma syndrome: A study in 25 Japanese patients. J. Oral. Pathol. Med. 2013, 42, 275–280. [Google Scholar] [CrossRef]
- Woolgar, J.A.; Rippin, J.W.; Browne, R.M. A comparative histological study of odontogenic keratocysts in basal cell naevus syndrome and control patients. J. Oral. Pathol. 1987, 16, 75–80. [Google Scholar] [CrossRef]
- PTCH1. The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000185920-PTCH1 (accessed on 15 May 2024).
- Evans, D.G. Nevoid Basal Cell Carcinoma Syndrome. In GeneReviews®; Adam, M.P., Feldman, J., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 2002. [Google Scholar]
- Morita, K.; Naruto, T.; Tanimoto, K.; Yasukawa, C.; Oikawa, Y.; Masuda, K.; Imoto, I.; Inazawa, J.; Omura, K.; Harada, H. Simultaneous Detection of Both Single Nucleotide Variations and Copy Number Alterations by Next-Generation Sequencing in Gorlin Syndrome. PLoS ONE 2015, 10, e0140480. [Google Scholar] [CrossRef]
- Valdivia, A.D.C.M.; Ramos-Ibarra, M.L.; Franco-Barrera, M.J.; Arias-Ruiz, L.F.; García-Cruz, J.M.; Torres-Bugarín, O. What is Currently Known about Odontogenic Keratocysts? Oral. Health Prev. Dent. 2022, 20, 321–330. [Google Scholar] [CrossRef]
- Peled, M.; Kohn, Y.; Laufer, D. Conservative approach to unerupted teeth within cystic lesions in Gorlin’s syndrome. Am. J. Orthod. Dentofacial Orthop. 1991, 99, 294–297. [Google Scholar] [CrossRef]
- Longley, D.B.; Harkin, D.P.; Johnston, P.G. 5-fluorouracil: Mechanisms of action and clinical strategies. Nat. Rev. Cancer 2003, 3, 330–338. [Google Scholar] [CrossRef]
- Ledderhof, N.J.; Caminiti, M.F.; Bradley, G.; Lam, D.K. Topical 5-Fluorouracil is a Novel Targeted Therapy for the Keratocystic Odontogenic Tumor. J. Oral. Maxillofac. Surg. 2017, 75, 514–524. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Kaur, A.; Gomez, R.S.; Ellis, E., 3rd. Effectiveness of different treatments for odontogenic keratocyst: A network meta-analysis. Int. J. Oral. Maxillofac. Surg. 2023, 52, 32–43. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Major Criteria | Minor Criteria |
|---|---|
| More than two basal cell carcinomas or one in a patient under 30 years of age | Macrocephaly determined after size adjustment |
| Histologically confirmed odontogenic keratocysts | Congenital malformations: cleft lip or palate, bulging of the frontal bone, coarse facies, hypertelorism |
| Three or more palmoplantar pits | Skeletal abnormalities: Sprengel deformity, syndactyly |
| Bilamellar calcification of the falx cerebri | Radiological abnormalities: pons sella turcica, vertebral abnormalities such as fusion or elongation of the vertebral bodies |
| Bifid or fused ribs | Ovarian fibromas |
| First-degree relative with GGS | Medulloblastoma |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-López, G.; Mendoza-Álvarez, S.; Mejia-Velazquez, C.P.; Ramírez-Martínez, C.M.; Alonso-Moctezuma, A.; Jacinto-Alemán, L.F. Clinical Features and PTCH1 Expression in Gorlin–Goltz Syndrome: A Case Report. Reports 2025, 8, 34. https://doi.org/10.3390/reports8010034
González-López G, Mendoza-Álvarez S, Mejia-Velazquez CP, Ramírez-Martínez CM, Alonso-Moctezuma A, Jacinto-Alemán LF. Clinical Features and PTCH1 Expression in Gorlin–Goltz Syndrome: A Case Report. Reports. 2025; 8(1):34. https://doi.org/10.3390/reports8010034
Chicago/Turabian StyleGonzález-López, Gabriela, Samuel Mendoza-Álvarez, Claudia Patricia Mejia-Velazquez, Carla Monserrat Ramírez-Martínez, Alejandro Alonso-Moctezuma, and Luis Fernando Jacinto-Alemán. 2025. "Clinical Features and PTCH1 Expression in Gorlin–Goltz Syndrome: A Case Report" Reports 8, no. 1: 34. https://doi.org/10.3390/reports8010034
APA StyleGonzález-López, G., Mendoza-Álvarez, S., Mejia-Velazquez, C. P., Ramírez-Martínez, C. M., Alonso-Moctezuma, A., & Jacinto-Alemán, L. F. (2025). Clinical Features and PTCH1 Expression in Gorlin–Goltz Syndrome: A Case Report. Reports, 8(1), 34. https://doi.org/10.3390/reports8010034