

Same Incision for Simultaneous Laparoscopic Hand-Assisted Native Nephrectomy Contralateral to the Site of the Kidney Transplant

 ,
,  , ,
, ,  ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Case Report
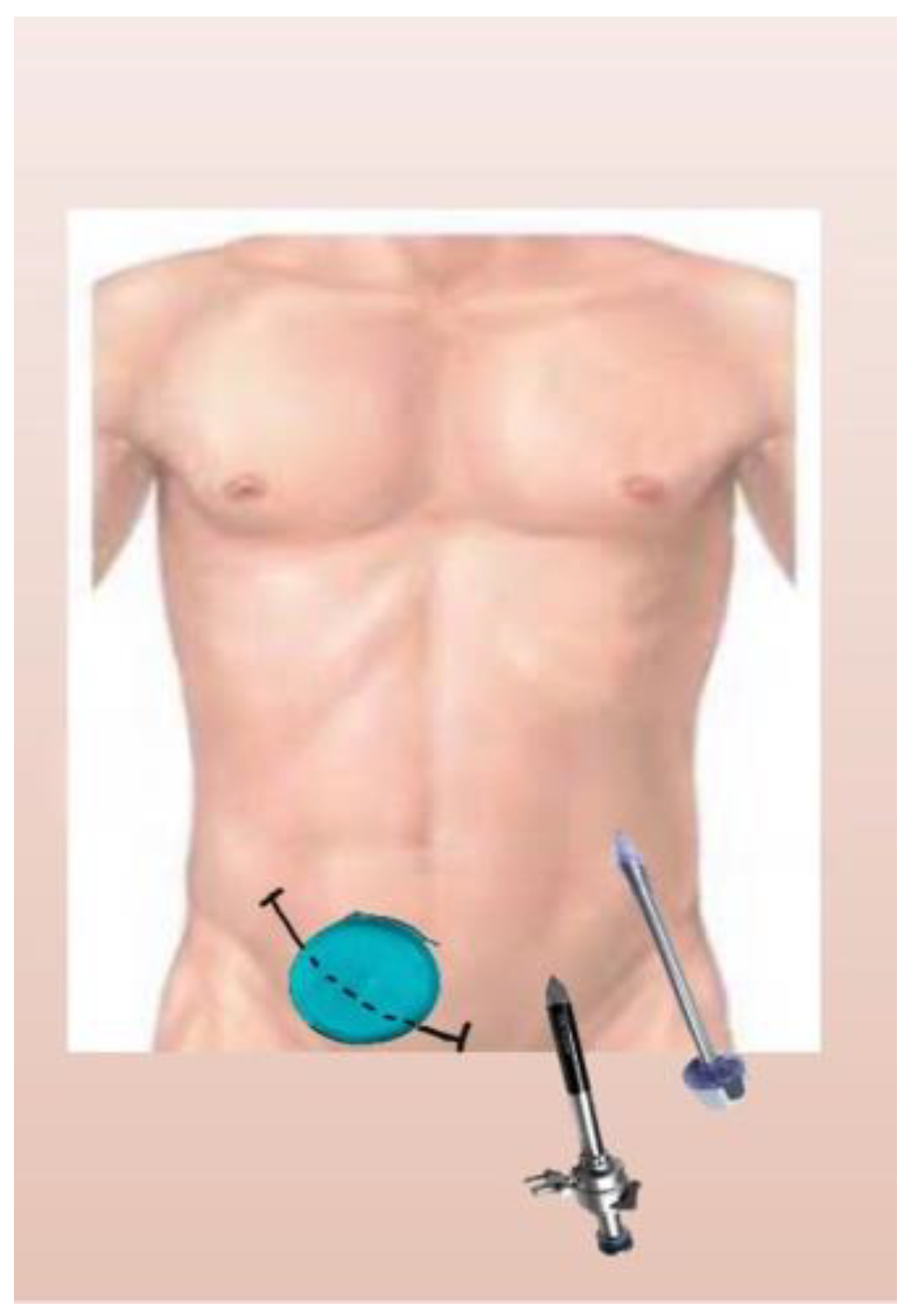
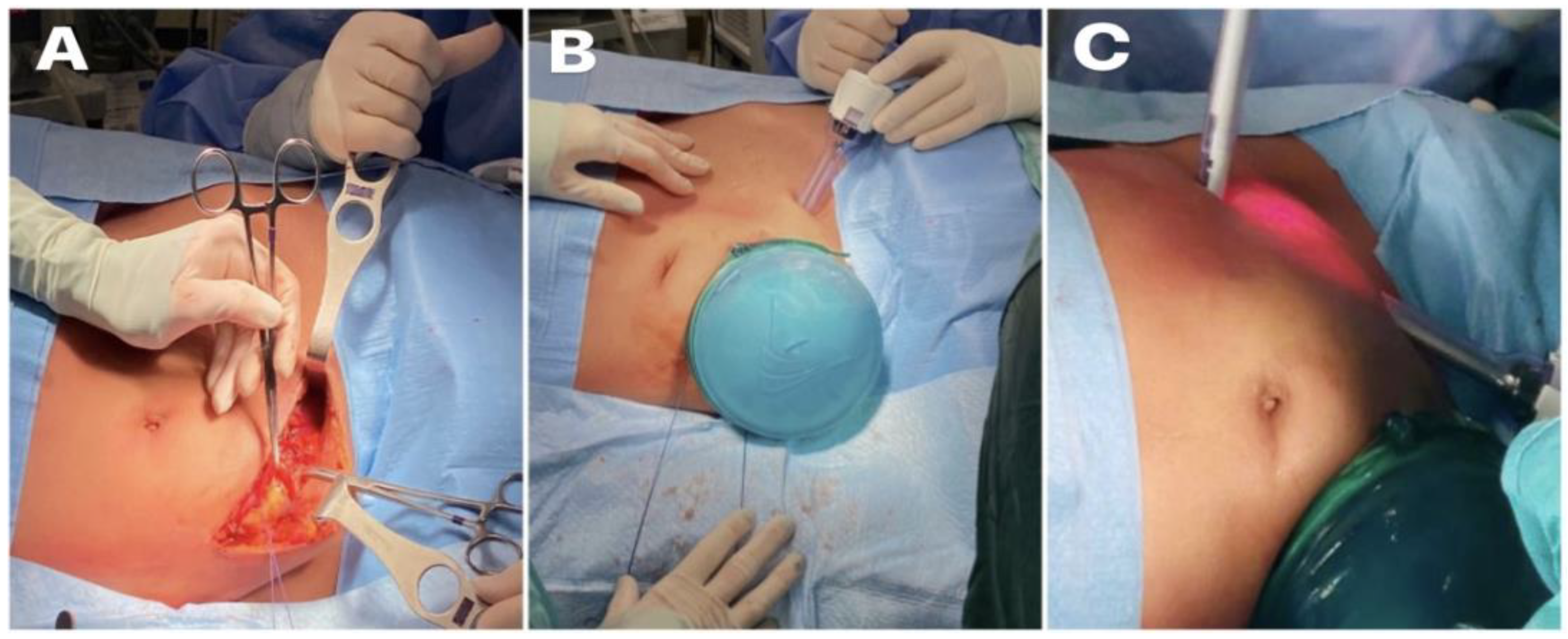
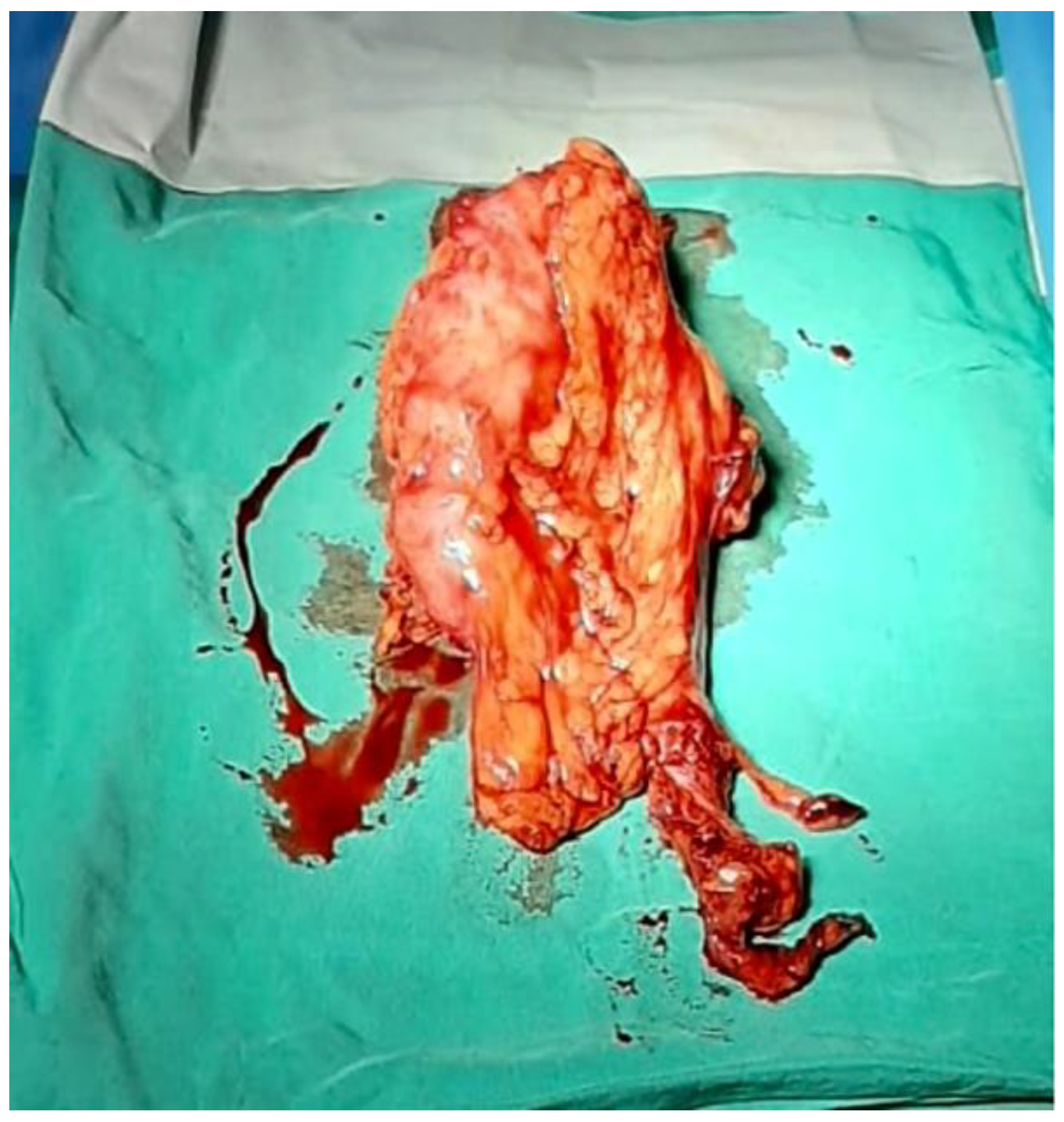
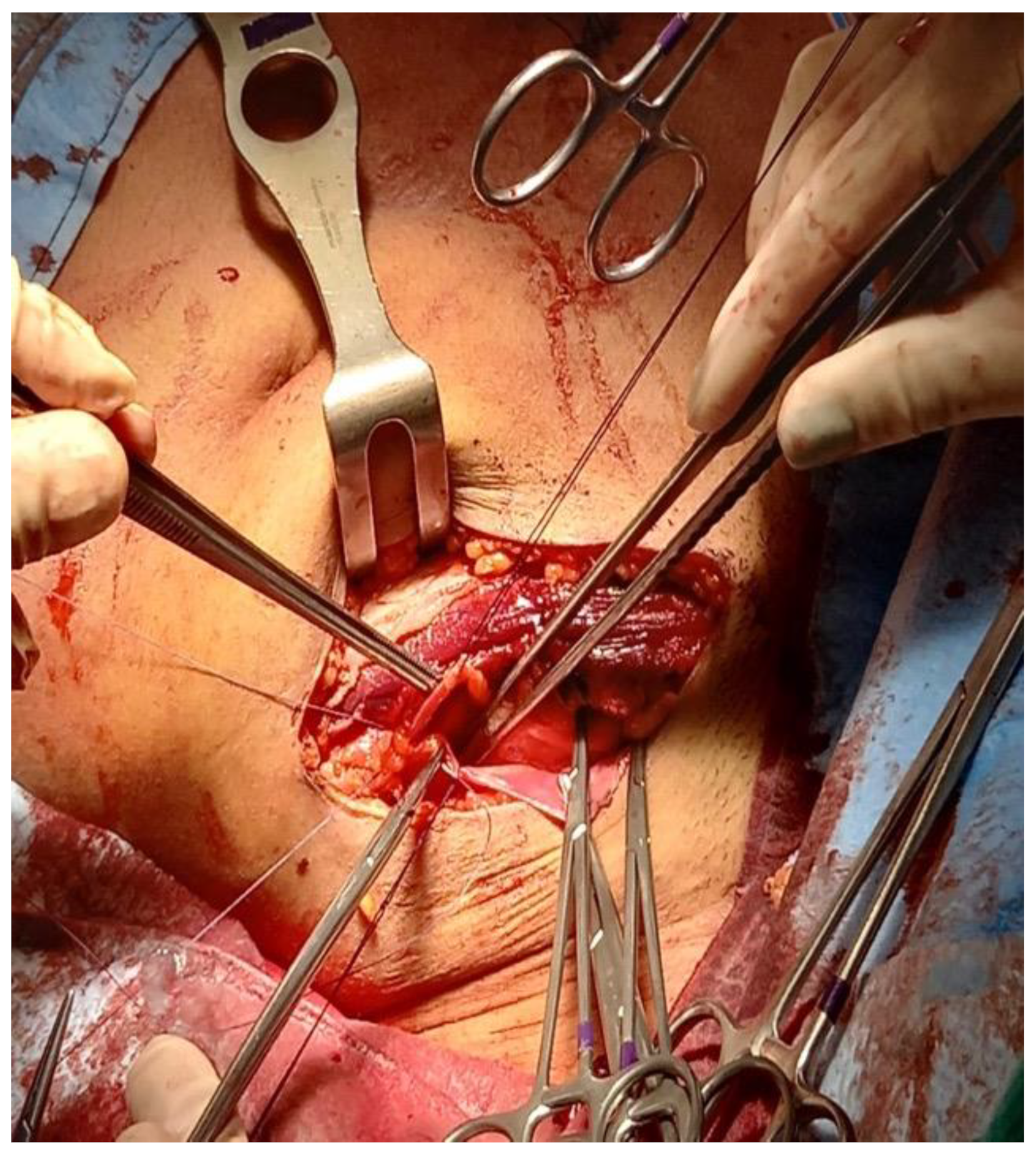
3. Methods and Procedure
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| APKD | Adult polycystic kidney disease |
| ESKD | End-stage kidney disease |
| KT | Kidney transplantation |
| LDKT | Living donor kidney transplantation |
| LHA-DN | Laparoscopic hand-assisted donor nephrectomy |
| LHA-NN | Laparoscopic hand-assisted native nephrectomy |
| LIF | Left iliac fossa |
| NN | Native nephrectomy |
| RIF | Right iliac fossa |
References
- Xu, J.; D’Souza, K.; Lau, N.S.; Leslie, S.; Lee, T.; Yao, J.; Lam, S.; Sandroussi, C.; Chadban, S.; Ying, T.; et al. Staged versus concurrent native nephrectomy and renal transplantation in patients with autosomal dominant polycystic kidney disease: A systematic review. Transplant. Rev. 2022, 36, 100652. [Google Scholar] [CrossRef] [PubMed]
- Kizilbash, S.J.; Huynh, D.; Kirchner, V.; Lewis, J.; Verghese, P.S. Timing of nativenephrectomy and kidney transplant outcomes in children. Pediatr. Transplant. 2021, 25, e13952. [Google Scholar] [CrossRef] [PubMed]
- Jean, R.A.; Alexandre, M.; Yoo, P.S. KidneyTransplantation with and without NativeNephrectomy for Polycystic Kidney Disease: Results of the National Inpatient Sample and the Rationale for a 2-Staged Procedure. J. Am. Coll. Surg. 2018, 226, 1079–1084. [Google Scholar] [CrossRef] [PubMed]
- Jänigen, B.M.; Hempel, J.; Holzner, P.; Schneider, J.; Fichtner-Feigl, S.; Thomusch, O.; Neeff, H.; Pisarski, P.; Glatz, T. Simultaneous ipsilateral nephrectomy during kidneytransplantation in autosomal dominant polycystic kidney disease: A matched pair analysis of 193 consecutive cases. Arch. Surg. 2020, 405, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Jochmans, I.; Monbaliu, D.; Ceulemans, L.; Pirenne, J.; Froněk, J. Simultaneous liver kidneytransplantation and (bilateral) nephrectomy through a midline is feasible and safe in polycystic disease. PLoS ONE 2017, 12, e0174123. [Google Scholar] [CrossRef] [PubMed]
- AbrolPrieto, N.; Prieto, M. Simultaneous Hand-assisted Laparoscopic Bilateral NativeNephrectomy and KidneyTransplantation for Patients with Large Polycystic Kidneys. Urology 2020, 146, 271–277. [Google Scholar] [CrossRef]
- Rasmussen, A.; Levine, M.; Mandurah, M.; Sener, A.; Luke, P. Staged vs. simultaneous bilateral nephrectomy and kidney transplantation in patients with autosomal dominant polycystic kidney disease: Outcomes and costs. Can. Urol. Assoc. J. 2022, 16, 424–429. [Google Scholar] [CrossRef] [PubMed]
- El-Galley, R.; Safavy, S.; Busby, J.E.; Colli, J. Outcome of hand assisted laparoscopic bilateral nativenephrectomy in transplantrecipients. J. Urol. 2011, 185, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Greenleaf, E.; Farooq, U.; Jain, A.; DiCristina, R.; Kadry, Z.; Sharma, R. Native kidney pyelonephritis as the cause of recurrent urinary tract infections in a kidneytransplantrecipient. Kidney Int. 2018, 93, 762. [Google Scholar] [CrossRef] [PubMed]
- Lich, R.; Howerton, L.W.; Davis, L.A. Childhood urosepsis. J. Ky. Med. Assoc. 1961, 59, 1177–1179. Available online: https://pubmed.ncbi.nlm.nih.gov/14465076/ (accessed on 1 June 2022). [PubMed]
- Joshi, P.; Lin, J.; Sura, T.; Limbu, P.S.; Melkonian, V.; Bastani, B.; Varma, C. Kidney Autotransplantation for Treatment of Ureteric Obstruction: A Case Report and Brief Review of the Literature. Case Rep. Surg. 2021, 2021, 6646958. [Google Scholar] [CrossRef] [PubMed]
- Aufhauser, D.D., Jr.; Peng, A.W.; Murken, D.R.; Concors, S.J.; Abt, P.L.; Sawinski, D.; Bloom, R.D.; Reese, P.P.; Levine, M.H. Impact of prolongeddialysis prior to renaltransplantation. Clin. Transplant. 2018, 32, e13260. [Google Scholar] [CrossRef] [PubMed]
- Argyrou, C.; Moris, D.; Vernadakis, S. Tailoring the ‘Perfect Fit’ for Renal Transplant Recipients with End-stage Polycystic Kidney Disease: Indications and Timing of Native Nephrectomy. In Vivo 2017, 31, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Chebib, F.T.; Prieto, M.; Yeonsoon, J.; Irazabal, M.V.; Kremers, W.K.; Dean, P.G.; Rea, D.J.; Cosio, F.G.; Torres, V.E.; El-Zoghby, Z.M. Native Nephrectomy in Renal Transplant Recipients with Autosomal Dominant Polycystic Kidney Disease. Transplant. Direct 2015, 1, e43. [Google Scholar] [CrossRef] [PubMed]
- Guo, P.; Xu, W.; Li, H.; Ren, T.; Ni, S.; Ren, M. Laparoscopic Nephrectomy versus Open Nephrectomy for Patients with Autosomal Dominant Polycystic Kidney Disease: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0129317. [Google Scholar] [CrossRef] [PubMed]
- Abrol, N.; Bentall, A.; Torres, V.E.; Prieto, M. Simultaneous bilateral laparoscopic nephrectomy with kidney transplantation in patients with ESRD due to ADPKD: A single-center experience. Am. J. Transplant. 2021, 21, 1513–1524. [Google Scholar] [CrossRef] [PubMed]
- Favi, E.; Iesari, S.; Catarsini, N.; Sivaprakasam, R.; Cucinotta, E.; Manzia, T.; Puliatti, C.; Cacciola, R. Outcomes and surgical complications following living-donor renal transplantation using kidneys retrieved with trans-peritoneal or retro-peritoneal hand-assisted laparoscopic nephrectomy. Clin. Transplant. 2020, 34, e14113. [Google Scholar] [CrossRef] [PubMed]
- Angelico, R.; Guzzo, I.; Pellicciaro, M.; Saffioti, M.C.; Grimaldi, C.; Mourani, C.; Smedile, F.; Pariante, R.; Semprini, A.; Monti, L.; et al. Same Donor Laparoscopic Liver and Kidney Procurement for Sequential Living Donor Liver-Kidney Transplantation in Primary Hyperoxaluria Type I. J. Laparoendosc. Adv. Surg. Tech. 2019, 29, 1616–1622. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.; Robb, M.; Hughes, W.; Johnson, R.; Ploeg, R.; Neuberger, J.; Forsythe, J.; Cacciola, R. Outcomes of Patients Suspended from the National Kidney Transplant Waiting List in the United Kingdom between 2000 and 2010. Transplantation 2020, 104, 1654–1661. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angelico, R.; Keçi, L.; Tariciotti, L.; Anselmo, A.; Favi, E.; Manzia, T.M.; Tisone, G.; Cacciola, R. Same Incision for Simultaneous Laparoscopic Hand-Assisted Native Nephrectomy Contralateral to the Site of the Kidney Transplant. Reports 2023, 6, 29. https://doi.org/10.3390/reports6020029
Angelico R, Keçi L, Tariciotti L, Anselmo A, Favi E, Manzia TM, Tisone G, Cacciola R. Same Incision for Simultaneous Laparoscopic Hand-Assisted Native Nephrectomy Contralateral to the Site of the Kidney Transplant. Reports. 2023; 6(2):29. https://doi.org/10.3390/reports6020029
Chicago/Turabian StyleAngelico, Roberta, Laura Keçi, Laura Tariciotti, Alessandro Anselmo, Evaldo Favi, Tommaso Maria Manzia, Giuseppe Tisone, and Roberto Cacciola. 2023. "Same Incision for Simultaneous Laparoscopic Hand-Assisted Native Nephrectomy Contralateral to the Site of the Kidney Transplant" Reports 6, no. 2: 29. https://doi.org/10.3390/reports6020029
APA StyleAngelico, R., Keçi, L., Tariciotti, L., Anselmo, A., Favi, E., Manzia, T. M., Tisone, G., & Cacciola, R. (2023). Same Incision for Simultaneous Laparoscopic Hand-Assisted Native Nephrectomy Contralateral to the Site of the Kidney Transplant. Reports, 6(2), 29. https://doi.org/10.3390/reports6020029