
The Relationship between the Items of the Barthel Index and Short-Term Prognosis in Terminal Cancer Patients

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
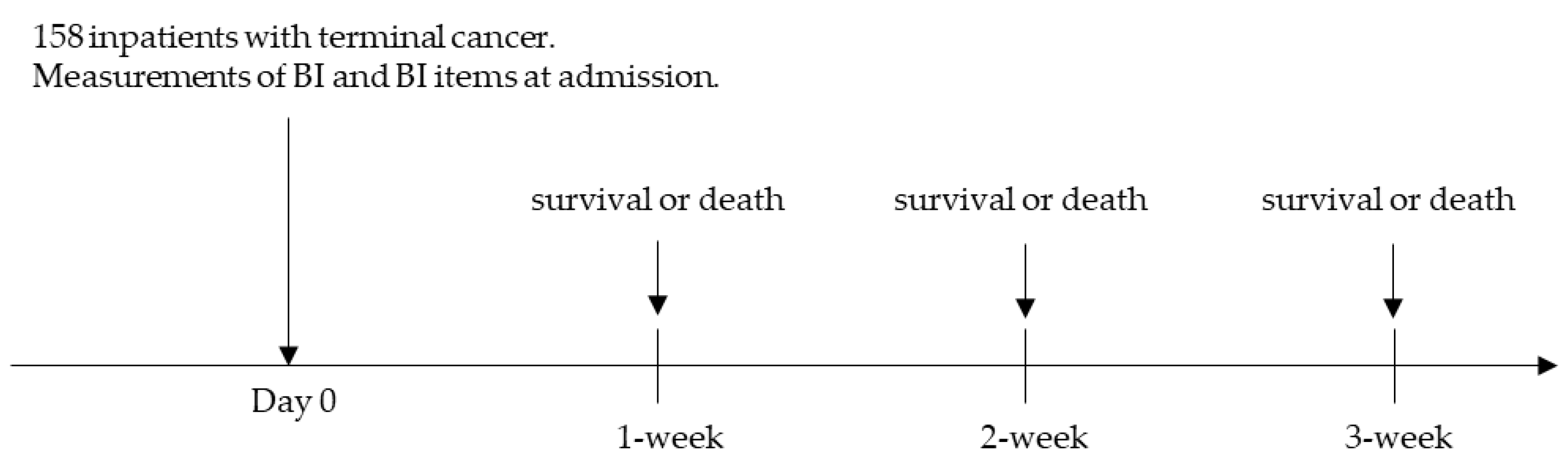
2.1. Patients
2.2. BI evaluation Methods
2.3. Predictive Performance
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steinhauser, K.E.; Christakis, N.A.; Clipp, E.C.; McNeilly, M.; McIntyre, L.; Tulsky, J.A. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA 2000, 284, 2476–2482. [Google Scholar] [CrossRef] [PubMed]
- Niki, K.; Okamoto, Y.; Matano, Y.; Ishii, R.; Matsuda, Y.; Takagi, T.; Uejima, E. Validation of a short–term, objective, prognostic predictive method for terminal cancer patients in a palliative care unit using a combination of six laboratory test items. J. Palliat. Med. 2019, 22, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Tei, Y.; Inoue, S. Correlation of the dose of midazolam for symptom control with administration periods: The possibility of tolerance. J. Pain Symptom Manag. 2003, 25, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.; Harth, T.; Hruby, G.; Finkelstein, J.; Wu, J.; Danjoux, C. How accurate are physicians’ clinical predictions of survival and the available prognostic tools in estimating survival times in terminally ill cancer patients?—A systematic review. Clin. Oncol. 2001, 13, 209–218. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Maryland. State. Mad. J. 1965, 14, 61–65. [Google Scholar]
- Godfrey, J.; Poole, L. An audit of the use of the Barthel Index in palliative care. Int. J. Palliat. Nurs. 2007, 13, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Okazaki, K.; Murakami, F.; Okamoto, S.; Sugihara, H.; Banshoya, K.; Onoda, T.; Takei, E.; Takeda, S.; Sugihara, N. Examination of a Short–Term, Prognostic Predictive Method for Terminal Cancer Patients Using the Barthel Index. Reports 2020, 3, 26. [Google Scholar] [CrossRef]
- Okada, M.; Okazaki, K.; Murakami, F.; Okamoto, S.; Sugihara, H.; Hoshino, Y.; Goto, Y.; Banshoya, K.; Kimura, K.; Onoda, T.; et al. The Relationship between Components of the Barthel Index and Mortality of Terminal Cancer Patients. Iryo Yakugaku (Jpn. J. Pharm. Health Care Sci.) 2019, 45, 605–609. [Google Scholar] [CrossRef]
- Sinoff, G.; Ore, L. The Barthel activities of daily living index: Self–reporting versus actual performance in the old–old (> or = 75 years). J. Am. Geriatr. Soc. 1997, 45, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy–to–use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Baba, M.; Maeda, I.; Morita, T.; Inoue, S.; Ikenaga, M.; Matsumoto, Y.; Sekine, R.; Yamaguchi, T.; Hirohashi, T.; Tajima, T.; et al. Survival prediction for advanced cancer patients in the real world: A comparison of the Palliative Prognostic Score, Delirium–Palliative Prognostic Score, Palliative Prognostic Index and modified Prognosis in Palliative Care Study predictor model. Eur. J. Cancer 2015, 51, 1618–1629. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.; Ryall, N. Using the modified Barthel index to estimate survival in cancer patients in hospice: Observational study. BMJ 2000, 321, 1381–1382. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.; Jessop, E.G. A comparison of measures of disability and health status in people with physical disabilities undergoing vocational rehabilitation. J. Public Health 1996, 18, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Disease, P.V.; Kodama, A.; Koyama, A.; Sugimoto, M.; Niimi, K.; Banno, H.; Komori, K. Association Between Preoperative Frailty and Mortality in Patients With Critical Limb Ischemia Following Infrainguinal Bypass Surgery―Usefulness of the Barthel Index―. Circ. J. 2018, 82, 267–274. [Google Scholar] [CrossRef]
- Maltoni, M.; Caraceni, A.; Brunelli, C.; Broeckaert, B.; Christakis, N.; Eychmueller, S.; Glare, P.; Nabal, M.; Vigano, A.; Larkin, P.; et al. Prognostic factors in advanced cancer patients: Evidence-based clinical recommendations—A study by the steering committee of the european association for palliative care. J. Clin. Oncol. 2005, 23, 6240–6248. [Google Scholar] [CrossRef] [PubMed]
- Lau, F.; Cloutier-Fisher, D.; Kuziemsky, C.; Black, F.; Downing, M.; Borycki, E.; Ho, F. A Systematic Review of Prognostic Tools for Estimating Survival Time in Palliative Care. J. Palliat Care 2007, 23, 93–112. [Google Scholar] [CrossRef]
- Morita, T.; Tsunoda, J.; Inoue, S.; Chihara, S. The Palliative Prognostic Index: A scoring system for survival prediction of terminally ill cancer patients. Support. Care Cancer 1999, 7, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Tsunoda, J.; Inoue, S.; Chihara, S. Improved accuracy of physicians’ survival prediction for terminally ill cancer patients using the Palliative Prognostic Index. Palliat. Med. 2001, 15, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Paiva, C.E.; Del Fabbro, E.G.; Steer, C.; Naberhuis, J.; van de Wetering, M.; Fernández-Ortega, P.; Morita, T.; Suh, S.Y.; Bruera, E.; et al. Prognostication in advanced cancer: Update and directions for future research. Support. Care Cancer 2019, 27, 1973–1984. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Maxwell, J.P.; Paiva, C.E. Dealing with prognostic uncertainty: The role of prognostic models and websites for patients with advanced cancer. Curr. Opin. Support. Palliat. Care 2019, 13, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Iizuka-Honma, H.; Mitsumori, T.; Yoshikawa, S.; Takizawa, H.; Noguchi, M. Prognostic Value of Palliative Prognostic Index for Hospitalized Patients With End-of-Life Hematologic Malignancies in a Japanese University Hospital. JCO Oncol. Pract. 2022, 18, e108–e116. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Morita, T.; Maeda, I.; Inoue, S.; Ikenaga, M.; Matsumoto, Y.; Baba, M.; Sekine, R.; Yamaguchi, T.; Hirohashi, T.; et al. A prospective, multicenter cohort study to validate a simple performance status–based survival prediction system for oncologists. Cancer 2017, 123, 1442–1452. [Google Scholar] [CrossRef] [PubMed]
- Anderson, F.; Downing, G.M.; Hill, J.; Casorso, L.; Lerch, N. Palliative Performance Scale (PPS): A new tool. J. Palliat. Care 1996, 12, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Davis, T.E. Toxicology and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. Cancer Clin. Trials 1982, 5, 649–655. [Google Scholar]


{kind=link}
| Characteristic | Findings |
|---|---|
| N | 158 |
| Age (years) | 79 (71–85) |
| Sex (men/women), n (%) | 105/53 (66.5/33.5) |
| Primary cancer, n (%) | |
| Colorectal | 25 (15.8) |
| Lung malignant mesothelioma | 21 (13.3) |
| Gastric | 21 (13.3) |
| Liver | 17 (10.8) |
| Pancreatic | 15 (9.5) |
| Biliary Tract | 14 (8.9) |
| Blood | 12 (7.6) |
| Brain | 8 (5.1) |
| Prostate | 5 (3.2) |
| Bladder | 5 (3.2) |
| Others | 15 (9.5) |
| Duration between admission and death (days) | 20 (10–37) |
| Item | Cutoff Value | Sensitivity | Specificity | PPV | NPV | Accuracy | |
|---|---|---|---|---|---|---|---|
| 1-week | BI | 0–15/20–100 | 0.667 | 0.627 | 0.242 | 0.913 | 0.633 |
| Feeding | 0/5,10 | 0.625 | 0.791 | 0.349 | 0.922 | 0.766 | |
| Mobility | 0,5/10,15 | 0.833 | 0.507 | 0.233 | 0.944 | 0.557 | |
| Grooming | 0/5 | 0.875 | 0.276 | 0.178 | 0.925 | 0.367 | |
| Toilet use | 0/5,10 | 0.750 | 0.575 | 0.240 | 0.928 | 0.601 | |
| Bathing | 0/5 | 0.958 | 0.179 | 0.173 | 0.960 | 0.297 | |
| Transfer | 0/5,10,15 | 0.833 | 0.448 | 0.213 | 0.938 | 0.506 | |
| Stairs | 0/5,10 | 0.792 | 0.321 | 0.173 | 0.896 | 0.392 | |
| Dressing | 0/5,10 | 0.792 | 0.463 | 0.209 | 0.925 | 0.513 | |
| Bowels | 0/5,10 | 0.667 | 0.567 | 0.216 | 0.905 | 0.582 | |
| Bladder | 0/5,10 | 0.667 | 0.575 | 0.219 | 0.906 | 0.589 | |
| 2-week | BI | 0–15/20–100 | 0.571 | 0.667 | 0.485 | 0.739 | 0.633 |
| Feeding | 0/5,10 | 0.482 | 0.843 | 0.628 | 0.748 | 0.715 | |
| Mobility | 0,5/10,15 | 0.732 | 0.559 | 0.477 | 0.792 | 0.620 | |
| Grooming | 0/5 | 0.821 | 0.294 | 0.390 | 0.750 | 0.481 | |
| Toilet use | 0/5,10 | 0.607 | 0.598 | 0.453 | 0.735 | 0.601 | |
| Bathing | 0/5 | 0.893 | 0.186 | 0.376 | 0.760 | 0.437 | |
| Transfer | 0/5,10,15 | 0.714 | 0.471 | 0.426 | 0.750 | 0.557 | |
| Stairs | 0/5,10 | 0.821 | 0.373 | 0.418 | 0.792 | 0.532 | |
| Dressing | 0/5,10 | 0.661 | 0.471 | 0.407 | 0.716 | 0.538 | |
| Bowels | 0/5,10 | 0.589 | 0.598 | 0.446 | 0.726 | 0.595 | |
| Bladder | 0/5,10 | 0.571 | 0.598 | 0.438 | 0.718 | 0.589 | |
| 3-week | BI | 0–35/40–100 | 0.694 | 0.507 | 0.621 | 0.587 | 0.608 |
| Feeding | 0,5/10 | 0.647 | 0.521 | 0.611 | 0.559 | 0.589 | |
| Mobility | 0,5/10,15 | 0.659 | 0.589 | 0.651 | 0.597 | 0.627 | |
| Grooming | 0/5 | 0.835 | 0.356 | 0.602 | 0.650 | 0.614 | |
| Toilet use | 0,5/10 | 0.859 | 0.315 | 0.593 | 0.657 | 0.608 | |
| Bathing | 0/5 | 0.894 | 0.219 | 0.571 | 0.640 | 0.582 | |
| Transfer | 0/5,10,15 | 0.682 | 0.507 | 0.617 | 0.578 | 0.601 | |
| Stairs | 0/5,10 | 0.776 | 0.397 | 0.600 | 0.604 | 0.601 | |
| Dressing | 0/5,10 | 0.659 | 0.521 | 0.615 | 0.567 | 0.595 | |
| Bowels | 0,5/10 | 0.682 | 0.493 | 0.611 | 0.571 | 0.595 | |
| Bladder | 0,5/10 | 0.706 | 0.466 | 0.606 | 0.576 | 0.595 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okamoto, S.; Okazaki, K.; Okada, M.; Murakami, F.; Sugihara, H.; Hoshino, Y.; Ogawa, Y.; Banshoya, K.; Takei, E.; Takeda, S.; et al. The Relationship between the Items of the Barthel Index and Short-Term Prognosis in Terminal Cancer Patients. Reports 2023, 6, 5. https://doi.org/10.3390/reports6010005
Okamoto S, Okazaki K, Okada M, Murakami F, Sugihara H, Hoshino Y, Ogawa Y, Banshoya K, Takei E, Takeda S, et al. The Relationship between the Items of the Barthel Index and Short-Term Prognosis in Terminal Cancer Patients. Reports. 2023; 6(1):5. https://doi.org/10.3390/reports6010005
Chicago/Turabian StyleOkamoto, Shinya, Kazuko Okazaki, Masahiro Okada, Fumiyoshi Murakami, Hiroki Sugihara, Yoshinori Hoshino, Yuka Ogawa, Kengo Banshoya, Eisuke Takei, Shuso Takeda, and et al. 2023. "The Relationship between the Items of the Barthel Index and Short-Term Prognosis in Terminal Cancer Patients" Reports 6, no. 1: 5. https://doi.org/10.3390/reports6010005
APA StyleOkamoto, S., Okazaki, K., Okada, M., Murakami, F., Sugihara, H., Hoshino, Y., Ogawa, Y., Banshoya, K., Takei, E., Takeda, S., & Sugihara, N. (2023). The Relationship between the Items of the Barthel Index and Short-Term Prognosis in Terminal Cancer Patients. Reports, 6(1), 5. https://doi.org/10.3390/reports6010005