
Paroxysmal Atrial Fibrillation with Rapid Ventricular Response Following COVID-19 Nasopharyngeal Swab: A Case Report


 ,
, 

Abstract
1. Introduction
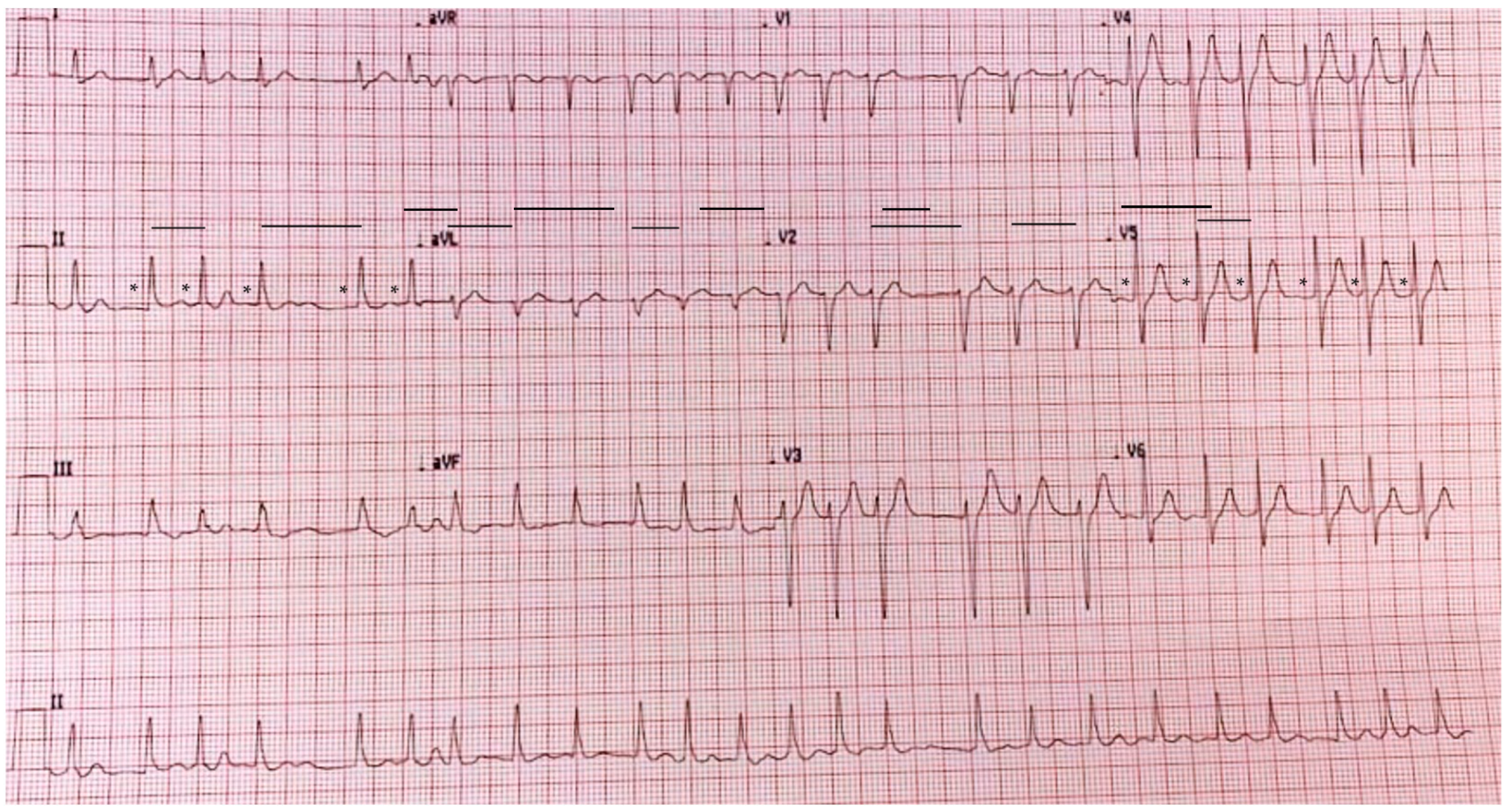
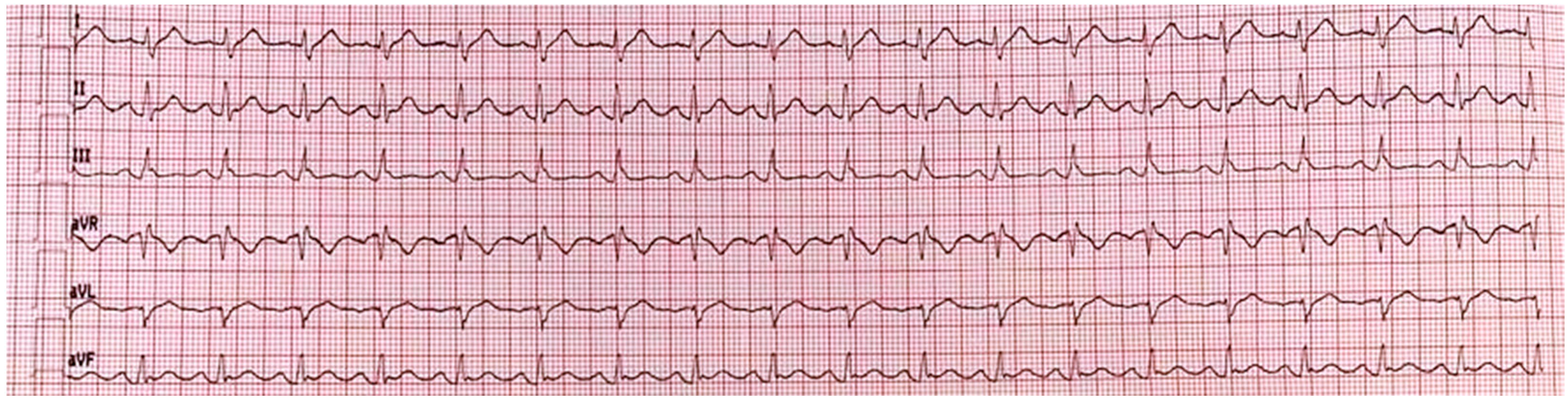
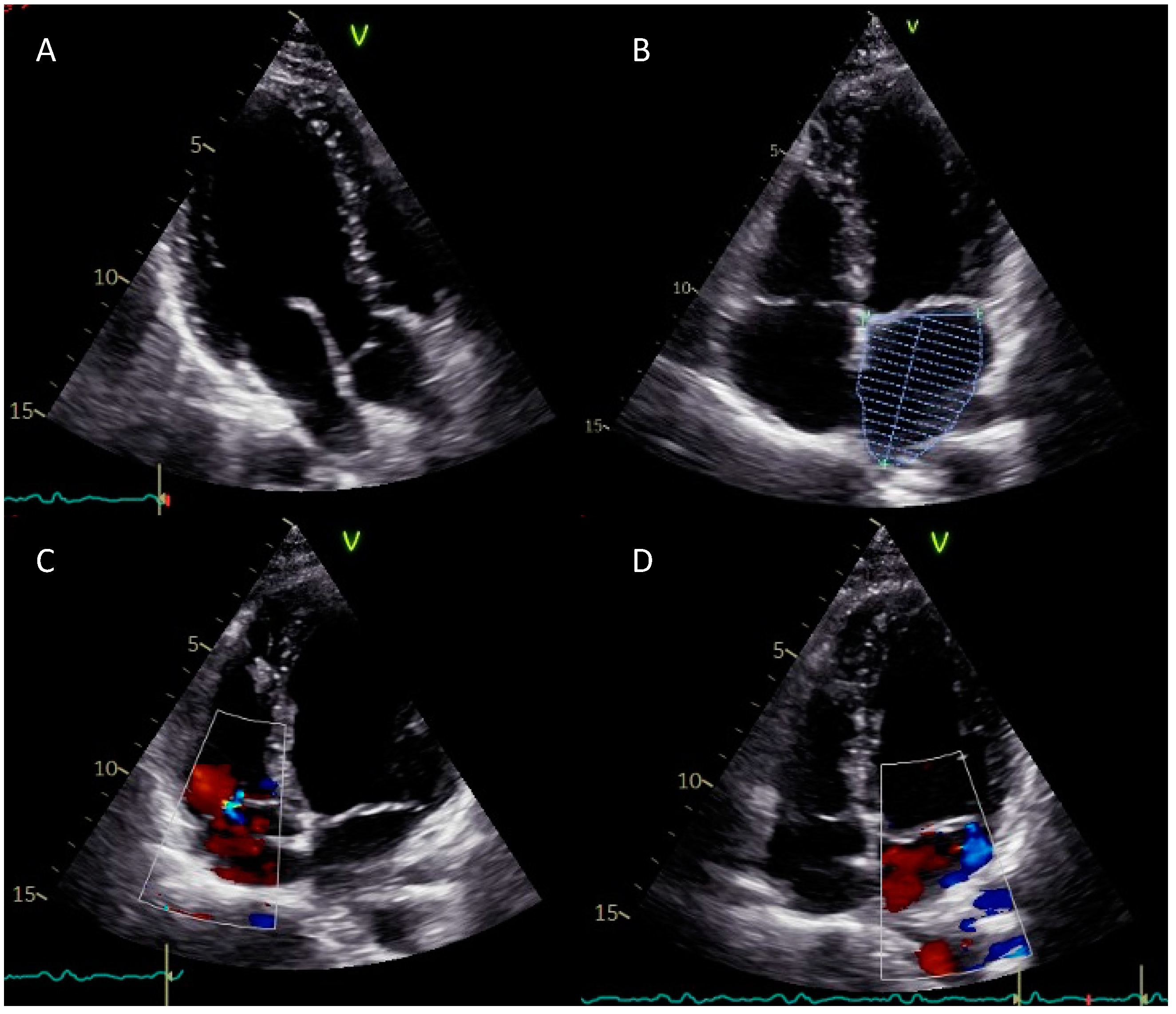
2. Case Report
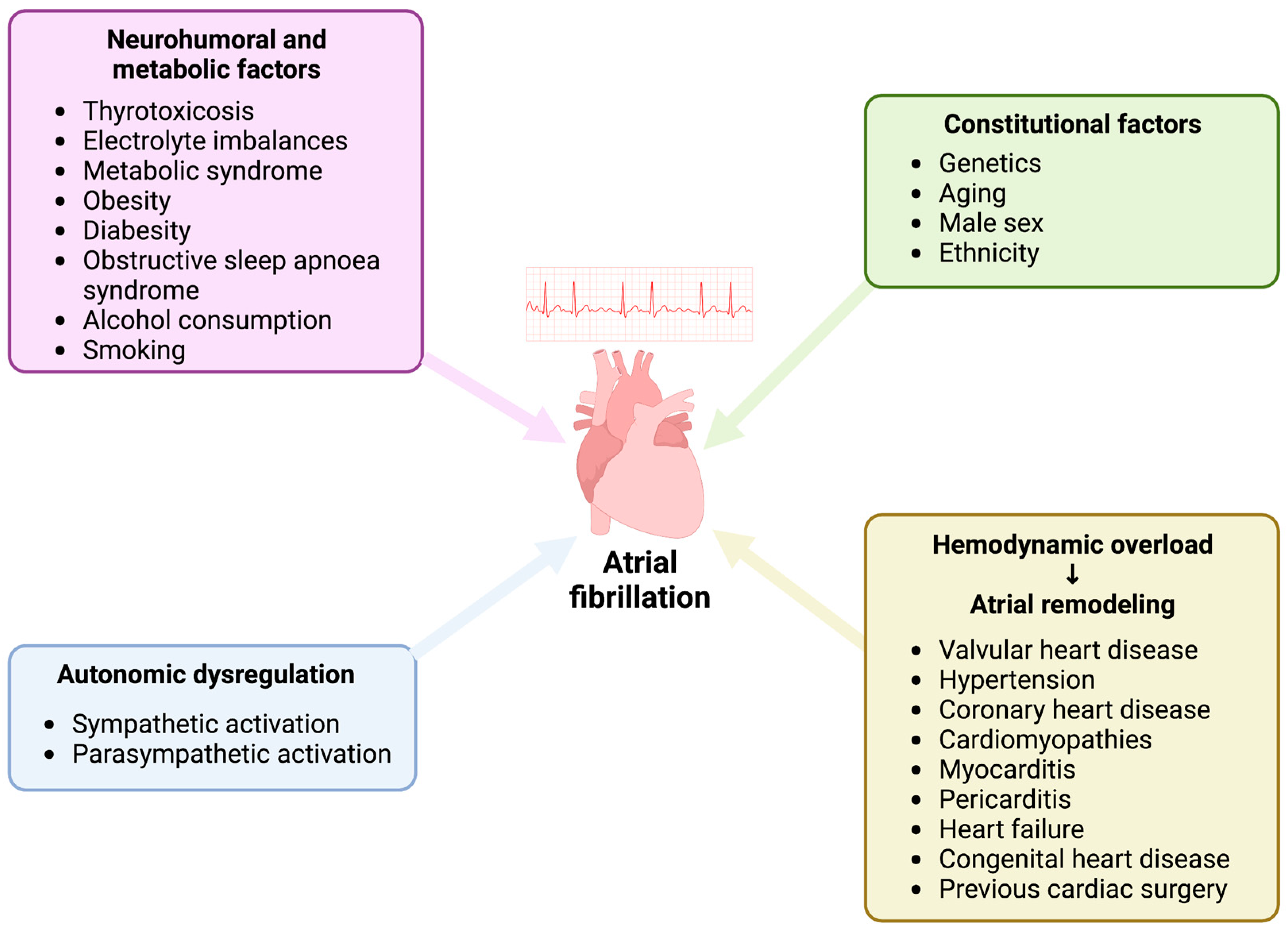
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Brundel, B.J.J.M.; Ai, X.; Hills, M.T.; Kuipers, M.F.; Lip, G.Y.H.; de Groot, N.M.S. Atrial fibrillation. Nat. Rev. Dis. Prim. 2022, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, A.; Frontera, A.; Bond, R.; Duncan, E.; Thomas, G. Vagal atrial fibrillation: What is it and should we treat it? Int. J. Cardiol. 2015, 201, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Qin, M.; Zeng, C.; Liu, X. The cardiac autonomic nervous system: A target for modulation of atrial fibrillation. Clin. Cardiol. 2019, 42, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ilsar, I.; Sabbah, H.N.; Ben David, T.; Mazgalev, T.N. Relationship between right cervical vagus nerve stimulation and atrial fibrillation inducibility: Therapeutic intensities do not increase arrhythmogenesis. Heart Rhythm. 2009, 6, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Gritzfeld, J.F.; Roberts, P.; Roche, L.; El Batrawy, S.; Gordon, S.B. Comparison between nasopharyngeal swab and nasal wash, using culture and PCR, in the detection of potential respiratory pathogens. BMC Res. Notes 2011, 4, 122. [Google Scholar] [CrossRef] [PubMed]
- Hasell, J.; Mathieu, E.; Beltekian, D.; Macdonald, B.; Giattino, C.; Ortiz-Ospina, E.; Roser, M.; Ritchie, H. A cross-country database of COVID-19 testing. Sci. Data 2020, 7, 345. [Google Scholar] [CrossRef] [PubMed]
- Piras, A.; Rizzo, D.; Longoni, E.; Turra, N.; Urru, S.; Saba, P.P.; Musumano, L.; Bussu, F. Nasopharyngeal swab collection in the suspicion of Covid-19. Am. J. Otolaryngol. 2020, 41, 102551. [Google Scholar] [CrossRef] [PubMed]
- Fabbris, C.; Cestaro, W.; Menegaldo, A.; Spinato, G.; Frezza, D.; Vijendren, A.; Borsetto, D.; Boscolo-Rizzo, P. Is oro/nasopharyngeal swab for SARS-CoV-2 detection a safe procedure? Complications observed among a case series of 4876 consecutive swabs. Am. J. Otolaryngol. 2021, 42, 102758. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.H.; Pang, S.; Naclerio, R.M.; Kashima, M. Complications of nasal SARS-CoV-2 testing: A review. J. Investig. Med. 2021, 69, 1399–1403. [Google Scholar] [CrossRef] [PubMed]
- Bloom, W.R.; Bloom, T.D. Neurally Mediated Syncope Triggered by COVID-19 Nasopharyngeal Swab Specimen Collection: A Case Report. Allergy Rhinol. 2022, 13, 21526567211073794. [Google Scholar] [CrossRef] [PubMed]
- Madanat, L.; Khalife, A.; Sims, M. Asystole During Nasopharyngeal Swab: Is COVID-19 to Blame? Cureus 2021, 13, e15448. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, T.; Mendelowith, D.; Golanov, E.; Spiriev, T.; Arasho, B.; Sandu, N.; Sadr-Eshkevari, P.; Meuwly, C.; Schaller, B.; Trigemino-Cardiac Reflex Examination Group. Trigeminocardiac reflex: The current clinical and physiological knowledge. J. Neurosurg. Anesthesiol. 2015, 27, 136–147. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Perez, M.V.; Mahaffey, K.W.; Hedlin, H.; Rumsfeld, J.S.; Garcia, A.; Ferris, T.; Balasubramanian, V.; Russo, A.M.; Rajmane, A.; Cheung, L.; et al. Large-Scale Assessment of a Smartwatch to Identify Atrial Fibrillation. N. Engl. J. Med. 2019, 381, 1909–1917. [Google Scholar] [CrossRef]
- Khan, A.A.; Lip, G.Y.H.; Shantsila, A. Heart rate variability in atrial fibrillation: The balance between sympathetic and parasympathetic nervous system. Eur. J. Clin. Investig. 2019, 49, e13174. [Google Scholar] [CrossRef] [PubMed]
- Meuwly, C.; Chowdhury, T.; Sandu, N.; Golanov, E.; Erne, P.; Rosemann, T.; Schaller, B. Definition and Diagnosis of the Trigeminocardiac Reflex: A Grounded Theory Approach for an Update. Front. Neurol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Laboratory Parameter (Unit of Measure) | Value | Normal Range |
|---|---|---|
| Hb (g/dL) | 15.50 | 13.50–17.50 |
| RBC (×106/μL) | 5.09 | 4.30–5.50 |
| WBC (×103/μL) | 6.70 | 4.00–10.00 |
| HCT (%) | 46.00 | 40.00–50.00 |
| MCV (fl) | 90.40 | 83.00–101.00 |
| RDW (%) | 12.40 | 11.00–16.00 |
| PLT (×103/μL) | 196.00 | 150.00–400.00 |
| AST (U/L) | 38.00 | 5.00–34.00 |
| ALT (U/L) | 51.00 | 0.00–55.00 |
| GGT (U/L) | 14.00 | 11.00–59.00 |
| CK (UI/L) | 161.00 | 30.00–200.00 |
| Plasma sodium (mmol/L) | 140.00 | 136.00–145.00 |
| Plasma potassium (mmol/L) | 4.10 | 3.50–5.10 |
| Creatinine (mg/dL) | 0.84 | 0.73–1.18 |
| Cholesterol (mg/dL) | 211.00 | <200.00 (optimal value) |
| HDL cholesterol (mg/dL) | 52.00 | >40 (optimal value) |
| LDL cholesterol (mg/dL) | 138.00 | <100.00 (optimal value) |
| Triglycerides (mg/dL) | 151.00 | 0.00–149.00 |
| Plasma glucose (mg/dL) | 96.00 | 74.00–106.00 |
| Blood urea (mg/dL) | 34.00 | 19.00–43.00 |
| Uric acid (mg/dL) | 5.30 | 3.50–7.20 |
| APTT (seconds) | 31.40 | 23.00–32.00 |
| INR | 1.02 | 0.80–1.20 |
| CRP (mg/dL) | 0.05 | <0.50 |
| Troponin I (pg/mL) | <10.0 | 0.00–34.20 |
| CKMB mass (ng/mL) | <0.3 | 0.00–5.20 |
| Myoglobin (ng/mL) | 38.00 | 0.00–154.90 |
| TSH (μUI/mL) | 1.96 | 0.35–4.94 |
| fT4 (pmol/L) | 11.10 | 9.01–19.50 |
| fT3 (pmol/L) | 5.76 | 2.89–4.88 |
| COVID-19 E gene | Negative | - |
| COVID-19 N gene | Negative | - |
| COVID-19 RdRp/s gene | Negative | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viscusi, M.M.; Ambrosio, L.; Ricciardi, D.; Mangiacapra, F.; Nusca, A.; Paolucci, L.; Ussia, G.P.; Grigioni, F. Paroxysmal Atrial Fibrillation with Rapid Ventricular Response Following COVID-19 Nasopharyngeal Swab: A Case Report. Reports 2023, 6, 15. https://doi.org/10.3390/reports6010015
Viscusi MM, Ambrosio L, Ricciardi D, Mangiacapra F, Nusca A, Paolucci L, Ussia GP, Grigioni F. Paroxysmal Atrial Fibrillation with Rapid Ventricular Response Following COVID-19 Nasopharyngeal Swab: A Case Report. Reports. 2023; 6(1):15. https://doi.org/10.3390/reports6010015
Chicago/Turabian StyleViscusi, Michele Mattia, Luca Ambrosio, Danilo Ricciardi, Fabio Mangiacapra, Annunziata Nusca, Luca Paolucci, Gian Paolo Ussia, and Francesco Grigioni. 2023. "Paroxysmal Atrial Fibrillation with Rapid Ventricular Response Following COVID-19 Nasopharyngeal Swab: A Case Report" Reports 6, no. 1: 15. https://doi.org/10.3390/reports6010015
APA StyleViscusi, M. M., Ambrosio, L., Ricciardi, D., Mangiacapra, F., Nusca, A., Paolucci, L., Ussia, G. P., & Grigioni, F. (2023). Paroxysmal Atrial Fibrillation with Rapid Ventricular Response Following COVID-19 Nasopharyngeal Swab: A Case Report. Reports, 6(1), 15. https://doi.org/10.3390/reports6010015