
Usefulness of Circulating CYFRA21-1 in Patients as a Biomarker in Patients Taking Sorafenib or Lenvatinib for Unresectable Hepatocellular Carcinoma

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Administration of SOR/LEN
2.3. Measurement of Serum CYFRA21-1
2.4. Follow-Up after Administration
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
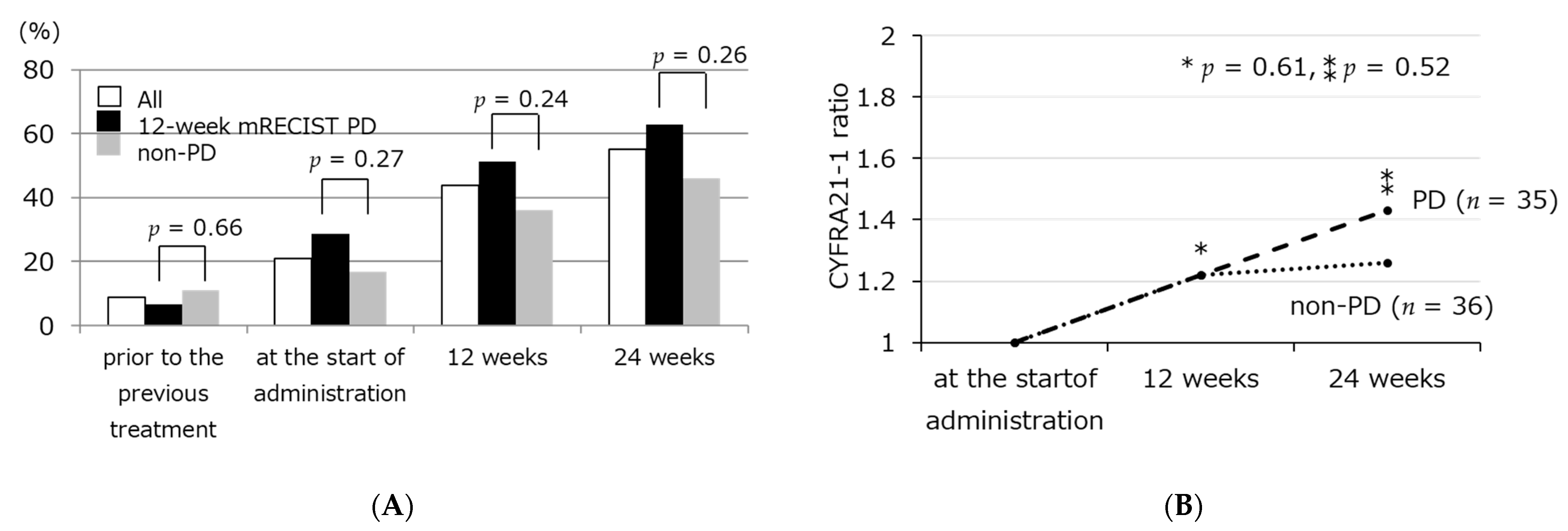
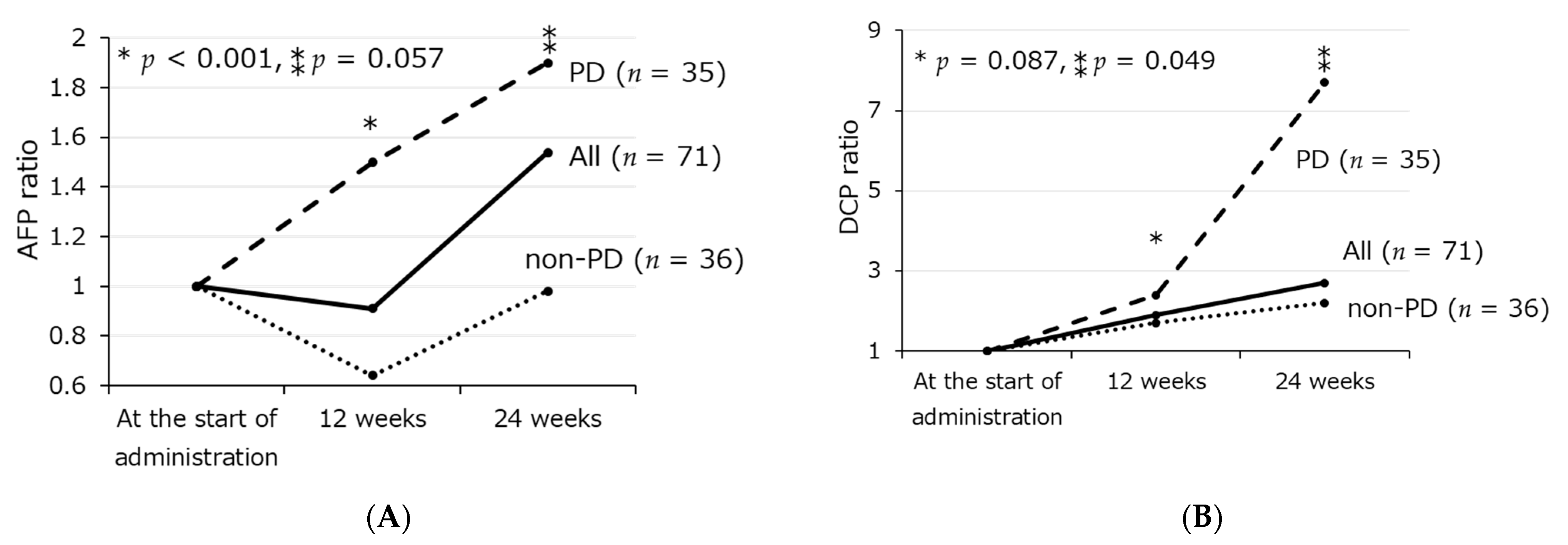
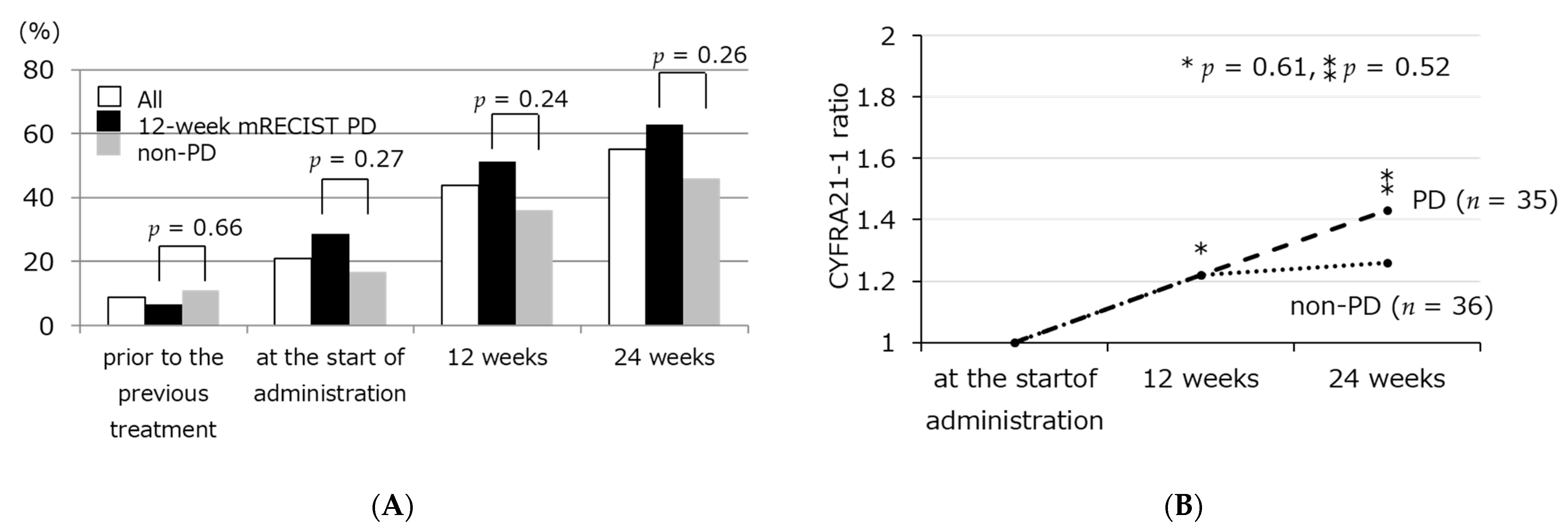
3.2. Transition of Tumor Markers Including Serum CYFRA21-1 Level
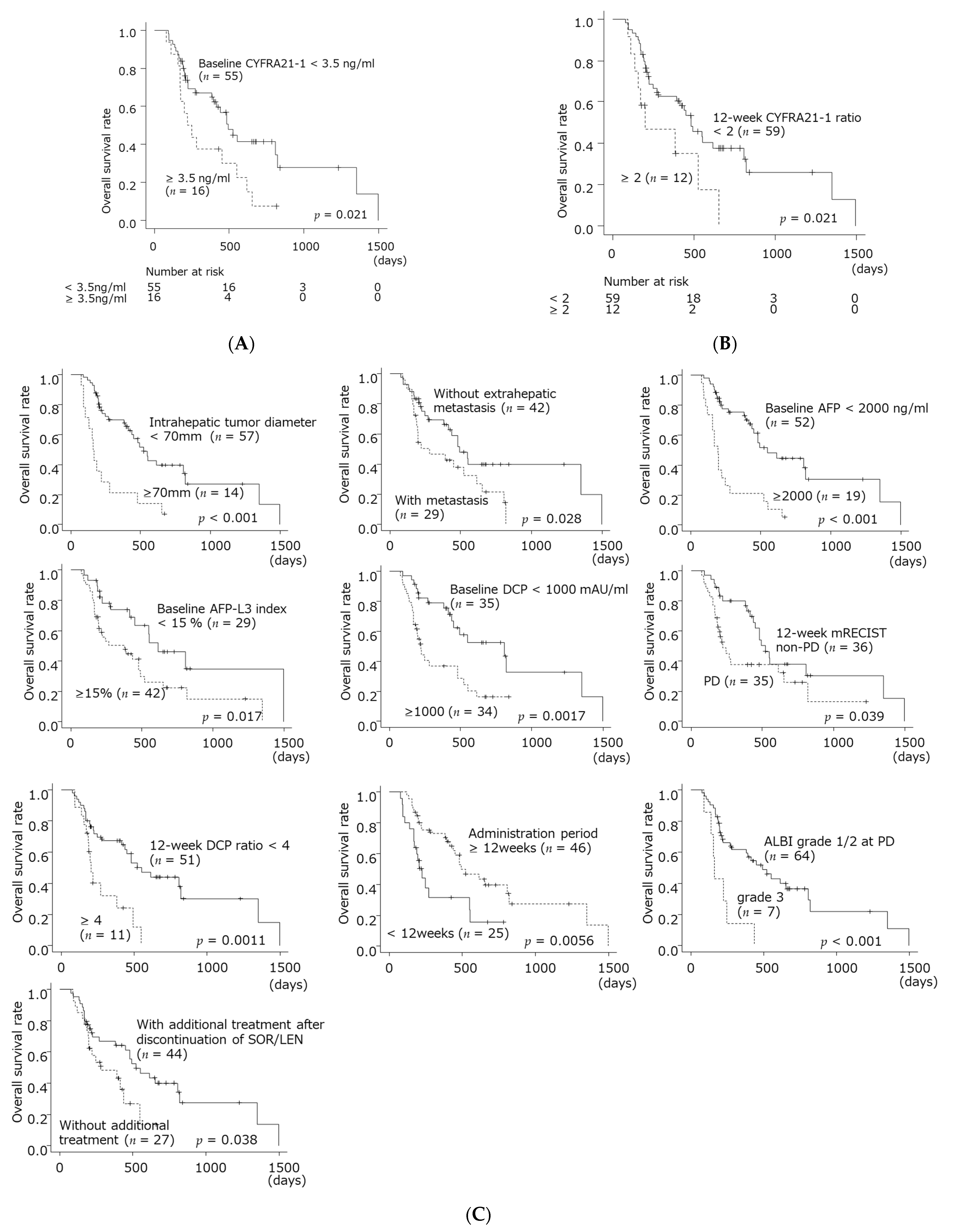
3.3. Factors Relating to Survival after SOR/LEN Administration
3.4. Characteristics in Patients with High CYFRA 21-1 Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Me, J.F.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.-Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Zhu, A.X.; Kang, Y.-K.; Yen, C.-J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Kudo, M.; Okusaka, T.; Motomura, K.; Ohno, I.; Morimoto, M.; Seo, S.; Wada, Y.; Sato, S.; Yamashita, T.; Furukawa, M.; et al. Ramucirumab after prior sorafenib in patients with advanced hepatocellular carcinoma and elevated alpha-fetoprotein: Japanese subgroup analysis of the REACH-2 trial. J. Gastroenterol. 2020, 55, 627–639. [Google Scholar] [CrossRef] [Green Version]
- Zhu, A.X.; Park, J.O.; Ryoo, B.-Y.; Yen, C.-J.; Poon, R.; Pastorelli, D.; Blanc, J.-F.; Chung, H.; Baron, A.D.; Pfiffer, T.E.F.; et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 859–870. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Ricci-Vitiani, L.; Lombardi, D.G.; Pilozzi, E.; Biffoni, M.; Todaro, M.; Peschle, C.; De Maria, R. Identification and expansion of human colon-cancer-initiating cells. Nature 2007, 445, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Al-Hajj, M.; Wicha, M.S.; Benito-Hernandez, A.; Morrison, S.J.; Clarke, M.F. Prospective identification of tumorigenic breast cancer cells. Proc. Natl. Acad. Sci. USA 2003, 100, 3983–3988. [Google Scholar] [CrossRef] [Green Version]
- Kawai, T.; Yasuchika, K.; Ishii, T.; Katayama, H.; Yoshitoshi, E.Y.; Ogiso, S.; Minami, T.; Miyauchi, Y.; Kojima, H.; Yamaoka, R.; et al. Identification of keratin 19-positive cancer stem cells associating human hepatocellular carcinoma using CYFRA 21-1. Cancer Med. 2017, 6, 2531–2540. [Google Scholar] [CrossRef] [Green Version]
- Kawai, T.; Yasuchika, K.; Ishii, T.; Katayama, H.; Yoshitoshi, E.Y.; Ogiso, S.; Kita, S.; Yasuda, K.; Fukumitsu, K.; Mizumoto, M.; et al. Keratin 19, a Cancer Stem Cell Marker in Human Hepatocellular Carcinoma. Clin. Cancer Res. 2015, 21, 3081–3091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association. Declaration of Helsinki. Law Med. Health Care 1991, 19, 264–265. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of Liver Function in Patients With Hepatocellular Carcinoma: A New Evidence-Based Approach—The ALBI Grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Kudo, M.; Han, K.-H.; Ye, S.-L.; Zhou, J.; Huang, Y.-H.; Lin, S.-M.; Wang, C.-K.; Ikeda, M.; Chan, S.L.; Choo, S.P.; et al. A Changing Paradigm for the Treatment of Intermediate-Stage Hepatocellular Carcinoma: Asia-Pacific Primary Liver Cancer Expert Consensus Statements. Liver Cancer 2020, 9, 245–260. [Google Scholar] [CrossRef] [PubMed]
- Kew, M.C. Hepatocellular carcinoma in developing countries: Prevention, diagnosis and treatment. World J. Hepatol. 2012, 4, 99–104. [Google Scholar] [CrossRef]
- Ueshima, K.; Kudo, M.; Takita, M.; Nagai, T.; Tatsumi, C.; Ueda, T.; Kitai, S.; Ishikawa, E.; Yada, N.; Inoue, T.; et al. Des-γ-Carboxyprothrombin May Be a Promising Biomarker to Determine the Therapeutic Efficacy of Sorafenib for Hepatocellular Carcinoma. Dig. Dis. 2011, 29, 321–325. [Google Scholar] [CrossRef]
- Miyahara, K.; Nouso, K.; Morimoto, Y.; Tomoda, T.; Kobayashi, S.; Takeuchi, Y.; Hagihara, H.; Kuwaki, K.; Ohnishi, H.; Ikeda, F.; et al. Evaluation of the effect of sorafenib using serum NX-des-γ-carboxyprothrombin in patients with hepatocellular carcinoma. Hepatol. Res. 2012, 43, 1064–1070. [Google Scholar] [CrossRef]
- Kuzuya, T.; Asahina, Y.; Tsuchiya, K.; Tanaka, K.; Suzuki, Y.; Hoshioka, T.; Tamaki, S.; Kato, T.; Yasui, Y.; Hosokawa, T.; et al. Early Decrease in α-Fetoprotein, but Not Des-γ-Carboxy Prothrombin, Predicts Sorafenib Efficacy in Patients with Advanced Hepatocellular Carcinoma. Oncology 2011, 81, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, H.; Ohno, S.; Miyazaki, M.; Hashimoto, K.; Egashira, A.; Saeki, H.; Watanabe, M.; Sugimachi, K. CYFRA 21-1 determination in patients with esophageal squamous cell carcinoma. Cancer 2000, 89, 1413–1417. [Google Scholar] [CrossRef]
- Anfuso, B.; El-Khobar, K.E.; Sukowati, C.; Tiribelli, C. The multiple origin of cancer stem cells in hepatocellular carcinoma. Clin. Res. Hepatol. Gastroenterol. 2015, 39, S92–S97. [Google Scholar] [CrossRef]
- Komuta, M.; Spee, B.; Borght, S.V.; De Vos, R.; Verslype, C.; Aerts, R.; Yano, H.; Suzuki, T.; Matsuda, M.; Fujii, H.; et al. Clinicopathological study on cholangiolocellular carcinoma suggesting hepatic progenitor cell origin. Hepatology 2008, 47, 1544–1556. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-S.; Heo, J.; Libbrecht, L.; Chu, I.-S.; Kaposi-Novak, P.; Calvisi, D.F.; Mikaelyan, A.; Roberts, L.; Demetris, A.J.; Sun, Z.; et al. A novel prognostic subtype of human hepatocellular carcinoma derived from hepatic progenitor cells. Nat. Med. 2006, 12, 410–416. [Google Scholar] [CrossRef]
- Dean, M.; Fojo, T.; Bates, S.E. Tumour stem cells and drug resistance. Nat. Rev. Cancer 2005, 5, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Caviglia, G.P.; Ciruolo, M.; Olivero, A.; Carucci, P.; Rolle, E.; Rosso, C.; Abate, M.L.; Risso, A.; Ribaldone, D.G.; Tandoi, F.; et al. Prognostic Role of Serum Cytokeratin-19 Fragment (CYFRA 21-1) in Patients with Hepatocellular Carcinoma. Cancers 2020, 12, 2776. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Fujita, J.; Murota, M.; Li, J.-Q.; Ishida, T.; Nishioka, M.; Imaida, Y.; Kuriyama, S. CYFRA 21-1 is released in TNF-α-induced apoptosis in the hepatocellular carcinoma cell line HuH-7. Int. J. Oncol. 2002, 21, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.-J.; Li, Y.; Tan, Y.-X.; Jiang, M.-R.; Tian, B.; Liu, Y.-K.; Shao, X.-X.; Ye, S.-L.; Wu, J.-R.; Zeng, R.; et al. From proteomic analysis to clinical significance: Overexpression of cytokeratin 19 correlates with hepatocellular carcinoma metastasis. Mol. Cell. Proteom. 2004, 3, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuchiya, K.; Komuta, M.; Yasui, Y.; Tamaki, N.; Hosokawa, T.; Ueda, K.; Kuzuya, T.; Itakura, J.; Nakanishi, H.; Takahashi, Y.; et al. Expression of Keratin 19 Is Related to High Recurrence of Hepatocellular Carcinoma after Radiofrequency Ablation. Oncology 2011, 80, 278–288. [Google Scholar] [CrossRef]
- Uenishi, T.; Kubo, S.; Yamamoto, T.; Shuto, T.; Ogawa, M.; Tanaka, H.; Tanaka, S.; Kaneda, K.; Hirohashi, K. Cytokeratin 19 expression in hepatocellular carcinoma predicts early postoperative recurrence. Cancer Sci. 2003, 94, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Uenishi, T.; Yamazaki, O.; Yamamoto, T.; Hirohashi, K.; Tanaka, H.; Tanaka, S.; Hai, S.; Ono, K.; Kubo, S. Clinical significance of serum cytokeratin-19 fragment (CYFRA 21-1) in hepatocellular carcinoma. J. Hepato-Biliary-Pancreat. Surg. 2006, 13, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Govaere, O.; Komuta, M.; Berkers, J.; Spee, B.; Janssen, C.; De Luca, F.; Katoonizadeh, A.; Wouters, J.; van Kempen, L.; Durnez, A.; et al. Keratin 19: A key role player in the invasion of human hepatocellular carcinomas. Gut 2013, 63, 674–685. [Google Scholar] [CrossRef] [Green Version]
- Durnez, A.; Verslype, C.; Nevens, F.; Fevery, J.; Aerts, R.; Pirenne, J.; Lesaffre, E.; Libbrecht, L.; Desmet, V.; Roskams, T. The clinicopathological and prognostic relevance of cytokeratin 7 and 19 expression in hepatocellular carcinoma. A possible progenitor cell origin. Histopathology 2006, 49, 138–151. [Google Scholar] [CrossRef]
- Ku, N.-O.; Strnad, P.; Bantel, H.; Omary, B. Keratins: Biomarkers and modulators of apoptotic and necrotic cell death in the liver. Hepatology 2016, 64, 966–976. [Google Scholar] [CrossRef] [Green Version]
- Zen, C.; Zen, Y.; Mitry, R.R.; Corbeil, D.; Karbanova, J.; O’Grady, J.; Karani, J.; Kane, P.; Heaton, N.; Portmann, B.C.; et al. Mixed phenotype hepatocellular carcinoma after transarterial chemoembolization and liver transplantation. Liver Transplant. 2011, 17, 943–954. [Google Scholar] [CrossRef]
- Zeng, Z.; Ren, J.; O’Neil, M.; Zhao, J.; Bridges, B.; Cox, J.; Abdulkarim, B.; Schmitt, T.M.; Kumer, S.C.; Weinman, S.A. Impact of stem cell marker expression on recurrence of TACE-treated hepatocellular carcinoma post liver transplantation. BMC Cancer 2012, 12, 584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terashima, T.; Yamashita, T.; Takata, N.; Nakagawa, H.; Toyama, T.; Arai, K.; Kitamura, K.; Yamashita, T.; Sakai, Y.; Mizukoshi, E.; et al. Post-progression survival and progression-free survival in patients with advanced hepatocellular carcinoma treated by sorafenib. Hepatol. Res. 2015, 46, 650–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraoka, A.; Kumada, T.; Kariyama, K.; Takaguchi, K.; Itobayashi, E.; Shimada, N.; Tajiri, K.; Tsuji, K.; Ishikawa, T.; Ochi, H.; et al. Therapeutic potential of lenvatinib for unresectable hepatocellular carcinoma in clinical practice: Multicenter analysis. Hepatol. Res. 2019, 49, 111–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomonari, T.; Sato, Y.; Tani, J.; Hirose, A.; Ogawa, C.; Morishita, A.; Tanaka, H.; Tanaka, T.; Taniguchi, T.; Okamoto, K.; et al. Comparison of therapeutic outcomes of sorafenib and lenvatinib as primary treatments for hepatocellular carcinoma with a focus on molecular-targeted agent sequential therapy: A propensity score-matched analysis. Hepatol. Res. 2020, 51, 472–481. [Google Scholar] [CrossRef]
- Takada, H.; Kurosaki, M.; Tsuchiya, K.; Komiyama, Y.; Itakura, J.; Takahashi, Y.; Nakanishi, H.; Yasui, Y.; Tamaki, N.; Maeyashiki, C.; et al. Baseline and Early Predictors of Good Patient Candidates for Second-Line after Sorafenib Treatment in Unresectable Hepatocellular Carcinoma. Cancers 2019, 11, 1256. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.-K.; Yen, C.-L.; Shiu, S.-I.; Lee, S.-W.; Chang, P.-Y.; Yeh, H.-Z.; Lee, T.-Y. Transcatheter arterial chemoembolization after stopping sorafenib therapy for advanced hepatocellular carcinoma. PLoS ONE 2017, 12, e0188999. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| All (n = 71) | SOR (n = 36) | LEN (n = 35) | p Value | |
|---|---|---|---|---|
| Male gender, n (%) | 62 (87) | 31 (86) | 31 (89) | 1.0 |
| Etiology: HBV/HCV/others, n (%) | 13/33/25 (18/47/35) | 7/19/10 (19/53/28) | 6/14/15 (17/40/43) | 0.42 |
| At the time of administration of SOR/LEN Age (years), median(range) | 70 (52–91) | 69 (56–91) | 70 (52–83) | 0.92 |
| Tumor diameter (mm), median(range) | 27 (8.4–180) | 29 (8.4–160) | 27 (12–180) | 0.85 |
| Tumor number, median(range) | 6 (1–10) | 10 (1–10) | 6 (1–10) | 0.046 |
| Portal vein tumor thrombosis (Vp 2/3), n (%) | 16 (22) | 8 (22) | 8 (23) | 1.0 |
| Extrahepatic metastasis, n (%) | 29 (41) | 19 (53) | 10 (29) | 0.054 |
| ALBI grade 1/2/3, n (%) | 20/48/3 (28/68/4) | 10/24/2 (28/67/5) | 10/24/1 (29/68/3) | 1.0 |
| BCLC stage B/C, n (%) | 32/39 (45/55) | 13/23 (36/64) | 19/16 (54/46) | 0.16 |
| AFP (ng/mL), median(range) | 143 (1.8–421,248) | 238 (1.8–421,248) | 143 (4.0–146,670) | 0.48 |
| AFP L3 index (%), median(range) | 18 (0.5–94) | 29 (0.5–87) | 15 (0.5–94) | 0.31 |
| DCP (mAU/mL), median(range) | 939 (15–616,708) | 1671 (15–616,708) | 513 (25–501,890) | 0.41 |
| CYFRA21-1 (ng/mL), median(range) | 2.6 (0.76–10.6) | 2.5 (0.76–10.6) | 2.7 (1.1–8.9) | 0.63 |
| Administration dose, reduction/full dose, n (%) | 16/55 (22/78) | 32/4 (89/11) | 12/23 (34/66) | 0.001 |
| Administration duration (weeks), median(range) | 17 (4–95) | 16 (4–95) | 21 (4–88) | 0.30 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| HR | p Value | HR | 95%CI | p Value | ||
| At the start of administration | Tumor diameter ≥ 70 mm | 3.4 | <0.001 | 2.3 | 0.97–5.3 | 0.059 |
| Tumor number ≥ 4 | 1.3 | 0.44 | ||||
| Portal vein tumor thrombosis (Vp 2/3) | 1.7 | 0.097 | ||||
| Extrahepatic metastasis | 2.0 | 0.031 | 1.6 | 0.81–3.0 | 0.19 | |
| ALBI grade 2/3 | 1.5 | 0.24 | ||||
| AFP ≥ 2000 ng/ml | 3.7 | <0.001 | 2.0 | 0.91–4.6 | 0.079 | |
| AFP-L3 index ≥ 15% | 2.2 | 0.020 | 2.2 | 1.1–4.6 | 0.030 | |
| DCP ≥ 1000 mAU/ml | 4.9 | 0.0025 | 1.3 | 0.55–2.9 | 0.59 | |
| CYFRA21-1 ≥ 3.5 ng/ml | 2.1 | 0.024 | 2.1 | 0.99–4.6 | 0.051 | |
| After the start of administration | 12-week mRECIST PD | 1.9 | 0.042 | 1.7 | 1.01–3.7 | 0.019 |
| 12-week AFP ratio ≥ 0.8 | 1.9 | 0.051 | ||||
| 12-week DCP ratio ≥ 4 | 3.0 | 0.018 | 2.5 | 1.1–6.3 | 0.047 | |
| 12-week CYFRA21-1 ratio ≥ 2 | 2.4 | 0.0025 | 3.6 | 1.2–11 | 0.023 | |
| Administration period < 12 weeks | 2.4 | 0.0071 | 2.4 | 1.1–5.7 | 0.046 | |
| ALBI grade 3 at PD | 3.9 | 0.0020 | 2.3 | 0.86–6.4 | 0.097 | |
| No additional treatment after discontinuation of SOR/LEN | 2.0 | 0.041 | 2.5 | 1.1–6.1 | 0.036 | |
| Baseline < 3.5 ng/mL and 12-Week CYFRA21-1 Ratio < 2 (n = 46) | Baseline ≥ 3.5 ng/mL or 12-Week CYFRA21-1 Ratio ≥ 2 (n = 25) | p Value | |
|---|---|---|---|
| Male gender, n (%) | 41 (89%) | 21 (84%) | 0.71 |
| At the time of administration of SOR/LEN Age (years), median(range) | 69 (52–86) | 72 (52–91) | 0.47 |
| Tumor size ≥70 mm, n (%) | 7 (15%) | 7 (28%) | 0.22 |
| Tumor number ≥4, n (%) | 38 (83%) | 17 (68%) | 0.23 |
| up to 7 out, n (%) | 37 (80%) | 21 (84%) | 1.0 |
| Portal vein thrombosis (Vp 2/3), n (%) | 11 (24%) | 5 (20%) | 0.78 |
| Extrahepatic metastasis, n (%) | 16 (35%) | 13 (52%) | 0.21 |
| ALBI grade 2or3, n (%) | 34 (74) | 17 (68) | 0.59 |
| AFP ≥2000 ng/mL, n (%) | 7 (15%) | 12 (48%) | 0.005 |
| AFP L3 index ≥ 15%, n (%) | 24 (52%) | 18 (72%) | 0.13 |
| DCP ≥ 1000 mAU/mL, n (%) | 19 (42%) | 15 (63%) | 0.13 |
| 12-week mRECIST PD, n (%) | 21 (47%) | 12 (52%) | 0.80 |
| TACE unsuitable pattern, n (%) | 19 (41%) | 19 (76%) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takada, H.; Osawa, L.; Komiyama, Y.; Kato, R.; Nakakuki, N.; Muraoka, M.; Suzuki, Y.; Tatsumi, A.; Sato, M.; Takahashi, E.; et al. Usefulness of Circulating CYFRA21-1 in Patients as a Biomarker in Patients Taking Sorafenib or Lenvatinib for Unresectable Hepatocellular Carcinoma. Reports 2021, 4, 25. https://doi.org/10.3390/reports4030025
Takada H, Osawa L, Komiyama Y, Kato R, Nakakuki N, Muraoka M, Suzuki Y, Tatsumi A, Sato M, Takahashi E, et al. Usefulness of Circulating CYFRA21-1 in Patients as a Biomarker in Patients Taking Sorafenib or Lenvatinib for Unresectable Hepatocellular Carcinoma. Reports. 2021; 4(3):25. https://doi.org/10.3390/reports4030025
Chicago/Turabian StyleTakada, Hitomi, Leona Osawa, Yasuyuki Komiyama, Ryoh Kato, Natsuko Nakakuki, Masaru Muraoka, Yuichiro Suzuki, Akihisa Tatsumi, Mitsuaki Sato, Ei Takahashi, and et al. 2021. "Usefulness of Circulating CYFRA21-1 in Patients as a Biomarker in Patients Taking Sorafenib or Lenvatinib for Unresectable Hepatocellular Carcinoma" Reports 4, no. 3: 25. https://doi.org/10.3390/reports4030025
APA StyleTakada, H., Osawa, L., Komiyama, Y., Kato, R., Nakakuki, N., Muraoka, M., Suzuki, Y., Tatsumi, A., Sato, M., Takahashi, E., Takano, S., Fukasawa, M., Yamaguchi, T., Inoue, T., Maekawa, S., & Enomoto, N. (2021). Usefulness of Circulating CYFRA21-1 in Patients as a Biomarker in Patients Taking Sorafenib or Lenvatinib for Unresectable Hepatocellular Carcinoma. Reports, 4(3), 25. https://doi.org/10.3390/reports4030025